
Time Trend Analysis of Tuberculosis Treatment While Using Digital Adherence Technologies—An Individual Patient Data Meta-Analysis of Eleven Projects across Ten High Tuberculosis-Burden Countries

 , , , and add
Show full author list
, , , and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Study Population
- Patients with zero doses taken during all first six treatment months;
- Patients aged fourteen years or younger;
- Patients whose type of TB (DS or DR) differed from the type of TB the project focused on;
- DS-TB patients who started DAT more than two weeks after they started with medication.
2.3. Operationalization of Variables
2.3.1. Dependent Variable
2.3.2. Independent Variables
2.4. Statistical Analysis
2.4.1. Descriptive Analysis
2.4.2. Regression Analysis
2.4.3. Sensitivity Analyses
3. Results
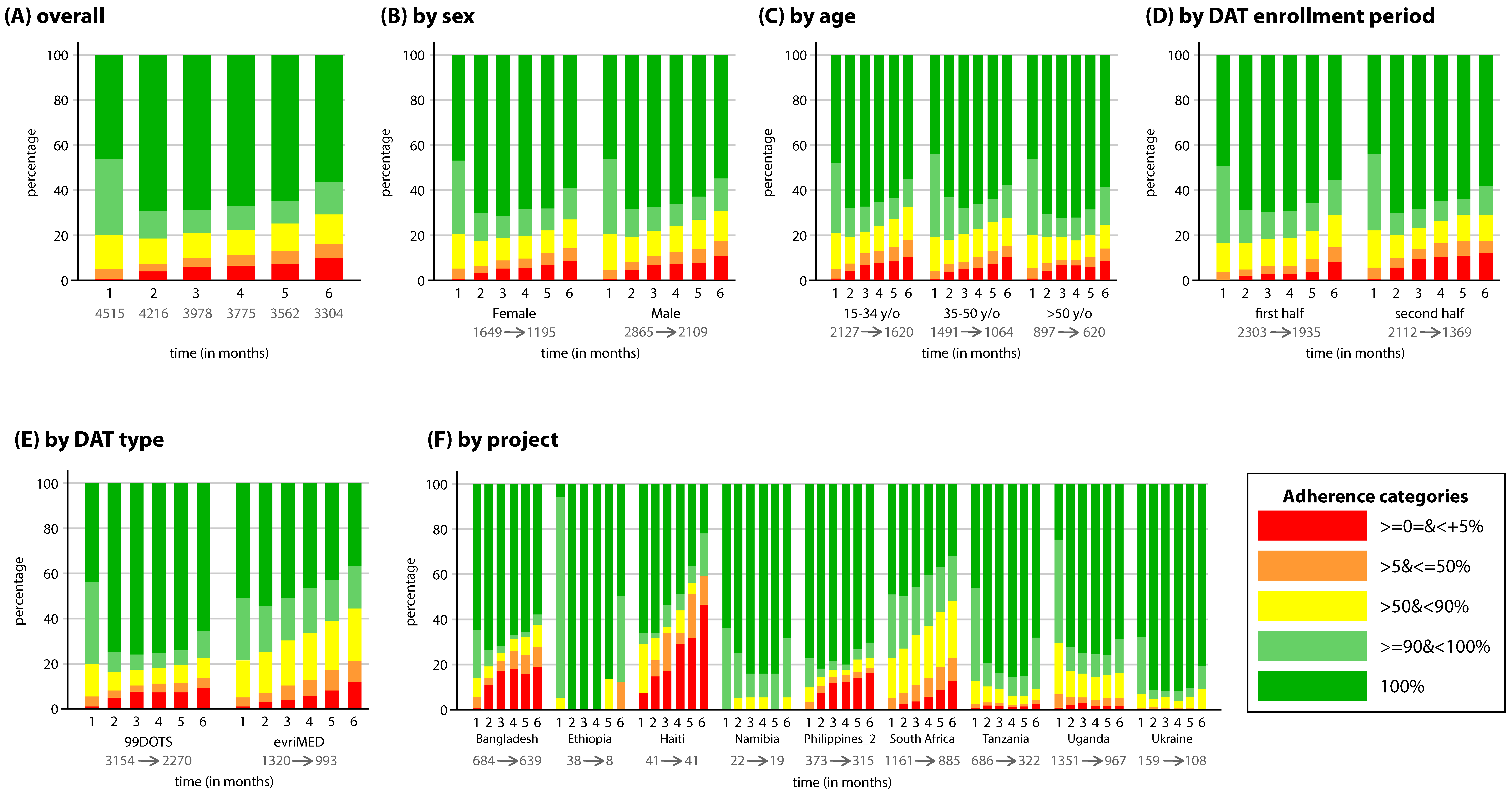
3.1. DS-TB Population
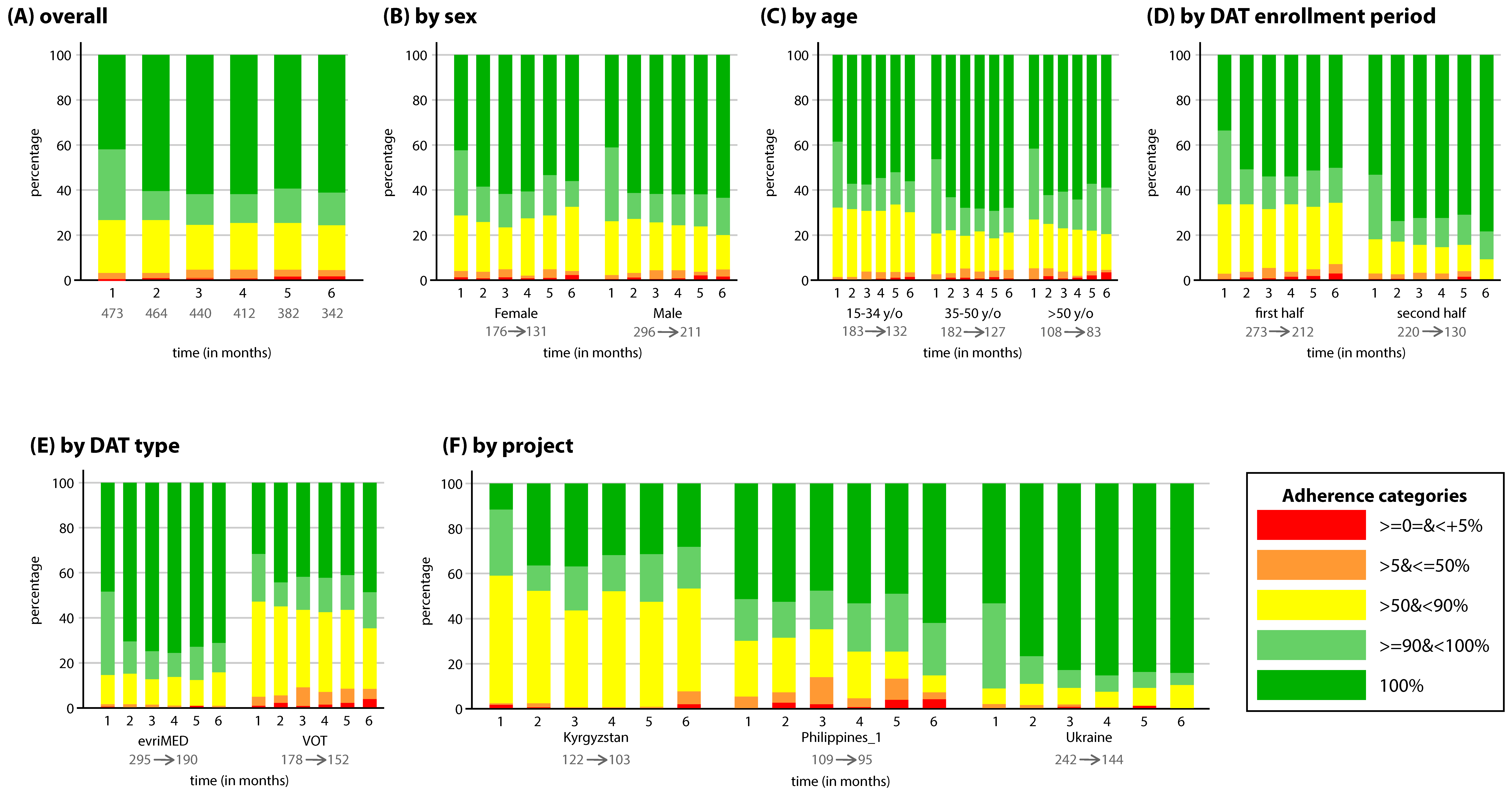
3.2. DR-TB Population
3.3. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report 2021; World Health Organization: Geneva, Switzerland, 2021; Available online: https://www.who.int/publications/i/item/9789240013131 (accessed on 25 January 2022).
- World Health Organization. The End TB Strategy. 2015. Available online: https://www.who.int/teams/global-tuberculosis-programme/the-end-tb-strategy (accessed on 30 November 2021).
- World Health Organization. Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection. 2016. Available online: https://www.who.int/publications/i/item/9789241549684 (accessed on 30 November 2021).
- Pradipta, I.S.; Forsman, L.D.; Bruchfeld, J.; Hak, E.; Alffenaar, J.W. Risk factors of multidrug-resistant tuberculosis: A global systematic review and meta-analysis. J. Infect. 2018, 77, 469–478. [Google Scholar] [CrossRef] [Green Version]
- Chimeh, R.A.; Gafar, F.; Pradipta, I.S.; Akkerman, O.W.; Hak, E.; Alffenaar, J.-W.C. Clinical and economic impact of medication non-adherence in drug-susceptible tuberculosis: A systematic review. Int. J. Tuberc. Lung Dis. 2020, 24, 811–819. [Google Scholar] [CrossRef]
- World Health Organization. What Is DOTS? A Guide to Understanding the WHO Recommended TB Control Strategy Known as DOTS; World Health Organization: Geneva, Switzerland, 1999; Available online: https://apps.who.int/iris/bitstream/handle/10665/65979/WHO_CDS_CPC_TB_99.270.pdf (accessed on 12 January 2021).
- Alipanah, N.; Jarlsberg, L.; Miller, C.; Linh, N.N.; Falzon, D.; Jaramillo, E.; Nahid, P. Adherence interventions and outcomes of tuberculosis treatment: A systematic review and meta-analysis of trials and observational studies. PLoS Med. 2018, 15, e1002595. [Google Scholar] [CrossRef]
- Valencia, S.; León, M.; Losada, I.; Sequera, V.G.; Fernández Quevedo, M.; García-Basteiro, A.L. How do we measure adherence to anti-tuberculosis treatment? Expert Rev. Anti-Infect. Ther. 2017, 15, 157–165. [Google Scholar] [CrossRef]
- Karumbi, J.; Garner, P. Directly observed therapy for treating tuberculosis. Cochrane Infectious Diseases Group, ed. Cochrane Database Syst. Rev. 2015, 5, CD003343. Available online: https://0-doi-wiley-com.brum.beds.ac.uk/10.1002/14651858.CD003343.pub4 (accessed on 1 December 2021).
- Sagbakken, M.; Frich, J.C.; Bjune, G.A.; Porter, J.D. Ethical aspects of directly observed treatment for tuberculosis: A cross-cultural comparison. BMC Med. Ethics. 2013, 14, 25. [Google Scholar] [CrossRef] [Green Version]
- Subbaraman, R.; de Mondesert, L.; Musiimenta, A.; Pai, M.; Mayer, K.H.; Thomas, B.E.; Haberer, J. Digital adherence technologies for the management of tuberculosis therapy: Mapping the landscape and research priorities. BMJ Glob. Health 2018, 3, e001018. [Google Scholar] [CrossRef] [Green Version]
- Katamba, A.; Neuheuser, D.B.; Smyth, K.A.; Adatu, F.; Katabira, E.; Whalen, C.C. Patients perceived stigma associated with community-based directly observed therapy of tuberculosis in Uganda. East Afr. Med. J. 2005, 82, 337–428. [Google Scholar]
- Stagg, H.R.; Flook, M.; Martinecz, A.; Kielmann, K.; Zur Wiesch, P.A.; Karat, A.S.; Lipman, M.C.I.; Sloan, D.J.; Walker, E.F.; Fielding, K.L. All nonadherence is equal but is some more equal than others? Tuberculosis in the digital era. ERJ Open Res. 2020, 6, 00315–2020. [Google Scholar] [CrossRef]
- Lee, Y.; Raviglione, M.C.; Flahault, A. Use of Digital Technology to Enhance Tuberculosis Control: Scoping Review. J. Med. Internet Res. 2020, 22, e15727. [Google Scholar] [CrossRef] [Green Version]
- Chuck, C.; Robinson, E.; Macaraig, M.; Alexander, M.; Burzynski, J. Enhancing management of tuberculosis treatment with video directly observed therapy in New York City. Int. J. Tuberc. Lung Dis. 2016, 20, 588–593. [Google Scholar] [CrossRef]
- Thakkar, D.; Piparva, K.; Lakkad, S. A pilot project: 99DOTS information communication technology-based approach for tuberculosis treatment in Rajkot district. Lung India 2019, 36, 108. [Google Scholar]
- Ratchakit-Nedsuwan, R.; Nedsuwan, S.; Sawadna, V.; Chaiyasirinroje, B.; Bupachat, S.; Ngamwithayapong-Yanai, J.; Kantima, T.; Luangjina, S.; Boonyamanonukul, P.; Wongyai, J.; et al. Ensuring tuberculosis treatment adherence with a mobile-based CARE-call system in Thailand: A pilot study. Infect. Dis. 2020, 52, 121–129. [Google Scholar] [CrossRef]
- Ngwatu, B.K.; Nsengiyumva, N.P.; Oxlade, O.; Mappin-Kasirer, B.; Nguyen, N.L.; Jaramillo, E.; Falzon, D.; Schwartzman, K. The impact of digital health technologies on tuberculosis treatment: A systematic review. Eur. Respir. J. 2018, 51, 1701596. [Google Scholar] [CrossRef] [Green Version]
- Mekonnen, H.S.; Azagew, A.W. Non-adherence to anti-tuberculosis treatment, reasons and associated factors among TB patients attending at Gondar town health centers, Northwest Ethiopia. BMC Res. Notes 2018, 11, 691. [Google Scholar] [CrossRef]
- Stagg, H.R.; Lewis, J.J.; Liu, X.; Huan, S.; Jiang, S.; Chin, D.P.; Fielding, K.L. Temporal Factors and Missed Doses of Tuberculosis Treatment. A Causal Associations Approach to Analyses of Digital Adherence Data. Ann. Am. Thorac. Soc. 2020, 17, 438–449. [Google Scholar] [CrossRef]
- Mukherjee, A.; Sarkar, A.; Saha, I.; Chowdhury, R. Gender differences in notification rates, clinical forms and treatment outcome of tuberculosis patients under the RNTCP. Lung India 2012, 29, 120. [Google Scholar] [CrossRef]
- Gosavi, A.D.; Nandimath, V.A.; Mangulikar, S.K. A cross-sectional study among defaulters of DOTS under RNTCP in tuberculosis units of Solapur city. Int. J. Community Med. Public Health 2019, 6, 1167. [Google Scholar] [CrossRef]
- Gust, D.A.; Mosimaneotsile, B.; Mathebula, U.; Chingapane, B.; Gaul, Z.; Pals, S.L.; Samandari, T. Risk Factors for Non-Adherence and Loss to Follow-Up in a Three-Year Clinical Trial in Botswana. PLoS ONE 2011, 6, e18435. [Google Scholar] [CrossRef] [Green Version]
- Tesfahuneygn, G.; Medhin, G.; Legesse, M. Adherence to Anti-tuberculosis treatment and treatment outcomes among tuberculosis patients in Alamata District, northeast Ethiopia. BMC Res. Notes 2015, 8, 503. [Google Scholar] [CrossRef] [Green Version]
- Koo, H.-K.; Min, J.; Kim, H.W.; Lee, J.; Kim, J.S.; Park, J.S.; Lee, S.S. Prediction of treatment failure and compliance in patients with tuberculosis. BMC Infect. Dis. 2020, 20, 622. [Google Scholar] [CrossRef]
- Krasniqi, S.; Jakupi, A.; Daci, A.; Tigani, B.; Jupolli-Krasniqi, N.; Pira, M.; Zhjeqi, V.; Nezeri, B. Tuberculosis Treatment Adherence of Patients in Kosovo. Tuberc. Res. Treat. 2017, 2017, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Mendys, P.; Zullig, L.; Burkholder, R.; Granger, B.; Bosworth, H. Medication adherence: Process for implementation. Patient Prefer. Adherence 2014, 8, 1025. [Google Scholar]
- LeFevre, A.E.; Shah, N.; Bashingwa, J.J.H.; George, A.S.; Mohan, D. Does women’s mobile phone ownership matter for health? Evidence from 15 countries. BMJ Glob. Health 2020, 5, e002524. [Google Scholar] [CrossRef]
- Stop TB partnership. Wave 6 Digital Adherence Technology Projects [Internet]. Stop TB Partnership. Available online: http://stoptb.org/global/awards/tbreach/wave6DAT.asp (accessed on 23 June 2021).
- Twisk, J.; Rijmen, F. Longitudinal tobit regression: A new approach to analyze outcome variables with floor or ceiling effects. J. Clin. Epidemiol. 2009, 62, 953–958. [Google Scholar] [CrossRef]
- Twisk, J.; Spriensma, A.; Eekhout, I.; de Boer, M.; Luime, J.; de Jong, P.; Bahçecitapar, M.K.; Heymans, M. Analysing outcome variables with floor effects due to censoring: A simulation study with longitudinal trial data. Epidemiol. Biostat. Public Health 2018, 15, 1–9. [Google Scholar]
- AlSahafi, A.J.; Shah, H.B.U.; AlSayali, M.M.; Mandoura, N.; Assiri, M.; Almohammadi, E.L.; Khalawi, A.; AlGarni, A.; Filemban, M.K.; AlOtaibe, A.K.; et al. High non-compliance rate with anti-tuberculosis treatment: A need to shift facility-based directly observed therapy short course (DOTS) to community mobile outreach team supervision in Saudi Arabia. BMC Public Health 2019, 19, 1168. [Google Scholar] [CrossRef] [Green Version]
- Do, D.; Garfein, R.S.; Cuevas-Mota, J.; Collins, K.; Liu, L. Change in Patient Comfort Using Mobile Phones Following the Use of an App to Monitor Tuberculosis Treatment Adherence: Longitudinal Study. JMIR MHealth UHealth 2019, 7, e11638. [Google Scholar] [CrossRef]
- El-Muttalut, M.; Khidir Elnimeiri, M. Factors contributing to non-compliance with treatment among tuberculosis patients-Kassala State-Sudan-2016. Int. J. Public Health 2017, 6, 332–338. [Google Scholar]
- Nour El Din, M.; Elhoseeny, T.; Mohsen, A.M.M.A. Factors affecting defaulting from DOTS therapy under the national programme of tuberculosis control in Alexandria, Egypt. E. Mediterr. Health J. 2013, 19, 107–113. [Google Scholar] [CrossRef]
- Alhazami, M.; Pontinha, V.M.; Patterson, J.A.; Holdford, D.A. Medication Adherence Trajectories: A Systematic Literature Review. J. Manag. Care Spec. Pharm. 2020, 26, 1138–1152. [Google Scholar] [CrossRef]
- Mohammed, S.; Glennerster, R.; Khan, A.J. Impact of a Daily SMS Medication Reminder System on Tuberculosis Treatment Outcomes: A Randomized Controlled Trial. PLoS ONE 2016, 11, e0162944. [Google Scholar] [CrossRef] [Green Version]
- Mohammed, S.; Siddiqi, O.; Ali, O.; Habib, A.; Haqqi, F.; Kausar, M.; Khan, A.J. User engagement with and attitudes towards an interactive SMS reminder system for patients with tuberculosis. J. Telemed. Telecare 2012, 18, 404–408. [Google Scholar] [CrossRef]
- Haberer, J.E.; Subbaraman, R. Digital Technology for Tuberculosis Medication Adherence: Promise and Peril. Ann. Am. Thorac. Soc. 2020, 17, 421–423. [Google Scholar] [CrossRef]
- Drabarek, D.; Anh, N.T.; Nhung, N.V.; Hoa, N.B.; Fox, G.J.; Bernays, S. Implementation of Medication Event Reminder Monitors among patients diagnosed with drug susceptible tuberculosis in rural Viet Nam: A qualitative study. PLoS ONE 2019, 14, e0219891. [Google Scholar] [CrossRef]
- Thomas, B.E.; Kumar, J.V.; Chiranjeevi, M.; Shah, D.; Khandewale, A.; Thiruvengadam, K.; Haberer, J.E.; Mayer, K.H.; Subbaraman, R. Evaluation of the Accuracy of 99DOTS, a Novel Cellphone-based Strategy for Monitoring Adherence to Tuberculosis Medications: Comparison of DigitalAdherence Data With Urine Isoniazid Testing. Clin. Infect. Dis. 2020, 71, e513–e516. [Google Scholar] [CrossRef] [Green Version]
- Kigozi, G.; Heunis, C.; Chikobvu, P.; Botha, S.; van Rensburg, D. Factors influencing treatment default among tuberculosis patients in a high burden province of South Africa. Int. J. Infect. Dis. 2017, 54, 95–102. [Google Scholar] [CrossRef] [Green Version]
- Afshari, M.; Aarabi, M.; Parsaee, M.; Nezammahalleh, A.; Moosazadeh, M. Treatment default and its related factors among tuberculosis patients, a case-control study in Iran. GMS Hyg. Infect. Control 2020, 15, Doc33. [Google Scholar]
- Kulkarni, P.; Akarte, S.; Mankeshwar, R.; Bhawalkar, J.; Banerjee, A.; Kulkarni, A. Non-Adherence of New Pulmonary Tuberculosis Patients to Anti-Tuberculosis Treatment. Ann. Med. Health Sci. Res. 2013, 3, 67–74. [Google Scholar]
- Ajao, K.O.; Ogundun, O.A.; Afolabi, O.T.; Ojo, T.O.; Atiba, B.P.; Oguntunase, D.O. Treatment compliance and challenges among tuberculosis patients across selected health facilities in Osun State Nigeria. Afr. J. Med. Med. Sci. 2014, 43, S21–S29. [Google Scholar]
- Ogundele, O.A.; Moodley, D.; Pillay, A.; Seebregts, C. An ontology for factors affecting tuberculosis treatment adherence behavior in sub-Saharan Africa. Patient Prefer. Adherence 2016, 10, 669–681. [Google Scholar] [CrossRef]
- Tola, H.H.; Garmaroudi, G.; Shojaeizadeh, D.; Tol, A.; Yekaninejad, M.S.; Ejeta, L.T.; Kassa, D.; Klinkenberg, E. The effect of psychosocial factors and patients’ perception of tuberculosis treatment non-adherence in Addis Ababa, Ethiopia. Ethiop. J. Health Sci. 2017, 27, 447. [Google Scholar] [CrossRef] [Green Version]
- Kiros, Y.K.; Teklu, T.; Desalegn, F.; Tesfay, M.; Klinkenberg, E.; Mulugeta, A. Adherence to anti-tuberculosis treatment in Tigray, Northern Ethiopia. Public Health Action 2014, 4 (Suppl. 3), S31–S36. [Google Scholar] [CrossRef] [Green Version]
- Lackey, B.; Seas, C.; Van der Stuyft, P.; Otero, L. Patient Characteristics Associated with Tuberculosis Treatment Default: A Cohort Study in a High-Incidence Area of Lima, Peru. PLoS ONE 2015, 10, e0128541. [Google Scholar] [CrossRef] [Green Version]
- Du, L.; Chen, X.; Zhu, X.; Zhang, Y.; Wu, R.; Xu, J.; Ji, H.; Zhou, L.; Lu, X. Determinants of Medication Adherence for Pulmonary Tuberculosis Patients During Continuation Phase in Dalian, Northeast China. Patient Prefer. Adherence 2020, 14, 1119–1128. [Google Scholar] [CrossRef]
- Ruru, Y.; Matasik, M.; Oktavian, A.; Senyorita, R.; Mirino, Y.; Tarigan, L.H.; Van der Werf, M.J.; Tiemersma, E.; Alisjahbana, B. Factors associated with non-adherence during tuberculosis treatment among patients treated with DOTS strategy in Jayapura, Papua Province, Indonesia. Glob. Health Action 2018, 11, 1510592. [Google Scholar] [CrossRef]
- Alobu, I.; Oshi, S.N.; Oshi, D.C.; Ukwaja, K.N. Risk factors of treatment default and death among tuberculosis patients in a resource-limited setting. Asian Pac. J. Trop. Med. 2014, 7, 977–984. [Google Scholar] [CrossRef]
- Mukasa, J.; Kayongo, E.; Kawooya, I.; Lukoye, D.; Etwom, A.; Mugabe, F.; Tweya, H.; Izizinga, R.; Mijumbi-Deve, R. Adherence to the MDR-TB intensive phase treatment protocol amongst individuals followed up at central and peripheral health care facilities in Uganda—A descriptive study. Afr. Health Sci. 2020, 20, 625–632. [Google Scholar] [CrossRef]
- Cross, A.; Gupta, N.; Liu, B.; Nair, V.; Kumar, A.; Kuttan, R.; Ivatury, P.; Chen, A.; Lakshman, K.; Rodrigues, R.; et al. 99DOTS: A low-cost approach to monitoring and improving medication adherence. In Proceedings of the Tenth International Conference on Information and Communication Technologies and Development, Ahmedabad, India, 4–7 January 2019; pp. 1–12. Available online: https://0-dl-acm-org.brum.beds.ac.uk/doi/10.1145/3287098.3287102 (accessed on 23 June 2021).
- Craig, G.M.; Daftary, A.; Engel, N.; O’Driscoll, S.; Ioannaki, A. Tuberculosis stigma as a social determinant of health: A systematic mapping review of research in low incidence countries. Int. J. Infect. Dis. 2017, 56, 90–100. [Google Scholar] [CrossRef] [Green Version]
- Stop TB Partnership. Grant Management System. Stop TB Partnership. 2021. Available online: http://www.stoptb.org/global/awards/tbreach/gm/default.asp (accessed on 23 June 2021).
- Nguyen, T.A.; Pham, M.T.; Nguyen, T.L.; Nguyen, V.N.; Pham, D.C.; Nguyen, B.H.; Fox, G.J. Video Directly Observed Therapy to support adherence with treatment for tuberculosis in Vietnam: A prospective cohort study. Int. J. Infect. Dis. 2017, 65, 85–89. [Google Scholar] [CrossRef] [Green Version]
- Wiltsey Stirman, S.; Kimberly, J.; Cook, N.; Calloway, A.; Castro, F.; Charns, M. The sustainability of new programs and innovations: A review of the empirical literature and recommendations for future research. Implement Sci. 2012, 7, 17. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Du, L.; Wu, R.; Xu, J.; Ji, H.; Zhang, Y.; Zhu, X.; Zhou, L. The effects of family, society and national policy support on treatment adherence among newly diagnosed tuberculosis patients: A cross-sectional study. BMC Infect. Dis. 2020, 20, 623. [Google Scholar] [CrossRef]
- Orlandi, G.M.; Pereira, É.G.; Biagolini, R.E.M.; França, F.O.D.S.; Bertolozzi, M.R. Social incentives for adherence to tuberculosis treatment. Rev. Bras. Enferm. 2019, 72, 1182–1188. [Google Scholar] [CrossRef]
- Aibana, O.; Dauria, E.; Kiriazova, T.; Makarenko, O.; Bachmaha, M.; Rybak, N.; Flanigan, T.P.; Petrenko, V.; Becker, A.E.; Murray, M.B. Patients’ perspectives of tuberculosis treatment challenges and barriers to treatment adherence in Ukraine: A qualitative study. BMJ Open 2020, 10, e032027. [Google Scholar] [CrossRef] [Green Version]
- Gebreweld, F.H.; Kifle, M.M.; Gebremicheal, F.E.; Simel, L.L.; Gezae, M.M.; Ghebreyesus, S.S.; Mengsteab, Y.T.; Wahd, N.G. Factors influencing adherence to tuberculosis treatment in Asmara, Eritrea: A qualitative study. J. Health Popul. Nutr. 2018, 37, 1. [Google Scholar] [CrossRef]
- Forbes, C.A.; Deshpande, S.; Sorio-Vilela, F.; Kutikova, L.; Duffy, S.; Gouni-Berthold, I.; Hagström, E. A systematic literature review comparing methods for the measurement of patient persistence and adherence. Curr. Med. Res. Opin. 2018, 34, 1613–1625. [Google Scholar] [CrossRef]
- Karve, S.; Cleves, M.A.; Helm, M.; Hudson, T.J.; West, D.S.; Martin, B.C. Prospective Validation of Eight Different Adherence Measures for Use with Administrative Claims Data among Patients with Schizophrenia. Value Health 2009, 12, 989–995. [Google Scholar] [CrossRef] [Green Version]
- MacEwan, J.P.; Silverstein, A.R.; Shafrin, J.; Lakdawalla, D.N.; Hatch, A.; Forma, F.M. Medication Adherence Patterns Among Patients with Multiple Serious Mental and Physical Illnesses. Adv. Ther. 2018, 35, 671–685. [Google Scholar] [CrossRef] [Green Version]
- Llor, C.; Hernández, S.; Bayona, C.; Moragas, A.; Sierra, N.; Hernández, M.; Miravitlles, M. A study of adherence to antibiotic treatment in ambulatory respiratory infections. Int. J. Infect. Dis. 2013, 17, e168–e172. [Google Scholar] [CrossRef] [Green Version]
- Monnette, A.; Zhang, Y.; Shao, H.; Shi, L. Concordance of Adherence Measurement Using Self-Reported Adherence Questionnaires and Medication Monitoring Devices: An Updated Review. PharmacoEconomics 2018, 36, 17–27. [Google Scholar] [CrossRef]
- Van den Boogaard, J.; Lyimo, R.; Boeree, M.; Kibiki, G.; Aarnoutse, R. Electronic monitoring of treatment adherence and validation of alternative adherence measures in tuberculosis patients: A pilot study. Bull. World Health Organ. 2011, 89, 632–639. [Google Scholar] [CrossRef]
- Mkopi, A.; Range, N.; Lwilla, F.; Egwaga, S.; Schulze, A.; Geubbels, E.; Van Leth, F. Validation of indirect tuberculosis treatment adherence measures in a resource-constrained setting. Int. J. Tuberc. Lung Dis. 2018, 18, 804–809. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Bangladesh | Ethiopia | Haiti | Kyrgyzstan | Namibia | Philippines_1 | Philippines_2 | South Africa | Tanzania | Uganda | Ukraine | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DAT 1 type | 99DOTS | 99DOTS | VOT 2 | evriMed | VOT | 99DOTS | VOT | 99DOTS | evriMED | 99DOTS | 99DOTS | evriMED | evriMED |
| N total | 719 | 44 | 77 | 54 | 85 | 24 | 110 | 396 | 1258 | 976 | 1535 | 540 | 258 |
| N study | 684 | 38 | 41 | 53 | 69 | 22 | 109 | 373 | 1161 | 686 | 1351 | 159 | 242 |
| Target group | |||||||||||||
| Age | ≥8 | ≥16 | ≥18 | 18–65 | ≥16 | ≥13 | ≥15 | ≥2 | >15 | ≥19 | ≥18 | ||
| Type of TB | DS-TB | DS-TB | DS-TB | DR-TB | DS-TB | DR-TB | DS-TB | DS-TB | DS-TB | DS-TB | DS-TB | DR-TB | |
| Additional characteristics | private patients from Dhaka | (semi-) nomadic/agro- pastoralists | prisoners | continuation phase from Bishkek and Chui-region | semi-mobile hunters and gatherers | semi-urban | urban poor, elderly, HIV+ | N/A | rural miners | N/A | from Mykolayiv and Odesa oblasts | ||
| Enrollment dates | |||||||||||||
| Start | 10-4-2019 | 29-3-2019 | 9-3-2019 | 11-1-2019 | 9-4-2019 | 27-12-2018 | 6-12-2018 | 1-5-2019 | 25-2-2019 | 10-1-2019 | 13-2-2019 | ||
| End | 28-7-2020 | 27-2-2020 | 21-2-2020 | 28-12-2019 | 13-3-2020 | 14-12-2019 | 16-3-2020 | 16-10-2020 | 30-6-2020 | 31-12-2019 | 11-11-2019 | ||
| Inclusion criteria Additional to:
|
|
|
|
|
|
|
|
|
|
|
| ||
| Sex n (%) | |||||||||||||
| Female | 275 (40.2) | 12 (31.6) | 0 | 18 (34.0) | 34 (49.3) | 16 (72.7) | 38 (34.9) | 101 (27.1) | 413 (35.6) | 260 (37.9) | 506 (37.5) | 66 (41.5) | 86 (35.5) |
| Male | 409 (59.8) | 26 (68.4) | 41 (100) | 35 (66.0) | 34 (49.3) | 6 (27.3) | 71 (65.1) | 271 (72.7) | 748 (64.4) | 426 (62.1) | 845 (62.6) | 93 (58.5) | 156 (64.5) |
| Unknown | 1 (1.4) | 1 (0.3) | |||||||||||
| Age median (IQR) 3 | 31 (22;45) | 29 (23;41) | 31 (27;37) | 47 (33;60) | 29 (24;40) | 25.5 (20;34) | 30 (39;51) | 32 (25;47) | 37 (29;46) | 43 (32;56) | 36 (27;46) | 38 (32;46) | 39 (31;47) |
| Age categories n (%) 15–34 y/o 4 35–50 y/o >50 y/o | 391 (57.2) 164 (24.0) 129 (18.9) | 22 (57.9) 8 (21.1) 8 (21.1) | 29 (70.3) 9 (22.0) 3 (7.3) | 14 (26.4) 14 (26.4) 25 (47.2) | 43 (62.3) 19 (27.5) 7 (10.1) | 17 (77.3) 4 (18.2) 1 (4.6) | 44 (40.4) 37 (33.9) 28 (25.7) | 208 (55.8) 96 (25.7) 69 (18.5) | 553 (47.6) 406 (35.0) 202 (17.4) | 222 (32.4) 241 (35.1) 223 (32.5) | 623 (46.1) 494 (36.6) 234 (17.3) | 62 (39.0) 69 (43.4) 28 (17.6) | 82 (33.9) 112 (46.3) 48 (19.8) |
| Enrollment period n (%) First half Second half | 360 (52.6) 324 (47.4) | 8 (21.1) 30 (78.9) | 19 (46.3) 22 (53.7) | 45 (85.9) 8 (15.1) | 61 (88.4) 8 (11.6) | 9 (40.9) 13 (59.1) | 53 (48.6) 56 (51.4) | 247 (66.2) 126 (37.8) | 787 (67.8) 374 (32.2) | 359 (52.3) 327 (47.7) | 462 (34.2) 889 (65.8) | 52 (32.7) 107 (67.3) | 114 (47.1) 128 (52.9) |
| HCF 5 n | 5 | 2 | 5 (prisons) | 10 | 11 | 1 | 6 | 3 | 9 | 11 | 18 | 14 | 16 |
| Time points n (%) Month 1 Month 2 Month 3 Month 4 Month 5 Month 6 | 684 (100) 671 (98) 662 (97) 653 (95) 644 (94) 639 (93) | 38 (100) 28 (74) 24 (63) 15 (39) 15 (39) 8 (21) | 41 (100) 41 (100) 41 (100) 41 (100) 41 (100) 41 (100) | 53 (100) 53 (100) 52 (98) 52 (98) 49 (92) 46 (87) | 69 (100) 68 (99) 67 (97) 67 (97) 63(91) 57(83) | 22 (100) 20 (91) 19 (86) 19 (86) 19 (86) 19 (86) | 109 (100) 108 (99) 105 (96) 103 (84) 98 (80) 95 (78) | 373 (100) 364 (98) 355 (95) 336 (90) 326 (87) 315 (84) | 1161 (100) 1090 (94) 1003 (86) 947 (82) 909 (78) 885 (76) | 686 (100) 565 (82) 481 (70) 428 (62) 373 (52) 322 (47) | 1351 (100) 1286 (95) 1248 (92) 1204 (89) 1112 (82) 967 (72) | 159 (100) 151 (95) 145 (91) 132 (83) 123 (77) 108 (68) | 242 (100) 235 (97) 216 (89) 190 (79) 172 (71) 144 (60) |
| Doses taken manually registered n (%) | 3135 (3.6) | 3069 (95.1) | 0 (0) | 9721 (57.2) | 3209 (1.9) | 0 (0) | 6080 (12.2) | 0 (0) | 28186 (39.4) | 76891 (43.0) | 2903 (13.6) | 4059 (13.1) | |
| Overall average adherence (planned/taken) | 90% | 81% | 80% | 80% | 81% | 81% | 82% | 84% | 84% | 88% | 86% | 87% | 87% |
| DS-TB 1 Population (n = 4515) | DR-TB 2 Population (n = 473) | ||
|---|---|---|---|
| Projects n (%) | Bangladesh Ethiopia Haiti Kyrgyzstan Namibia Philippines_1 Philippines_2 South Africa Tanzania Uganda Ukraine | 684 (15.1) 38 (0.8) 41 (0.9) 22 (0.5) 373 (8.3) 1161 (25.7) 686 (15.2) 1351 (29.9) 159 (3.5) | 122 (25.8) 109 (23.0) 242 (51.2) |
| DAT 3 type n (%) | 99DOTS evriMED VOT 4 | 2468 (64.5) 1320 (34.5) 41 (1.1) | 295 (62.4) 178 (37.6) |
| Sex n (%) | Female Male Unknown | 1389 (36.3) 2439 (63.7) 1 (0.0) | 176 (37.2) 296 (62.6) 1 (0.2) |
| Age median (IQR) 5 | 35 (27;46) | 38 (30;49) | |
| Age categories n (%) | 15–34 y/o 6 35–50 y/o >50 y/o | 1905 (49.8) 1250 (32.7) 674 (17.6) | 183 (38.7) 182 (38.5) 108 (22.8) |
| Enrollment period n (%) | First half Second half | 1944 (50.8) 1885 (49.2) | 273 (57.7) 200 (42.3) |
| HCF 7 n | 58 | 35 | |
| Time points n (%) | Month 1 Month 2 Month 3 Month 4 Month 5 Month 6 | 3829 (100) 3651 (95) 3497 (91) 3347 (87) 3189 (83) 2982 (78) | 473 (100) 464 (98) 440 (93) 412 (87) 382 (81) 342 (72) |
| Doses taken manually registered n (%) | 120,324 (21.6) | 13,780 (21.9) |
| DS-TB I Population (n = 4515) | DR-TB II Population (n = 473) | ||
|---|---|---|---|
| Overall statement | Increase followed by decrease | Increase followed by decrease | |
| Time trend between months | 1–2 | ↑ ** | ↑ ** |
| 2–3 | ↓ ** | ↑ | |
| 3–4 | ↓ ** | ↓ | |
| 4–5 | ↓ ** | ↓ | |
| 5–6 | ↓ ** | ↓ | |
| Factors | Sex | Males − ** | Males − |
| Age (years) | 15–34 − 35–50 − | 15–34 + 35–50 + | |
| DAT III start date | Second half − ** | Second half + ** | |
| DAT type | evriMED + | VOT IV − * | |
| Project | +/− * | +/− * | |
| Time patterns between subgroups | Time * sex | Males ↘ * 3,4,5,6 | +/− |
| Time * age | 15–34↘ * 3,4,5,6 | +/− | |
| Time * Enrollment period | Second half ↘ * 2,4,6 | Second half ↗ ** 6 | |
| Time * DAT type | evriMED ↘ ** all | VOT ↘ ** 3,4,5,6 | |
| Time * project | +/− * | +/− * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Groot, L.M.; Straetemans, M.; Maraba, N.; Jennings, L.; Gler, M.T.; Marcelo, D.; Mekoro, M.; Steenkamp, P.; Gavioli, R.; Spaulding, A.; et al. Time Trend Analysis of Tuberculosis Treatment While Using Digital Adherence Technologies—An Individual Patient Data Meta-Analysis of Eleven Projects across Ten High Tuberculosis-Burden Countries. Trop. Med. Infect. Dis. 2022, 7, 65. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed7050065
de Groot LM, Straetemans M, Maraba N, Jennings L, Gler MT, Marcelo D, Mekoro M, Steenkamp P, Gavioli R, Spaulding A, et al. Time Trend Analysis of Tuberculosis Treatment While Using Digital Adherence Technologies—An Individual Patient Data Meta-Analysis of Eleven Projects across Ten High Tuberculosis-Burden Countries. Tropical Medicine and Infectious Disease. 2022; 7(5):65. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed7050065
Chicago/Turabian Stylede Groot, Liza M., Masja Straetemans, Noriah Maraba, Lauren Jennings, Maria Tarcela Gler, Danaida Marcelo, Mirchaye Mekoro, Pieter Steenkamp, Riccardo Gavioli, Anne Spaulding, and et al. 2022. "Time Trend Analysis of Tuberculosis Treatment While Using Digital Adherence Technologies—An Individual Patient Data Meta-Analysis of Eleven Projects across Ten High Tuberculosis-Burden Countries" Tropical Medicine and Infectious Disease 7, no. 5: 65. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed7050065