Merkel Cell Carcinoma of the Mandible: A Case of Spontaneous Acceleration of the Growth


 ,
, {kind=link}
{kind=link}
Abstract
:1. Introduction
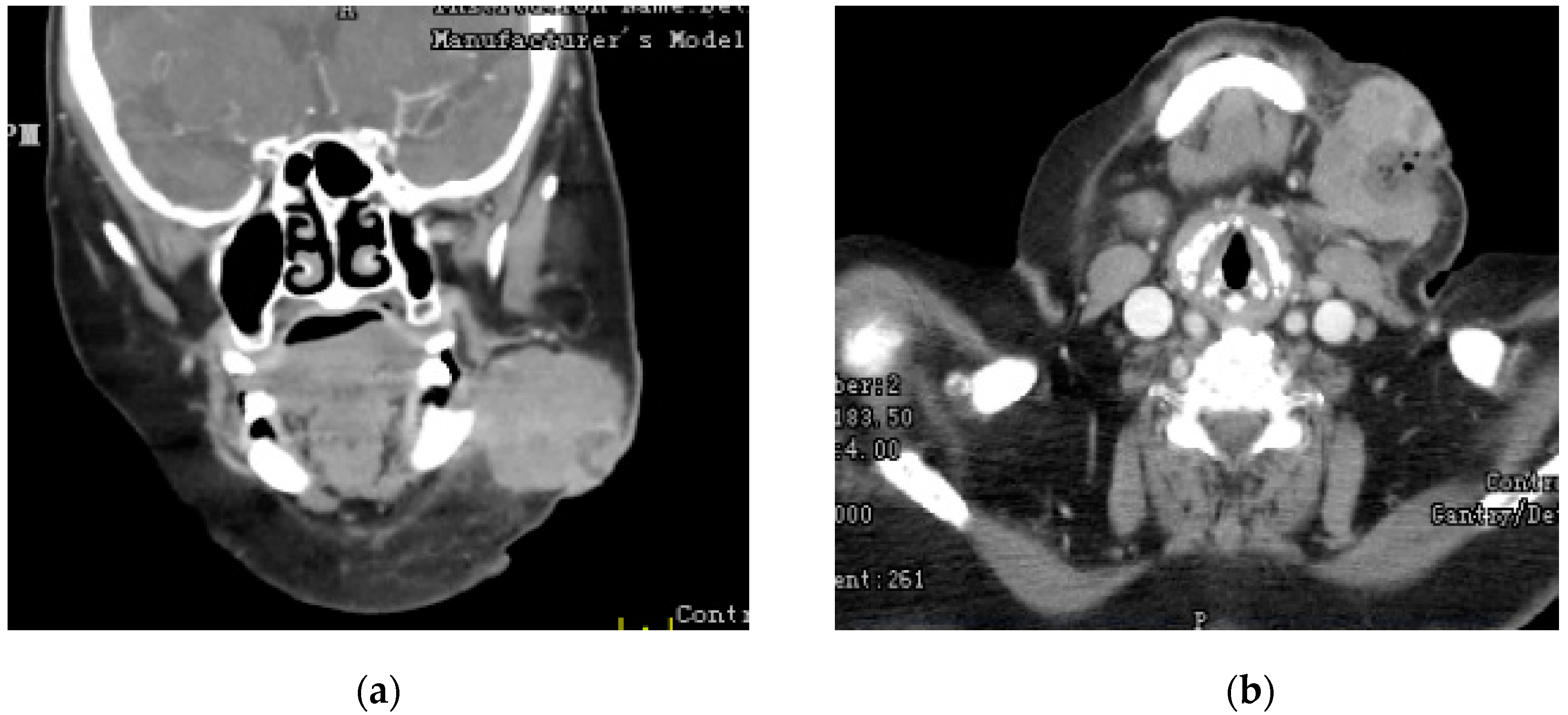
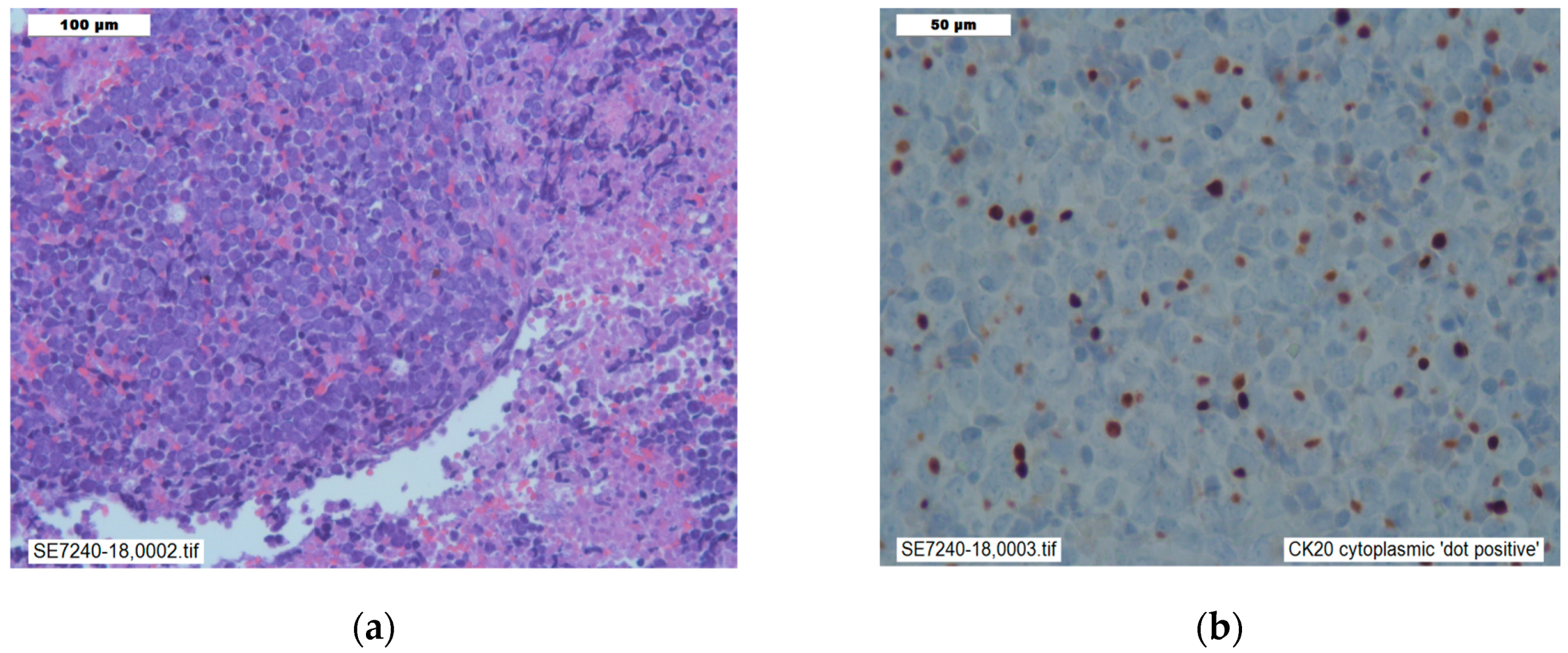
2. Case Presentation Section
3. Discussion
4. Conclusions
Author Contributions
Conflicts of Interest
References
- Feng, H.; Shuda, M.; Chang, Y.; Moore, P.S. Clonal integration of a polyomavirus in human Merkel cell carcinoma. Science 2008, 319, 1096–1100. [Google Scholar] [CrossRef] [PubMed]
- Shuda, M.; Feng, H.; Kwun, H.J.; Rosen, S.T.; Gjoerup, O.; Moore, P.S.; Chang, Y. T antigen mutations are a human tumor-specific signature for Merkel cell polyomavirus. Proc. Natl. Acad. Sci. USA 2008, 105, 16272–16277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houben, R.; Shuda, M.; Weinkam, R.; Schrama, D.; Feng, H.; Chang, Y.; Moore, P.S.; Becker, J.C. Merkel cell polyomavirus-infected Merkel cell carcinoma cells require expression of viral T antigens. J. Virol. 2010, 84, 7064–7072. [Google Scholar] [CrossRef] [PubMed]
- Schrama, D.; Ugurel, S.; Becker, J.C. Merkel cell carcinoma: Recent insights and new treatment options. Curr. Opin. Oncol. 2012, 24, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.Q.; Waldeck, K.; Vergara, I.A.; Schröder, J.; Madore, J.; Wilmott, J.S.; Colebatch, A.J.; De Paoli-Iseppi, R.; Li, J.; Lupat, R.; et al. UV-associated mutations underlie the etiology of MCV-negative Merkel cell carcinomas. Cancer Res. 2015, 75, 5228–5234. [Google Scholar] [CrossRef] [PubMed]
- Bichakjian, C.K.; Lowe, L.; Lao, C.D.; Sandler, H.M.; Bradford, C.R.; Johnson, T.M.; Wong, S.L. Merkel cell carcinoma: Critical review with guidelines for multidisciplinary management. Cancer 2007, 110, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schadendorf, D.; Lebbé, C.; Zur Hausen, A.; Avril, M.F.; Hariharan, S.; Bharmal, M.; Becker, J.C. Merkel cell carcinoma: Epidemiology, prognosis, therapy and unmet medical needs. Eur. J. Cancer 2017, 71, 53–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barksdale, S.K. Advances in Merkel cell carcinoma from a pathologist’s perspective. Pathology 2017, 49, 568–574. [Google Scholar] [CrossRef] [PubMed]
- Heath, M.; Jaimes, N.; Lemos, B.; Mostaghimi, A.; Wang, L.C.; Peñas, P.F.; Nghiem, P. Clinical characteristics of Merkel cell carcinoma at diagnosis in 195 patients: The AEIOU features. J. Am. Acad. Dermatol. 2008, 58, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.N.; Chehal, H.; Smith, M.H.; Islam, S.; Bhattacharyya, I. Merkel cell carcinoma of the buccal mucosa and lower lip. Head Neck Pathol. 2018, 12, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, D.; Accorona, R.; Ungari, M.; Melocchi, L.; Bell, D.; Nicolai, P. Primary Merkel cell carcinoma of the submandibular gland: When CK20 status complicates the diagnosis. Head Neck Pathol. 2015, 9, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Howard, R.A.; Dores, G.M.; Curtis, R.E.; Anderson, W.F.; Travis, L.B. Merkel cell carcinoma and multiple primary cancers. Cancer Epidemiol. Prev. Biomark. 2006, 15, 1545–1549. [Google Scholar] [CrossRef] [PubMed]
- Clarke, C.A.; Robbins, H.A.; Tatalovich, Z.; Lynch, C.F.; Pawlish, K.S.; Finch, J.L.; Hernandez, B.Y.; Fraumeni, J.F., Jr.; Madeleine, M.M.; Engels, E.A. Risk of Merkel cell carcinoma after solid organ transplantation. J. Natl. Cancer Inst. 2015, 107, dju382. [Google Scholar] [CrossRef] [PubMed]
- Shah, I.A.; Netto, D.; Schlageter, M.O.; Muth, C.; Fox, I.; Manne, R.K. Neurofilament immunoreactivity in Merkel-cell tumors: A differentiating feature from small-cell carcinoma. Mod. Pathol. 1993, 6, 3–9. [Google Scholar] [PubMed]
- He, W.; Zhang, D.; Jiang, J.; Chen, Y.; Wu, C. Merkel cell carcinoma in the left groin: A case report and review of the literature. Oncol. Lett. 2015, 9, 1197–1200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, I.S.; Bhatia, S.; Kaufman, H.L.; Lipson, E.J. Immunotherapy for Merkel cell carcinoma: A turning point in patient care. J. Immunother. Cancer 2018, 6, 23. [Google Scholar] [CrossRef] [PubMed]


© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choudhry, M.; Danial, M.; Bolduc, J.; Rizvi, S.A.A.; Rabionet, P.; Westine, J. Merkel Cell Carcinoma of the Mandible: A Case of Spontaneous Acceleration of the Growth. Reports 2019, 2, 21. https://0-doi-org.brum.beds.ac.uk/10.3390/reports2030021
Choudhry M, Danial M, Bolduc J, Rizvi SAA, Rabionet P, Westine J. Merkel Cell Carcinoma of the Mandible: A Case of Spontaneous Acceleration of the Growth. Reports. 2019; 2(3):21. https://0-doi-org.brum.beds.ac.uk/10.3390/reports2030021
Chicago/Turabian StyleChoudhry, Mansoor, Muhammad Danial, James Bolduc, Syed A. A. Rizvi, Pedro Rabionet, and John Westine. 2019. "Merkel Cell Carcinoma of the Mandible: A Case of Spontaneous Acceleration of the Growth" Reports 2, no. 3: 21. https://0-doi-org.brum.beds.ac.uk/10.3390/reports2030021