
Implementation of an Effective Decentralised Programme for Detection, Treatment and Prevention of Tuberculosis in Children


 ,
,
Abstract
:1. Background
2. Project Implementation
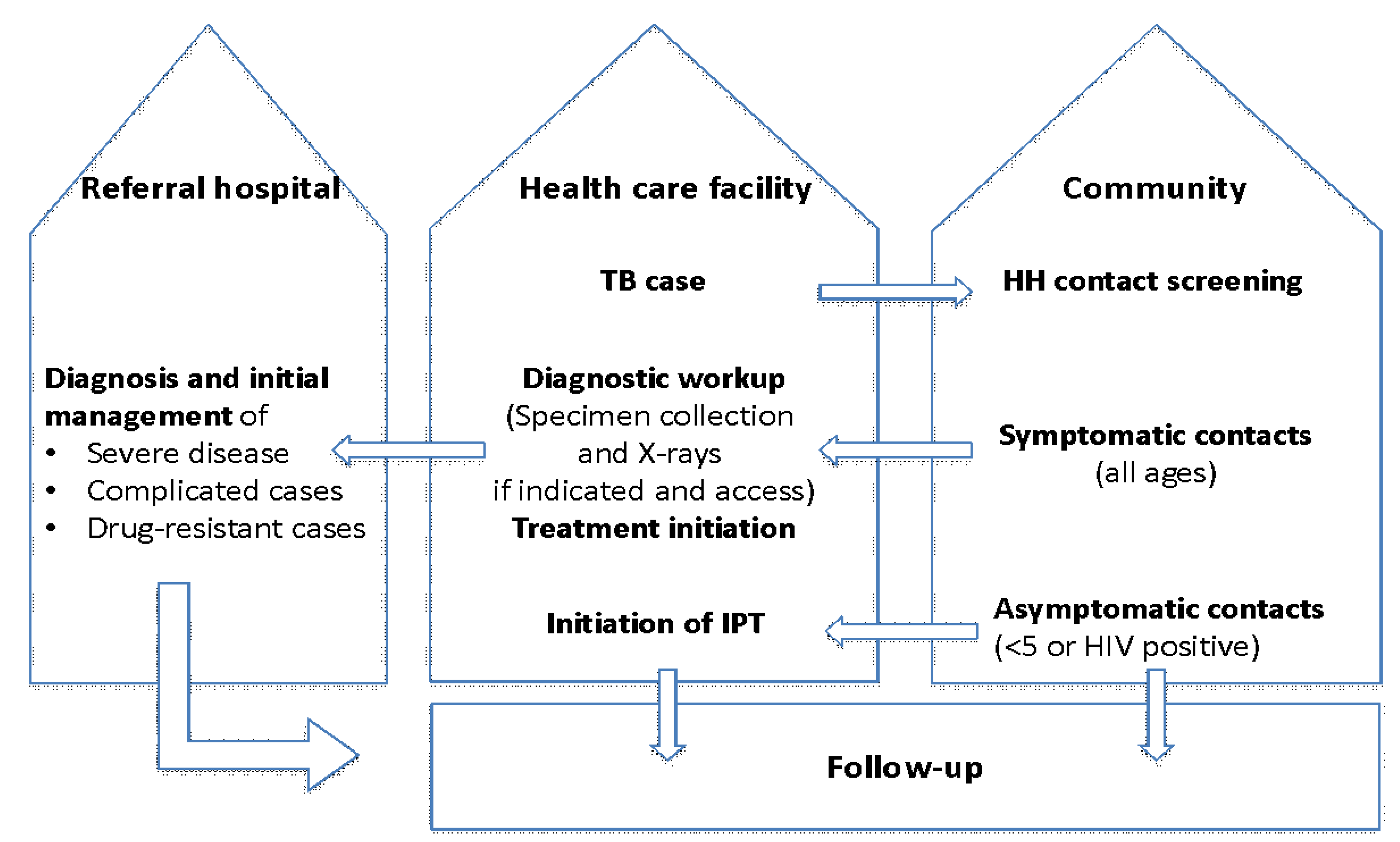
2.1. Project Design
2.2. Project Setting
2.3. Programmatic Engagement and Collaborative Partnership
2.4. Project Activities
- collecting baseline data for the project districts;
- conducting stakeholder engagement meetings at the national and district levels;
- training of facility and community teams;
- supporting and strengthening the health systems delivery; and
- reviewing and optimising performance management at all levels.
2.4.1. Baseline Survey
2.4.2. Stakeholder Engagement
2.4.3. Training of Healthcare Workers and Community Teams
- (a)
- Training materials developed
- (b)
- Training provided
- (c)
- Post-training follow-up support
2.4.4. Health Systems Strengthening Support
2.4.5. Optimising Performance Development
2.5. Project Data Management
2.6. Project Evaluations
3. Main Project Outcomes
- strengthening of child TB health service delivery capacity through:
- ○
- building confidence of healthcare workers to diagnose, manage and report TB, including TB in children, with continuous mentorship and supervision being vital for building capacity and capability;
- ○
- establishing and maintaining laboratory capacity for TB diagnosis in peripheral health facilities;
- ○
- consistent availability of anti-TB medicines, including formulations suitable for TPT for children; and
- ○
- training and linking community healthcare workers to primary care facilities and supporting them to integrate treatment support and education for the index case with household contact screening and management for case detection and prevention.
- Decentralisation of child TB services with strengthening of capacity for detection, treatment and prevention at peripheral health facilities through:
- ○
- training and support of healthcare workers, including use of the Union’s child TB tools such as the online child TB course, and in-service updates to improve and maintain clinical diagnosis;
- ○
- improved access to diagnostics to aid clinical diagnosis of TB among children, e.g., chest radiographs for children and strengthening of healthcare worker capacity to interpret them; and
- ○
- improved capacity for sample collection in children and laboratory diagnosis, including wider availability and use of GeneXpert.
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Global TB Report 2020; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Dodd, P.J.; Yuen, C.M.; Sismanidis, C.; Seddon, J.A.; Jenkins, H.E. The global burden of tuberculosis mortality in children: A mathematical modelling study. Lancet Glob. Health 2017, 5, e898–e906. [Google Scholar] [CrossRef] [Green Version]
- Graham, S.M.; Sismanidis, C.; Menzies, H.J.; Marais, B.J.; Detjen, A.K.; Black, R.E. Importance of tuberculosis control to address child survival. Lancet 2014, 383, 1605–1607. [Google Scholar] [CrossRef] [Green Version]
- Graham, S.M.; Sismanidis, C.; Menzies, H.J.; Marais, B.J.; Detjen, A.K.; Black, R.E. The risk of tuberculosis in children after close exposure: A systematic review and individual-participant meta-analysis. Lancet 2020, 395, 973–984. [Google Scholar]
- World Health Organization. Roadmap towards Ending TB in Children and Adolescents; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Graham, S.M.; Sekadde, M.P. Case detection and diagnosis of tuberculosis in primary-care settings. Paediatr. Int. Child Health 2019, 39, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Uganda Bureau of Statistics. National Population and Housing Census 2014; UBS: Kampala, Uganda, 2014.
- Jaganath, D.; Zalwango, S.; Okware, B.; Nsereko, M.; Kisingo, H.; Malone, L.; Lancioni, C.; Okwera, A.; Joloba, M.; Mayanja-Kizza, H.; et al. Contact investigation for active tuberculosis among child contacts in Uganda. Clin. Infect. Dis. 2013, 57, 1685–1692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, A. Tackling childhood tuberculosis in Uganda. Lancet Respir. Med. 2015, 3, 273. [Google Scholar] [CrossRef]
- International Union against Tuberculosis and Lung Disease. Desk-Guide for the Diagnosis and Management of TB in Children, 1st ed.; The Union: Paris, France, 2010. [Google Scholar]
- World Health Organization. Guidance for National Tuberculosis Programmes on the Management of Tuberculosis in Children, 2nd ed.; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- World Health Organization. Child TB Training Toolkit; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- International Union against Tuberculosis and Lung Disease. Childhood TB for Healthcare Workers: An Online Course; The Union: Paris, France, 2014. [Google Scholar]
- Zawedde-Muyanja, S.; Nakanwagi, A.; Dongo, J.P.; Sekadde, M.P.; Nyinoburyo, R.; Ssentongo, G.; Detjen, A.K.; Mugabe, F.; Nakawesi, J.; Karamagi, Y.; et al. Decentralisation of child tuberculosis services increases case finding and uptake of preventive therapy in Uganda. Int. J. Tuberc. Lung Dis. 2018, 11, 1314–1321. [Google Scholar] [CrossRef] [PubMed]
- DETECT Child TB Project. Report of an External Evaluation, November–December 2016; The Union: Kampala, Uganda, 2016. [Google Scholar]
- Ereso, B.M.; Yimer, S.A.; Gradmann, C.; Sagbakken, M. Barriers for tuberculosis case finding in Southwest Ethiopia: A qualitative study. PLoS ONE 2020, 15, e0226307. [Google Scholar] [CrossRef] [PubMed]
- Marahatta, S.B.; Yadav, R.K.; Giri, D.; Lama, S.; Rijal, K.R.; Mishra, S.R.; Shrestha, A.; Bhattrai, P.R.; Mahato, R.K.; Adhikari, B. Barriers in the access, diagnosis and treatment completion for tuberculosis patients in central and western Nepal: A qualitative study among patients, community members and health care workers. PLoS ONE 2020, 15, e0227293. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://hmis1.health.go.ug/hmis2/dhis-web-commons/security/login.action (accessed on 26 April 2021).
- Available online: https://theunion.org/our-work/tuberculosis/child-adolescent-tuberculosis/child-and-adolescent-tb-centre-of-excellence (accessed on 5 May 2021).
- Schwoebel, V.; Koura, K.G.; Adjobimey, M.; Gnanou, S.; Wandji, A.G.; Gody, J.C.; Delacourt, C.; Detjen, A.; Graham, S.M.; Masserey, E.; et al. Tuberculosis contact investigation and short-course preventive therapy among young children in four African countries. Int. J. Tuberc. Lung Dis. 2020, 24, 452–460. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Project Outcome | Data Analysis # | External Evaluation Findings |
|---|---|---|
| Decentralisation and Strengthening of Child TB Services | ||
| Proportion of all diagnosed child TB cases by health facility level * | Baseline: 96% at level V, 3% at level IV and 1% at level III By end implementation (Q4 2016): 50% at level V, 21% at level IV and 29% at level III | The DETECT model demonstrated that child TB services can be successfully decentralised with the greatest increase in detection occurring at the level III facility in both districts. |
| Health worker knowledge, Wakiso District | Average (range) test score Baseline: 40 (28–70)% Implementation: 75 (64–89)% | The ability and confidence of health workers in peripheral health facilities to diagnose TB in children was improved and the numbers of of unnecessary referrals were reduced. |
| Health worker knowledge, Kabarole District | Average (range) test score Baseline: 45 (32–64)% Implementation: 78 (68–96)% | |
| Number of functional TB basic management units for diagnosis and treatment by district | Baseline: 24 in Kabarole and 41 in Wakiso District By end implementation: 30 in Kabarole and 46 in Wakiso District | Repair of non-functional microscopes and re-training of laboratory personnel benefit TB services and detection for all ages. Improved laboratory and drug supplies with reduced stock-outs. |
| Changes to TB Case Detection and Treatment Outcomes | ||
| Caseload of child TB and as a proportion of total TB notifications | 139% increase in 0–14 years Baseline: 271, 8.8% Implementation: 647, 14.9% | The majority of respondents from the focus group discussions and in-depth interviews felt that the project had improved delivery of TB services, as it had accomplished the following:
|
| TB cases in young children, proportion of all child TB cases | Increase in <5 years ageBaseline: 99, 36.5% Implementation: 324, 50.1% | |
| Bacteriologically confirmed (BC) TB cases in children | 61% increase in BC cases detected, but proportion with BC remained low in children. Baseline: 44 (9 young) children 0–14 years: 44/171 = 16% BC <5 years: 9/99 = 9% BC Implementation: 71 (16 young) children 0–14 years: 71/647 = 11% BC <5 years: 16/324 = 5% BC | |
| Cases of TB in older adolescents and adults | 32% increase Baseline: 2805 Implementation: 3693 | |
| Treatment success, cure or treatment complete | Significant improvement Baseline: 65% Implementation: 81% | |
| Died or treatment failure | Reduction in poor outcomes: Baseline: 15% Implementation: 4% | |
| Household Child Contact Screening and Management ^ | ||
| Training and support of community health workers to implement | 178 (target was 168) community health workers received training | At least two per facility were trained over 2 days, provided with job aides and recording tools, linked with the facility-based TB focal person for ongoing mentorship and supervision. |
| Households screened | 1617 households with 2270 child contacts | The project increased screening of households of smear-positive TB patients by 142%. |
| Child contacts with positive symptom screen | 602 (27%) of 2270 child contacts were symptomatic | Screening symptoms used were cough, weight loss or poor weight gain, fever or lethargy/reduced playfulness. |
| Child contacts evaluated for TB disease | 486 (81%) of 602 symptomatic child contacts | 19% of symptomatic child contacts did not present to the health facility for further evaluation. |
| Child contacts diagnosed with TB | 55 child TB cases detected | Lower numbers than expected for overall case detection—2.4% of all child contacts. Of symptomatic child contacts who presented to the facility for evaluation, 11% diagnosed with TB. |
| Child contacts eligible for TPT | 910 young child contacts without active TB identified | Challenges with availability of isoniazid-alone preparation for TPT at beginning of project. |
| Eligible child contacts who initiated IPT | 670 or 77% of 910 eligible | Remarkable improvements in IPT uptake noted in both districts over time but lower than the 90% target. |
| Child contacts who completed IPT | 569 or 85% of 670 who commenced IPT | Although short of the 90% target, a high rate of completion. |
| Key Challenges and Responses |
|
| Lessons learnt |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dongo, J.P.; Graham, S.M.; Nsonga, J.; Wabwire-Mangen, F.; Maleche-Obimbo, E.; Mupere, E.; Nyinoburyo, R.; Nakawesi, J.; Sentongo, G.; Amuge, P.; et al. Implementation of an Effective Decentralised Programme for Detection, Treatment and Prevention of Tuberculosis in Children. Trop. Med. Infect. Dis. 2021, 6, 131. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed6030131
Dongo JP, Graham SM, Nsonga J, Wabwire-Mangen F, Maleche-Obimbo E, Mupere E, Nyinoburyo R, Nakawesi J, Sentongo G, Amuge P, et al. Implementation of an Effective Decentralised Programme for Detection, Treatment and Prevention of Tuberculosis in Children. Tropical Medicine and Infectious Disease. 2021; 6(3):131. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed6030131
Chicago/Turabian StyleDongo, John Paul, Stephen M. Graham, Joseph Nsonga, Fred Wabwire-Mangen, Elizabeth Maleche-Obimbo, Ezekiel Mupere, Rodrigo Nyinoburyo, Jane Nakawesi, Gerald Sentongo, Pauline Amuge, and et al. 2021. "Implementation of an Effective Decentralised Programme for Detection, Treatment and Prevention of Tuberculosis in Children" Tropical Medicine and Infectious Disease 6, no. 3: 131. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed6030131