Advancing Therapies for Cancer—From Mustard Gas to CAR T


1
Department of Bioengineering, University of Colorado Anschutz Medical Campus, Aurora, CO 80045, USA
2
Cell and Molecular Biology Program, Colorado State University, Fort Collins, CO 80523, USA
3
Department of Clinical Sciences, Colorado State University, Fort Collins, CO 80523, USA
4
Epidemiology Section, Colorado School of Public Health, Colorado State University, Fort Collins, CO 80523, USA
*
Author to whom correspondence should be addressed.
Sci 2020, 2(4), 90; https://0-doi-org.brum.beds.ac.uk/10.3390/sci2040090
Submission received: 27 May 2020
/
Accepted: 5 June 2020
/
Published: 7 December 2020
(This article belongs to the Special Issue Development of Targeted Therapies for the Clinical Management of Cancer)
{kind=link}
Abstract
:The development of targeted therapeutics for cancer continues to receive intense research attention as laboratories and pharmaceutical companies seek to develop drugs and technologies that improve treatment efficacy and mitigate harmful side effects. In the aftermath of World War I, it was discovered that mustard gas destroys rapidly dividing cells and could be used to treat cancer. Since then, chemotherapy has remained a predominant treatment for cancer; however, the destruction of dividing cells throughout the body yields devastating side effects including off-target damage of the digestive tract, bone marrow, skin, and reproductive tract. Furthermore, the high mutation rate of cancerous cells often renders chemotherapy ineffective long-term. Therapies with improved specificity, localization, and efficacy are redefining cancer treatment. Herein, we define and summarize the principal advancements in targeted cancer treatment and briefly comment on the march towards personalized medicine in the treatment of human cancer.
1. Introduction
Cancer remains one of the principal public health concerns throughout the world [1]. The remarkable heterogeneity of cancer, even within tissue types, has rendered it extremely difficult to diagnose and treat. Throughout most of human history, surgical resection of tumors has been the only treatment option [2]. While effective when possible, the complete removal of a tumor is notoriously difficult, and resection is impossible for metastasized tumors or blood cancers. In the early 1900s, low-dose radiation therapy emerged as a second strategy for cancer treatment. Again, while effective in some cases, it was soon discovered that radiation therapy can cause cancer as well as cure it, and is often accompanied by severe side effects [2]. Following World War I, it was discovered that mustard gas selectively kills prolific cells; soon thereafter, it underwent testing as a treatment for cancer [3,4]. The success of these experiments effectively established the third method of cancer treatment: chemotherapy. For over half a century, these three “pillars” of cancer treatment have remained largely unchanged.
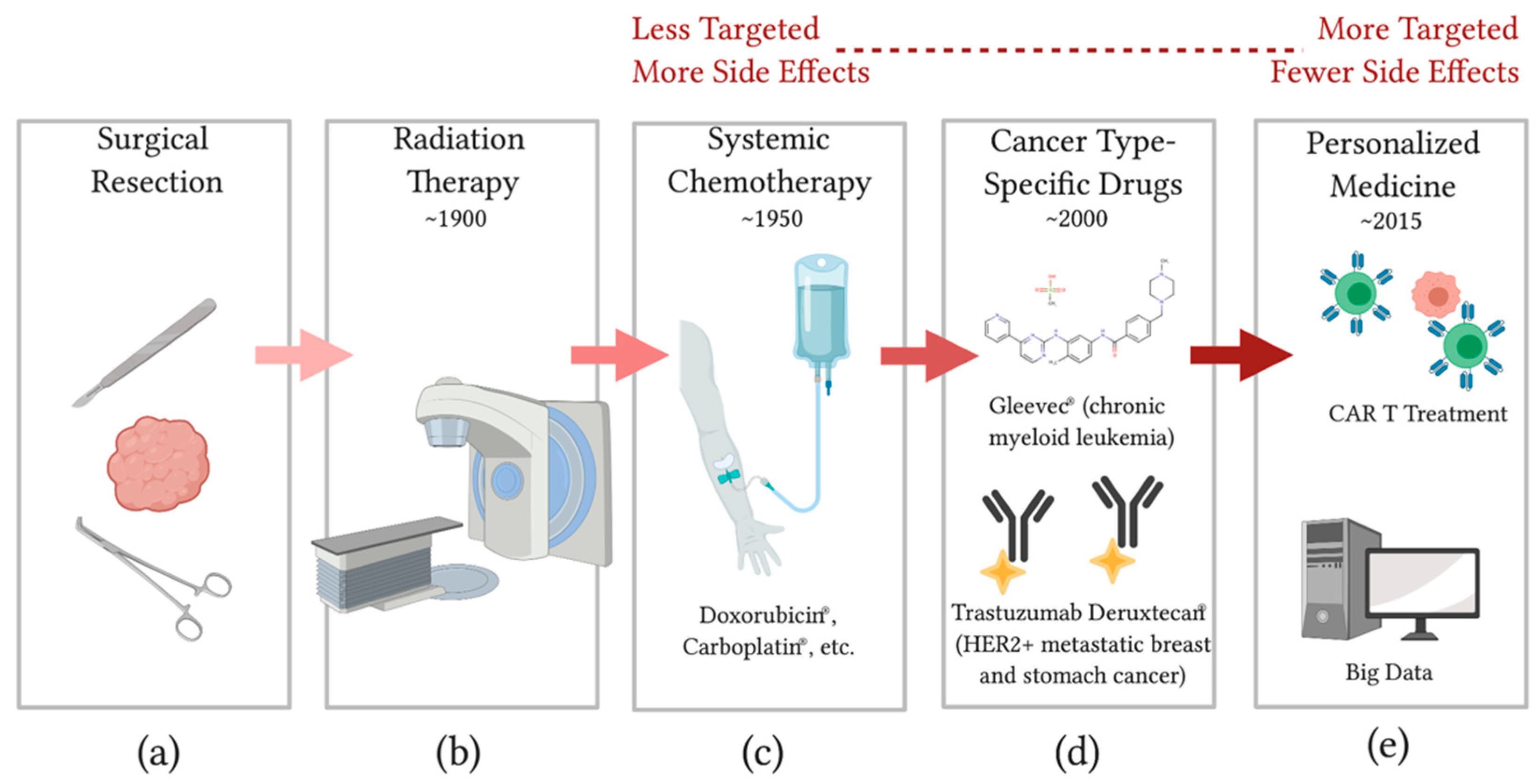
While chemotherapy and radiation therapy have certainly revolutionized the clinical management of cancer, the off-target toxicity of both approaches remains a critical problem [5]. Furthermore, even the combination of these treatment strategies is often ineffective in the presence of aggressive, metastatic, or rapidly mutating cancers. In the context of these clinical problems, two principal approaches to improving the specificity and efficacy of cancer treatments have emerged. First, advancing technologies for cancer imaging/mapping, surgical and radiation precision, or localized delivery of chemotherapeutic drugs are sharpening the three canonical pillars of cancer treatment by improving specificity (reducing side-effects) and efficacy [6,7]. Second, the identification of cancer cell-specific pathways and biochemical markers are enabling the development of targeted and personalized therapeutics [8]. These include targeted small molecule enzyme inhibitors, antibody-based therapeutics, and personalized adoptive cell transfer (ACT), such as chimeric antigen receptor T-cell (CAR T) therapy. Targeted therapy has again revolutionized cancer treatment and has become the fourth “pillar” in the clinic. Figure 1 summarizes the current strategies for cancer treatment and illustrates the advancement of the field towards powerful, personalized, patient-specific therapeutics that minimize harmful and dreaded side effects.
2. Discussion
The development and approval of Gleevec® (imatinib) in 1998, a small molecule drug that inhibits the cancer-specific BCR-ABL fusion protein in chronic myelogenous leukemias (CML), marked the dawn of targeted therapeutics [9]. Small molecule enzyme inhibitors are attractive because of their specificity, ease of manufacture, predictability, and ease of administration [10,11]. Furthermore, small molecule enzyme inhibitors can be used to target extracellular, cell-surface, and intracellular pathways, giving them a remarkable range of utility. Finally, as will be discussed below, libraries of small molecule inhibitors can be rapidly screened in high-throughput arrays, making them promising in the development of patient-specific treatment.
The recent approval of ENHERTU® (trastuzumab deruxtecan) marked the success of another approach to targeted drug delivery; the therapeutic uses a human epidermal growth factor receptor-2 (HER2)-directed antibody to deliver a topoisomerase I inhibitor (broad-spectrum chemotherapy drug) specifically to HER2+ breast cancer cells [12,13]. Rather than implementing an inhibitor specific to cancer cells, this approach uses a cancer-specific, antibody-based delivery system for a broad-spectrum chemotherapy agent. Antibody targeting of other cancer-associated pathways, including immune checkpoints, has shown great promise, and is being actively pursued in the field [14].
Within the field of targeted therapeutics, CAR T has perhaps received the most attention in recent years. CAR T involves isolating a patient’s circulating killer T cells, genetically engineering the cells to express a chimeric antigen receptor that recognizes a cancer-specific antigen, and then expanding the cells and infusing them back into the patient. This “living therapeutic” trains the patient’s own immune system to recognize and kill cancer cells. Third generation CAR T therapy is particularly exciting because it bypasses the need for proper MHC antigen presentation within the cancer cells, which is often defective in cancer cells due to mutation [15].
Notably, each of these three approaches to targeted therapy depend entirely on the identification of cancer-specific pathways and markers. Inhibiting the pathways or using the markers to selectively deliver cytotoxic drugs has been shown to be extremely effective, but identifying targets that are truly cancer-specific is difficult. Two approaches to this challenge in the development of targeted therapeutics are being pursued. First, as in the cases of Gleevec® and ENHERTU®, a pathway/marker that is present predominantly in the cancer cells of most patients with the specific cancer type was exploited for cancer treatment. Again, while effective, side effects are not eliminated and a significant proportion of patients do not respond. A second approach involves truly personalized medicine: using “Big Data” (the combination of patient genetics, epigenetics, transcriptomics, proteomics, RNA-seq, etc.), gene therapy, or high-throughput drug screening using patient-specific cancer biopsies, clinics can predict, develop, and prescribe “tailor-made” treatment regimens on an individual level [16,17,18,19,20,21]. This type of personalized medicine needs fine-tuning and greater validation of efficacy before it will be profitable, but is exceedingly promising. Improved identification of cancer-specific pathways and markers, streamlined development of small molecule inhibitors, effective patient data analysis, and fast high-throughput screening methods will all prove to be valuable advancements in the march towards patient-specific cancer treatment.
Author Contributions
Research and writing by D.K.J., Figure development by S.D., Paper conception and advising by M.A.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Sudhakar, A. History of cancer, ancient and modern treatment methods. J. Cancer Sci. Ther. 2009, 1, 1–4. [Google Scholar] [CrossRef] [Green Version]
- DeVita, V.T.; Chu, E. A history of cancer chemotherapy. Cancer Res. 2008, 68, 8643–8653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, S.L. War! What is it good for? Mustard gas medicine. Can. Med. Assoc. J. 2017, 189, E321–E322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coates, A.; Abraham, S.; Kaye, S.; Sowerbutts, T.; Frewin, C.; Fox, R.; Tattersall, M. On the receiving end—Patient perception of the side-effects of cancer chemotherapy. Eur. J. Cancer Clin. Oncol. 1983, 19, 203–208. [Google Scholar] [CrossRef]
- Friedman, A.A.; Letai, A.; Fisher, D.E.; Flaherty, K.T. Precision medicine for cancer with next-generation functional diagnostics. Nat. Rev. Cancer 2015, 15, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Herrero, E.; Fernandez-Medarde, A. Advanced targeted therapies in cancer: Drug nanocarriers, the future of chemotherapy. Eur. J. Pharm. Biopharm. 2015, 93, 52–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.T.; Tan, Y.J.; Oon, C.E. Molecular targeted therapy: Treating cancer with specificity. Eur. J. Pharmacol. 2018, 834, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Boluda, J.C.; Cervantes, F. Imatinib mesylate (Gleevec, Glivec): A new therapy for chronic myeloid leukemia and other malignancies. Drugs Today 2002, 38, 601. [Google Scholar] [CrossRef]
- Chen, S.; Song, Z.; Zhang, A. Small-molecule immuno-oncology therapy: Advances, challenges and new directions. Curr. Top. Med. Chem. 2019, 19, 180–185. [Google Scholar] [CrossRef]
- Imai, K.; Takaoka, A. Comparing antibody and small-molecule therapies for cancer. Nat. Rev. Cancer 2006, 6, 714–727. [Google Scholar] [CrossRef] [PubMed]
- Modi, S.; Saura, C.; Yamashita, T.; Park, Y.H.; Kim, S.-B.; Tamura, K.; Andre, F.; Iwata, H.; Ito, Y.; Tsurutani, J.; et al. Trastuzumab deruxtecan in previously treated HER2-positive breast cancer. N. Engl. J. Med. 2019, 382, 610–621. [Google Scholar] [CrossRef] [PubMed]
- Tamura, K.; Tsurutani, J.; Takahashi, S.; Iwata, H.; Krop, I.; Redfern, C.; Sagara, Y.; Doi, T.; Park, H.; Murthy, R.K.; et al. Trastuzumab deruxtecan (DS-8201a) in patients with advanced HER2-positive breast cancer previously treated with trastuzumab emtansine: A dose-expansion, phase 1 study. Lancet Oncol. 2019, 20, 816–826. [Google Scholar] [CrossRef]
- Leach, D.R.; Krummel, M.F.; Allison, J.P. Enhancement of antitumor immunity by CTLA-4 blockade. Science 1996, 271, 1734–1736. [Google Scholar] [CrossRef] [Green Version]
- Stern, L.A.; Jonsson, V.D.; Priceman, S.J. CAR T cell therapy progress and challenges for solid tumors. Cancer Treat. Res. 2020, 180, 297–326. [Google Scholar] [CrossRef]
- Cappello, P.; Novelli, F. Next generation of cancer immunotherapy calls for combination. Oncoscience 2017, 4, 19–20. [Google Scholar] [CrossRef]
- He, L.; Kulesskiy, E.; Saarela, J.; Turunen, L.; Wennerberg, K.; Aittokallio, T.; Tang, J. Methods for high-throughput drug combination screening and synergy scoring. Methods Mol. Biol. 2018, 1711, 351–398. [Google Scholar] [CrossRef]
- Kantarjian, H.; Yu, P.P. Artificial intelligence, big data, and cancer. JAMA Oncol. 2015, 1, 573–574. [Google Scholar] [CrossRef]
- Kather, J.N.; Charoentong, P.; Suarez-Carmona, M.; Herpel, E.; Klupp, F.; Ulrich, A.; Schneider, M.; Zoernig, I.; Luedde, T.; Jaeger, D.; et al. High-throughput screening of combinatorial immunotherapies with patient-specific in silico models of metastatic colorectal cancer. Cancer Res. 2018, 78, 5155–5163. [Google Scholar] [CrossRef] [Green Version]
- Kondo, J.; Ekawa, T.; Endo, H.; Yamazaki, K.; Tanaka, N.; Kukita, Y.; Okuyama, H.; Okami, J.; Imamura, F.; Ohue, M.; et al. High-throughput screening in colorectal cancer tissue-originated spheroids. Cancer Sci. 2018, 110, 345–355. [Google Scholar] [CrossRef]
- Low, S.-K.; Zembutsu, H.; Nakamura, Y. Breast cancer: The translation of big genomic data to cancer precision medicine. Cancer Sci. 2017, 109, 497–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Progress of the clinical management of cancer. Throughout most of human history, surgical resection of solid tumors was the only possible treatment (a). Radiation therapy (b) can be very effective, but comes with severe side effects and, like resection, is limited to localized tumors. Chemotherapy, targeted therapies, and personalized medicine (c–e) are new, powerful drug-based strategies that aim to improve treatment efficacy and/or reduce patient side effects.
Figure 1.
Progress of the clinical management of cancer. Throughout most of human history, surgical resection of solid tumors was the only possible treatment (a). Radiation therapy (b) can be very effective, but comes with severe side effects and, like resection, is limited to localized tumors. Chemotherapy, targeted therapies, and personalized medicine (c–e) are new, powerful drug-based strategies that aim to improve treatment efficacy and/or reduce patient side effects.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Jarrell, D.K.; Drake, S.; Brown, M.A. Advancing Therapies for Cancer—From Mustard Gas to CAR T. Sci 2020, 2, 90. https://0-doi-org.brum.beds.ac.uk/10.3390/sci2040090
AMA Style
Jarrell DK, Drake S, Brown MA. Advancing Therapies for Cancer—From Mustard Gas to CAR T. Sci. 2020; 2(4):90. https://0-doi-org.brum.beds.ac.uk/10.3390/sci2040090
Chicago/Turabian StyleJarrell, Dillon K., Seth Drake, and Mark A. Brown. 2020. "Advancing Therapies for Cancer—From Mustard Gas to CAR T" Sci 2, no. 4: 90. https://0-doi-org.brum.beds.ac.uk/10.3390/sci2040090