
Newly Diagnosed Diabetes in Patients with COVID-19: Different Types and Short-Term Outcomes

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Methods
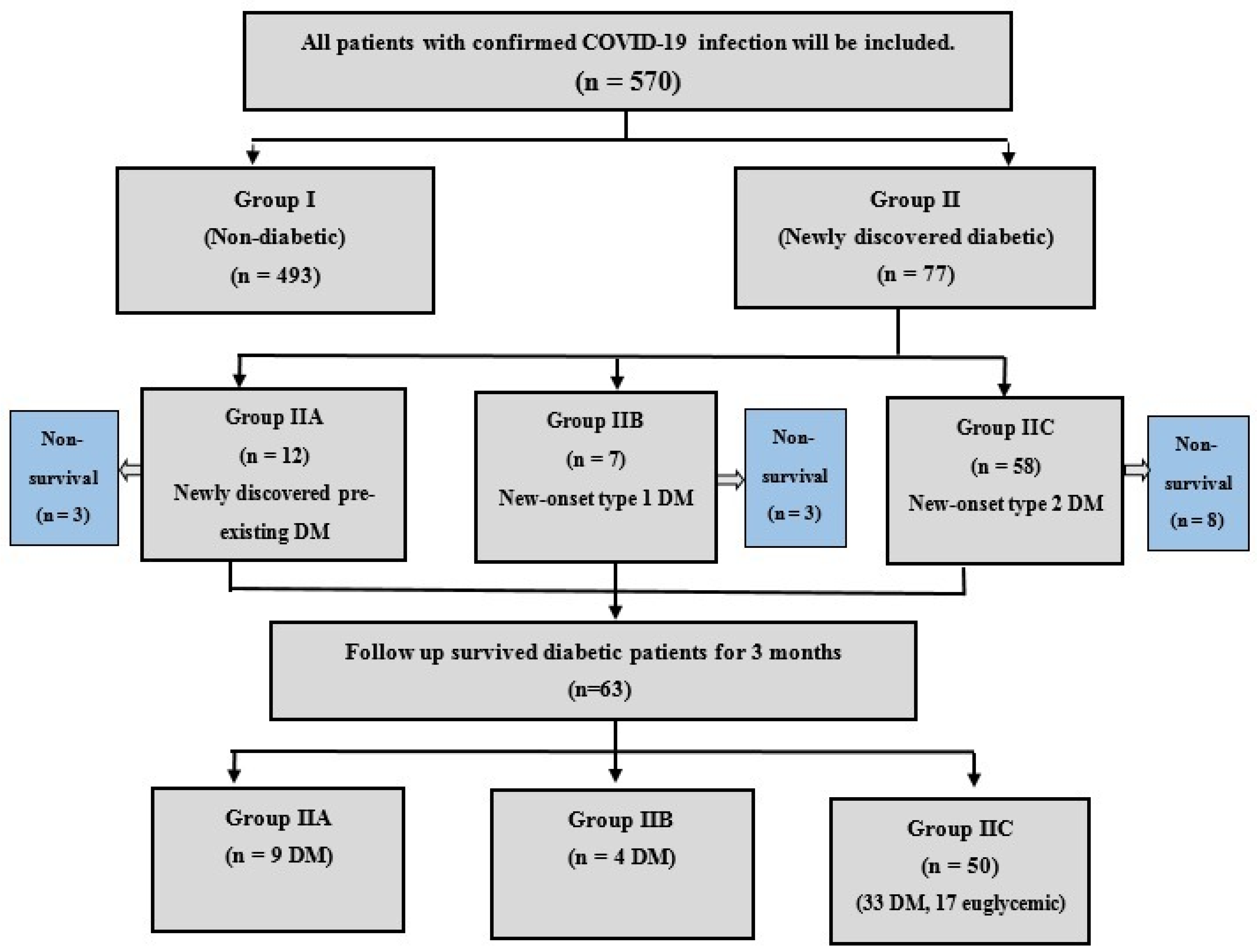
2.1. Study Population and Recruitment
2.2. Patient Assessment
2.3. Study Design and Setting
2.4. Statistical Analysis
3. Results
3.1. Cross-Sectional Phase
3.2. Follow-Up Phase (for DM)
3.3. Study Endpoint (Glycemic Control after 3 Months)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, Y.; Wang, Y.; Chen, Y.; Qin, Q. Unique epidemiological and clinical features of the emerging 2019 novel coronavirus pneumonia (COVID-19) implicate special control measures. J. Med. Virol. 2020, 92, 568–576. [Google Scholar] [CrossRef] [Green Version]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef] [Green Version]
- WHO. Coronavirus (COVID-19) Dashboard|WHO Coronavirus (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int/ (accessed on 7 July 2021).
- Pearson-Stuttard, J.; Blundell, S.; Harris, T.; Cook, D.G.; Critchley, J. Diabetes and infection: Assessing the association with glycaemic control in population-based studies. Lancet Diabetes Endocrinol. 2016, 4, 148–158. [Google Scholar] [CrossRef]
- Gentile, S.; Strollo, F.; Mambro, A.; Ceriello, A. COVID-19, ketoacidosis and new-onset diabetes: Are there possible cause and effect relationships among them? Diabetes Obes. Metab. 2020, 22, 2507–2508. [Google Scholar] [CrossRef]
- Apicella, M.; Campopiano, M.C.; Mantuano, M.; Mazoni, L.; Coppelli, A.; Del Prato, S. COVID-19 in people with diabetes: Understanding the reasons for worse outcomes. Lancet Diabetes Endocrinol. 2020, 8, 782–792. [Google Scholar] [CrossRef]
- Li, J.; Wang, X.; Chen, J.; Zuo, X.; Zhang, H.; Deng, A. COVID-19 infection may cause ketosis and ketoacidosis. Diabetes Obes. Metab. 2020, 22, 1935–1941. [Google Scholar] [CrossRef]
- Maddaloni, E.; Buzzetti, R. COVID-19 and diabetes mellitus: Unveiling the interaction of two pandemics. Diabetes/Metab. Res. Rev. 2020, 36, e3321. [Google Scholar] [CrossRef] [PubMed]
- Prete, M.; Favoino, E.; Catacchio, G.; Racanelli, V.; Perosa, F. SARS-CoV-2 inflammatory syndrome. Clinical features and rationale for immunological treatment. Int. J. Mol. Sci. 2020, 21, 3377. [Google Scholar] [CrossRef]
- COVID-19 Diagnosis and Treatment Guideline in China, 7th ed.; National Health Commission of the People’s Republic of China. Available online: http://www.nhc.gov.cn/yzygj/s7653p/202003/46c9294a7dfe4cef80dc7f5912eb1989.shtml (accessed on 17 March 2020).
- American Diabetes Association. 2. Classification and diagnosis of diabetes: Standards of medical Care in diabetes-2020. Diabetes Care 2020, 43 (Suppl. 1), S14–S31. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Gong, X.; Wang, L.; Guo, J. Effects of hypertension, diabetes and coronary heart disease on COVID-19 diseases severity: A systematic review and meta-analysis. medRxiv 2020. [Google Scholar] [CrossRef]
- Sathish, T.; Tapp, R.J.; Cooper, M.E.; Zimmet, P. Potential metabolic and inflammatory pathways between COVID-19 and new-onset diabetes. Diabetes Metab. 2021, 47, 101204. [Google Scholar] [CrossRef]
- Wang, S.; Ma, P.; Zhang, S.; Song, S.; Wang, Z.; Ma, Y.; Xu, J.; Wu, F.; Duan, L.; Yin, Z.; et al. Fasting blood glucose at admission is an independent predictor for 28-day mortality in patients with COVID- 19 without previous diagnosis of diabetes: A multi-centre retrospective study. Diabetologia 2020, 63, 2102–2111. [Google Scholar] [CrossRef]
- Smith, S.M.; Boppana, A.; Traupman, J.A.; Unson, E.; Maddock, D.A.; Chao, K.; Dobesh, D.P.; Brufsky, A.; Connor, R.I. Impaired glucose metabolism in patients with diabetes, prediabetes, and obesity is associated with severe COVID-19. J. Med. Virol. 2021, 93, 409–415. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.; et al. Clinical characteristics of corona virus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Sathish, T.; Kapoor, N.; Cao, Y.; Tapp, R.J.; Zimmet, P. Proportion of newly diagnosed diabetes in COVID-19 patients: A systematic review and meta-analysis. Diabetes Obes. Metab. 2021, 23, 870–874. [Google Scholar] [CrossRef] [PubMed]
- Fadini, G.P.; Morieri, M.L.; Boscari, F.; Fioretto, P.; Maran, A.; Busetto, L.; Tresso, S.; Cattelan, A.M.; Vettor, R. Newly diagnosed diabetes and admission hyperglycemia predict COVID-19 severity by aggravating respiratory deterioration. Diabetes Res. Clin. Pract. 2020, 168, 108374. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Tian, S.; Chen, T.; Cui, Z.; Shi, N.; Zhong, X.; Qiu, K.; Zhang, J.; Zeng, T.; Chen, L.; et al. Newly diagnosed diabetes is associated with a higher risk of mortality than known diabetes in hospitalized patients with COVID-19. Diabetes Obes. Metab. 2020, 22, 1897–1906. [Google Scholar] [CrossRef] [PubMed]
- Reddy, P.K.; Kuchay, M.S.; Mehta, Y.; Mishra, S.K. Diabetic ketoacidosis precipitated by COVID-19: A report of two cases and review of literature. Diabetes Metab. Syndr. 2020, 14, 1459–1462. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280. [Google Scholar] [CrossRef]
- Bode, B.; Garrett, V.; Messler, J.; McFarland, R.; Crowe, J.; Booth, R.; Klonoff, D.C. Glycemic Characteristics and Clinical Outcomes of COVID-19 Patients Hospitalized in the United States. J. Diabetes Sci. Technol. 2020, 14, 813–821. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Rodelo, J.R.; De la Rosa, G.; Valencia, M.L.; Ospina, S.; Arango, C.M.; Gómez, C.I.; García, A.; Nuñez, E.; Jaimes, F.A. D-dimer is a significant prognostic factor in patients with suspected infection and sepsis. Am. J. Emerg. Med. 2012, 30, 1991–1999. [Google Scholar] [CrossRef]
- Lippi, G.; Wong, J.; Henry, B.M. Hypertension in patients with coronavirus disease 2019 (COVID-19): A pooled analysis. Pol. Arch. Intern. Med. 2020, 130, 304–309. [Google Scholar] [PubMed] [Green Version]
- Bonow, R.O.; Fonarow, G.C.; O’Gara, P.T.; Yancy, C.W. Association of coronavirus disease 2019 (COVID-19) with myocardial injury and mortality. JAMA Cardiol. 2020, 5, 751–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variables | No. (%), Mean ± SD or Median. | p | ||
|---|---|---|---|---|
| All Participants (n = 570) | Non-Diabetic Patients (Group I, n = 493) | Newly Diagnosed Diabetic Patients (Group II, n = 77) | ||
| Age (years) | 47.9 ± 10.9 | 46.4 ± 10 | 57.7 ± 11.4 | <0.001 |
| Male gender | 317 (55.5%) | 276 (56%) | 41(53.2) | 0.712 * |
| BMI | 26 ± 5.9 | 25 ± 4.5 | 32 ± 9 | <0.001 ** |
| Hypertensive | 45 (7.9%) | 36 (7.3%) | 9 (11.7%) | 0.178 * |
| IHD | 19 (3.3%) | 12 (2.4%) | 7 (9.1%) | 0.008 * |
| Family history of DM | 56 (9.8%) | 22 (4.5%) | 34 (44.2%) | <0.001 * |
| Severe COVID-19 | 297 (52.1%) | 228 (46.2%) | 69 (89.6%) | <0.001 * |
| Fever | 327 (57.4%) | 257 (52.1%) | 70 (90.9%) | <0.001 * |
| Cough | 312 (54.7%) | 242 (49.1%) | 70 (90.9%) | <0.001 * |
| Dyspnea | 301 (52.8%) | 235 (47.7%) | 66 (85.7%) | <0.001 * |
| Diarrhea | 78 (13.7%) | 67 (13.6%) | 11 (14.3%) | 0.859 * |
| FPG (mg/dL) | 105.9 ± 57.9 | 89.9 ± 10.3 | 208.3 ± 109.9 | <0.001 ** |
| HbA1C | 5.4 ± 0.6 | 5.4 ± 0.6 | 5.7 ± 0.8 | <0.001 |
| Positive urinary acetone | 4 (0.7%) | 0 | 4 (5.2%) | <0.001 * |
| DKA on presentation | 4 (0.7%) | 0 | 4 (5.2%) | <0.001 * |
| Hemoglobin (g/dL) | 11.8 ± 1.4 | 11.7 ± 1.4 | 11.9 ± 1.4 | 0.234 |
| Platelets count (×103/mm3) | 191.3 ± 50.6 | 192.3 ± 50.1 | 184.9 ± 53.1 | 0.230 |
| WBCs (×103/mm3) | 6.4 ± 2.5 | 6.4 ± 2.6 | 6.2 ± 2.3 | 0.511 |
| Lymphocytes (×103/mm3) | 2.1 ± 1.1 | 2.2 ± 1.1 | 1.5 ± 0.8 | <0.001 ** |
| Absolute lymphopenia (<1 × 103/mm3) | 169 (29.6%) | 123 (24.9%) | 46 (59.7%) | <0.001 ** |
| CRP (mg/dL) | 38.8 ± 23.8 | 36.3 ± 19.9 | 55.4 ± 37.2 | 0.009 ** |
| ESR (mm/h) | 41.3 ± 14 | 41.1 ± 13.9 | 42.6 ± 14.5 | 0.389 |
| Serum ferritin (ng/mL) | 236 ± 170.3 | 217.9 ± 150.4 | 351.7 ± 234.6 | <0.001 ** |
| LDH (IU/L) | 246.2 ± 80.5 | 239.9 ± 77.4 | 287 ± 88.7 | <0.001 ** |
| D-dimer (μg/mL) | 1 ± 1.4 | 0.9 ± 1.2 | 1.5 ± 2 | <0.001 ** |
| Serum creatinine (mg/dL) | 1 ± 0.3 | 1 ± 0.3 | 1 ± 0.2 | 0.727 |
| Blood urea (mg/dL) | 36.6 ± 25.5 | 36.5 ± 25.3 | 37 ± 26.3 | 0.893 |
| INR | 1.1 ± 0.2 | 1.1 ± 0.2 | 1.1 ± 0.1 | 0.098 |
| Serum albumin (g/dL) | 3.6 ± 0.5 | 3.6 ± 0.5 | 3.7 ± 0.4 | 0.352 |
| Serum total bilirubin (g/dL) | 1.1 ± 0.2 | 1.1 ± 0.2 | 1.1 ± 0.1 | 0.058 ** |
| ALT (IU/L) | 33.9 ± 23.7 | 33.4 ± 23.2 | 36.6 ± 26.7 | 0.278 |
| AST (IU/L) | 56.2 ± 37.7 | 55.4 ± 36.8 | 60.8 ± 43 | 0.249 |
| Positive chest CT findings | 297 (52.1%) | 228 (46.2%) | 69 (89.6%) | <0.001 * |
| Deceased | 62 (10.9%) | 48 (9.7%) | 14 (18.2%) | 0.046 * |
| Variables | No. (%), Mean ± SD or Median. | p | ||
|---|---|---|---|---|
| Pre-Existing DM (Group IIA, n = 12) | New-Onset Type 1 DM (Group IIB, n = 7) | New-Onset Type 2 DM (Group IIC, n = 58) | ||
| Age (years) | 58.3 ± 8.7 | 36 ± 8.6 | 60.1 ± 9.3 | <0.001 |
| Male patients | 7 (58.3%) | 4 (57.1%) | 30 (51.7%) | 0.895 |
| BMI | 29.1 ± 6.7 | 21.4 ± 2.4 | 33.9 ± 9 | <0.001 ** |
| Hypertensive | 1 (8.3%) | 0 | 8 (13.8%) | 0.520 |
| IHD | 0 | 0 | 7 (12.1%) | 0.283 |
| Family history of DM | 5 (41.7%) | 2 (28.6%) | 27 (46.6%) | 0.652 |
| Severe COVID-19 | 8 (66.7%) | 7 (100%) | 54 (93.1%) | 0.015 |
| FPG (mg/dL) | 194.3 ± 64.3 | 473.4 ± 124.4 | 179.2 ± 64.5 | <0.001 ** |
| HbA1C | 7.2 ± 0.4 | 5.3 ± 0.5 | 5.4 ± 0.5 | <0.001 |
| Fasting insulin (mIU/L) | 33.4 ± 9.2 | 3.6 ± 1.3 | 38.1 ± 9.1 | <0.001 |
| C-peptide (ng/mL) | 3.5 ± 1 | 0.3 ± 0.1 | 3.6 ± 0.8 | <0.001 ** |
| Positive urinary acetone | 0 | 4 (57.1%) | 0 | <0.001 |
| DKA on presentation | 0 | 4 (57.1%) | 0 | <0.001 |
| Hemoglobin (g/dL) | 12.2 ± 1.9 | 10.9 ± 1.4 | 12 ± 1.3 | 0.119 |
| Platelets count (×103/mm3) | 154.9 ± 32.4 | 190.1 ± 88.2 | 190.4 ± 50.1 | 0.103 |
| WBCs (×103/mm3) | 6.3 ± 2.5 | 6.9 ± 2.9 | 6.2 ± 2.3 | 0.747 |
| Lymphocytes (mean ± SD, ×103/mm3) | 1.7 ± 0.9 | 1 ± 0.3 | 1.5 ± 0.8 | 0.282 |
| Absolute lymphopenia (<1 ×103/mm3) | 6 (50%) | 6 (85.7%) | 34 (58.6%) | 0.291 |
| CRP (mg/L) | 55.7 ± 31 | 113.1 ± 56.9 | 48.4 ± 29.2 | 0.004 ** |
| ESR ((mm/h) | 39.5 ± 15.3 | 52.7 ± 14.4 | 42 ± 14.1 | 0.130 |
| Serum ferritin (ng/mL) | 318.9 ± 177.9 | 832 ± 252.7 | 300.6 ± 171.2 | 0.002 ** |
| LDH (IU/L) | 256.1 ± 82.5 | 360 ± 100.8 | 284.6 ± 85.1 | 0.100 ** |
| D-dimer (μg/mL) | 0.9 ± 0.5 | 5 ± 5.3 | 1.2 ± 0.9 | 0.007 s** |
| Serum creatinine (mg/dL) | 1 ± 1.3 | 1.1 ± 0.3 | 1 ± 0.2 | 0.336 |
| Blood urea (mg/dL) | 29 ± 19 | 49.3 ± 37.6 | 37.1 ± 26 | 0.272 |
| Positive chest CT findings | 8 (66.7%) | 7 (100%) | 54 (93.1%) | 0.015 |
| Deceased | 3 (25%) | 3 (42.9%) | 8 (13.8%) | 0.136 |
| Variables | R | p |
|---|---|---|
| Age (years) | 0.354 | <0.001 * |
| BMI | 0.312 | <0.001 ** |
| Severe COVID-19 | 0.297 | <0.001 ** |
| Lymphocytes (×103/mm3) | −0.236 | <0.001 * |
| Absolute lymphopenia (<1 × 103/mm3) | 0.260 | <0.001 * |
| CRP (mg/L) | 0.186 | <0.001 ** |
| Serum ferritin (ng/mL) | 0.222 | <0.001 ** |
| LDH | 0.191 | <0.001** |
| D-dimer (μg/mL) | 0.202 | <0.001 ** |
| Positive chest CT findings | 0.297 | <0.001 ** |
| Variables | B | Exp (B) | 95% C.I. for Exp (B) | p | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| COVID-19 severity | −1.300 | 0.272 | 0.096 | 0.776 | 0.015 |
| Age | 0.081 | 1.084 | 1.047 | 1.123 | <0.001 |
| BMI | 0.175 | 1.192 | 1.123 | 1.265 | <0.001 |
| Lymphocytes | −0.562 | 0.570 | 0.329 | 0.988 | 0.045 |
| Lymphopenia | 0.975 | 2.650 | 0.859 | 8.176 | 0.090 |
| CRP | 0.023 | 1.024 | 1.010 | 1.037 | <0.001 |
| Ferritin | 0.003 | 1.003 | 1.001 | 1.004 | <0.001 |
| LDH | −0.002 | 0.998 | 0.994 | 1.003 | 0.456 |
| D. dimer | 0.020 | 1.020 | 0.824 | 1.264 | 0.854 |
| Variables | No. (%), Mean ± SD or Median. | p | |
|---|---|---|---|
| Survived Patients (n = 508) | Died Patients (n = 62) | ||
| Age (years) | 47.4 ± 10.9 | 52.2 ± 9.6 | <0.001 |
| Male gender | 279 (54.9%) | 38 (61.3) | 0.341 |
| BMI | 25.9 ± 5.6 | 26.7 ± 7.8 | 0.284 |
| Hypertensive | 33 (6.5%) | 12 (19.4%) | <0.001 * |
| IHD | 14 (2.8%) | 5 (8.1%) | 0.028 * |
| Newly discovered DM | 63 (12.4%) | 14 (22.6%) | 0.027 |
| Type of DM | |||
| Pre-existing DM | 9 (1.8%) | 3 (4.8%) | 0.012 * |
| DM type 1 | 4 (0.8%) | 3 (4.8%) | |
| DM type 2 | 50 (9.8%) | 8 (12.9%) | |
| Severe COVID-19 | 247 (48.6%) | 50 (80.6%) | <0.001 |
| FPG (mg/dL) | 103.5 ± 49.9 | 125.5 ± 100.5 | 0.179 ** |
| HbA1C | 5.4 ± 0.6 | 5.4 ± 0.6 | 0.966 |
| DKA on presentation | 2 (0.4%) | 2 (3.2%) | <0.012 * |
| Hemoglobin (g/dL) | 11.8 ± 1.4 | 11.7 ± 1.1 | 0.455 |
| Platelets count (×103/mm3) | 192.1 ± 50.5 | 185.1 ± 51.2 | 0.305 |
| WBCs (×103/mm3) | 6.5 ± 2.6 | 5.9 ± 2.4 | 0.113 |
| Lymphocytes (×103/mm3) | 2.3 ± 1.1 | 1.2 ± 0.9 | <0.001 ** |
| Absolute lymphopenia (<1 × 103/mm3) | 116 (22.8%) | 53 (85.5%) | <0.001 * |
| CRP (mg/dL) | 36.2 ± 20.2 | 60.9 ± 36.9 | <0.001 ** |
| ESR (mm/h) | 41.4 ± 14.1 | 40.0 ± 13.4 | 0.458 |
| Serum ferritin (ng/mL) | 223.4 ± 157.2 | 338.7 ± 230.5 | <0.001 ** |
| LDH (IU/L) | 237.7 ± 75.5 | 316.2 ± 86.6 | <0.001 ** |
| D-dimer (μg/mL) | 0.9 ± 0.9 | 1.9 ± 3.1 | <0.001 ** |
| Serum creatinine (mg/dL) | 1 ± 0.3 | 1 ± 0.3 | 0.610 |
| Blood urea (mg/dL) | 36.1 ± 24.8 | 40.3 ± 30.5 | 0.367 ** |
| INR | 1.1 ± 0.2 | 1.2 ± 0.2 | 0.321 |
| Serum albumin (g/dL) | 3.6 ± 0.5 | 3.6 ± 0.5 | 0.328 |
| Serum total bilirubin (g/dL) | 1.1 ± 0.2 | 1.1 ± 0.2 | 0.764 ** |
| ALT (IU/L) | 34.4 ± 24.1 | 29.6 ± 19.5 | 0.269 ** |
| AST (IU/L) | 56.9 ± 38.7 | 50.2 ± 27.7 | 0.435 ** |
| Positive chest CT findings | 247 (48.6%) | 50 (80.6%) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farag, A.A.; Hassanin, H.M.; Soliman, H.H.; Sallam, A.; Sediq, A.M.; Abd elbaser, E.S.; Elbanna, K. Newly Diagnosed Diabetes in Patients with COVID-19: Different Types and Short-Term Outcomes. Trop. Med. Infect. Dis. 2021, 6, 142. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed6030142
Farag AA, Hassanin HM, Soliman HH, Sallam A, Sediq AM, Abd elbaser ES, Elbanna K. Newly Diagnosed Diabetes in Patients with COVID-19: Different Types and Short-Term Outcomes. Tropical Medicine and Infectious Disease. 2021; 6(3):142. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed6030142
Chicago/Turabian StyleFarag, Alaa A., Hassan M. Hassanin, Hanan H. Soliman, Ahmad Sallam, Amany M. Sediq, Elsayed S. Abd elbaser, and Khaled Elbanna. 2021. "Newly Diagnosed Diabetes in Patients with COVID-19: Different Types and Short-Term Outcomes" Tropical Medicine and Infectious Disease 6, no. 3: 142. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed6030142