Air Quality in the Working Environment and Respiratory Health of Female Congolese Stone Quarry Workers

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
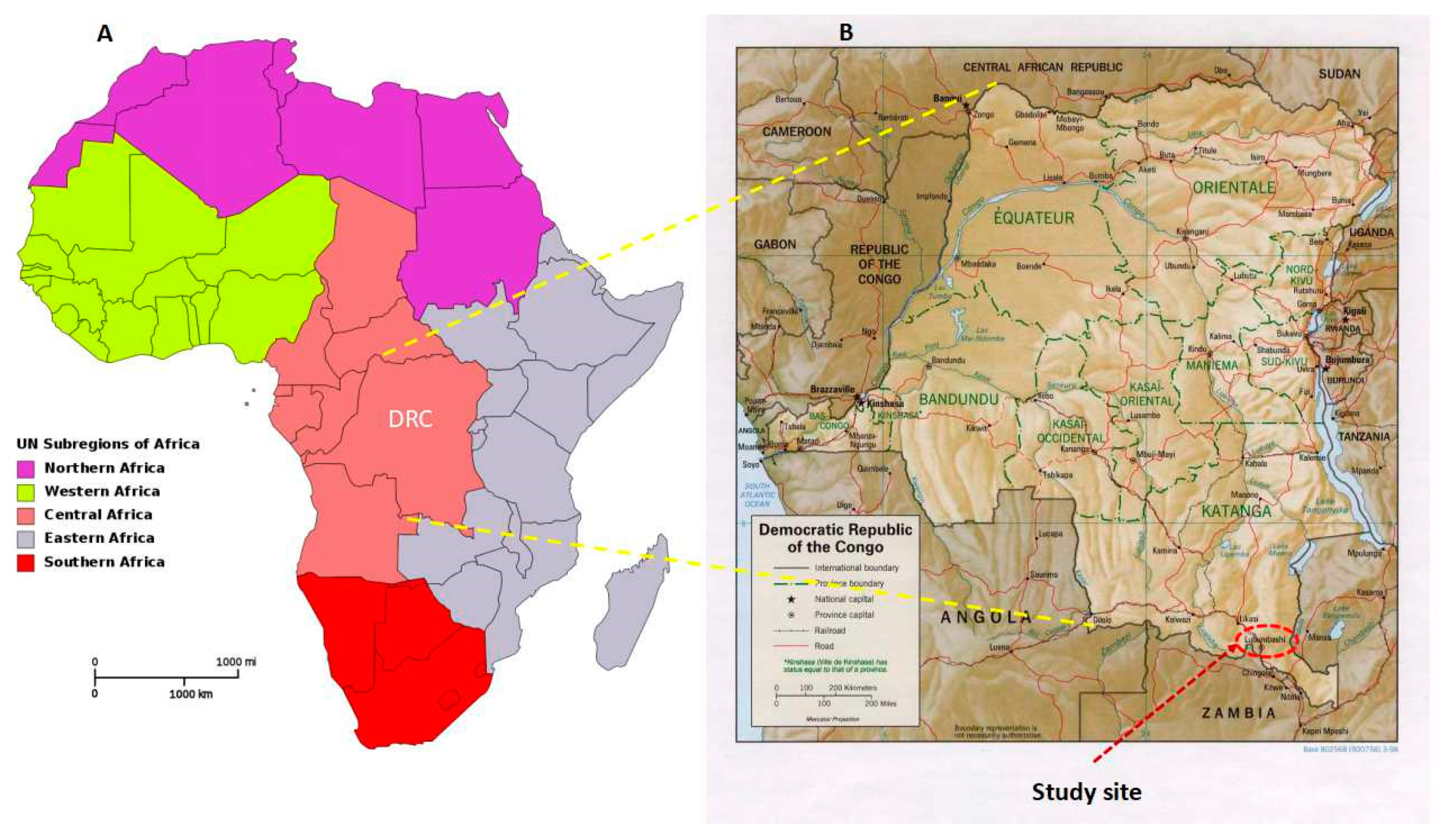
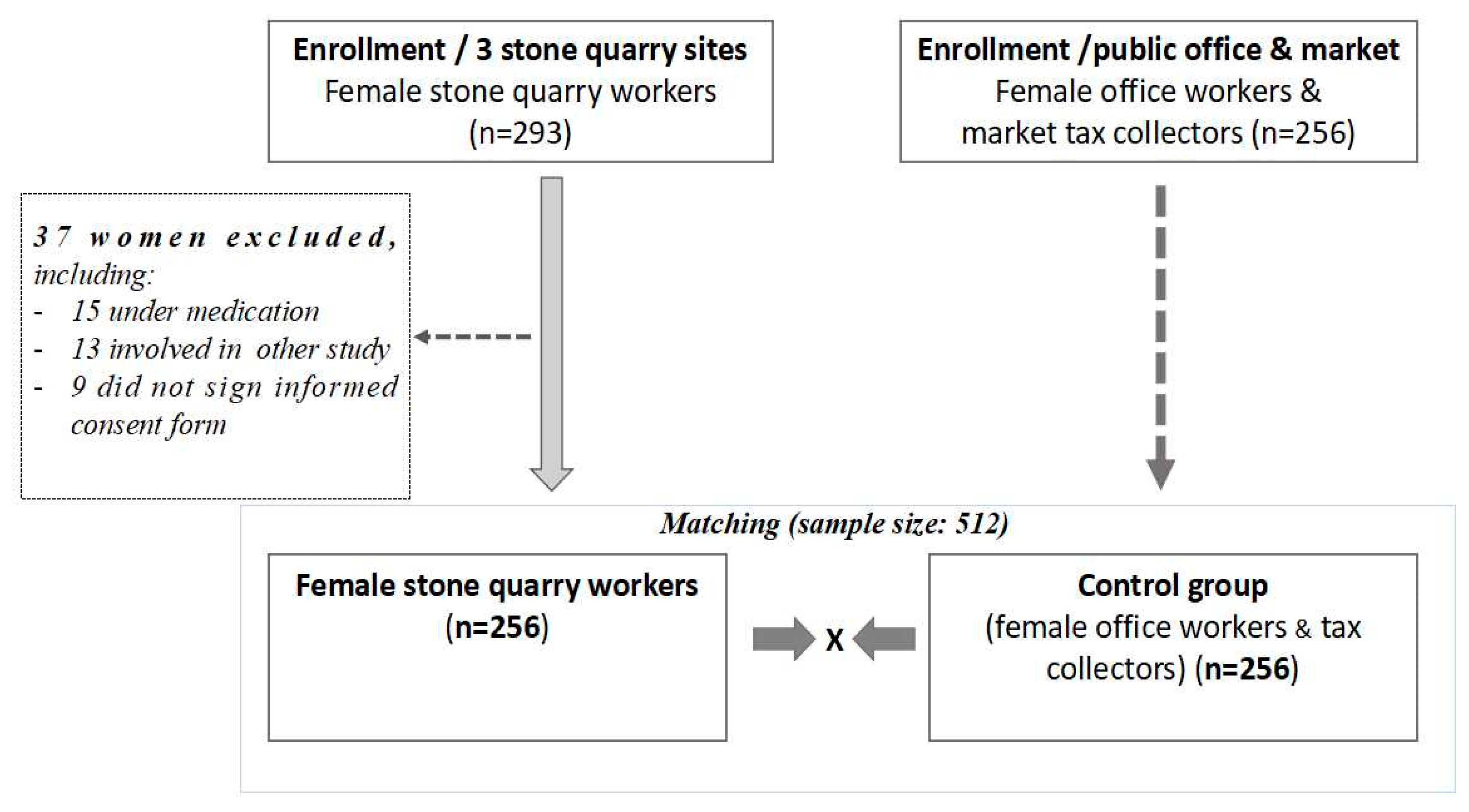
2.1. Study Design, Sites, and Participants
2.2. Survey Questionnaire and Outcome Variables
2.3. Ethical Considerations, Data Collection, and Statistical Analysis
3. Results
3.1. Air Quality in the Working Environment and Characteristics of the Participants
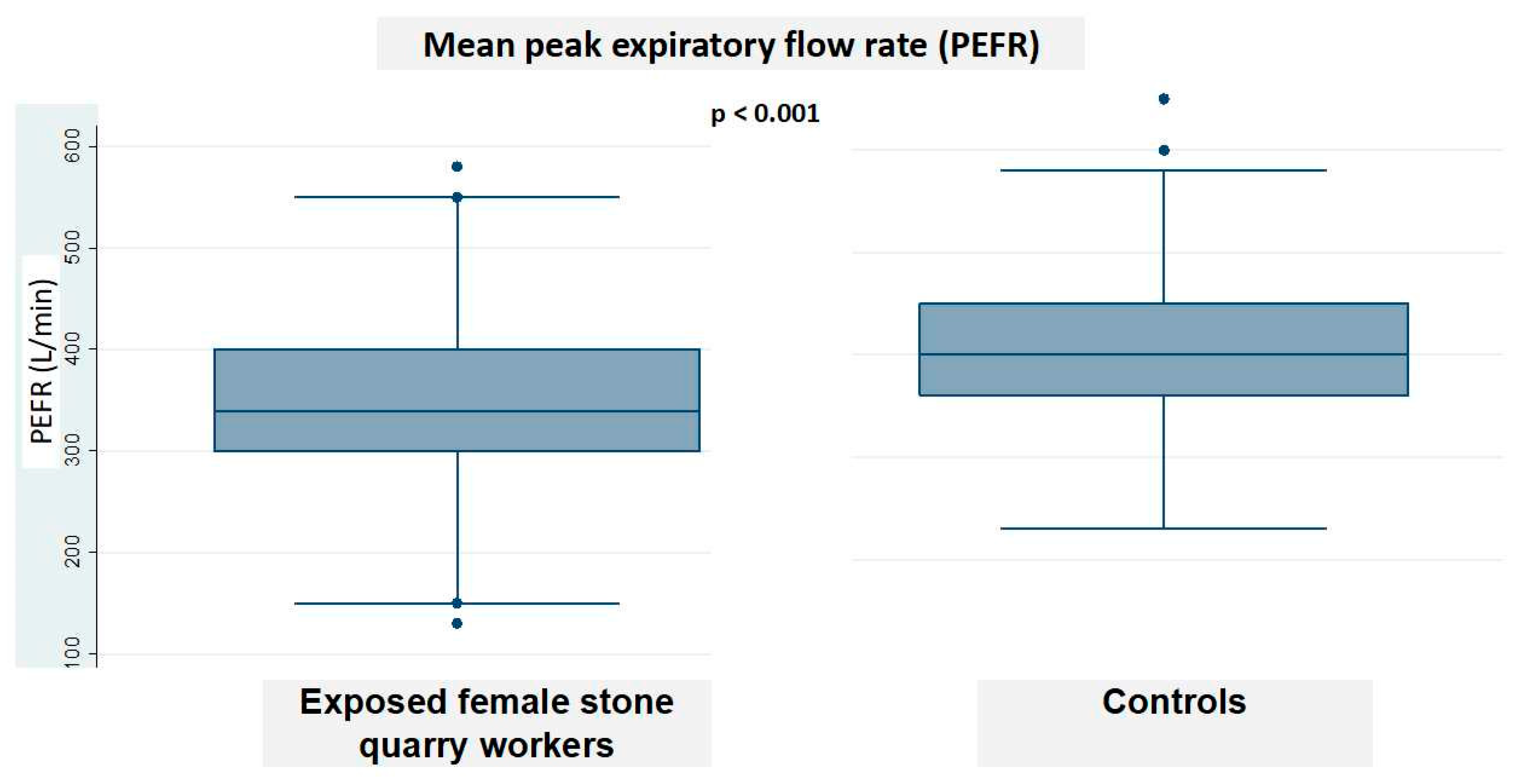
3.2. Prevalence of Respiratory Complaints Among the Exposed Workers and Controls, and Lung Function Outcomes
3.3. Association Between Occupational Characteristics and Respiratory Manifestations
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Availability of data and materials
References
- World Health Organization (WHO). Air Pollution. Available online: https://www.who.int/airpollution/ambient/about/en/ (accessed on 4 August 2020).
- UN Environment. Towards a Pollution-Free Planet. Available online: https://www.unenvironment.org/resources/report/towards-pollution-free-planet-background-report (accessed on 4 August 2020).
- Wang, H.; Song, L.; Ju, W.; Wang, X.; Dong, L.; Zhang, Y.; Ya, P.; Yang, C.; Li, F. The acute airway inflammation induced by PM2.5 exposure and the treatment of essential oils in Balb/c mice. Sci. Rep. 2017, 7, 44256–44269. [Google Scholar] [CrossRef]
- Xing, Y.F.; Xu, Y.H.; Shi, M.H.; Lian, Y.X. The impact of PM2.5 on the human respiratory system. J. Thorac. Dis. 2016, 8, E69–E74. [Google Scholar] [PubMed]
- Herrera, R.; Berger, U.; Von Ehrenstein, O.S.; Diaz, I.; Huber, S.; Muñoz, D.M.; Radon, K. Estimating the causal impact of proximity to gold and copper mines on respiratory diseases in Chilean children: An application of targeted maximum likelihood estimation. Int. J. Environ. Res. Public Health 2018, 15, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, R.; Zhou, R.; Zhang, J. Function of PM2.5 in the pathogenesis of lung cancer and chronic airway inflammatory diseases. Oncol. Lett. 2018, 15, 7506–7514. [Google Scholar] [CrossRef] [Green Version]
- Kurai, J.; Watanabe, M.; Noma, H.; Iwata, K.; Taniguchi, J.; Sano, H.; Tohda, Y.; Shimizu, E. Estimation of the effects of heavy Asian dust on respiratory function by definition type. Genes Environ. 2017, 39, 25–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United Nations General Assembly. Transforming Our World: The 2030 Agenda for Sustainable Development. Resolution Adopted by the General Assembly on 25 September 2015. Available online: https://www.un.org/ga/search/view_doc.asp?symbol=A/RES/70/1&Lang=E (accessed on 10 September 2020).
- Isara, A.R.; Adam, V.Y.; Aigbokhaode, A.Q.; Alenoghena, I.O. Respiratory symptoms and ventilatory functions among quarry workers in Edo state, Nigeria. Pan Afr. Med. J. 2016, 23, 212–221. [Google Scholar] [CrossRef]
- Nwibo, A.N.; Ugwuia, E.I.; Nwambeke, N.O.; Emelumadu, O.F.; Ogbonnaya, L.U. Pulmonary problems among quarry workers of stone crushing industrial site at Umuoghara, Ebony State, Nigeria. Int. J. Occup. Environ. Med. 2012, 3, 178–185. [Google Scholar]
- Perry-Castaneda Library (University of Texas). Map of Democratic Republic of Congo. Available online: https://legacy.lib.utexas.edu/maps/algeria.html (accessed on 8 August 2020).
- Leon-Kabamba, N.; Ngatu, N.R.; Kakoma, S.J.B.; Nyembo, C.; Mbelambela, E.P.; Moribe, R.J.; Wembonyama, S.; Danuser, B.; Oscar-Luboya, N. Respiratory health of dust-exposed Congolese coltan miners. Int. Arch. Occup. Environ. Health 2018, 91, 859–864. [Google Scholar] [CrossRef]
- American Conference of Governmental Industrial Hygienists. Threshold Limits Values for Chemical Substances and Physical Agents in the Work Environment and Biological Exposure Indices. Cincinnati: Conference. 2009. Available online: https://www.acgih.org/ (accessed on 4 August 2020).
- Hentschel, T.; Hruschka, F.; Priester, M. Global Report on Artisanal and Small-Scale Mining. Mining Minerals and Sustainable Development. 2002. Available online: http://www.ddiglobal.org/login/resources/g00723.pdf (accessed on 30 August 2020).
- Yingratanasuk, T.; Seixas, N.; Barnhart, S.; Brodkin, D. Respiratory health and silica exposure of stone carvers in Thailand. Int. J. Occup. Environ. Health 2002, 8, 301–308. [Google Scholar] [CrossRef]
- Ghotkar, V.B.; Maldhure, B.R.; Zodpey, S.P. Involvement of lung and lung function tests in stone quarry workers. Ind. J. Tuberc. 1995, 42, 155–160. [Google Scholar]
- Ashrafi-Asgarabad, A.; Samareh-Fekri, M.; Khanjani, N.; Ghotbi Ravandi, M.R. Exposure to particles and respiratory symptoms in stone carvers of Kerman, Iran. J. Occup. Health Epidemiol. 2016, 2, 146–156. [Google Scholar] [CrossRef]
- Yadav, S.P.; Anand, P.K.; Singh, H. Awareness and Practices about Silicosis among the Sandstone Quarry Workers in Desert Ecology of Jodhpur, Rajasthan, India. J. Hum. Ecol. 2011, 33, 191–196. [Google Scholar] [CrossRef]
- Richard, E.E.; Chinyere, N.A.A.; Jeremaiah, O.S.; Opara, U.C.A.; Henrieta, E.M.; Ifunanya, E.D. Cement dust exposure and perturbations in some elements and lung and liver functions and cement factory workers. J. Toxicol. 2016, 2016, 6104719–6104726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fatusi, A.; Erbabor, G. Occupational health status of sawmill workers in Nigeria. Int. J. Phys. Sci. 2007, 2, 33–38. [Google Scholar] [CrossRef]
- Olusegun, O.; Adeniyi, A.; Adeola, G.T. Impact of granite quarrying on the health of workers and nearby residents in Abeokuta Ogun State, Nigeria. Ethiop. J. Environ. Stud. Manag. 2009, 2, 1–11. [Google Scholar] [CrossRef]
- Guo, C.; Zhang, Z.; Lau, A.K.H.; Lin, C.Q.; Chuang, Y.C.; Chan, J.; Jiang, W.K.; Tam, T.; Yeoh, E.K.; Chan, T.C.; et al. Effect of long-term exposure to fine particulate matter on lung function decline and risk of chronic obstructive pulmonary disease in Taiwan: A longitudinal cohort study. Lancet Planet Health 2018, 2, e114–e125. [Google Scholar] [CrossRef]
- Wen, C.P.; Gao, W. PM2.5: An important cause for chronic obstructive pulmonary disease. Lancet Planet Health 2018, 2, e105–e106. [Google Scholar] [CrossRef]
- Paulin, L.; Hansel, N. Particulate air pollution and impaired lung function. F1000Research 2016, 5, 1–9. [Google Scholar] [CrossRef]
- World Health Organization. Air Quality Guidelines. Global update 2005. Particulate Matter, Ozone, Nitrogen Dioxide and Sulfur Dioxide. Available online: https://www.euro.who.int/en/health-topics/environment-and-health/air-quality/publications/pre2009 (accessed on 2 September 2020).
- Shaikh, S.; Nafees, A.A.; Khetpal, V.; Jamali, A.A.; Arain, A.M.; Yousuf, A. Respiratory symptoms and illnesses among brick kiln workers: A cross-sectional study from rural districts of Pakistan. BMC Public Health 2012, 12, 999. [Google Scholar] [CrossRef] [Green Version]
- Peterman, A.; Palemo, T.; Bredenkamp, C. Estimates and determinants of sexual violence against women in the Democratic Republic of Congo. Am. J. Public Health 2011, 101, 1060–1067. [Google Scholar] [CrossRef]
- Kohli, A.; Makambo, M.T.; Ramazani, P.; Zahiga, I.; Mbika, B.; Safari, O.; Bachunguye, R.; Mirindi, J.; Glassm, N. A Congolese community-based health program for survivors of sexual violence. Confl. Health 2002, 6, 6–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Sociodemographic and Clinical Characteristics | Exposed Female Quarry Workers (N = 256) | Controls (n = 256) | p-Value |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| Age (years) | 43.26 ± 10.82 | 44.07 ± 9.41 | 0.38 |
| Working years | 2.92 ± 4.55 | 8.35 ± 7.06 | <0.001 |
| Daily work duration (hours) | 12 ± 0.00 | 9.41 ± 1.43 | <0.001 |
| n (%) | n (%) | ||
| Education, primary/secondary | 245 (95.7) | 197 (76.9) | <0.01 |
| High school or higher | 11 (4.3) | 59 (23.1) | |
| Smoking status, Yes | 2 (0.8) | 9 (3.5) | 0.033 |
| No | 254 (96.2) | 247 (96.5) | |
| Alcohol intake, Yes | 37 (14.5) | 31 (12.1) | 0.435 |
| No | 219 (85.5) | 225 (87.9) | |
| Lung auscultation, Abnormal | 83 (32.4) | 09 (3.5) | <0.01 |
| Normal | 173 (67.6) | 247 (96.5) |
| Respiratory Complaints/Disorders | Female Quarry Workers N = 256 (%) | Controls N = 256 (%) | p-Value |
|---|---|---|---|
| Wheezing | 69 (27) | 17 (9.1) | <0.001 |
| Wheezing/effort | 57 (22.3) | 17 (9.1) | <0.001 |
| Night cough | 64 (25) | 23 (12.3) | 0.001 |
| Shortness of breath/rest | 80 (31.3) | 2 (1.1) | <0.001 |
| Shortness of breath/effort | 99 (38.7) | 1 (0.5) | <0.001 |
| Asthma | 6 (2.3) | 3 (1.6) | 0.43 |
| Morning cough | 132 (51.6) | 6 (3.2) | <0.001 |
| Morning phlegm | 105 (41) | 3 (1.6) | <0.001 |
| Chronic bronchitis | 45 (17.6) | 2 (1.1) | <0.001 |
| Rhinitis | 148 (57.8) | 25 (13.4) | <0.001 |
| Respiratory Manifestations | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| 95%CI | p-Value | aOR (SE) | 95%CI | p-Value | ||
| Wheezing at rest | 1.09 (0.26) | 0.67–1.76 | 0.714 | - | - | - |
| Wheezing after effort | 2.42 (0.61) | 1.47–3.98 | <0.001 | 3.36 (1.64) | 1.28–8.78 | 0.013 |
| Night cough | 0.42 (0.11) | 0.26–0.68 | <0.01 | 0.65 (0.23) | 0.32–1.31 | 0.234 |
| Morning cough | 7.72 (1.76) | 4.93–12.09 | <0.001 | 6.06 (1.88) | 3.29–11.15 | <0.001 |
| Morning phlegm | 5.89 (1.41) | 3.68–9.43 | <0.001 | 2.62 (0.99) | 1.24–5.52 | 0.011 |
| Breathlessness at rest | 8.49 (2.67) | 4.58–15.75 | <0.001 | 3.95 (1.15) | 2.22–7.02 | <0.001 |
| Breathlessness after effort | 6.09 (1.52) | 3.73–9.94 | <0.001 | 5.16 (1.95) | 2.46–10.84 | <0.001 |
| Asthma | 1.21 (0.73) | 0.36–3.99 | 0.761 | - | - | - |
| Chronic bronchitis | 2.66 (0.77) | 1.50–4.69 | 0.001 | 2.61 (0.75) | 1.48–4.61 | <0.001 |
| Rhinitis | 5.37 (1.07) | 3.63–7.96 | <0.001 | 2.13 (0.21) | 1.18–3.39 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leon-Kabamba, N.; Ngatu, N.R.; Muzembo, B.A.; Kakoma, S.; Michel-Kabamba, N.; Danuser, B.; Luboya, O.; Hirao, T. Air Quality in the Working Environment and Respiratory Health of Female Congolese Stone Quarry Workers. Trop. Med. Infect. Dis. 2020, 5, 171. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed5040171
Leon-Kabamba N, Ngatu NR, Muzembo BA, Kakoma S, Michel-Kabamba N, Danuser B, Luboya O, Hirao T. Air Quality in the Working Environment and Respiratory Health of Female Congolese Stone Quarry Workers. Tropical Medicine and Infectious Disease. 2020; 5(4):171. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed5040171
Chicago/Turabian StyleLeon-Kabamba, Ngombe, Nlandu Roger Ngatu, Basilua Andre Muzembo, Sakatolo Kakoma, Nzaji Michel-Kabamba, Brigitta Danuser, Oscar Luboya, and Tomohiro Hirao. 2020. "Air Quality in the Working Environment and Respiratory Health of Female Congolese Stone Quarry Workers" Tropical Medicine and Infectious Disease 5, no. 4: 171. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed5040171