
Increasing Antimicrobial Resistance in Surgical Wards at Mulago National Referral Hospital, Uganda, from 2014 to 2018—Cause for Concern?

 ,
,  ,
,  , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.2.1. General Setting
2.2.2. Specific Setting
2.3. Variables and Data Acquisition
2.4. Data Collection
2.5. Microbiological Process of Phenotypic Resistance
2.6. Data Analysis
3. Results
3.1. Bacterial Isolates from the Samples
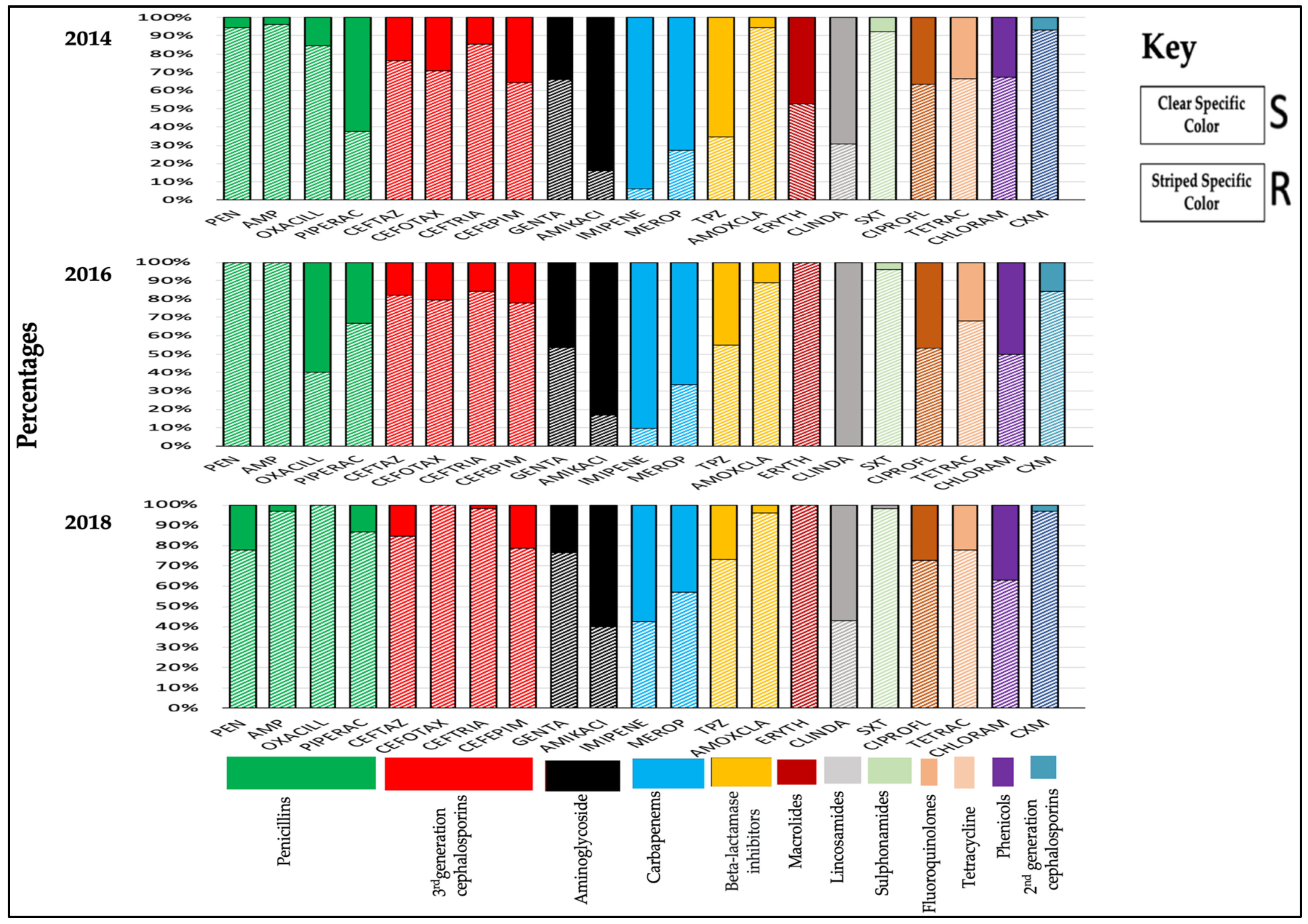
3.2. Antimicrobial Susceptibility Profiles of Bacterial Isolates during 2014, 2016, and 2018
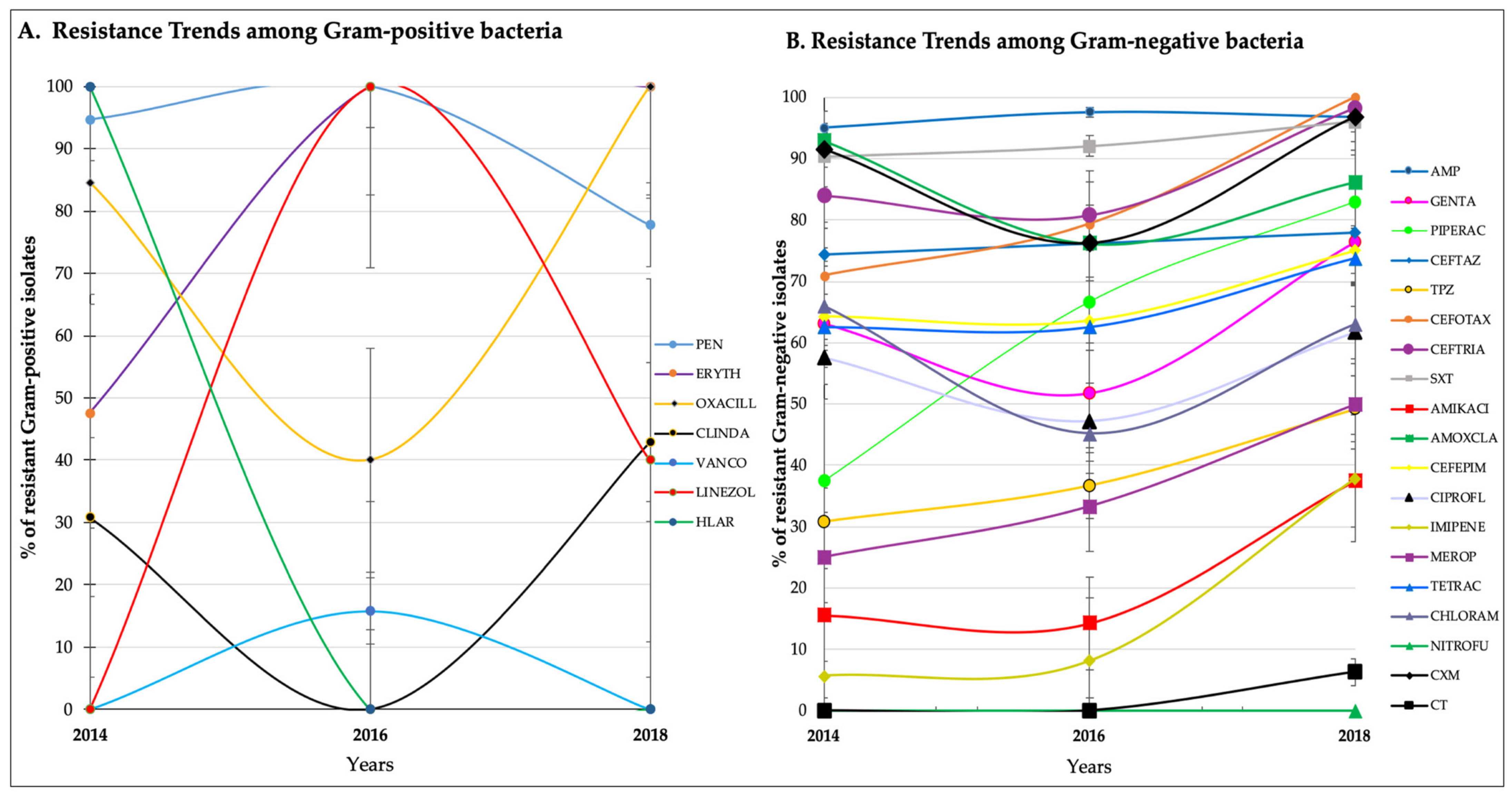
3.3. Antimicrobial Resistance Trends over the Years
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Open Access Statement and Disclaimer
References
- Irek, E.O.; Amupitan, A.A.; Obadare, T.O.; Aboderin, A.O. A systematic review of healthcare-associated infections in Africa: An antimicrobial resistance perspective. Afr. J. Lab. Med. 2018, 7, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sengupta, S.; Barman, P.; Lo, J. Opportunities to overcome implementation challenges of infection prevention and control in low-middle income countries. Curr. Treat. Options Infect. Dis. 2019, 11, 267–280. [Google Scholar] [CrossRef] [Green Version]
- WHO. Health-Care-Associated Infection in Africa: A Systematic Review; WHO World Health Organization: Geneva, Switzerland, 2011; Available online: https://www.who.int/bulletin/volumes/89/10/11-088179/en/ (accessed on 6 March 2021).
- Greco, D.; Magombe, I. Hospital acquired infections in a large north Ugandan hospital. J. Prev. Med. Hyg. 2011, 52, 55–58. [Google Scholar] [PubMed]
- Hope, D.; Ampaire, L.; Oyet, C.; Muwanguzi, E.; Twizerimana, H.; Apecu, R.O. Antimicrobial resistance in pathogenic aerobic bacteria causing surgical site infections in Mbarara regional referral hospital, Southwestern Uganda. Sci. Rep. 2019, 9, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Antimicrobial Resistance. Available online: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance (accessed on 28 February 2021).
- Ampaire, L.; Muhindo, A.; Orikiriza, P.; Mwanga-Amumpaire, J.; Bebell, L.; Boum, Y. A review of antimicrobial resistance in East Africa. Afr. J. Lab. Med. 2016, 5, 432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SSI-Surveillance-Protocol.pdf. Available online: https://www.who.int/infection-prevention/tools/surgical/SSI-surveillance-protocol.pdf?ua=1 (accessed on 28 February 2021).
- Dessie, W.; Mulugeta, G.; Fentaw, S.; Mihret, A.; Hassen, M.; Abebe, E. Pattern of bacterial pathogens and their susceptibility isolated from surgical site infections at selected referral hospitals, Addis Ababa, Ethiopia. Int. J. Microbiol. 2016, 2016, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seni, J.; Najjuka, C.F.; Kateete, D.P.; Makobore, P.; Joloba, M.L.; Kajumbula, H.; Kapesa, A.; Bwanga, F. Antimicrobial resistance in hospitalized surgical patients: A silently emerging public health concern in Uganda. BMC Res. Notes 2013, 6, 298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manyahi, J.; Matee, M.I.; Majigo, M.; Moyo, S.; Mshana, S.E.; Lyamuya, E.F. Predominance of multi-drug resistant bacterial pathogens causing surgical site infections in Muhimbili national hospital, Tanzania. BMC Res. Notes 2014, 7, 500. [Google Scholar] [CrossRef] [Green Version]
- Leaper, D.J.; Van Goor, H.; Reilly, J.; Petrosillo, N.; Geiss, H.K.; Torres, A.J.; Berger, A. Surgical site infection—A European perspective of incidence and economic burden. Int. Wound J. 2004, 1, 247–273. [Google Scholar] [CrossRef] [PubMed]
- GoU_AMR-NAP.pdf. Available online: https://cddep.org/wp-content/uploads/2018/12/GoU_AMR-NAP.pdf (accessed on 3 April 2021).
- World Health Organization. Antimicrobial Resistance: Global Report on Surveillance; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- GtR. Available online: https://gtr.ukri.org/projects?ref=MR%2FS004793%2F1 (accessed on 3 April 2021).
- The University of Edinburgh. Uganda Fleming Fellowships in AMR Surveillance at the University of Edinburgh. Available online: https://www.ed.ac.uk/edinburgh-infectious-diseases/news/news/uganda-fleming-fellowships-in-amr-surveillance (accessed on 3 April 2021).
- Uganda Population (2021)-Worldometer. Available online: https://www.worldometers.info/world-population/uganda-population/ (accessed on 1 March 2021).
- Micah, A.E.; Su, Y.; Bachmeier, S.D.; Chapin, A.; Cogswell, I.E.; Crosby, S.W.; Cunningham, B.; Harle, A.C.; Maddison, E.R.; Moitra, M.; et al. Health sector spending and spending on HIV/AIDS, tuberculosis, and malaria, and development assistance for health: Progress towards Sustainable Development Goal 3. Lancet 2020, 396, 693–724. [Google Scholar] [CrossRef]
- Uganda GDP per Capita|1982–2019 Data|2020–2021 Forecast|Historical|Chart. Available online: https://tradingeconomics.com/uganda/gdp-per-capita (accessed on 1 March 2021).
- Institute for Health Metrics and Evaluation. Uganda. 2015. Available online: http://www.healthdata.org/uganda (accessed on 1 March 2021).
- Albutt, K.; Punchak, M.; Kayima, P.; Namanya, D.B.; Shrime, M.G. Operative volume and surgical case distribution in Uganda’s public sector: A stratified randomized evaluation of nationwide surgical capacity. BMC Health Serv. Res. 2019, 19, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulago National Referral Hospital|EA Health. Available online: https://www.eahealth.org/directory/search/organisations/mulago-national-referral-hospital-0 (accessed on 27 February 2021).
- Performance standards for antimicrobial susceptibility testing. 30th edition. CLSI Suppl. M100 2020, 40, 1–332.
- Antibiotic Resistance in Uganda: Situation Analysis and Recommendations. Available online: https://www.cddep.org/wp-content/uploads/2017/06/uganda_antibiotic_resistance_situation_reportgarp_uganda_0-1.pdf (accessed on 1 March 2021).
- Yallew, W.W.; Takele, A.K.; Yehuala, F.M. Point prevalence of hospital-acquired infections in two teaching hospitals of Amhara region in Ethiopia. Drug Health Patient Saf. 2016, 8, 71–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kajumbula, H.; Fujita, A.W.; Meya, D.B.; Boulware, D.R.; Manabe, Y.C.; Mbabazi, O.; Najjuka, C.; Izale, C.; Akampurira, A.; Aisu, S.; et al. Antimicrobial drug resistance in blood culture isolates at a tertiary hospital, Uganda. Emerg. Infect. Dis. 2018, 24, 174–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wekesa, Y.N.; Namusoke, F.; Sekikubo, M.; Mango, D.W.; Bwanga, F. Ceftriaxone- and ceftazidime-resistant Klebsiella species, Escherichia coli, and methicillin-resistant Staphylococcus aureus dominate caesarean surgical site infections at Mulago Hospital, Kampala, Uganda. SAGE Open Med. 2020, 8. [Google Scholar] [CrossRef]
- Aruhomukama, D.; Najjuka, C.F.; Kajumbula, H.; Okee, M.; Mboowa, G.; Sserwadda, I.; Mayanja, R.; Joloba, M.L.; Kateete, D.P. blaVIM- and blaOXA-mediated carbapenem resistance among Acinetobacter baumannii and Pseudomonas aeruginosa isolates from the Mulago hospital intensive care unit in Kampala, Uganda. BMC Infect. Dis. 2019, 19, 853. [Google Scholar] [CrossRef] [PubMed]
- Kateete, D.P.; Nakanjako, R.; Okee, M.; Joloba, M.L.; Najjuka, C.F. Genotypic diversity among multidrug resistant Pseudomonas aeruginosa and Acinetobacter species at Mulago Hospital in Kampala, Uganda. BMC Res. Notes 2017, 10, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carroll, M.; Singer, D.; Ogbuagu, O.; Rangaiahagari, A.; Musabeyezu, E. Five-year antimicrobial susceptibility trends among bacterial isolates from a tertiary health-care facility in Kigali, Rwanda. Am. J. Trop. Med. Hyg. 2016, 95, 1277–1283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papp-Wallace, K.M.; Endimiani, A.; Taracila, M.A.; Bonomo, R.A. Carbapenems: Past, present, and future. Antimicrob. Agents Chemother. 2011, 55, 4943–4960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Field, N.; Cohen, T.; Charlett, A.; Egger, M.; Green, J.; Vineis, P.; Abubakar, I.; Struelens, M.J.; Palm, D.; Cookson, B.; et al. Strengthening the reporting of molecular epidemiology for infectious diseases (Strome-ID): An extension of the strobe statement. Lancet Infect. Dis. 2014, 14, 341–352. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Antibiotic Classes | Antibiotics (Abbreviation) |
|---|---|
| Penicillins | penicillin (PEN), ampicillin (AMP), piperacillin (PIPERAC), piperacillin-tazobactam (TPZ), oxacillin (OXACILL), amoxicillin-clavulanic acid (AMOXCLAV) |
| Third generation cephalosporins | cefotaxime (CEFOTAX), ceftriaxone (CEFTRIA), ceftazidime (CAZ) |
| Macrolides | erythromycin (ERYTH) |
| Second generation cephalosporins | cefuroxime (CXM) |
| Sulphonamides | trimethoprim-sulfamethoxazole (SXT) |
| Aminoglycoside | gentamicin (GENTA), amikacin (AMIKACI), high-level aminoglycoside (HLAR), |
| Tetracycline | tetracycline (TETRAC) |
| Phenicols | chloramphenicol (CHLORAM) |
| Fluoroquinolones | ciprofloxacin (CIPROFL) |
| Carbapenems | meropenem (MEROP), imipenem (IMIPENE) |
| Lincosamides | clindamycin (CLINDA) |
| Oxazolidinones | linezolid (LINEZOL) |
| Polymyxin E | colistin (CT) |
| Nitrofurans | nitrofurantoin (NITROFU) |
| Glycopeptide | vancomycin (VANCO) |
| Fourth-generation cephalosporin | cefepime (CEFEPIM) |
| Sample | Frequency (n = 428) | Percentage (%) |
|---|---|---|
| Tracheal aspirate | 156 | (36.5) |
| Pus swab | 120 | (28.0) |
| Blood | 88 | (20.6) |
| Urine | 22 | (5.1) |
| Pus aspirate | 20 | (4.7) |
| Catheter tip | 13 | (3.0) |
| High vaginal swab | 3 | (0.7) |
| Ear swab | 3 | (0.7) |
| Wound swab | 2 | (0.5) |
| Stool | 1 | (0.2) |
| Classification | Frequency (n = 428) | Percentage (%) | |
|---|---|---|---|
| Gram-negative Enterobacteriaceae (n = 216) | Klebsiella spp. | 93 | (21.7) |
| E. coli | 68 | (15.9) | |
| Proteus spp. | 19 | (4.4) | |
| Enterobacter spp. | 18 | (4.2) | |
| Citrobacter spp. | 11 | (2.6) | |
| Serratia marcescens | 4 | (0.9) | |
| Providencia spp. | 3 | (0.7) | |
| Gram-negative non-Enterobacteriaceae (n = 122) | Acinetobacter spp. | 75 | (17.5) |
| Pseudomonas spp. | 47 | (11.0) | |
| Gram-positive (n = 90) | Staphylococcus spp. | 53 | (12.4) |
| Enterococcus spp. | 26 | (6.1) | |
| Streptococcus spp. | 9 | (2.1) | |
| Corynebacteria | 2 | (0.5) | |
| Antibiotic/Years | 2014 n (%) | 2015 n (%) | 2016 n (%) | 2017 n (%) | 2018 n (%) | Chi2 Value for Trends | p-Value |
|---|---|---|---|---|---|---|---|
| Penicillin | 18 (94.7) | 16 (88.9) | 10 (100.0) | 7 (77.8) | 7 (77.8) | 2.13 | 0.144 |
| Erythromycin | 10 (47.6) | 13 (68.4) | 21 (100.0) | 8 (72.7) | 9 (100.0) | 9.94 | 0.002 |
| Oxacillin | 11 (84.6) | 6 (40.0) | 3 (60.0) | 2 (40.0) | 4 (100.0) | 0.03 | 0.871 |
| Clindamycin | 4 (30.8) | 2 (18.2) | 0 (0.0) | 1 (14.3) | 3 (42.9) | 0.01 | 0.938 |
| Linezolid | 0 (0.0) | 1 (50.0) | 3 (100) | 0 (0.0) | 2 (40.0) | 0.08 | 0.778 |
| HLAR | 2 (100.0) | 2 (100.0) | - | 2 (50.0) | 0 (0.0) | 3.56 | 0.059 |
| Antibiotic/Year | 2014 n (%) | 2015 n (%) | 2016 n (%) | 2017 n (%) | 2018 n (%) | Chi2 Value for Trends | p-Value |
|---|---|---|---|---|---|---|---|
| Ampicillin | 76 (95.0) | 34 (100.0) | 41 (97.6) | 44 (97.8) | 30 (96.8) | 0.27 | 0.603 |
| Gentamicin | 70 (63.1) | 19 (61.3) | 30 (51.7) | 42 (57.5) | 55 (76.4) | 0.72 | 0.397 |
| Piperacillin | 3 (37.5) | 7 (58.3) | 6 (66.7) | 16 (64.0) | 39 (83.0) | 9.58 | 0.002 |
| Cefotaxime | 58 (74.4) | 9 (42.9) | 32 (76.2) | 30 (75.0) | 39 (78.0) | 1.72 | 0.189 |
| Piperacillin-Tazobactam | 8 (30.8) | 7 (21.9) | 11 (36.7) | 19 (41.3) | 30 (49.2) | 14.83 | <0.001 |
| Cefotaxime | 22 (71.0) | 3 (33.3) | 27 (79.4) | 27 (93.1) | 7 (100) | 8.02 | 0.005 |
| Ceftriaxone | 58 (84.1) | 11 (61.1) | 21 (80.8) | 34 (89.5) | 53 (98.2) | 9.95 | 0.008 |
| Trimethoprim-sulfamethoxazole | 74 (90.2) | 35 (87.5) | 23 (92.0) | 39 (90.7) | 49 (96.1) | 1.34 | 0.245 |
| Amikacin | 6 (15.6) | 6 (15.6) | 4 (14.3) | 9 (20.9) | 18 (37.5) | 7.01 | 0.008 |
| Amoxicillin clavulanic acid | 52 (92.9) | 31 (93.9) | 16 (76.2) | 24 (80.0) | 25 (86.2) | 0.84 | 0.361 |
| Cefepime | 9 (64.3) | 4 (40.0) | 7 (63.6) | 24 (63.2) | 33 (75.0) | 2.25 | 0.134 |
| Ciprofloxacin | 38 (57.6) | 18 (42.9) | 17 (47.2) | 38 (58.5) | 37 (61.7) | 2.01 | 0.156 |
| Imipenem | 4 (5.7) | 1 (3.3) | 3 (8.1) | 14 (22.6) | 25 (37.9) | 32.29 | <0.001 |
| Meropenem | 3 (25.0) | 2 (100.0) | 1 (33.3) | 1 (14.3) | 4 (50.0) | 0.36 | 0.547 |
| Tetracycline | 10 (62.5) | 8 (47.1) | 15 (62.5) | 8 (44.4) | 14 (73.7) | 0.56 | 0.453 |
| Chloramphenicol | 31 (66.0) | 22 (50.0) | 19 (45.2) | 28 (59.6) | 17 (63.0) | 0.03 | 0.863 |
| Nitrofurantoin | 0 (0.0) | 0 (0.0) | - | 2 (22.2) | 0 (0.0) | 0.84 | 0.358 |
| Cefuroxime | 54 (91.5) | 15 (53.6) | 16 (76.2) | 33 (89.2) | 30 (96.8) | 1.87 | 0.171 |
| Colistin | - | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (6.25) | 0.49 | 0.483 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mboowa, G.; Aruhomukama, D.; Sserwadda, I.; Kitutu, F.E.; Davtyan, H.; Owiti, P.; Kamau, E.M.; Enbiale, W.; Reid, A.; Bulafu, D.; et al. Increasing Antimicrobial Resistance in Surgical Wards at Mulago National Referral Hospital, Uganda, from 2014 to 2018—Cause for Concern? Trop. Med. Infect. Dis. 2021, 6, 82. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed6020082
Mboowa G, Aruhomukama D, Sserwadda I, Kitutu FE, Davtyan H, Owiti P, Kamau EM, Enbiale W, Reid A, Bulafu D, et al. Increasing Antimicrobial Resistance in Surgical Wards at Mulago National Referral Hospital, Uganda, from 2014 to 2018—Cause for Concern? Tropical Medicine and Infectious Disease. 2021; 6(2):82. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed6020082
Chicago/Turabian StyleMboowa, Gerald, Dickson Aruhomukama, Ivan Sserwadda, Freddy Eric Kitutu, Hayk Davtyan, Philip Owiti, Edward Mberu Kamau, Wendemagegn Enbiale, Anthony Reid, Douglas Bulafu, and et al. 2021. "Increasing Antimicrobial Resistance in Surgical Wards at Mulago National Referral Hospital, Uganda, from 2014 to 2018—Cause for Concern?" Tropical Medicine and Infectious Disease 6, no. 2: 82. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed6020082