
Modeling the Cost-Effectiveness of Interventions to Prevent Plague in Madagascar


Abstract
:1. Introduction
2. Methods
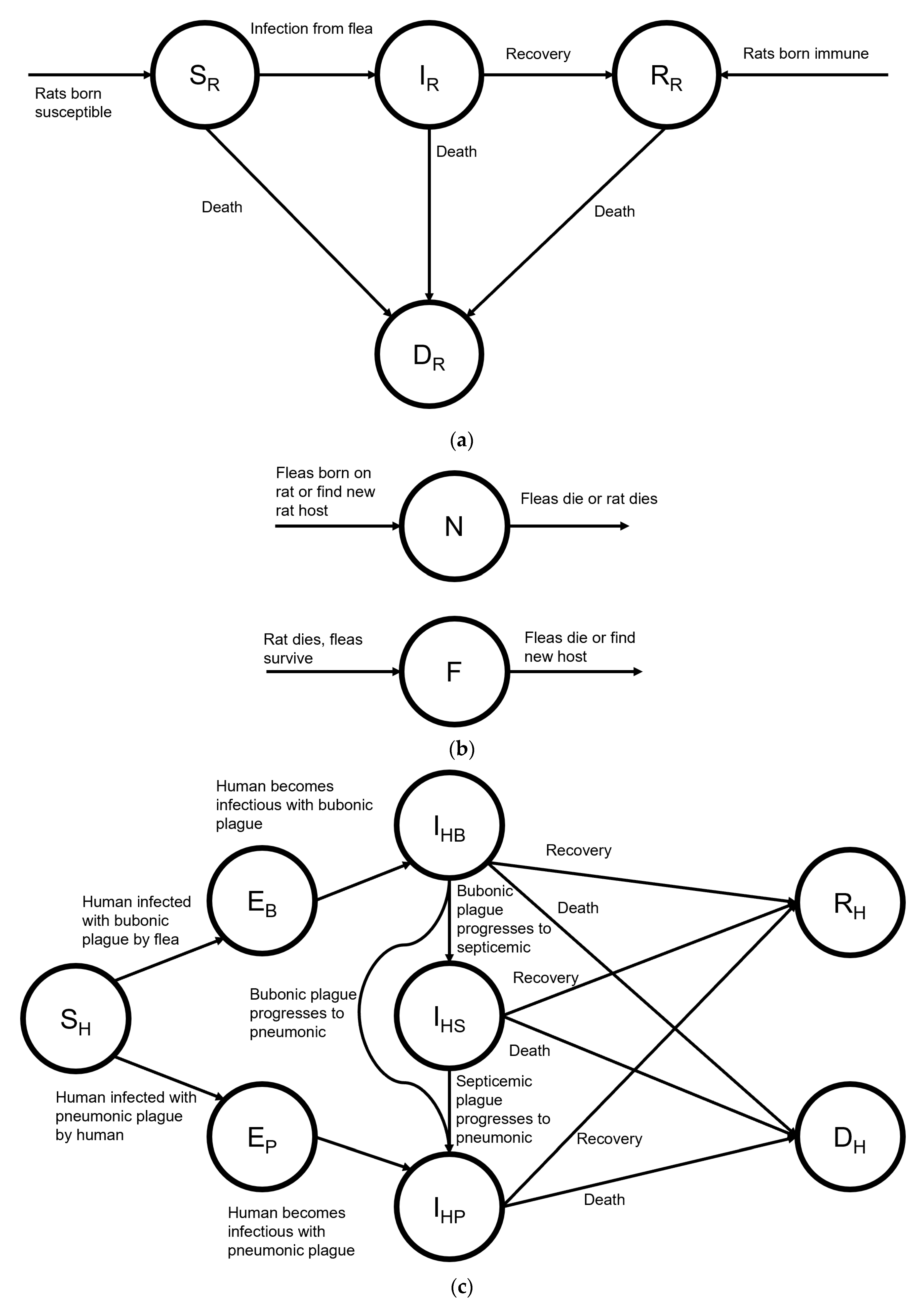
2.1. Model
2.2. Interventions
2.3. Sensitivity Analysis
2.4. Patient and Public Involvement
3. Results
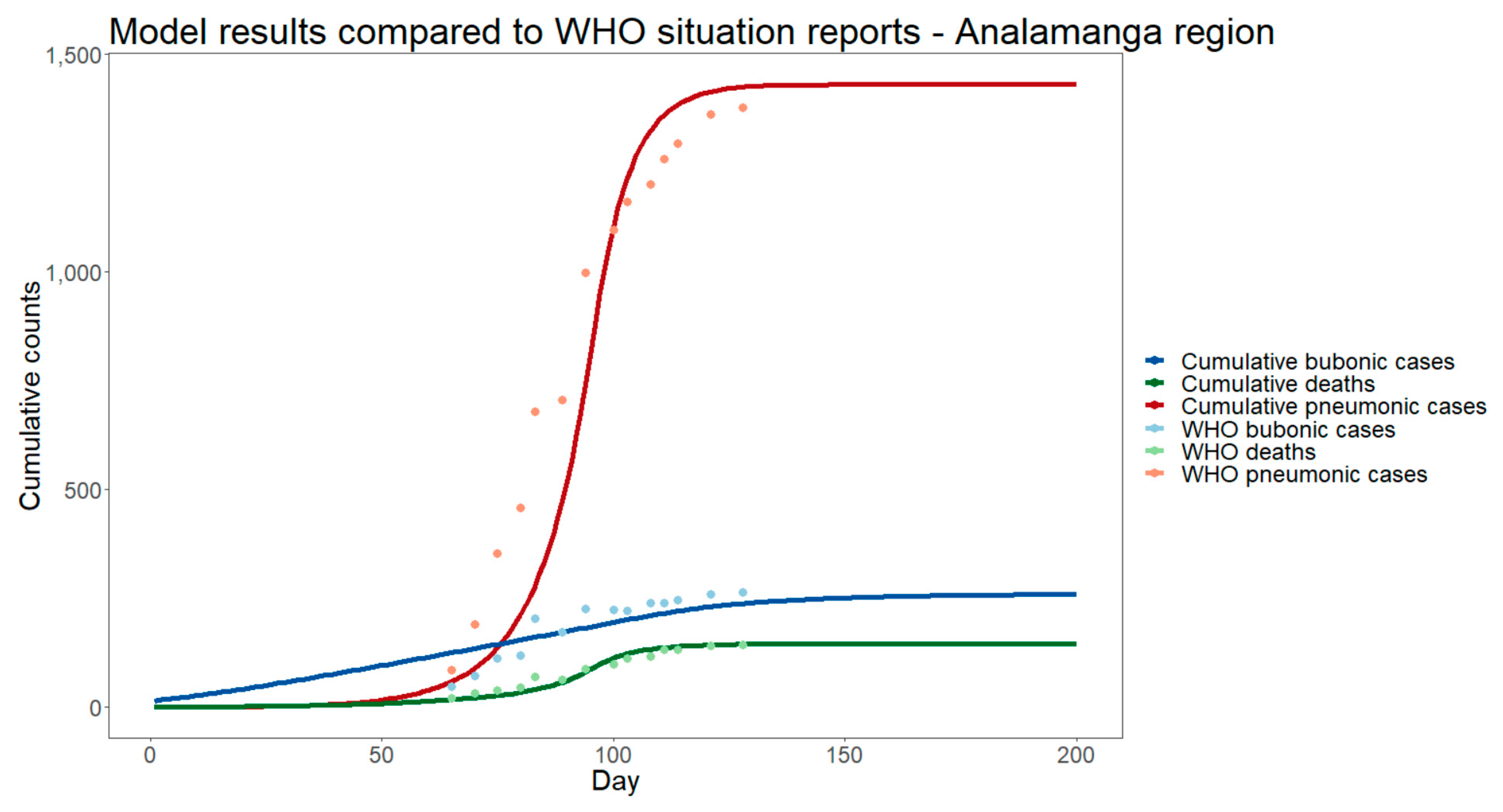
3.1. Base Case
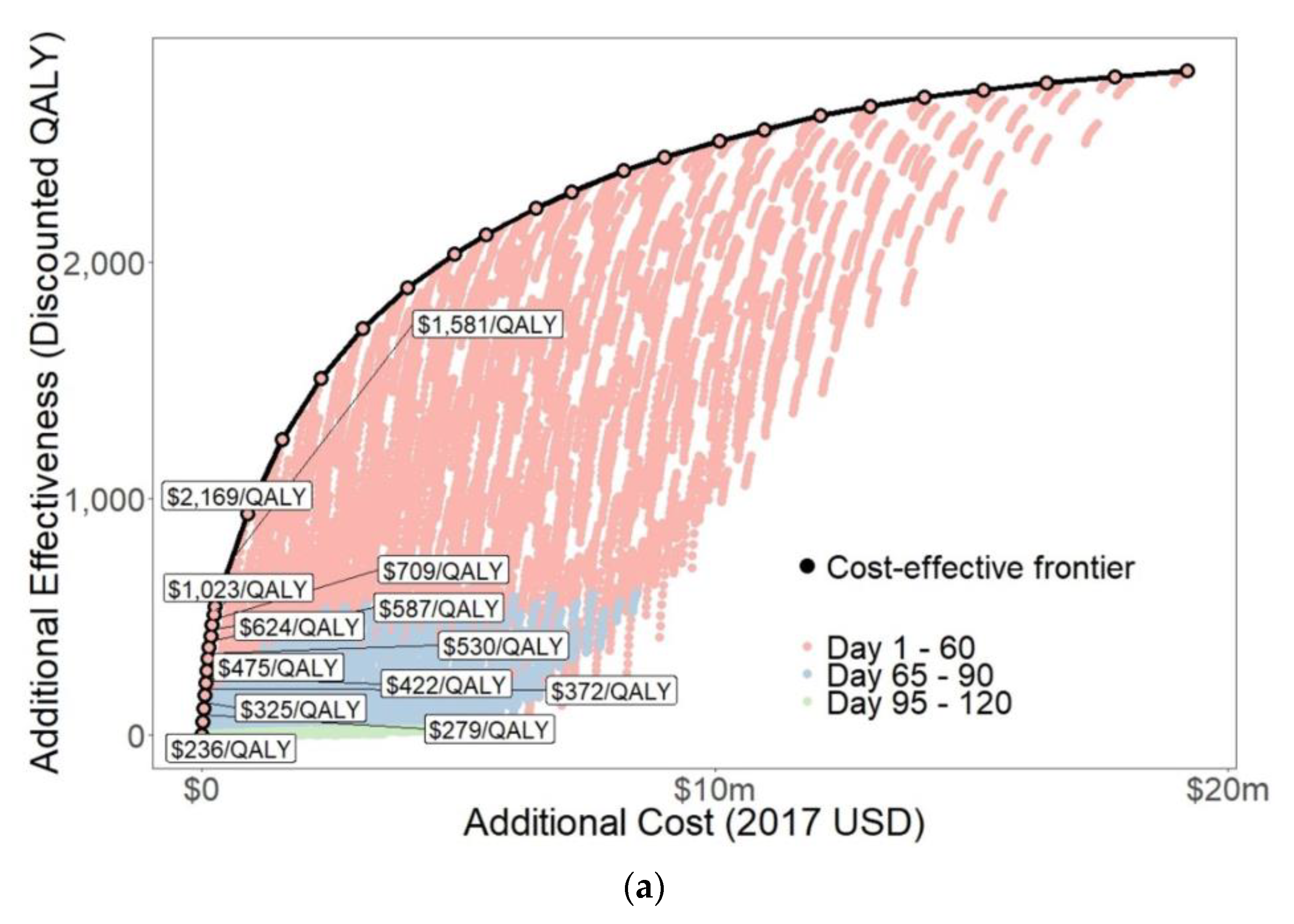
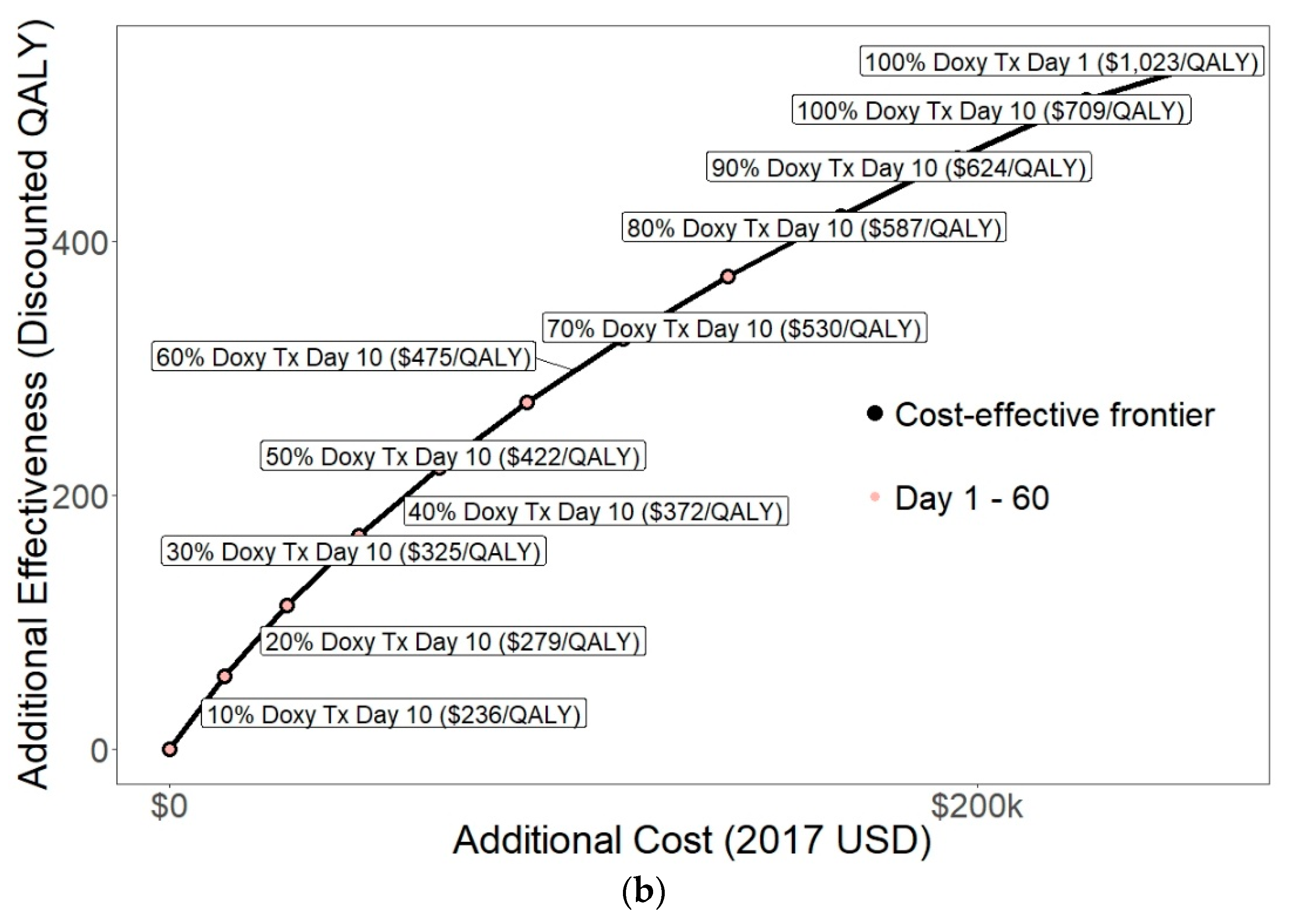
3.2. Sensitivity Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Recommended Antibiotic Treatment for Plague. Available online: https://www.cdc.gov/plague/resources/Recommended-antibiotics-for-plague_revision-Aug-2015_Final-(00000002).pdf (accessed on 20 June 2019).
- Hull, H.F.; Montes, J.M.; Mann, J.M. Septicemic plague in New Mexico. J. Infect. Dis. 1987, 155, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Riedel, S. Plague: From natural disease to bioterrorism. Bayl. Univ. Med. Cent. Proc. 2005, 18, 116–124. [Google Scholar] [CrossRef]
- World Health Organization. Plague Outbreak Madagascar, External Situation Report 14. Available online: https://www.afro.who.int/health-topics/plague/plague-outbreak-situation-reports (accessed on 20 June 2019).
- World Health Organization. Interregional meeting on prevention and control of plague. In Epidemic and Pandemic Alert and Response; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- World Health Organization. Pesticides and Their Application: For the Control of Vectors and Pests of Public Health Importance, 6th ed.; World Health Organization: Geneva, Switzerland, 2006; Available online: https://apps.who.int/iris/handle/10665/69223 (accessed on 20 June 2019).
- Brouillard, J.E.; Terriff, C.M.; Tofen, A.; Garrison, M.W. Antibiotic selection and resistance issues with fluoroquinolones and doxycycline against bioterrorism agents. Pharmacotherapy 2006, 26, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Inglesby, T.V.; Dennis, D.T.; Henderson, D.A.; Bartlett, J.G.; Ascher, M.S.; Eitzen, E.; Fine, A.D.; Friedlander, A.M.; Hauer, J.; Koerner, J.F.; et al. Plague as a biological weapon. JAMA 2000, 283, 2281–2290. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Prevention of plague: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 1996, 45, 1–15. [Google Scholar]
- World Health Organization. Plague Manual: Epidemiology, Distribution, Surveillance and Control. Available online: https://www.who.int/csr/resources/publications/plague/WHO_CDS_CSR_EDC_99_2_EN/en/ (accessed on 20 June 2019).
- Keeling, M.J.; Gilligan, C.A. Bubonic plague: A metapopulation model of a zoonosis. Proc. Biol. Sci. 2000, 267, 2219–2230. [Google Scholar] [CrossRef] [Green Version]
- Keeling, M.J.; Gilligan, C.A. Metapopulation dynamics of bubonic plague. Nature 2000, 407, 903–906. [Google Scholar] [CrossRef] [PubMed]
- Tsuzuki, S.; Lee, H.; Miura, F.; Chan, Y.H.; Jung, S.M.; Akhmetzhanov, A.R.; Nishiura, H. Dynamics of the pneumonic plague epidemic in Madagascar, August to October 2017. Eurosurveillance 2017, 22, 17-00710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, V.K.; Parra-Rojas, C.; Hernandez-Vargas, E.A. The 2017 plague outbreak in Madagascar: Data descriptions and epidemic modelling. Epidemics 2018, 25, 20–25. [Google Scholar] [CrossRef]
- Fowler, R.A.; Sanders, G.D.; Bravata, D.M.; Nouri, B.; Gastwirth, J.M.; Peterson, D.; Broker, A.G.; Garber, A.M.; Owens, D.K. Cost-effectiveness of defending against bioterrorism: A comparison of vaccination and antibiotic prophylaxis against anthrax. Ann. Intern. Med. 2005, 142, 601–610. [Google Scholar] [CrossRef]
- Rupnow, M.F.; Chang, A.H.; Shachter, R.D.; Owens, D.K.; Parsonnet, J. Cost-effectiveness of a potential prophylactic Helicobacter pylori vaccine in the United States. J. Infect. Dis. 2009, 200, 1311–1317. [Google Scholar] [CrossRef] [Green Version]
- Cuong, H.Q.; Vu, N.T.; Cazelles, B.; Boni, M.F.; Thai, K.T.; Rabaa, M.A.; Quang, L.C.; Simmons, C.P.; Huu, T.N.; Anders, K.L. Spatiotemporal dynamics of dengue epidemics, southern Vietnam. Emerg. Infect. Dis. 2013, 19, 945–953. [Google Scholar] [CrossRef] [PubMed]
- Teklehaimanot, H.D.; Schwartz, J.; Teklehaimanot, A.; Lipsitch, M. Weather-based prediction of Plasmodium falciparum malaria in epidemic-prone regions of Ethiopia II. Weather-based prediction systems perform comparably to early detection systems in identifying times for interventions. Malar. J. 2004, 3, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gani, R.; Leach, S. Epidemiological determinants for modeling pneumonic plague outbreaks. Emerg. Infect. Dis. 2004, 10, 608–614. [Google Scholar] [CrossRef] [PubMed]
- Buckle, A.P.; Smith, R.H. (Eds.) Rodent Pests and Their Control; CAB International: Wallingford, UK, 1994. [Google Scholar]
- Hirst, L.F. Plague. In British Encyclopedia of Medical Practice, Volume 9; Butterworth and Co.: Oxford, UK, 1938; pp. 675–698. [Google Scholar]
- Hinnebusch, B.J.; Gage, K.L.; Schwan, T.G. Estimation of vector infectivity rates for plague by means of a standard curve-based competitive polymerase chain reaction method to quantify Yersinia pestis in fleas. Am. J. Trop. Med. Hyg. 1998, 58, 562–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macchiavello, A. Reservoirs and vectors of plague. J. Trop. Med. Hyg. 1954, 57, 139–146. [Google Scholar]
- Wheeler, C.M.; Douglas, J.R. Sylvatic plague studies: V. The determination of vector efficiency. J. Infect. Dis. 1945, 77, 1–12. [Google Scholar] [CrossRef]
- Bacot, A.W. Observations on the length of time that fleas (Ceratophyllus fasciatus) carrying Bacillus pestis in the alimentary canals are able to survive in the absence of a host and retain the power to re-infect with the plague. J. Hyg. 1915, 14, 770–773. [Google Scholar]
- Central Intelligence Agency. The World Factbook: Madagascar. Available online: https://www.cia.gov/library/publications/the-world-factbook/geos/ma.html (accessed on 3 May 2019).
- New Mexico Department of Health. Mass Post Exposure Prophylaxis Protocol. Available online: https://nmhealth.org/publication/view/policy/2964/ (accessed on 20 June 2019).
- Oklahoma State Department of Health. Plague Prophylaxis (Bioterrorism). Available online: https://www.ok.gov/health2/documents/Plague%20Prophylaxis.pdf (accessed on 20 June 2019).
- Narayanan, N.; Lacy, C.R.; Cruz, J.E.; Nahass, M.; Karp, J.; Barone, J.A.; Hermes-DeSantis, E.R. Disaster preparedness: Biological threats and treatment options. Pharmacotherapy 2018, 38, 217–234. [Google Scholar] [CrossRef]
- Mwengee, W.; Butler, T.; Mgema, S.; Mhina, G.; Almasi, Y.; Bradley, C.; Formanik, J.B.; Rochester, C.G. Treatment of plague with gentamicin or doxycycline in a randomized clinical trial in Tanzania. Clin. Infect. Dis. 2006, 42, 614–621. [Google Scholar] [CrossRef]
- Hinckley, A.F.; Biggerstaff, B.J.; Griffith, K.S.; Mead, P.S. Transmission dynamics of primary pneumonic plague in the USA. Epidemiol. Infect. 2012, 140, 554–560. [Google Scholar] [CrossRef] [Green Version]
- Miarinjara, A.; Vergain, J.; Kavaruganda, J.M.; Rajerison, M.; Boyer, S. Plague risk in vulnerable community: Assessment of Xenopsylla cheopis susceptibility to insecticides in Malagasy prisons. Infect. Dis. Poverty 2017, 6, 141. [Google Scholar] [CrossRef] [Green Version]
- Rajonhson, D.M.; Miarinjara, A.; Rahelinirina, S.; Rajerison, M.; Boyer, S. Effectiveness of fipronil as a systemic control agent against Xenopsylla cheopis (Siphonaptera: Pulicidae) in Madagascar. J. Med. Entomol. 2017, 54, 411–417. [Google Scholar] [CrossRef]
- Gold, M.R.; Siegel, J.E.; Russell, L.B.; Weinstein, M.C. Cost-Effectiveness in Health and Medicine, 1st ed.; Oxford University Press: Oxford, UK, 1996. [Google Scholar]
- Goldhaber-Fiebert, J.D.; Denny, L.A.; De Souza, M.; Kuhn, L.; Goldie, S.J. Program spending to increase adherence: South African cervical cancer screening. PLoS ONE 2009, 4, e5691. [Google Scholar] [CrossRef] [Green Version]
- Goldhaber-Fiebert, J.D.; Denny, L.E.; De Souza, M.; Wright, T.C.; Kuhn, L.; Goldie, S.J. The costs of reducing loss to follow-up in South African cervical cancer screening. Cost Eff. Resour. Alloc. 2005, 3, 11. [Google Scholar] [CrossRef] [Green Version]
- Votresalaire.org. Controle des Salaires [Wage Control]. Available online: https://votresalaire.org/madagascar/salaire/controle-des-salaires#/ (accessed on 20 June 2019).
- Lee, B.Y.; Brown, S.T.; Haidari, L.A.; Clark, S.; Abimbola, T.; Pallas, S.E.; Wallace, A.S.; Mitgang, E.A.; Leonard, J.; Bartsch, S.M.; et al. Economic value of vaccinating geographically hard-to-reach populations with measles vaccine: A modeling application in Kenya. Vaccine 2019, 37, 2377–2386. [Google Scholar] [CrossRef]
- World Health Organization. WHO-CHOICE Estimates of Cost for Inpatient and Outpatient Health Service Delivery. Available online: https://www.who.int/choice/cost-effectiveness/inputs/health_service/en/ (accessed on 28 October 2020).
- The World Bank. Madagascar. Available online: https://data.worldbank.org/country/madagascar (accessed on 3 May 2020).
- World Health Organization. Madagascar: WHO Statistical Profile. Available online: https://www.who.int/gho/countries/mdg/data/en/ (accessed on 28 October 2020).
- World Health Organization. Life Tables by Country: Madagascar. Available online: http://apps.who.int/gho/data/?theme=main&vid=60970 (accessed on 28 October 2020).
- Hollmann, M.; Garin, O.; Galante, M.; Ferrer, M.; Dominguez, A.; Alonso, J. Impact of influenza on health-related quality of life among confirmed (H1N1) 2009 patients. PLoS ONE 2013, 8, e60477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Sources and Prices of Selected Products for the Prevention, Diagnosis and Treatment of Malaria. Available online: https://apps.who.int/iris/handle/10665/43080 (accessed on 20 June 2019).
- United Nations. Household Size and Composition around the World 2017. Available online: https://www.un.org/en/development/desa/population/publications/pdf/ageing/household_size_and_composition_around_the_world_2017_data_booklet.pdf (accessed on 20 June 2019).
- Health Action International. Price and Availability for Doxycycline 100 mg cap/Table. Available online: http://www.haiweb.org/MedPriceDatabase/price_availability_medicine_main.php?MP_ID=0&MED_ID=1364 (accessed on 20 June 2019).
- Kolaczinski, J.H.; Robinson, E.; Finn, T.P. The cost of antibiotic mass drug administration for trachoma control in a remote area of South Sudan. PLoS Negl. Trop. Dis. 2011, 5, e1362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldman, A.S.; Guisinger, V.H.; Aikins, M.; Amarillo, M.L.; Belizario, V.Y.; Garshong, B.; Gyapong, J.; Kabali, C.; Kamal, H.A.; Kanjilal, S.; et al. National mass drug administration costs for lymphatic filariasis elimination. PLoS Negl. Trop. Dis. 2007, 1, e67. [Google Scholar] [CrossRef]
- Johns, B.; Baltussen, R.; Hutubessy, R. Programme costs in the economic evaluation of health interventions. Cost Eff. Resour. Alloc. 2003, 1, 1. [Google Scholar] [CrossRef] [PubMed]
- Woods, B.; Revill, P.; Sculpher, M.; Claxton, K. Country-level cost-effectiveness thresholds: Initial estimates and the need for further research. Value Health 2016, 19, 929–935. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Plague. Available online: https://www.who.int/news-room/fact-sheets/detail/plague (accessed on 20 June 2019).
- The World Bank. Congo, Democratic Republic. Available online: https://data.worldbank.org/country/congo-dem-rep (accessed on 20 June 2019).
- King, A.A.; Domenech de Celles, M.; Magpantay, F.M.; Rohani, P. Avoidable errors in the modelling of outbreaks of emerging pathogens, with special reference to Ebola. Proc. Biol. Sci. 2015, 282, 20150347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mead, P.S. Plague in Madagascar—A tragic opportunity for improving public health. N. Engl. J. Med. 2018, 378, 106–108. [Google Scholar] [CrossRef] [PubMed]
- Andrianaivoarimanana, V.; Piola, P.; Wagner, D.M.; Rakotomanana, F.; Maheriniaina, V.; Andrianalimanana, S.; Chanteau, S.; Rahalison, L.; Ratsitorahina, M.; Rajerison, M. Trends of human plague, Madagascar, 1998–2016. Emerg. Infect. Dis. 2019, 25, 220–228. [Google Scholar] [CrossRef] [Green Version]
- European Centre for Disease Prevention and Control. Factsheet about Plague. Available online: https://ecdc.europa.eu/en/plague/facts (accessed on 20 June 2019).
- New Mexico Department of Health Epidemiology and Response Division. Plague. Available online: https://nmhealth.org/publication/view/help/1009/ (accessed on 20 June 2019).
- Cabanel, N.; Bouchier, C.; Rajerison, M.; Carniel, E. Plasmid-mediated doxycycline resistance in a Yersinia pestis strain isolated from a rat. Int. J. Antimicrob. Agents 2018, 51, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Ranaivozanany, D.; Renaud, B.; Lucey, D. Containing pneumonic plague. BMJ 2020, 368, l7072. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Description | Value | Source |
|---|---|---|---|
| Initial Susceptible Population | Sum of populations in districts with plague | 13,731,412 people | [4] |
| Rat reproductive rate | 5 rats/day | [11,20] | |
| Rat carrying capacity | 2500 rats | [11] | |
| Probability of inherited resistance of rats | 0.975 | [11,21] | |
| Transmission rate of bubonic plague to rats | 4.7 contacts/(rat-day) | [11,22,23,24] | |
| α | Flea searching efficiency | 0.004 | [11] |
| (Infectious period of bubonic plague in rats)−1 | 0.05 people/day | [11] | |
| Death rate of rats | 0.2 rats/day | [11,20,25] | |
| Probability of recovery in rats | 0.02 | [11] | |
| Flea reproductive rate | 20 fleas/day | [11] | |
| Flea carrying capacity per rat | 6.57 fleas/rat | [11,21] | |
| Death rate of fleas | 10 fleas/day | [11,25] | |
| Flea searching efficiency | 0.004 | [11] | |
| (Latency period of bubonic plague)−1 | 0.25 people/day | [11] | |
| (Latency period of pneumonic plague)−1 | 0.23 people/day | [19] | |
| Progression rate: bubonic to septicemic plague | 0.001 people/day | Assumed | |
| Progression rate: bubonic to pneumonic plague | 0.001 people/day | Assumed | |
| Progression rate: septicemic to pneumonic plague | 0.001 people/day | Assumed | |
| (Infectious period of bubonic plague in humans)−1 | 0.04 people/day | [11] | |
| (Infectious period of septicemic plague)−1 | 0.07 people/day | Assumed | |
| (Infectious period of pneumonic plague)−1 | 0.4 people/day | [19] | |
| Probability of recovery from septicemic plague | 0.8 | [2,4,8] | |
| Transmission rate of bubonic plague to humans | Phase 1–3: 0.2 contacts/(person-day) | Calibrated | |
| Phase 4: 0 contacts/(person-day) | |||
| Transmission rate of pneumonic plague between humans at each phase (step) | Phase 1: 0.64 contacts/(person-day) | Calibrated | |
| Phase 2: 0.68 contacts/(person-day) | |||
| Phase 3: 0.10 contacts/(person-day) | |||
| Phase 4: 0 contacts/(person-day) | |||
| Probability of recovering from bubonic plague at each phase (step) | Phase 1: 0.90 | Calibrated | |
| Phase 2: 0.91 | |||
| Phase 3: 0.94 | |||
| Phase 4: 0.99 | |||
| Probability of recovering from pneumonic plague at each phase (step) | Phase 1: 0.81 | Calibrated | |
| Phase 2: 0.9 | |||
| Phase 3: 0.93 | |||
| Phase 4: 0.99 |
| Parameter Name/Description | Parameter Value | Source |
|---|---|---|
| Median age | 19.9 | [40] |
| Median life expectancy at birth | 66.6 | [40] |
| Quality-adjusted life expectancy | 55.0 | [41] |
| Mean life expectancy at age 20 | 50.6 | [42] |
| HRQoL during infection | 0.38 | [43] |
| Cost of inpatient hospitalization per patient per day | $9.17 | [39] |
| Mean daily salary for community health workers | $4.58 | [37] |
| Container of 50% malathion insecticide | $4.63 | [44] |
| Average household size | 4.7 | [45] |
| Price of generic doxycycline per daily dose | $0.014 | [46] |
| Overhead cost per individual receiving treatment | $0.32 | [47] |
| Overhead costs per individual receiving prophylaxis | ||
| Vehicles | $0.05 | [47] |
| Communication and IT equipment | $0.01 | [47] |
| Mass distribution equipment | $0.02 | [47] |
| Travel and transportation | $0.39 | [47] |
| Vehicle fuel and maintenance | $0.03 | [47] |
| Accommodation and sustenance | $0.13 | [47] |
| Mass distribution consumables and other charges | $0.08 | [47] |
| Communication | $0.01 | [47] |
| Personnel | $0.57 | [47] |
| Total | $1.61 | |
| Annual discount rate | 3% | [34] |
| Intervention Timing | Doxycycline Treatment Expanded Coverage | Doxycycline Prophylaxis Distribution Rate, People/Day (Final Coverage as % of Total Population) | Malathion Distribution Coverage | Total Cost | Total QALYs | Incremental Cost | Incremental QALYs | ICER (Cost/QALY Gained) |
|---|---|---|---|---|---|---|---|---|
| N/A | 0% | 0 (0%) | 0% | $0 | 0 | N/A | N/A | N/A |
| Day 10 | 10% | 0 (0%) | 0% | $13,620 | 57.7 | $13,620 | 57.7 | $236 |
| Day 10 | 20% | 0 (0%) | 0% | $29,290 | 113.9 | $15,670 | 56.2 | $279 |
| Day 10 | 30% | 0 (0%) | 0% | $47,000 | 168.4 | $17,710 | 54.5 | $325 |
| Day 10 | 40% | 0 (0%) | 0% | $66,750 | 221.5 | $19,750 | 53.1 | $372 |
| Day 10 | 50% | 0 (0%) | 0% | $88,550 | 273.1 | $21,800 | 51.6 | $422 |
| Day 10 | 60% | 0 (0%) | 0% | $112,400 | 323.3 | $23,840 | 50.2 | $475 |
| Day 10 | 70% | 0 (0%) | 0% | $138,300 | 372.1 | $25,880 | 48.8 | $530 |
| Day 10 | 80% | 0 (0%) | 0% | $166,200 | 419.7 | $27,920 | 47.6 | $587 |
| Day 10 | 90% | 0 (0%) | 0% | $195,000 | 465.9 | $28,850 | 46.2 | $624 |
| Day 10 | 100% | 0 (0%) | 0% | $227,000 | 511.0 | $31,950 | 45.1 | $709 |
| Day 1 | 100% | 0 (0%) | 0% | $259,400 | 542.7 | $32,380 | 31.7 | $1023 |
| Day 1 | 100% | 1000 (%) | 0% | $879,600 | 934.9 | $620,200 | 392.2 | $1581 |
| Day 1 | 100% | 2000 (%) | 0% | $1,567,000 | 1252 | $687,600 | 317.1 | $2169 |
| Day 1 | 100% | 3000 (%) | 0% | $2,318,000 | 1509 | $751,100 | 257.5 | $2917 |
| Day 1 | 100% | 4000 (%) | 0% | $3,129,000 | 1720 | $811,000 | 210.3 | $3857 |
| Day 1 | 100% | 5000 (%) | 0% | $3,997,000 | 1892 | $867,400 | 172.6 | $5027 |
| Day 1 | 100% | 6000 (%) | 0% | $4,917,000 | 2035 | $920,600 | 142.4 | $6465 |
| Day 1 | 100% | 6000 (%) | 10% | $5,529,000 | 2115 | $612,100 | 80.7 | $7584 |
| Day 1 | 100% | 7000 (%) | 10% | $6,500,000 | 2228 | $970,800 | 112.1 | $8658 |
| Day 1 | 100% | 7000 (%) | 20% | $7,201,000 | 2295 | $701,200 | 68.0 | $10,310 |
| Day 1 | 100% | 8000 (%) | 20% | $8,220,000 | 2384 | $1,018,00 | 88.7 | $11,470 |
| Day 1 | 100% | 8000 (%) | 30% | $9,010,000 | 2442 | $790,300 | 57.3 | $13,790 |
| Day 1 | 100% | 9000 (%) | 30% | $10,070,000 | 2512 | $1,063,000 | 70.6 | $15,060 |
| Day 1 | 100% | 9000 (%) | 40% | $10,950,000 | 2560 | $879,200 | 48.3 | $18,200 |
| Day 1 | 100% | 10,000 (%) | 40% | $12,060,000 | 2617 | $1,105,000 | 56.4 | $19,570 |
| Day 1 | 100% | 10,000 (%) | 50% | $13,020,000 | 2658 | $968,200 | 40.8 | $23,760 |
| Day 1 | 100% | 10,000 (%) | 60% | $14,080,000 | 2694 | $1,057,000 | 36.5 | $28,930 |
| Day 1 | 100% | 10,000 (%) | 70% | $15,230,000 | 2727 | $1,146,000 | 32.7 | $35,000 |
| Day 1 | 100% | 10,000 (%) | 80% | $16,460,000 | 2756 | $1,234,000 | 29.4 | $42,050 |
| Day 1 | 100% | 10,000 (%) | 90% | $17,780,000 | 2783 | $1,323,000 | 26.4 | $50,200 |
| Day 1 | 100% | 10,000 (%) | 100% | $19,200,000 | 2806 | $1,412,000 | 23.7 | $59,540 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malloy, G.S.P.; Brandeau, M.L.; Goldhaber-Fiebert, J.D. Modeling the Cost-Effectiveness of Interventions to Prevent Plague in Madagascar. Trop. Med. Infect. Dis. 2021, 6, 101. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed6020101
Malloy GSP, Brandeau ML, Goldhaber-Fiebert JD. Modeling the Cost-Effectiveness of Interventions to Prevent Plague in Madagascar. Tropical Medicine and Infectious Disease. 2021; 6(2):101. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed6020101
Chicago/Turabian StyleMalloy, Giovanni S. P., Margaret L. Brandeau, and Jeremy D. Goldhaber-Fiebert. 2021. "Modeling the Cost-Effectiveness of Interventions to Prevent Plague in Madagascar" Tropical Medicine and Infectious Disease 6, no. 2: 101. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed6020101