Transhepatic Vascular Access for Implantation of a Watchman Left Atrial Appendage Closure Device

1
Department of Internal Medicine, Florida Atlantic University, Boca Raton, FL 33486, USA
2
Department of Cardiovascular Diseases, Florida Atlantic University, Boca Raton, FL 33486, USA
3
Tenet Florida & Department of Cardiovascular Diseases, Florida Atlantic University, Boca Raton, FL 33486, USA
*
Author to whom correspondence should be addressed.
Reports 2018, 1(2), 15; https://doi.org/10.3390/reports1020015
Submission received: 31 July 2018
/
Revised: 26 August 2018
/
Accepted: 27 August 2018
/
Published: 6 September 2018
{kind=link}
{kind=link}
{kind=link}
Abstract
:Conventional access through femoral veins may be limited due to tortuosity and venous occlusion secondary to venous thrombosis or congenital anomalies. Another alternative is subclavian veins, but the difficulty in catheter manipulation and stability makes it less favorable in comparison to the transhepatic access for the delivery of the Watchman device.
1. Introduction
The standard treatments for non-valvular atrial fibrillation are rhythm control, heart rate control, and stroke prevention. Prophylactic anticoagulation with warfarin was the gold standard to prevent embolic strokes, but only 50–60% are therapeutically anticoagulated which make effective long-term anticoagulation very challenging. The use of new oral anticoagulant drugs are the alternative to warfarin, but there are bleeding complications associated with them. In 2001 a successful percutaneous implantation of a device to occlude the left atrial appendage (LAA) cavity was done in a patient with non-valvular atrial fibrillation (AF) to prevent embolism [1]. Conventional access through femoral veins may be limited due to occlusions from multiple vascular procedures or complex congenital anatomy. Percutaneous transhepatic access has been described most commonly as an alternative in pediatric cases and for central access [2,3,4,5,6]. In this report, we present a case of successful utilization of percutaneous transhepatic venous route to occlude the left atrial appendage with a Watchman device.
2. Case Report
The patient was an 86-year-old man with a history of multiple subdural hematomas, multiple bilateral deep vein thrombosis (DVT), pulmonary embolus, hypertension, non-rheumatic aortic valve insufficiency, paroxysmal atrial fibrillation (on warfarin, CHADSVASC score 4 and HAS-BLED score 4), and peripheral vascular disease. The patient required discontinuation of his chronic anticoagulation due to recurrent subdural hematomas and was admitted to the hospital for elective implantation of a Watchman left atrial appendage closure device. He was found to have an occluded femoral venous system attributed to multiple DVTs. Due to limited femoral venous access bilaterally, the procedure was abandoned. After a discussion with the patient and obtaining written informed consent, a different method was utilized the following day.
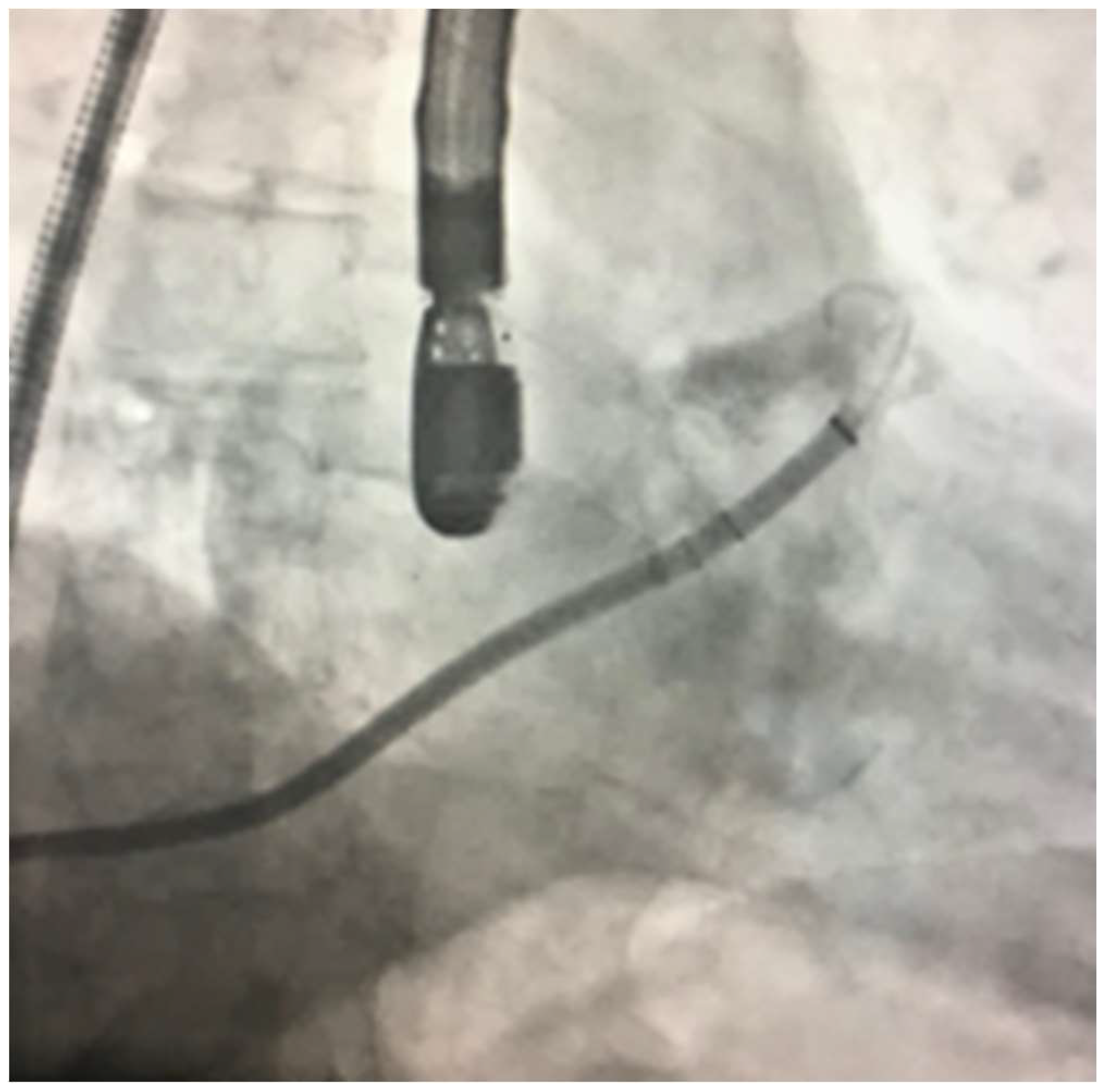
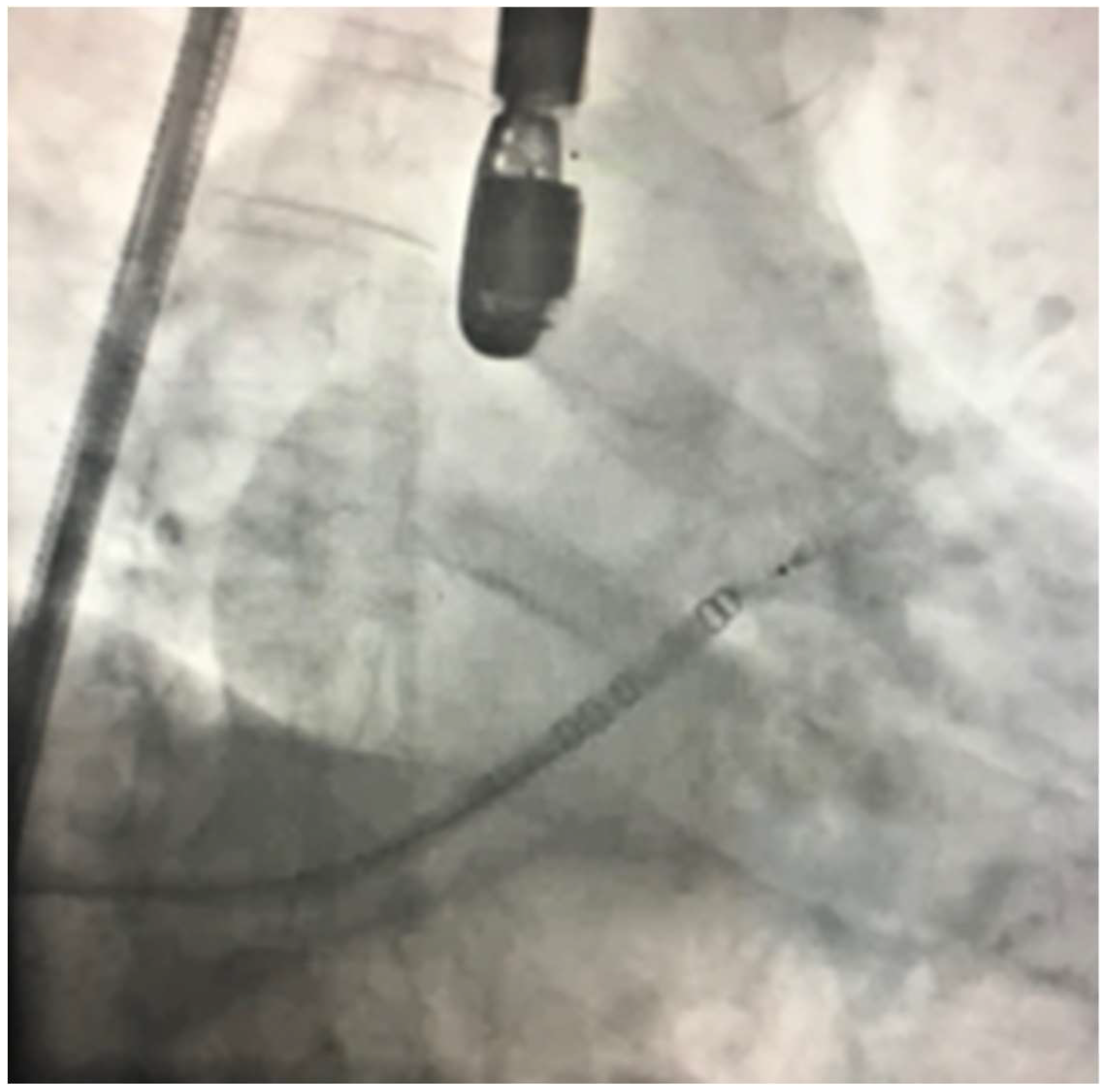
Under strict sterile conditions and general anesthesia, a percutaneous transhepatic puncture was obtained by an interventional radiologist below the right costal margin between the midclavicular and right anterior axillary line. The position and trajectory of the needle were guided by the visualization of the hepatic vein with ultrasound. The needle was advanced with intermittent aspiration and the injection of contrast to visualize entry into the hepatic vein. Once the vein was entered, a guidewire was advanced into the superior vena cava (SVC). Following this, an 8 mm French (8F) sheath was placed into the SVC and was exchanged out for a Baylis wire. (Figure 1) A Baylis trans-septal sheath was then advanced into the SVC, and a radiofrequency Trans-septal needle was advanced using echocardiographic guidance. The Fossa Ovalis was tented. The trans-septal needle was advanced into the left atrium and was exchanged out for a ProTrack wire. At this time, the patient was heparinized to maintain a goal anticoagulation time of greater than 250 s. A 14F double curve sheath was then advanced into the left atrium. A pigtail catheter was utilized and advanced into the left atrial appendage. (Figure 2) The sheath was then advanced into the left atrial appendage, and multiple left atrial appendage angiograms were performed. At this time, a 24 mm Watchman left atrial appendage occlude device was deployed successfully with excellent compression of the device (Figure 3). The 14F delivery sheath was removed without evidence of a new pericardial effusion. At this time, the 14F sheath was replaced with a 14-French dialysis catheter in the transhepatic tunnel. The patient was taken off general anesthesia and was transferred to recovery. The patient was discharged on Aspirin 81 mg and Coumadin 1 mg daily for 45 days then ASA alone. One week follow up was done, and he was found not to have any complications.
3. Discussion
Patients with atrial fibrillation may present with limited femoral venous system access, which may be occluded from prior procedures or have congenitally complex anatomy. Internal jugular or subclavian veins have been utilized as alternative access sites. However, difficulty in catheter manipulation and stability make these approaches less favorable.
Percutaneous transhepatic access has been well utilized in pediatric literature including diagnostic and interventional cardiac catheterizations, pacemaker placement, and electrophysiological procedures, as well as central access for hemodialysis [7,8], total parenteral nutrition [8], and chemotherapy [6,9,10,11,12,13,14,15]. The large caliber of hepatic veins makes them well suited to accommodate sheaths, though the site may offer less compressibility for hemostasis. In addition, it provides maneuverability and optimal stability to approach the right atrium and cross the atrial septum. The reported complication incidence is relatively low (<5%). Intraperitoneal bleeding, subcutaneous hematoma, infection, thrombosis, and pneumothorax are the major reported complications [13,16,17]. As with any other complex procedures, the complications rate depends on the center’s experience and volume.
Careful selection of patients and comprehensive planning are essential for reducing the risk of complications. With the use of anatomical landmarks, ultrasound, and fluoroscopy, successful access can be obtained, and large sheaths can be accommodated under a fully anticoagulated state for such procedures.
Hemostasis can be achieved with a variety of mechanisms, including manual pressure in the right lateral decubitus position, vascular coiling, vascular plugs or gelfoam, and cauterization with radiofrequency (RF) energy [2,8,15]. Regardless of the technique, it is important to leave the closure device within the tract in the direction but outside of the hepatic vein, to reduce the risk of thrombosis and embolization. In our case, a double lumen dialysis catheter was utilized which was removed one week after the procedure. Furthermore, continued close monitoring of coagulation markers and blood cell count in an intensive care unit setting for at least 24 h after the procedure is crucial.
We report the first successful case of utilizing transhepatic access in a Watchman left atrial appendage closure device implantation, which could be done safely in collaboration with an interventional radiologist. This method can be considered as a non-inferior alternative to patients who require Watchman device implantation and have limited femoral vein access.
Author Contributions
All authors contributed extensively to the work presented in case report. R.M. (Ramez Morcos) and H.T. collected the data and drafted the manuscript. P.B. performed the analysis and interpretation. R.M. (Rupesh Manam) performed Revision. B.M. reviewed the manuscript and provided critical Revision.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| LAA | left atrial appendage |
| AF | atrial fibrillation |
| DVT | deep vein thrombosis |
| SVC | superior vena cava |
| RF | radiofrequency |
References
- Wunderlich, N.C.; Beigel, R.; Swaans, M.J.; Ho, S.Y.; Siegel, R.J. Percutaneous interventions for left atrial appendage exclusion: Options, assessment, and imaging using 2D and 3D echocardiography. JACC Cardiovasc. Imaging 2015, 8, 472–488. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.M.; Neuzil, P.; Skoka, J.; Kriz, R.; Popelova, J.; Love, B.A.; Mittnacht, A.J.; Reddy, V.Y. Percutaneous transhepatic venous access for catheter ablation procedures in patients with interruption of the inferior vena cava. Circ. Arrhythm. Electrophysiol. 2011, 4, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, D.T.; Gupta, R.; Kay, J.; Fagan, T.; Lowery, C.; Collins, K.K.; Sauer, W.H. Percutaneous transhepatic access for catheter ablation of cardiac arrhythmias. Europace 2013, 15, 494–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebeid, M.R. Transhepatic vascular access for diagnostic and interventional procedures: Techniques, outcome, and complications. Catheter. Cardiovasc. Interv. 2007, 69, 594–606. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.L.; Fellows, K.E.; Murphy, J.D. Transhepatic central venous access for cardiac catheterization and radiologic intervention. Cathet. Cardiovasc. Diagn. 1995, 35, 168–171. [Google Scholar] [CrossRef] [PubMed]
- Wallace, M.J.; Hovsepian, D.M.; Balzer, D.T. Transhepatic venous access for diagnostic and interventional cardiovascular procedures. J. Vasc. Interv. Radiol. 1996, 7, 579–582. [Google Scholar] [CrossRef]
- Stavropoulos, S.W.; Pan, J.J.; Clark, T.W.; Soulen, M.C.; Shlansky-Goldberg, R.D.; Itkin, M.; Trerotola, S.O. Percutaneous transhepatic venous access for hemodialysis. J. Vasc. Interv. Radiol. 2003, 14, 1187–1190. [Google Scholar] [CrossRef] [PubMed]
- Crummy, A.B.; Carlson, P.; McDermott, J.C.; Andrews, D. Percutaneous transhepatic placement of a Hickman catheter. AJR Am. J. Roentgenol. 1989, 153, 1317–1318. [Google Scholar] [CrossRef] [PubMed]
- Rajappan, K.; Sporton, S.C.; Schilling, R.J. Left atrial tachycardia and inferior vena cava thrombotic occlusion complicating atrial fibrillation ablation successfully treated from the right subclavian vein. Heart 2007, 93, 28. [Google Scholar] [CrossRef] [PubMed]
- Davenport, J.J.; Lam, L.; Whalen-Glass, R.; Nykanen, D.G.; Burke, R.P.; Hannan, R.; Zahn, E.M. The successful use of alternative routes of vascular access for performing pediatric interventional cardiac catheterization. Catheter. Cardiovasc. Interv. 2008, 72, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Emmel, M.; Sreeram, N.; Pillekamp, F.; Boehm, W.; Brockmeier, K. Transhepatic approach for catheter interventions in infants and children with congenital heart disease. Clin. Res. Cardiol. 2006, 95, 329–333. [Google Scholar] [PubMed]
- McLeod, K.A.; Houston, A.B.; Richens, T.; Wilson, N. Transhepatic approach for cardiac catheterisation in children: Initial experience. Heart 1999, 82, 694–696. [Google Scholar] [CrossRef] [PubMed]
- Book, W.M.; Raviele, A.A.; Vincent, R.N. Transhepatic vascular access in pediatric cardiology patients with occlusion of traditional central venous sites. J. Invasive Cardiol. 1999, 11, 341–344. [Google Scholar] [PubMed]
- Punamiya, K.; Beekman, R.H.; Shim, D.; Muller, D.W. Percutaneous transhepatic mitral commissurotomy. Cathet. Cardiovasc. Diagn. 1996, 39, 204–206. [Google Scholar] [CrossRef]
- Shim, D.; Lloyd, T.R.; Cho, K.J.; Moorehead, C.P.; Beekman, R.H., 3rd. Transhepatic cardiac catheterization in children. Evaluation of efficacy and safety. Circulation 1995, 92, 1526–1530. [Google Scholar] [CrossRef] [PubMed]
- Sommer, R.J.; Golinko, R.J.; Mitty, H.A. Initial experience with percutaneous transhepatic cardiac catheterization in infants and children. Am. J. Cardiol. 1995, 75, 1289–1291. [Google Scholar] [CrossRef]
- Erenberg, F.G.; Shim, D.; Beekman, R.H., 3rd. Intraperitoneal hemorrhage associated with transhepatic cardiac catheterization: A report of two cases. Cathet. Cardiovasc. Diagn. 1998, 43, 177–178. [Google Scholar] [CrossRef]
Figure 1.
Advancing 8 mm French (8 fr) sheath into the superior vena cava (SVC).

Figure 2.
Advancing the pig-tail into left atrial appendage (LAA).

Figure 3.
Deploying the Watchman device.

© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Morcos, R.; Al Tahii, H.; Bansal, P.; Manam, R.; Maini, B. Transhepatic Vascular Access for Implantation of a Watchman Left Atrial Appendage Closure Device. Reports 2018, 1, 15. https://0-doi-org.brum.beds.ac.uk/10.3390/reports1020015
AMA Style
Morcos R, Al Tahii H, Bansal P, Manam R, Maini B. Transhepatic Vascular Access for Implantation of a Watchman Left Atrial Appendage Closure Device. Reports. 2018; 1(2):15. https://0-doi-org.brum.beds.ac.uk/10.3390/reports1020015
Chicago/Turabian StyleMorcos, Ramez, Haider Al Tahii, Priya Bansal, Rupesh Manam, and Brijeshwar Maini. 2018. "Transhepatic Vascular Access for Implantation of a Watchman Left Atrial Appendage Closure Device" Reports 1, no. 2: 15. https://0-doi-org.brum.beds.ac.uk/10.3390/reports1020015