The Cost of Lost Productivity Due to Premature Chagas Disease-Related Mortality: Lessons from Colombia (2010–2017)


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Estimation Methods
2.3. Sensitivity Analyses
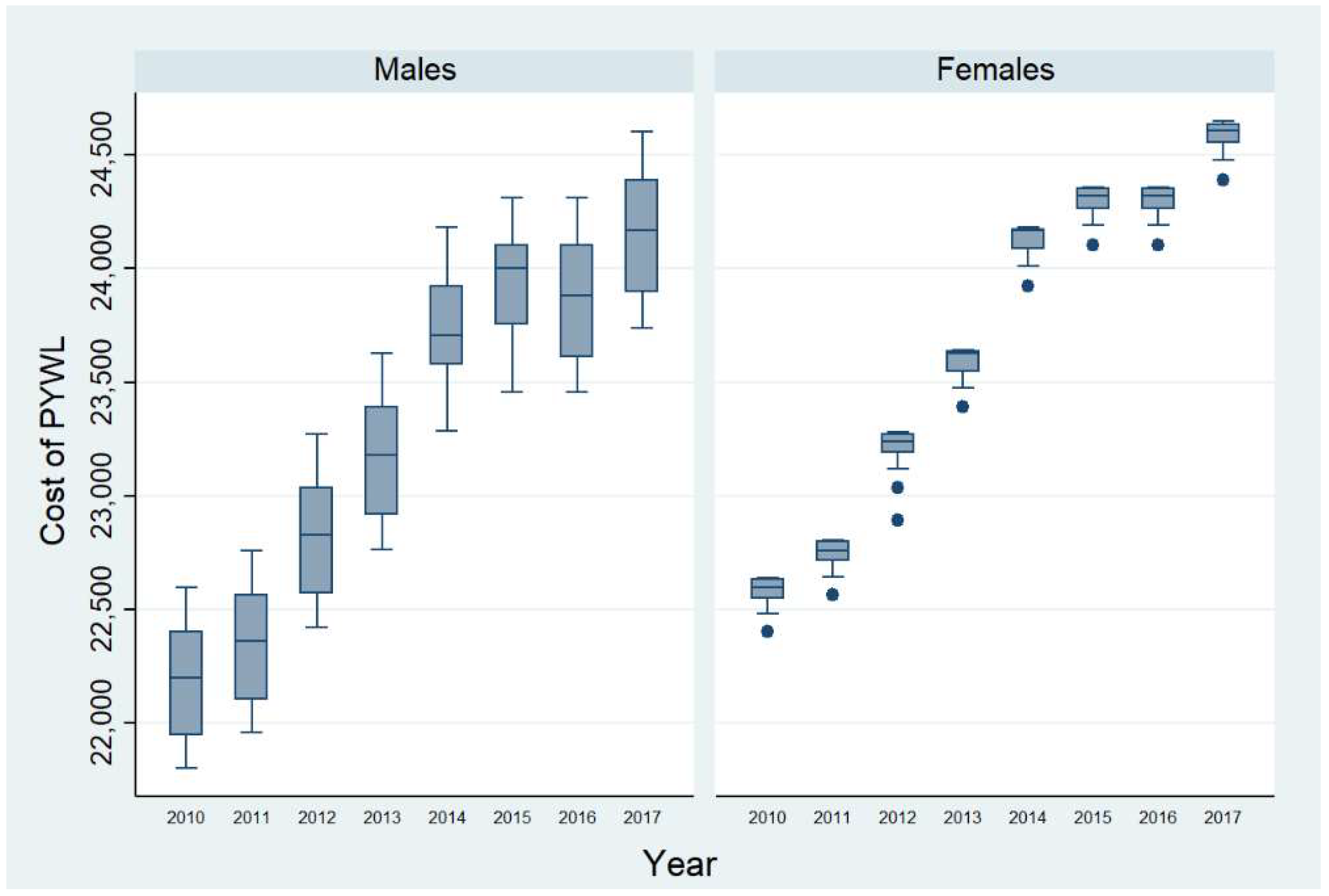
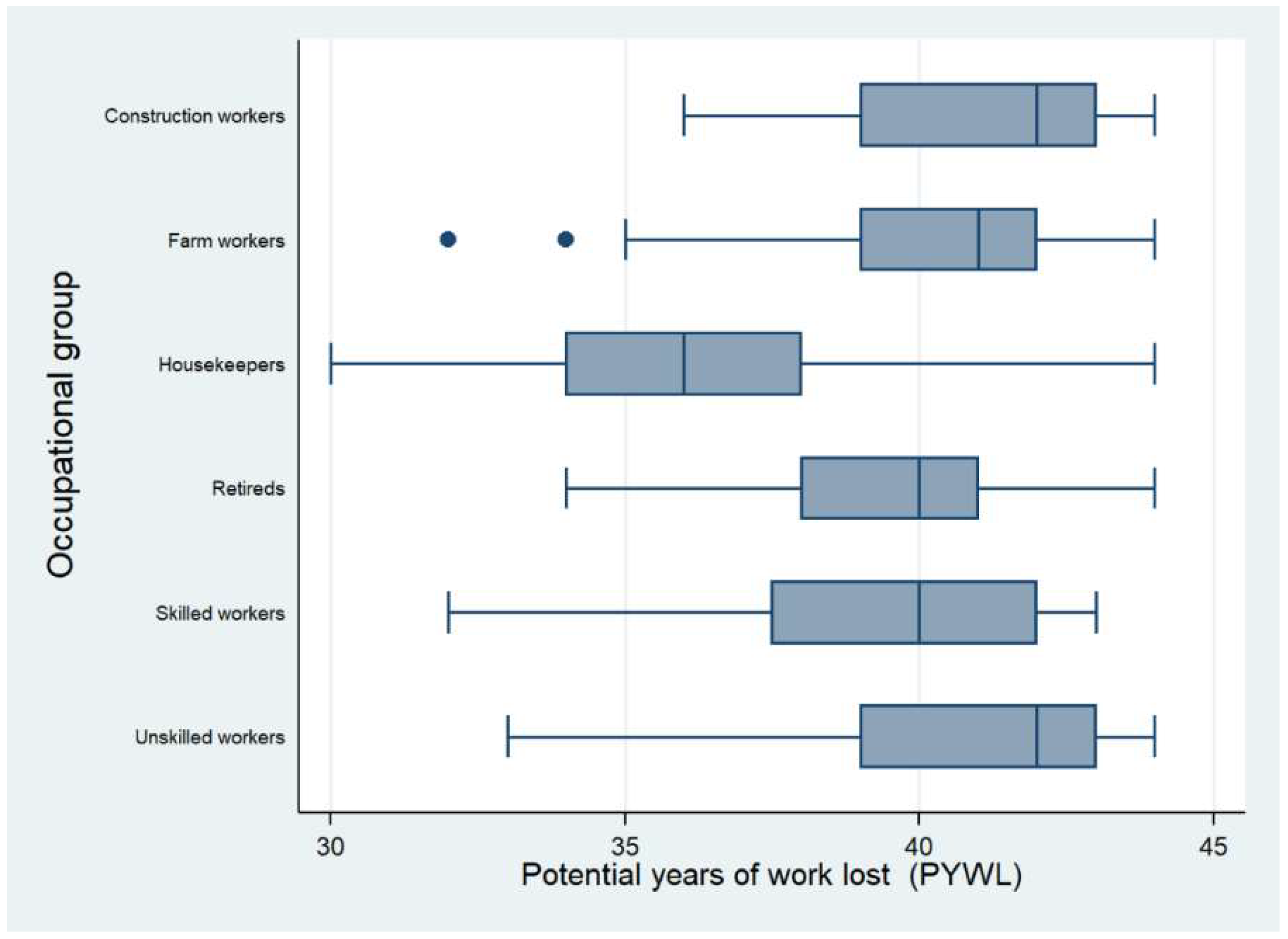
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Olivera, M.J.; Porras, J.; Toquica, C.; Rodríguez, J. Barriers to diagnosis dccess for Chagas disease in Colombia. J. Parasitol. Res. 2018, 2018, 4940796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinto Dias, J.C. Human Chagas disease and migration in the context of globalization: Some particular aspects. J. Trop. Med. 2013, 2013, 789758. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Chagas disease in Latin America: An epidemiological update based on 2010 estimates. Wkly. Epidemiol. Rec. 2015, 90, 33–44. [Google Scholar]
- Olivera, M.J.; Buitrago, G. Economic costs of Chagas disease in Colombia in 2017: A social perspective. Int. J. Infect. Dis. 2020, 91, 196–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. First WHO Report on Neglected Tropical Diseases: Working to Overcome the Global Impact of Neglected Tropical Diseases. France, 2010. Available online: https://www.who.int/neglected_diseases/2010report/en/ (accessed on 6 March 2020).
- Gardner, J.W.; Sanborn, J.S. Years of potential life lost (YPLL)-What does it measure? Epidemiology 1990, 1, 322–329. [Google Scholar] [CrossRef]
- Darbà, J.; Marsà, A. The cost of lost productivity due to premature lung cancer-related mortality: Results from Spain over a 10-year period. BMC Cancer 2019, 19, 992. [Google Scholar] [CrossRef]
- Cucunubá, Z.M.; Okuwoga, O.; Basáñez, M.G.; Nouvellet, P. Increased mortality attributed to Chagas disease: A systematic review and meta-analysis. Parasites Vectors 2016, 9, 42. [Google Scholar] [CrossRef] [Green Version]
- Wise, R.P.; Livengood, J.R.; Berkelman, R.L.; Goodman, R.A. Methodological alternatives for measuring premature mortality. Am. J. Prev. Med. 1988, 4, 268–273. [Google Scholar] [CrossRef]
- Romeder, J.M.; McWhinnie, J.R. Potential years of life lost between ages 1 and 70: An indicator of premature mortality for health planning. Int. J. Epidemiol. 1977, 6, 143–151. [Google Scholar] [CrossRef]
- Zhong, Y.; Li, D. Potential years of life lost and work tenure lost when silicosis is compared with other pneumoconioses. Scand. J. Work Environ. Health 1995, 21, 91–94. [Google Scholar]
- Olivera, M.J.; Fory, J.A.; Porras, J.F.; Buitrago, G. Prevalence of Chagas disease in Colombia: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0210156. [Google Scholar] [CrossRef] [PubMed]
- Banco de la República Colombia. Tasa Representativa del Mercado (TRM-Peso por dólar). Available online: https://www.banrep.gov.co/es/estadisticas/trm (accessed on 24 February 2020).
- Departamento Administrativo Nacional de Estadística. Mortalidad en Colombia, 2017. Available online: https://www.dane.gov.co/index.php/estadisticas-por-tema/demografia-y-poblacion/nacimientos-y-defunciones (accessed on 6 March 2020).
- Congreso de Colombia. Ley 100 de 1993. Por la Cual se Crea el Sistema de Seguridad Social Integral y se Dictan Otras Disposiciones. Available online: http://www.secretariasenado.gov.co/senado/basedoc/ley_0100_1993.html (accessed on 6 March 2020).
- Augustovski, F.; Alcaraz, A.; Caporale, J.; García Martí, S.; Pichon Riviere, A. Institutionalizing health technology assessment for priority setting and health policy in Latin America: From regional endeavors to national experiences. Expert Rev. Pharmacoecon. Outcomes Res. 2015, 15, 9–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Departamento Administrativo Nacional de Estadística. Encuesta Nacional de Calidad de vida 2018. 2019. Available online: https://www.dane.gov.co/index.php/estadisticas-por-tema/pobreza-y-condiciones-de-vida/calidad-de-vida-ecv (accessed on 6 March 2020).
- Olivera, M.J.; Cucunuba, Z.M.; Alvarez, C.A.; Nicholls, R.S. Safety profile of nifurtimox and treatment interruption for chronic Chagas disease in Colombian adults. Am. J. Trop. Med. Hyg. 2015, 93, 1224–1230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olivera, M.J.; Cucunuba, Z.M.; Valencia-Hernandez, C.A.; Herazo, R.; Agreda-Rudenko, D.; Florez, C.; Duque, S.; Nicholls, R.S. Risk factors for treatment interruption and severe adverse effects to benznidazole in adult patients with Chagas disease. PLoS ONE 2017, 12, e0185033. [Google Scholar] [CrossRef] [PubMed]
- Olivera, M.J.; Fory, J.A.; Olivera, A.J. Quality assessment of clinical practice guidelinesfor Chagas disease. Rev. Soc. Bras. Med. Trop. 2015, 48, 343–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olivera, M.J.; Fory, J.A.; Olivera, A.J. Therapeutic drug monitoring of benznidazole and nifurtimox: A systematic review and quality assessment of published clinical practice guidelines. Rev. Soc. Bras. Med. Trop. 2017, 50, 748–755. [Google Scholar] [CrossRef] [Green Version]
- Basquiera, A.L.; Sembaj, A.; Aguerri, A.M.; Omelianiuk, M.; Guzmán, S.; Moreno Barral, J.; Caeiro, T.F.; Madoery, R.J.; Salomone, O.A. Risk progression to chronic Chagas cardiomyopathy: Influence of male sex and of parasitaemia detected by polymerase chain reaction. Heart 2003, 89, 1186–1190. [Google Scholar] [CrossRef] [Green Version]
- Sabino, E.C.; Ribeiro, A.L.; Salemi, V.M.C.; Di Lorenzo Oliveira, C.; Antunes, A.P.; Menezes, M.M.; Lanni, B.M.; Nastari, L.; Fernandes, F.; Patavino, G.M.; et al. Ten-year incidence of Chagas cardiomyopathy among asymptomatic trypanosoma cruzi-seropositive former blood donors. Circulation 2013, 127, 1105–1115. [Google Scholar] [CrossRef] [Green Version]
- Pelegrino, V.M.; Dantas, R.A.S.; Ciol, M.A.; Clark, A.M.; Rossi, L.A.; Simoes, M.V. Health-related quality of life in Brazilian outpatients with Chagas and non-Chagas cardiomyopathy. Heart Lung 2011, 40, e25–e31. [Google Scholar] [CrossRef]
- Oliveira, B.G.; Abreu, M.N.S.; Abreu, C.D.G.; da Costa Rocha, M.O.; Ribeiro, A.L. Health-related quality of life in patients with Chagas disease. Rev. Soc. Bras. Med. Trop. 2011, 44, 150–156. [Google Scholar] [CrossRef] [Green Version]
- Olivera, M.J.; Chaverra, K.A. New diagnostic algorithm for Chagas disease: Impact on access to diagnosis and out-of-pocket expenditures in Colombia. Iran. J. Public Health 2019, 48, 1379–1381. [Google Scholar] [CrossRef] [PubMed]
- Drummond, M.; Sculpher, M.; Claxton, K.; Stoddart, G.; Torrance, G. Methods for the Economic Evaluation of Health Care Programmes, 4th ed.; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Pike, J.; Grosse, S.D. Friction cost estimates of productivity costs in cost-of-illness studies in comparison with human capital estimates: A review. Appl. Health Econ. Health Policy 2018, 16, 765–778. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Year | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | Total |
| Number of Deaths | |||||||||
| Males | 102 | 87 | 101 | 110 | 113 | 93 | 132 | 128 | 866 |
| Females | 58 | 51 | 59 | 71 | 79 | 85 | 92 | 85 | 580 |
| Total | 160 | 138 | 160 | 181 | 192 | 178 | 224 | 213 | 1446 |
| Deaths at Working Age | |||||||||
| Males | 84 | 69 | 88 | 95 | 93 | 83 | 117 | 112 | 741 |
| Females | 52 | 45 | 51 | 64 | 72 | 76 | 84 | 76 | 520 |
| Total | 136 | 114 | 139 | 159 | 165 | 159 | 201 | 188 | 1261 |
| PYWL | |||||||||
| Males | 3441 | 2822 | 3594 | 3900 | 3777 | 3348 | 4772 | 4583 | 30,237 |
| Females | 1854 | 1593 | 1824 | 2263 | 2521 | 2682 | 2968 | 2679 | 18,384 |
| Total | 5295 | 4415 | 5418 | 6163 | 6298 | 6030 | 7740 | 7262 | 48,621 |
| Total Premature Mortality Cost | % of the Total | Premature Mortality Cost per Death | Premature Mortality Cost per PYWL | |
|---|---|---|---|---|
| Males | 17,301,237 | 58 | 23,348 | 572 |
| Females | 12,382,676 | 42 | 23,813 | 674 |
| Total | 29,683,913 | 100 | 23,540 | 611 |
| Year | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 |
|---|---|---|---|---|---|---|---|---|
| Males | 1,862,873 | 1,541,799 | 2,008,175 | 2,198,782 | 2,206,153 | 1,986,068 | 2,793,321 | 2,704,067 |
| Females | 1,174,136 | 1,023,484 | 1,183,187 | 1,509,232 | 1,736,916 | 1,846,584 | 2,040,400 | 1,868,737 |
| Total | 3,037,009 | 2,565,283 | 3,191,362 | 3,708,014 | 3,943,069 | 3,832,652 | 4,833,722 | 4,572,803 |
| Age Group/Year | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 |
|---|---|---|---|---|---|---|---|---|
| Adults | 22,597 | 68,203 | 46,165 | 47,106 | 96,491 | 72,932 | 170,012 | 98,320 |
| Young | 3,014,412 | 2,497,081 | 3,145,197 | 3,660,908 | 3,846,578 | 3,759,719 | 4,663,710 | 4,474,483 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olivera, M.J.; Palencia-Sánchez, F.; Riaño-Casallas, M. The Cost of Lost Productivity Due to Premature Chagas Disease-Related Mortality: Lessons from Colombia (2010–2017). Trop. Med. Infect. Dis. 2021, 6, 17. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed6010017
Olivera MJ, Palencia-Sánchez F, Riaño-Casallas M. The Cost of Lost Productivity Due to Premature Chagas Disease-Related Mortality: Lessons from Colombia (2010–2017). Tropical Medicine and Infectious Disease. 2021; 6(1):17. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed6010017
Chicago/Turabian StyleOlivera, Mario J., Francisco Palencia-Sánchez, and Martha Riaño-Casallas. 2021. "The Cost of Lost Productivity Due to Premature Chagas Disease-Related Mortality: Lessons from Colombia (2010–2017)" Tropical Medicine and Infectious Disease 6, no. 1: 17. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed6010017