
Bayesian Network Analysis of Lymphatic Filariasis Serology from Myanmar Shows Benefit of Adding Antibody Testing to Post-MDA Surveillance

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Sample Collection
2.2. Selection of Samples for Testing
2.3. Serological Testing
2.4. Statistical Analysis
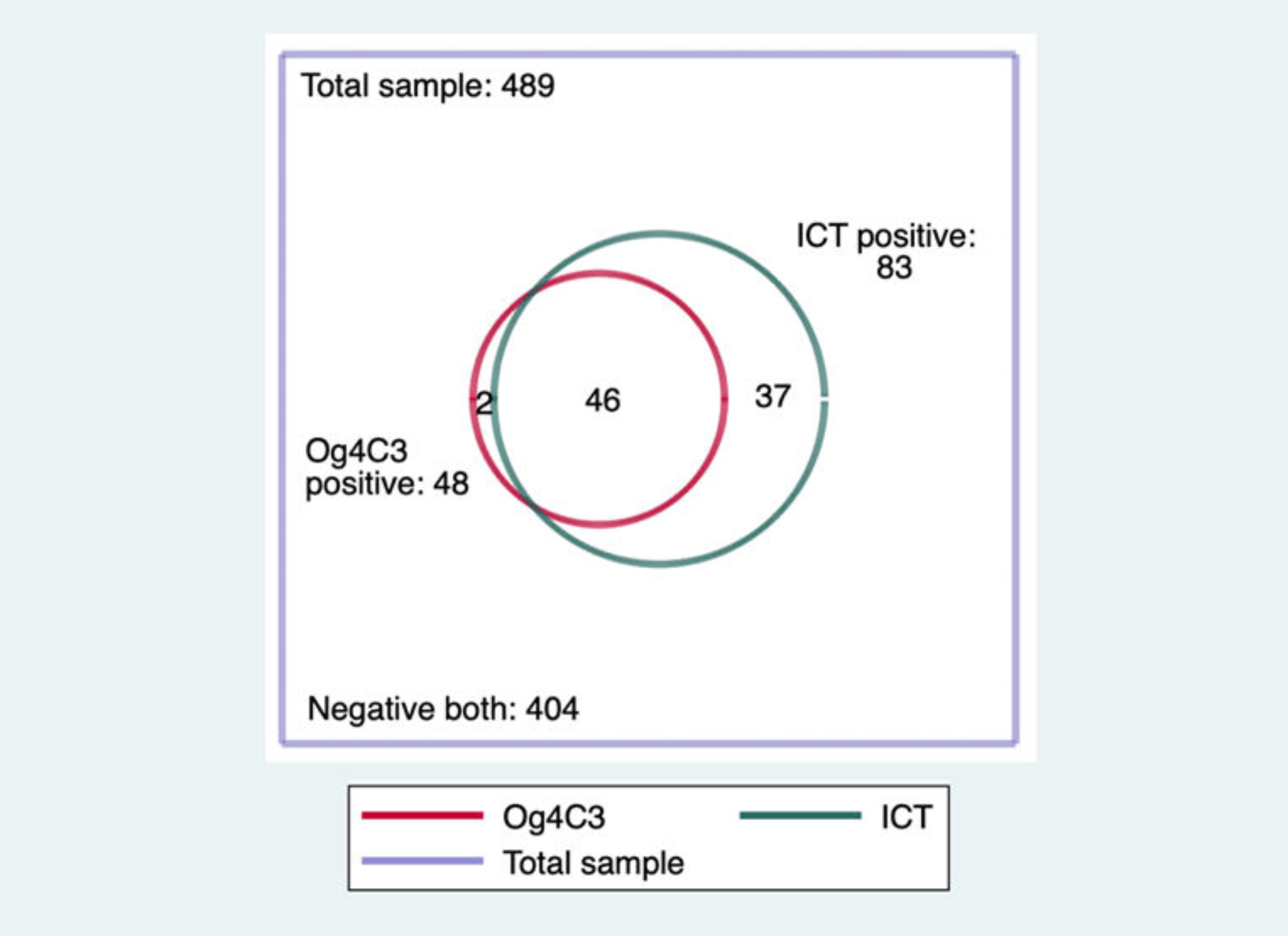
- (1)
- Antigen positive: Since the Og4C3 ELISA done with dried blood spots is less sensitive than ICT (see above), the definition of “antigen positive” was “positivity for ICT and/or Og4C3”.
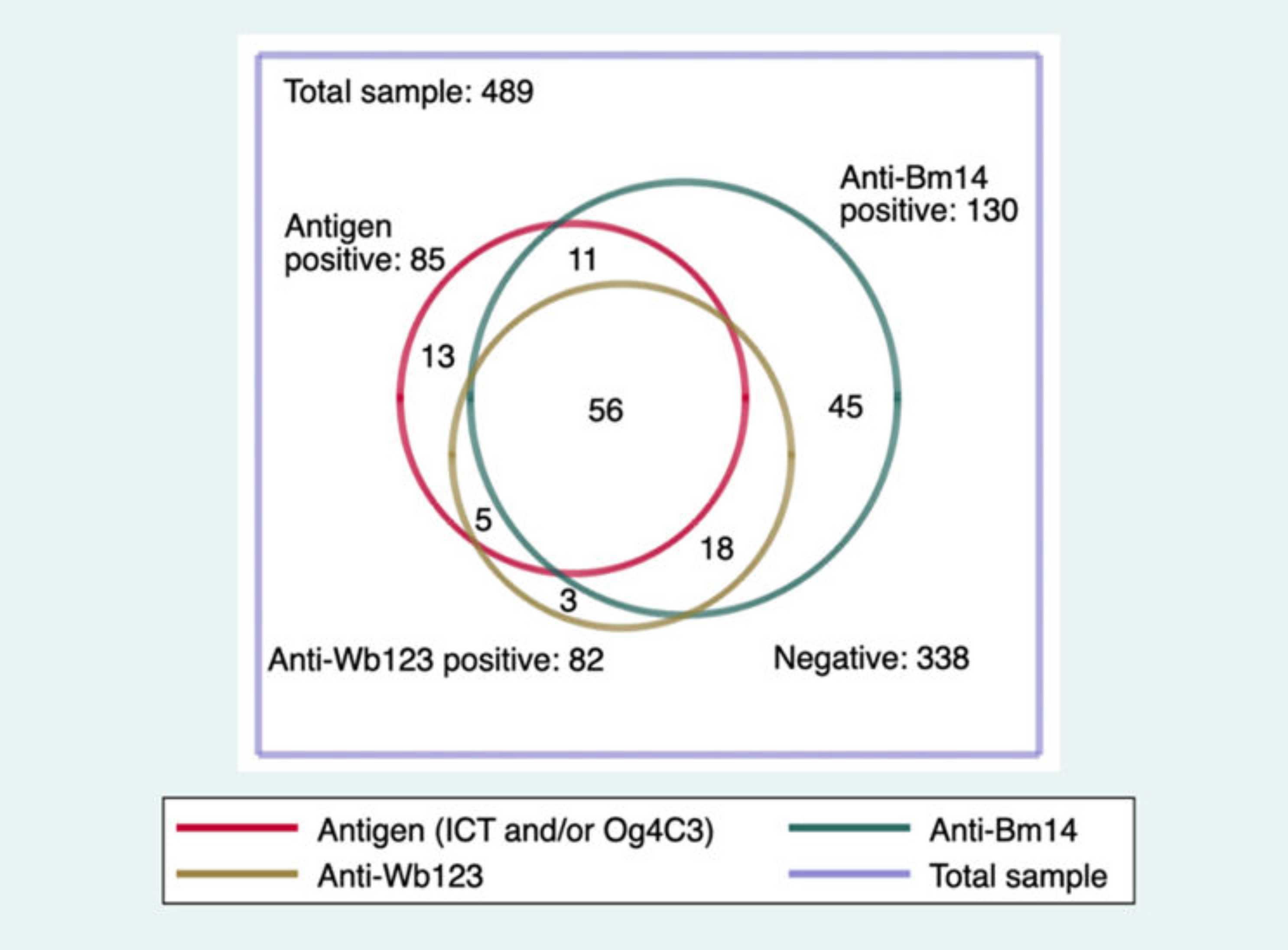
- (2)
- Antibody positive: samples positive for either or both Bm14 and Wb123 antibody was defined as “antibody positive”.
- (3)
- Any infection marker positive: samples positive for at least one marker (antigen or either antibody) was defined as “any positive”.
- (4)
- Missed positive: A “missed positive” was defined as a sample that had a negative result but was positive for one or more alternate markers.
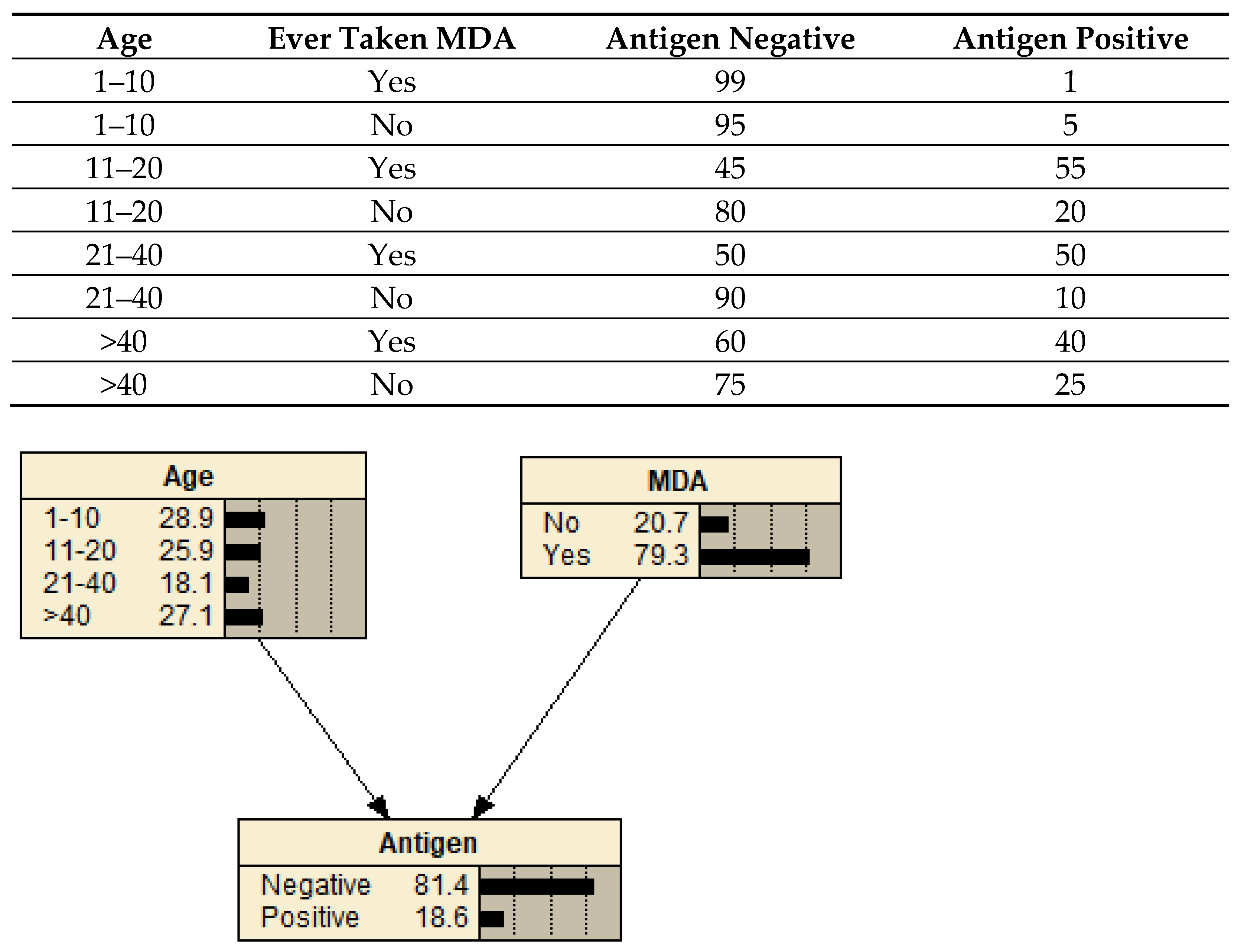
2.5. Bayesian Network Analysis
2.5.1. Bayesian Networks
2.5.2. Network Design
2.5.3. Network Testing
2.5.4. Scenario Analysis
3. Results
3.1. Infection Marker Positivity in the Overall Sample
3.2. Consumption of MDA Medication in the Overall Sample
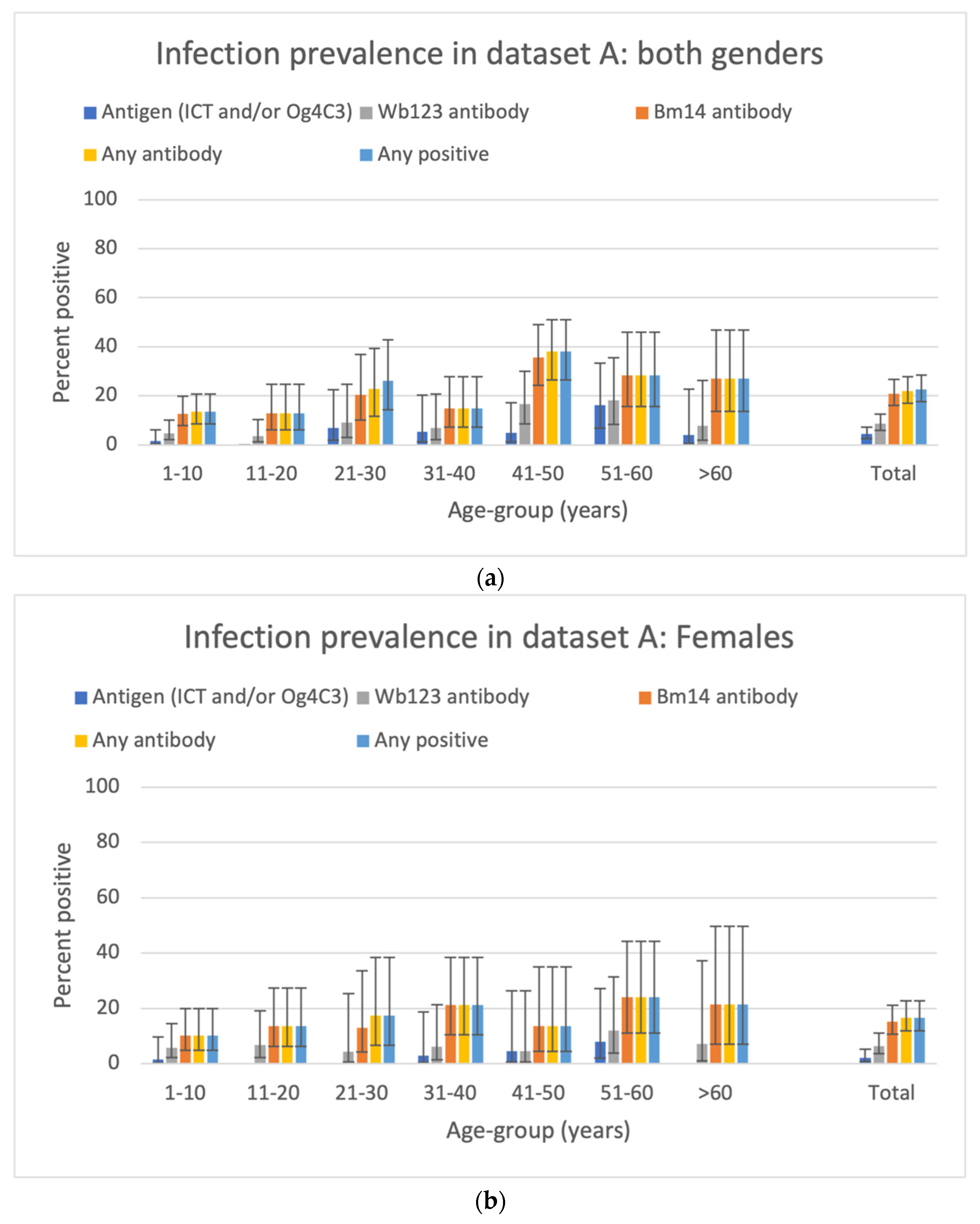
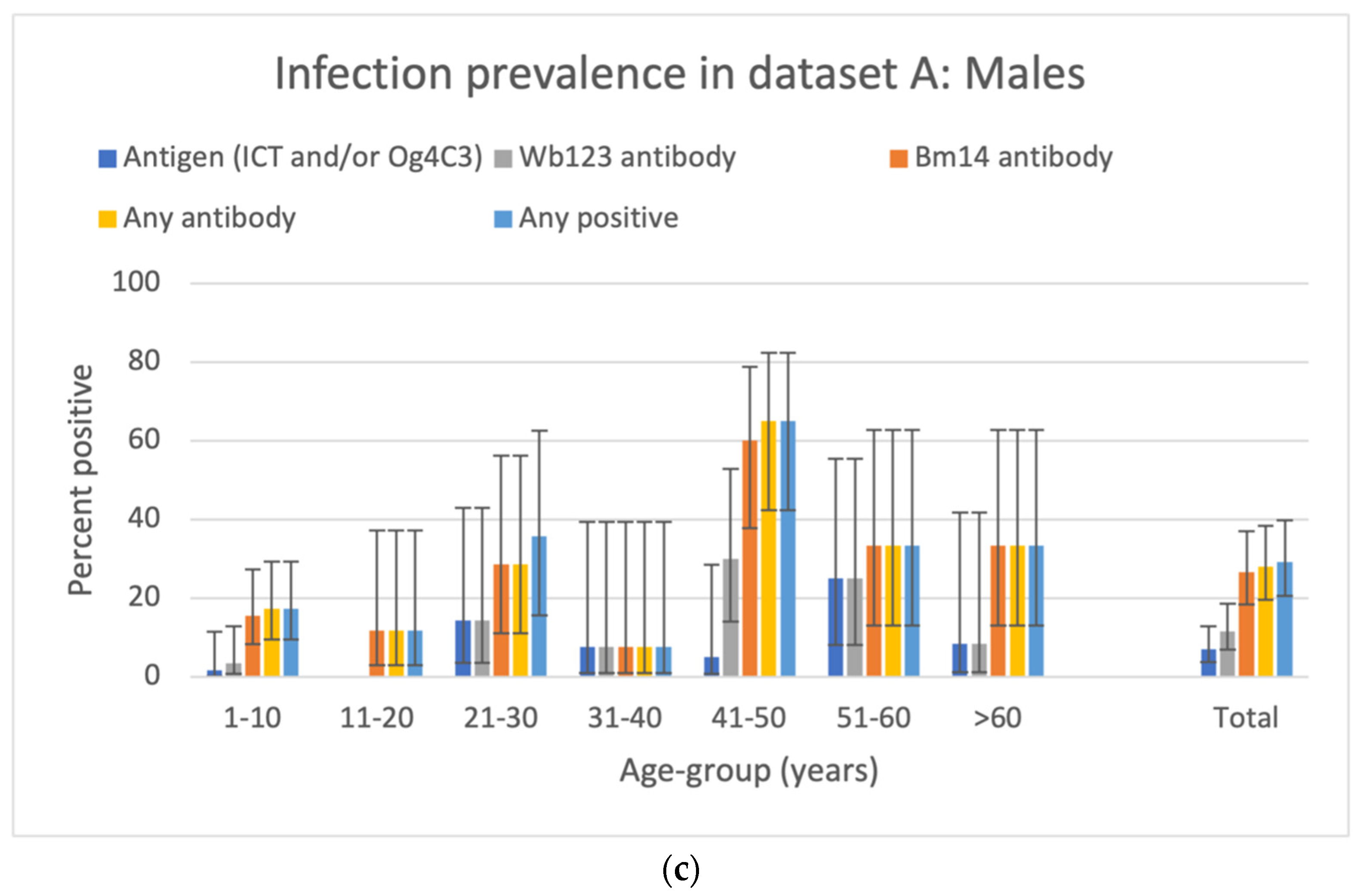
3.3. Prevalence of Antigen and Antibody in the SET A Samples
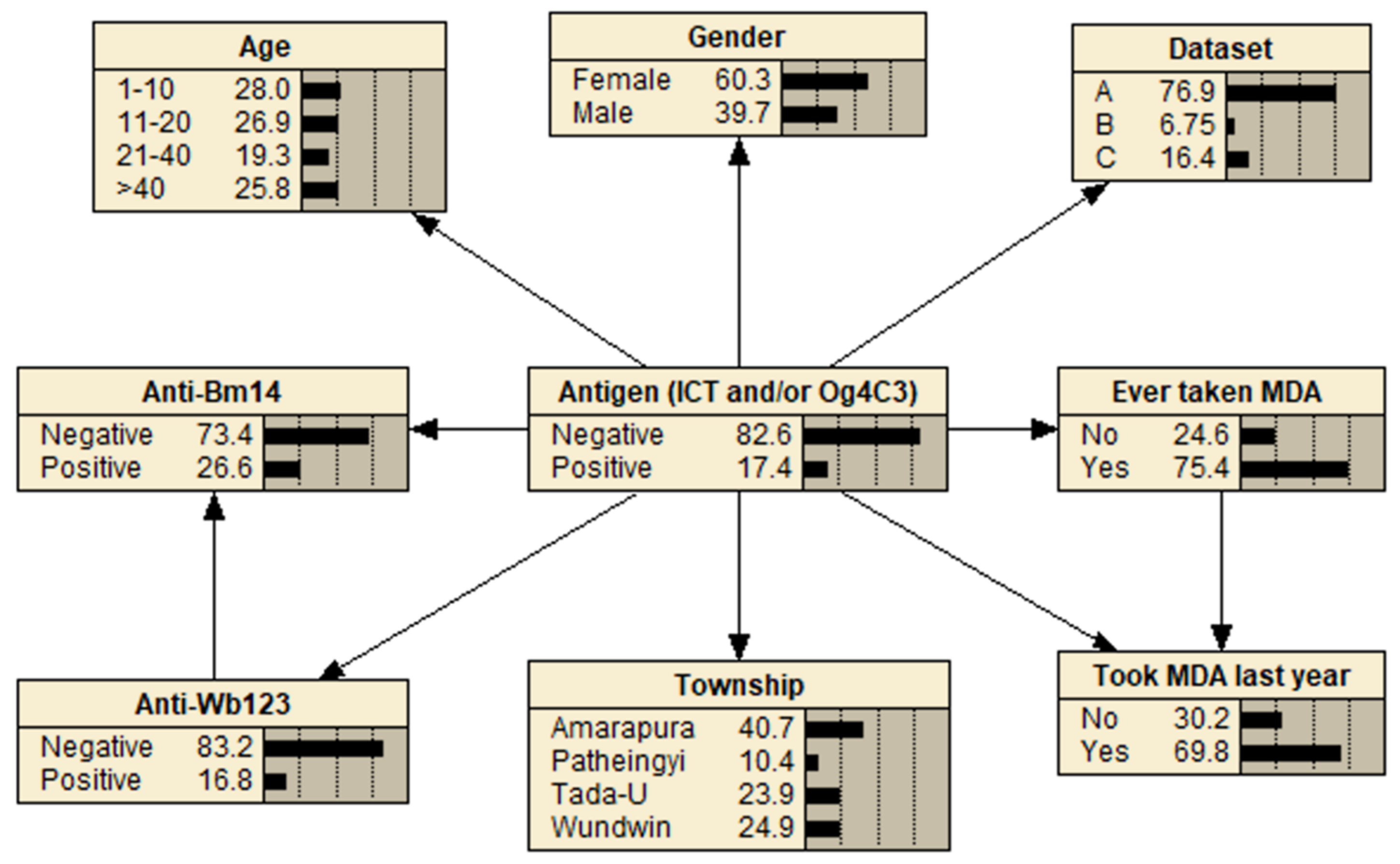
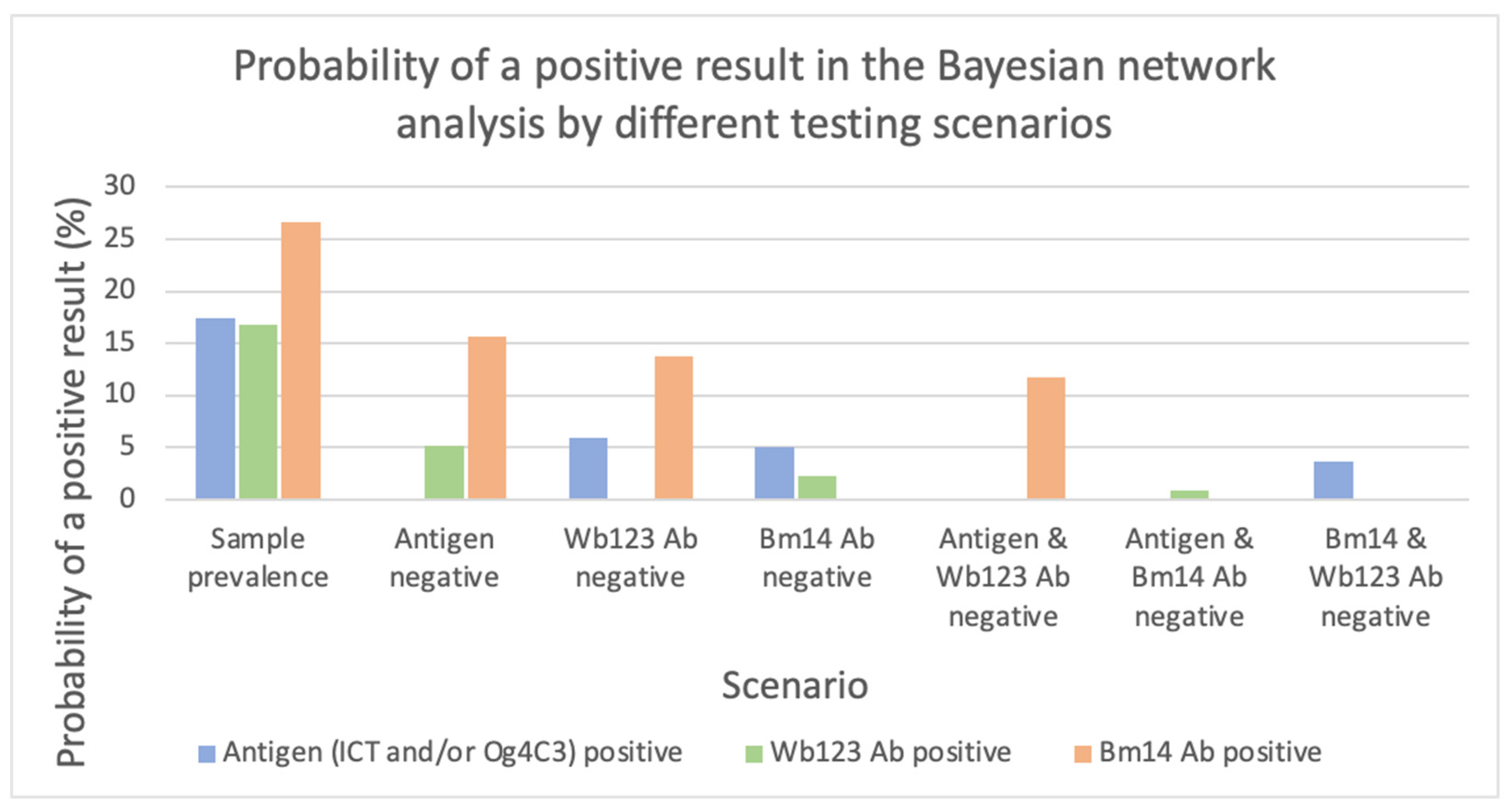
3.4. Bayesian Network Analysis for SETS A, B and C Combined
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Global programme to eliminate lymphatic filariasis: Progress report, 2020. Wkly. Epidemiol. Rec. 2021, 41, 497–508. [Google Scholar]
- WHO. Global Programme to Eliminate Lymphatic Filariasis. In Monitoring and Epidemiological Assessment of Mass Drug Administration; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- WHO. Validation of Elimination of Lymphatic Filariasis as a Public Health Problem; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Pastor, A.F.; Silva, M.R.; Dos Santos, W.J.T.; Rego, T.; Brandao, E.; de-Melo-Neto, O.P.; Rocha, A. Recombinant antigens used as diagnostic tools for lymphatic filariasis. Parasit Vectors 2021, 14, 474. [Google Scholar] [CrossRef] [PubMed]
- More, S.J.; Copeman, D.B. A highly specific and sensitive monoclonal antibody-based ELISA for the detection of circulating antigen in bancroftian filariasis. Trop. Med. Parasitol. 1990, 41, 403–406. [Google Scholar] [PubMed]
- Masson, J.; Douglass, J.; Roineau, M.; Aye, K.S.; Htwe, K.M.; Warner, J.; Graves, P.M. Relative Performance and Predictive Values of Plasma and Dried Blood Spots with Filter Paper Sampling Techniques and Dilutions of the Lymphatic Filariasis Og4C3 Antigen ELISA for Samples from Myanmar. Trop. Med. Infect. Dis. 2017, 2, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berg Soto, A.; Xu, Z.; Wood, P.; Sanuku, N.; Robinson, L.J.; King, C.L.; Tisch, D.; Susapu, M.; Graves, P.M. Combining different diagnostic studies of lymphatic filariasis for risk mapping in Papua New Guinea: A predictive model from microfilaraemia and antigenaemia prevalence surveys. Trop. Med. Health 2018, 46, 41. [Google Scholar] [CrossRef] [PubMed]
- Hamlin, K.L.; Moss, D.M.; Priest, J.W.; Roberts, J.; Kubofcik, J.; Gass, K.; Streit, T.G.; Nutman, T.B.; Eberhard, M.L.; Lammie, P.J. Longitudinal monitoring of the development of antifilarial antibodies and acquisition of Wuchereria bancrofti in a highly endemic area of Haiti. PLoS Negl. Trop. Dis. 2012, 6, e1941. [Google Scholar] [CrossRef] [Green Version]
- Lau, C.L.; Sheel, M.; Gass, K.; Fuimaono, S.; David, M.C.; Won, K.Y.; Sheridan, S.; Graves, P.M. Potential strategies for strengthening surveillance of lymphatic filariasis in American Samoa after mass drug administration: Reducing ‘number needed to test’ by targeting older age groups, hotspots, and household members of infected persons. PLoS Negl. Trop. Dis. 2021, 14, e0008916. [Google Scholar] [CrossRef]
- King, C.L.; Weil, G.J.; Kazura, J.W. Single-Dose Triple-Drug Therapy for Wuchereria bancrofti-5-Year Follow-up. N. Engl. J. Med. 2020, 382, 1956–1957. [Google Scholar] [CrossRef]
- Dickson, B.F.R.; Graves, P.M.; McBride, W.J. Lymphatic Filariasis in Mainland Southeast Asia: A Systematic Review and Meta-Analysis of Prevalence and Disease Burden. Trop. Med. Infect. Dis. 2017, 2, 32. [Google Scholar] [CrossRef] [Green Version]
- Bizhani, N.; Hashemi Hafshejani, S.; Mohammadi, N.; Rezaei, M.; Rokni, M.B. Lymphatic filariasis in Asia: A systematic review and meta-analysis. Parasitol. Res. 2021, 120, 411–422. [Google Scholar] [CrossRef]
- Ramaiah Kapa, D.; Mohamed., A.J. Progress and impact of 20 years of a lymphatic filariasis elimination programme in South-East Asia. Int. Health 2021, 13, S17–S21. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization, Regional Office for South-East Asia. Towards Eliminating Lymphatic Filariasis: Progress in the South-East Region (2001–2011); World Health Organization, Regional Office for South-East Asia: New Delhi, India, 2013. [Google Scholar]
- Aye, N.N.; Lin, Z.; Lon, K.N.; Linn, N.Y.Y.; Nwe, T.W.; Mon, K.M.; Ramaiah, K.; Betts, H.; Kelly-Hope, L.H. Mapping and modelling the impact of mass drug adminstration on filariasis prevalence in Myanmar. Infect. Dis. Poverty 2018, 7, 56. [Google Scholar] [CrossRef] [PubMed]
- UNDP; World Bank; WHO Special Programme for Research and Training in Tropical Diseases; WHO-UNICEF Joint Programme for Health Mapping; World Health Organization Division of Tropical Diseases. Research on Rapid Geographical Assessment of Bancroftian Filariasis; World Health Organization: Geneva, Switzerland, 1998. [Google Scholar]
- Win, K.M.; Tripathy, J.P.; Maung, T.M.; Oo, T.; Thi, A.; Lon, K.N.; Lin, Z. Rapid progress towards elimination of lymphatic filariasis in endemic regions of Myanmar as a result of 16 years of anti-filarial activities (2001–2016). Trop. Med. Health 2018, 46, 14. [Google Scholar] [CrossRef] [PubMed]
- de Meillon, B.; Grab, B.; Sebastian, A. Evaluation of Wuchereria bancrofti infection in Culex pipiens fatigans in Rangoon, Burma. Bull. World Health Organ. 1967, 36, 91–100. [Google Scholar] [PubMed]
- Dickson, B.F.R.; Graves, P.M.; Aye, N.N.; Nwe, T.W.; Wai, T.; Win, S.S.; Shwe, M.; Douglass, J.; Bradbury, R.S.; McBride, W.J. The prevalence of lymphatic filariasis infection and disease following six rounds of mass drug administration in Mandalay Region, Myanmar. PLoS Negl. Trop. Dis. 2018, 12, e0006944. [Google Scholar] [CrossRef] [PubMed]
- Dickson, B.F.R.; Graves, P.M.; Aye, N.N.; Nwe, T.W.; Wai, T.; Win, S.S.; Shwe, M.; Douglass, J.; Wood, P.; Wangdi, K.; et al. Risk factors for lymphatic filariasis and mass drug administration non-participation in Mandalay Region, Myanmar. Parasit Vectors 2021, 14, 72. [Google Scholar] [CrossRef] [PubMed]
- Douglass, J.; Graves, P.; Lindsay, D.; Becker, L.; Roineau, M.; Masson, J.; Aye, N.N.; Win, S.S.; Wai, T.; Win, Y.Y.; et al. Lymphatic Filariasis Increases Tissue Compressibility and Extracellular Fluid in Lower Limbs of Asymptomatic Young People in Central Myanmar. Trop. Med. Infect. Dis. 2017, 2, 50. [Google Scholar] [CrossRef] [Green Version]
- Douglass, J.; Dykes, L.; Kelly-Hope, L.; Gordon, S.; Leggat, P.; Aye, N.N.; Win, S.S.; Wai, T.; Win, Y.Y.; Nwe, T.W.; et al. Preventive chemotherapy reverses covert, lymphatic-associated tissue change in young people with lymphatic filariasis in Myanmar. Trop. Med. Int. Health 2019, 24, 463–476. [Google Scholar] [CrossRef]
- Masson, J.; Douglass, J.; Roineau, M.; Aye, K.S.; Htwe, K.M.; Warner, J.; Graves, P.M. Concordance between Plasma and Filter Paper Sampling Techniques for the Lymphatic Filariasis Bm14 Antibody ELISA. Trop. Med. Infect. Dis. 2017, 2, 6. [Google Scholar] [CrossRef] [Green Version]
- Gass, K.; Beau de Rochars, M.V.; Boakye, D.; Bradley, M.; Fischer, P.U.; Gyapong, J.; Itoh, M.; Ituaso-Conway, N.; Joseph, H.; Kyelem, D. A multicenter evaluation of diagnostic tools to define endpoints for programs to eliminate bancroftian filariasis. PLoS Negl. Trop. Dis. 2012, 6, e1479. [Google Scholar] [CrossRef]
- Lau, C.L.; Won, K.Y.; Becker, L.; Soares Magalhaes, R.J.; Fuimaono, S.; Melrose, W.; Lammie, P.J.; Graves, P.M. Seroprevalence and spatial epidemiology of Lymphatic Filariasis in American Samoa after successful mass drug administration. PLoS Negl. Trop. Dis. 2014, 8, e3297. [Google Scholar] [CrossRef] [PubMed]
- Lau, C.L.; Sheridan, S.; Ryan, S.; Roineau, M.; Andreosso, A.; Fuimaono, S.; Tufa, J.; Graves, P.M. Detecting and confirming residual hotspots of lymphatic filariasis transmission in American Samoa 8 years after stopping mass drug administration. PLoS Negl. Trop. Dis. 2017, 11, e0005914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graves, P.M.; Sheridan, S.; Fuimaono, S.; Lau, C.L. Demographic, socioeconomic and disease knowledge factors, but not population mobility, associated with lymphatic filariasis infection in adult workers in American Samoa in 2014. Parasit Vectors 2020, 13, 125. [Google Scholar] [CrossRef] [PubMed]
- Fenton, N.; Neil, M. Risk Assessment and Decision Analysis with Bayesian Networks; CRC Press: New York, NY, USA, 2013. [Google Scholar]
- Lau, C.L.; Mayfield, H.; Lowry, J.H.; Watson, C.H.; Kama, M.; Nilles, E.J.; Smith, C.H. Unravelling infectious disease eco-epidemiology using Bayesian networks and scenario analysis: A case study of leptospirosis in Fiji. Environ. Model. Softw. 2017, 97, 271–286. [Google Scholar] [CrossRef]
- Mayfield, H.J.; Smith, C.S.; Lowry, J.H.; Watson, C.H.; Baker, M.G.; Kama, M.; Nilles, E.J.; Lau, C.L. Predictive risk mapping of an environmentally-driven infectious disease using spatial Bayesian networks: A case study of leptospirosis in Fiji. PLoS Negl. Trop. Dis. 2018, 12, e0006857. [Google Scholar] [CrossRef] [PubMed]
- Prodhan, G.; Fenton, N. Extending the range of COVID-19 risk factors in a Bayesian network model for personalised risk assessment. medRxiv 2020. [Google Scholar] [CrossRef]
- Lau, C.L.; Mayfield, H.J.; Sinclair, J.E.; Brown, S.J.; Waller, M.; Enjeti, A.K.; Baird, A.; Short, K.R.; Mengersen, K.; Litt, J. Risk-benefit analysis of the AstraZeneca COVID-19 vaccine in Australia using a Bayesian network modelling framework. Vaccine 2021, 39, 7429–7440. [Google Scholar] [CrossRef]
- Pitchforth, J.; Mengersen, K. A proposed validation framework for expert elicited Bayesian Networks. Expert Syst. Appl. 2013, 40, 162–167. [Google Scholar] [CrossRef] [Green Version]
- Allouche, O.; Tsoar, A.; Kadmon, R. Assessing the accuracy of species distribution models: Prevalence, kappa and the true skill statistic (TSS). J. Appl. Ecol. 2006, 43, 1223–1232. [Google Scholar] [CrossRef]
- Fielding, A.B.J. A review of methods for the assessment of prediction errors in conservation presence/absence models. Environ. Conserv. 1997, 24, 38–49. [Google Scholar] [CrossRef]
- Michael, E.; Bundy, D.A.; Grenfell, B.T. Re-assessing the global prevalence and distribution of lymphatic filariasis. Parasitology 1996, 112 Pt 4, 409–428. [Google Scholar] [CrossRef] [PubMed]
- Tisch, D.J.; Bockarie, M.J.; Dimber, Z.; Kiniboro, B.; Tarongka, N.; Hazlett, F.E.; Kastens, W.; Alpers, M.P.; Kazura, J.W. Mass drug administration trial to eliminate lymphatic filariasis in Papua New Guinea: Changes in microfilaremia, filarial antigen, and Bm14 antibody after cessation. Am. J. Trop. Med. Hyg. 2008, 78, 289–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dataset | |||
|---|---|---|---|
| Survey 1 | Survey 2 | ||
| A | B | C | |
| Data Characteristics | |||
| Study date | January–March 2015 | January–March 2015 | October 2014 |
| Study type | Representative cross-sectional | Representative cross-sectional | Cohort |
| Study population | Community | Community | Community |
| Participant selection | Household members ≥ 1 y.o | Household members ≥ 1 y.o | 10–21 y.o age- and sex-matched antigen positive and negative |
| Sample selection | ≤ 14 y.o: all ≥15 y.o: age-stratified sample (25%) | All remaining ICT positives | All |
| Participant Characteristics | |||
| Sample size | 376 | 33 | 80 |
| Median age (years) (interquartile range) | 20.5 (9, 43) | 46.5 (35.5, 57) | 15 (12.5, 18.5) |
| Proportion female (%) | 61 | 58 | 58 |
| Township (n) | Amarapura: 94 | Amarapura: 25 | Amarapura: 80 |
| Patheingyi: 50 | Patheingyi: 1 | ||
| Tada-U: 112 | Tada-U: 5 | ||
| Wundwin: 120 | Wundwin: 2 | ||
| Ever taken MDA medication (%) | 81 | 64 | – a |
| Took MDA medication last year (%) | 76 | 61 | 45 |
| Antigen positive (ICT and/or Og4C3) (%) | 3.7 | 100 | 47.5 |
| Wb123 Ab positive (%) | 8.0 | 69.7 | 36.3 |
| Bm14 Ab positive (%) | 18.9 | 69.7 | 45.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dickson, B.F.R.; Masson, J.J.R.; Mayfield, H.J.; Aye, K.S.; Htwe, K.M.; Roineau, M.; Andreosso, A.; Ryan, S.; Becker, L.; Douglass, J.; et al. Bayesian Network Analysis of Lymphatic Filariasis Serology from Myanmar Shows Benefit of Adding Antibody Testing to Post-MDA Surveillance. Trop. Med. Infect. Dis. 2022, 7, 113. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed7070113
Dickson BFR, Masson JJR, Mayfield HJ, Aye KS, Htwe KM, Roineau M, Andreosso A, Ryan S, Becker L, Douglass J, et al. Bayesian Network Analysis of Lymphatic Filariasis Serology from Myanmar Shows Benefit of Adding Antibody Testing to Post-MDA Surveillance. Tropical Medicine and Infectious Disease. 2022; 7(7):113. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed7070113
Chicago/Turabian StyleDickson, Benjamin F. R., Jesse J. R. Masson, Helen J. Mayfield, Khin Saw Aye, Kyi May Htwe, Maureen Roineau, Athena Andreosso, Stephanie Ryan, Luke Becker, Janet Douglass, and et al. 2022. "Bayesian Network Analysis of Lymphatic Filariasis Serology from Myanmar Shows Benefit of Adding Antibody Testing to Post-MDA Surveillance" Tropical Medicine and Infectious Disease 7, no. 7: 113. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed7070113