Management of Descemet’s Membrane Detachment after Cataract Surgery—A Case Series
by
 ,
,
Heng-Chiao Huang
1, 
Ren-Long Jan
2,3,
Sung-Huei Tseng
1,4,
Chia-Yi Lee
5,
Fu-Tsung Wei
1,† and
Yuh-Shin Chang
1,2,*,† 1
Department of Ophthalmology, Chi Mei Medical Center, Tainan 710, Taiwan
2
Graduate Institute of Medical Science, College of Health Science, Chang Jung Christian University, Tainan 711, Taiwan
3
Department of Pediatrics, Chi Mei Medical Center, Liouying, Tainan 736, Taiwan
4
Department of Ophthalmology, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan 701, Taiwan
5
Department of Ophthalmology, Show Chwan Memorial Hospital, Changhua 500, Taiwan
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to this study.
Reports 2020, 3(2), 13; https://0-doi-org.brum.beds.ac.uk/10.3390/reports3020013
Submission received: 25 March 2020
/
Revised: 16 April 2020
/
Accepted: 26 April 2020
/
Published: 27 April 2020
Abstract
:Descemet’s membrane detachment (DMD) is an uncommon, vision-threatening, ocular surface complication of cataract surgery. Among several treatment strategies, sulfur hexafluoride (SF6) descemetopexy is the standard of care. Herein, we report three cases of DMD after cataract surgery managed with SF6 descemetopexy, showing different outcomes. Anatomical success was achieved in cases 1 and 2 while intraocular pressure (IOP) was elevated in case 2. In case 3, despite SF6 descemetopexy, recurrent DMD was observed. Due to persistent corneal edema and possible corneal decompensation in case 3, Descemet’s stripping automated endothelial keratoplasty was performed and a clear graft was found at the final visit. In conclusion, descemetopexy with 20 % SF6 is an effective and safe procedure for repairing DMD in most cases. Pupillary block with elevated IOP is another concern and prophylactic peripheral iridectomy is recommended. For recurrent DMDs, repeat descemetopexy could be considered. However, close monitoring is advocated since secondary management, such as endothelial keratoplasty, may be required.
1. Introduction
Descemet’s membrane (DM) detachment (DMD), first reported in the late 1920s, is an uncommon but vision-threatening complication of cataract surgery [1]. The most common cause of DMD is cataract surgery [1] but other surgeries, such as iridectomy or penetrating keratoplasty, can cause DMD [2]. In cases of less severity, DMD may resolve spontaneously without treatment [3,4]. However, in cases of extensive DMD spreading to the corneal center, early surgical intervention is advocated to prevent corneal edema and decline in visual acuity [5,6].
There are several surgical interventions to manage DMD, including the injection of air, viscoelastic materials or expandable gases into the anterior chamber (AC) and suturing DM to the stroma [7]. Descemetopexy with air was first applied by Spark et al. in 1967 for extensive DMD and showed a good anatomical outcome [8]. However, AC tamponade with non-expansile and expansile gases such as sulfur hexafluoride (SF6) or perfluoropropane (C3F8) has recently gained popularity as a method to avoid fast absorption of air [9]. Zusman first reported SF6 descemetopexy of an intractable DMD in 1987 [10]. Since then, both air and SF6 have been used widely but no strong evidence supports what is the more appropriated gas to deal with DMD. Chaurasia et al. and Singh et al. have suggested air descemetopexy as a safe treatment option for DMD in most patients [11,12]; however, some researchers prefer the long-lasting effect of SF6 descemetopexy [1,13]. Air resolution occurs within 3–4 days and might not be long enough for reattachment of the DM. Repeat descemetopexy to reach fair visual and anatomical outcomes in some cases may indicate the need for longer tamponade [14]. Although SF6 descemetopexy had been proposed as initial management, it has different outcomes. For cases of failed SF6 descemetopexy, further treatment remains controversial and is decided on a case-to-case basis.
Here, we report a case series of three cases of DMD that occurred after cataract surgery and managed with descemetopexy using a single injection of 20% SF6. We analyzed the different conditions of the three patients, including the possible causes of the poor visual outcome with anatomical success in case 1, increased intraocular pressure (IOP) in case 2 and failed descemetopexy that resulted in corneal transplantation in case 3.
2. Materials and Methods
2.1. Ethics Statement
This case series included three eyes of three patients who were diagnosed with DMD after phacoemulsification surgery. Further, the outcomes after descemetopexy with 20% SF6 were evaluated. We received signed informed consent forms from all patients. The cases were of category 4 of the 45 CFR 46.101(b) Categories of Exempt Human Subjects Research, which involves the collection or study of pathological specimens, diagnostic specimens, existing data, documents or records and requires these sources to be publicly available or recorded by the investigator in such a manner that the subjects cannot be identified directly or through identifiers linked to the subjects. Furthermore, the Institutional Review Board approval for the case series was not required as no identifiable information has been included in the paper.
2.2. Measurement Parameters
2.2.1. Best-Corrected Visual Acuity
Autorefraction was performed by experienced technicians. We used illiterate E’s Chart in an auto chart projector (Topcon, Japan) at a 6-m distance for visual acuity measurement. Best-corrected visual acuity (BCVA) was obtained by correcting the refractive error with suitable glasses. We recorded the distant BCVA with a constant numerator of 20 (20 feet) and a variable denominator that was translated from visual acuity in decimal notation (e.g., 20/20 equals to 1.0 in decimal notation).
2.2.2. Slit-Lamp Biomicroscopy
All the patients underwent a comprehensive eye examination with a slit-lamp biomicroscopy (Topcon, Japan), which consists of an intense light source that can narrow light into a slit and biomicroscope. Both the anterior and posterior eye segments were examined. The binocular eyepieces provided the examiner a detailed stereopsis view of the ocular structures. In the case of DMD, the slit lamp can reveal the extent (large area or not), location (peripheral or central) and distance of the DM separation from stromal side and the severity of the corneal edema. The volume of the degraded bubble in AC after descemetopexy was also documented.
2.2.3. Anterior Segment Optical Coherence Tomography
High-speed anterior segment optical coherence tomography (AS-OCT; Optovue, CA, USA) is a noncontact method using a 1310-nm wavelength to provide objective and high-resolution images. The structure of the anterior segment, such as the corneal thickness, DM, anterior chamber depth, lens thickness and chamber angle, can be assessed and quantified. AS-OCT is particularly useful in the detection of early and minimal DMD when the corneal is edematous with poor visualization by slit-lamp biomicroscopy. The area of DMD delineated by slit-lamp biomicroscopy can be confirmed further by AS-OCT before and after intervention.
2.3. Descemetopexy with 20% SF6
The descemetopexy procedure was performed under retrobulbar anesthesia and 5% betaiodine disinfection. A 0.2-mL 20% SF6 injection was administered through a paracentesis via a bevel-up 30-gauge needle with a 1-mL syringe. The entry site was the site where the DM was still attached and filled with 70% of the AC volume. The patient was advised to remain in the supine position. Peripheral iridectomy (PI) was performed using Westcott scissors. The entry wound for the PI was sutured with 10-0 nylon. The procedures were all performed by the same operator in the operating room.
3. Results
3.1. Characteristics of the Patients
The patients’ demographic characteristics, including age, sex and clinical characteristics, including the operated eye, BCVA of the pre-cataract surgery, DMD diagnosis, post-descemetopexy 20% SF6 injection, DMD features and time from surgery to descemetopexy are summarized in Table 1. We described DMD as a either a planar or nonplanar type [15], depending on whether the DM and stroma separation was greater than 1 mm or not and as peripheral or central DMD [16], depending on whether the detachment area involved a visual axis or not, in our cases, on slit-lamp biomicroscopy and AS-OCT. The BCVA at DMD diagnosis of case 2 was not available and the DMD features were evaluated by an experienced operator only because the descemetopexy with 20% SF6 was performed intraoperatively.
3.2. Case 1
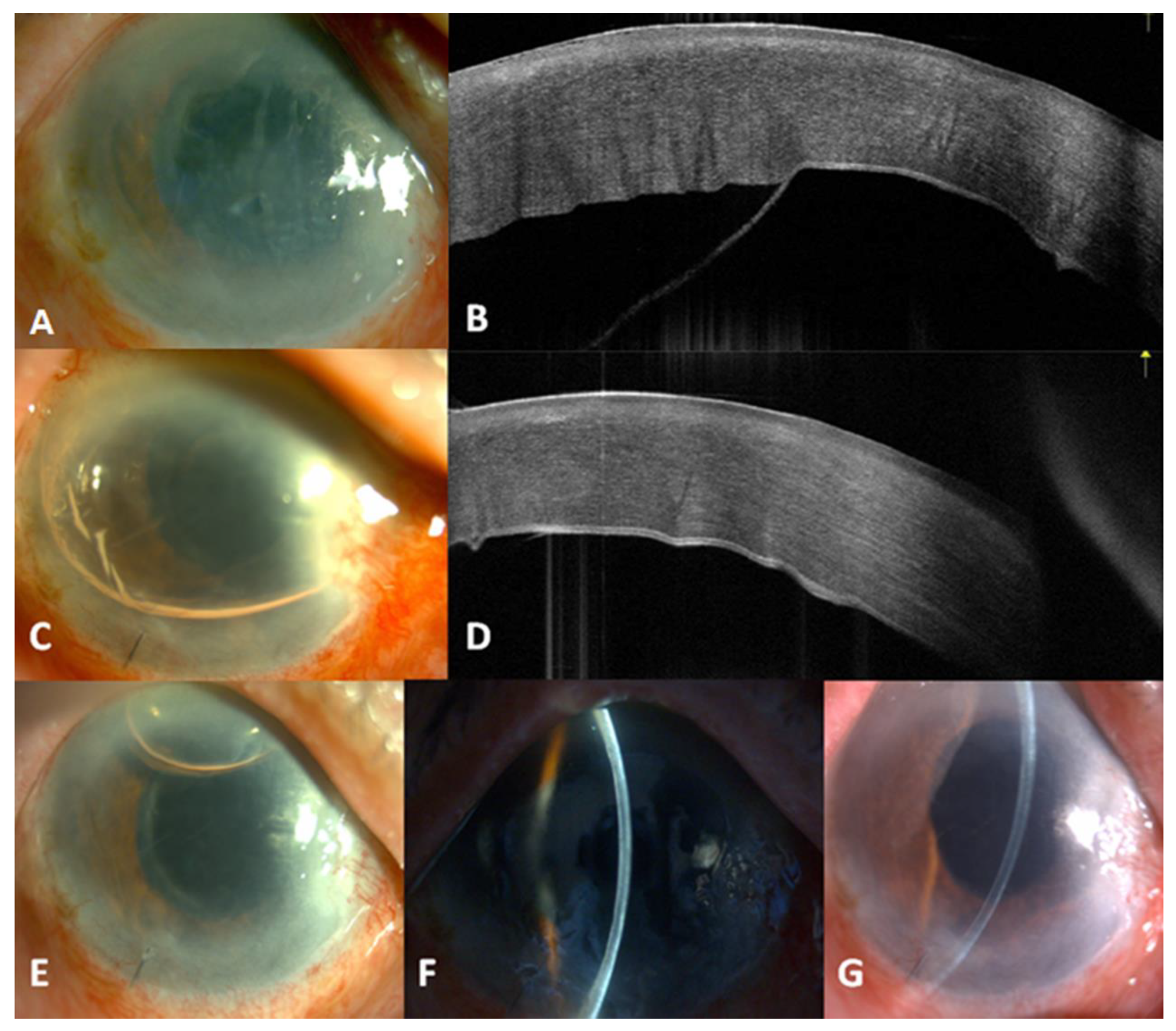
An 81-year-old man, who had undergone a cataract surgery in the right eye 2 weeks before, presented with persistent corneal edema. The BCVA was 20/800 in the right eye. Examination revealed DMD in the central-lower portion with bullous formation (Figure 1A) and AS-OCT showed the same finding (Figure 1B). Descemetopexy with 0.2 mL of 20 % SF6 and PI were performed. One day later, silt-lamp revealed corneal edema regression and AS-OCT showed DM reattachment (Figure 1C,D). Nine days later, the bubbles in AC had disappeared (Figure 1E) and the cystic edema had subsided (Figure 1F). Six months later, BCVA was 20/200 without obvious corneal edema (Figure 1G). The patient was lost to follow-up afterwards.
3.3. Case 2
An 81-year-old woman underwent cataract surgery in the left eye with a preoperative BCVA of 20/60. During the surgery, large and central DMD was noted and descemetopexy with 0.2 mL of 20 % SF6 was performed immediately (Figure 2A). However, the IOP increased to 61 mmHg on the following day despite mannitol infusion and carteolol and brimonidine instillations. Three days after the initial cataract surgery, due to persistent ocular hypertension and suspected pupillary block, PI was performed and AC was partially filled with SF6 to approximately 70 % in volume. The ocular hypertension subsided immediately after the intervention. Ten days later, the gas bubbles had decreased with a well-attached DM (Figure 2B,C) and AS-OCT also showed an attached DM (Figure 2D). Five months later, BCVA improved to 20/30 (Figure 2E) and persisted for 31 postoperative months.
3.4. Case 3
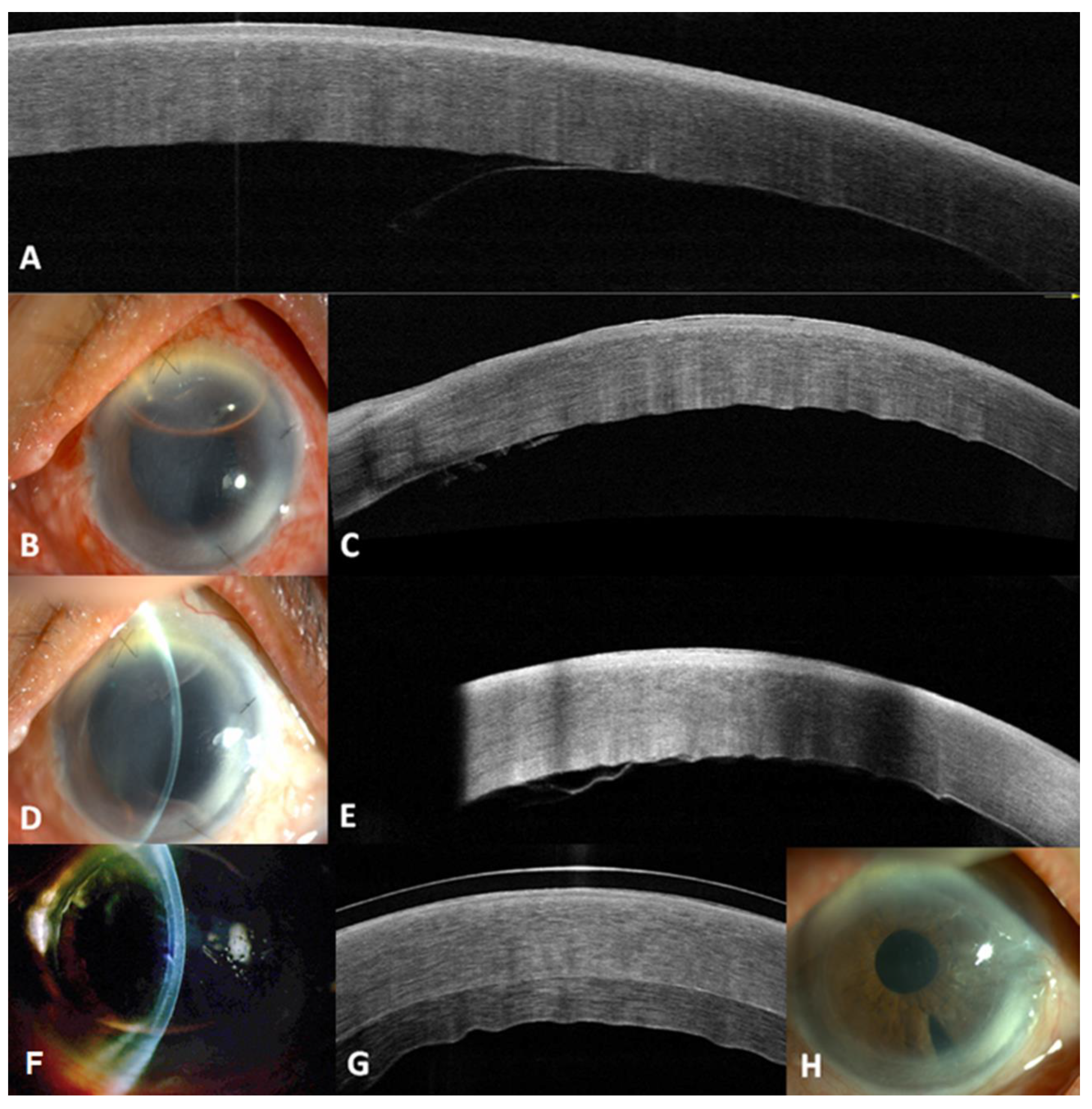
An 82-year-old woman underwent cataract surgery in the left eye with a preoperative BCVA of 20/100. One day later, persistent corneal edema was noted. Three weeks later, BCVA had deteriorated to 20/200 and DMD was found in the nasal portion on AS-OCT (Figure 3A). Descemetopexy with 0.2 mL of 20 % SF6 and PI were performed. Four days later, DM had re-attached and BCVA had improved to 20/50 (Figure 3B,C). One week later, recurrent DMD on the nasal side had developed following gas resolution and BCVA had decreased to 20/100 (Figure 3D,E). Six months after the initial cataract surgery, due to persistent corneal edema and possible loss of DM on the nasal side, Descemet’s stripping automated endothelial keratoplasty (DSAEK) was performed. Five months later, the corneal edema had resolved (Figure 3F) and BCVA had improved to 20/50 (Figure 3G,H). The patient was lost to follow-up afterwards.
4. Discussion
DMD occurs during several ocular surgeries, characterized by a demarcation line and detached DM on slit-lamp biomicroscopy [6,9].Tamponade with the injection of air, SF6 or C3F8 in AC is effective and considered as the standard of care for DMD [1,9,17]. A previous study showed that air descemetopexy was comparable with SF6descemetopexy [18] but the SF6tamponade showed a better outcome than the air tamponade in endothelial keratoplasty and DMD refractory to air descemetopexy [19,20].C3F8descemetopexy illustrated an excellent reattachment rate in DMD [7] but the injection of C3F8 was less favorable because of its greater effect on IOP elevation compared to the injection of SF6 [21]. In this case series, we chose 20 % SF6 descemetopexy for an immediate intervention in patients with DMD.
In 2016, Samarawickrama et al. proposed the classification of DMD into two categories—peripheral and central DMD [16]. The central type was defined as DMD involving the visual axis, whereas the peripheral type was defined as DMD not involving the visual axis. The classification aims to provide clinicians guidance on whether surgical intervention is to be indicated. Peripheral DMD is often treated conservatively, while central DMD is indicated for early surgical intervention. Mackool and Holtz defined planar or nonplanar DMD according to the DM separated from the corneal stroma by less than or greater than 1 mm [15]. They assumed that planar DMD has the possibility of spontaneous reattachment and better prognosis. The nonplanar type should receive early surgical treatment. In our report, cases 1 and 3 had central and nonplanar DMDs. Thus, 20% SF6 descemetopexy was performed. In case 2, DMD occurred intraoperatively and a large area with central detachment was observed. Although case 2 was not examined under slit-lamp biomicroscopy and AS-OCT at diagnosis, a nonplanar type was highly suspected. Immediate SF6 descemetopexy was performed during operation.
In case 1, although DM reattached successfully and corneal edema and macular disease resolved, the BCVA was only 20/400. The poor visual improvement in case 1 may be caused by large, corneal center-involved and nonplanar DMD, which is defined as > 1 mm of detachment with a worse prognosis than the planar type [15]. The degree of endothelial cell trauma resulting from DMD was an indicator of persistent poor visual acuity [16]. A previous study suggested that early surgical intervention may benefit the anatomical success of DMD and prevent scarring of the cornea [22]. The surgical intervention in this case was performed in postoperative week 3 and prolonged surgical intervention is the possible reason for poor vision recovery.
Case 2 had elevated IOP one day after 20% SF6descemetopexy possibly caused by pupillary block and expansible gas. The incidence of postoperative pupillary block was 7.7% in a previous study [14]. To prevent pupillary block and IOP elevation, cycloplegics, prophylactic PI, anti-glaucoma agents or partial filling of gas in AC can be used. Partial air–fluid exchange in AC could be performed to avoid fullness of expansible gases associated with IOP elevation. However, quick absorption of gas bubbles can reduce the efficacy of the tamponade and lead to a failed reattachment. Ocular hypertension and pupillary block in case 2 were possibly caused by no PI and AC filled with gas. PI and AC partially filled with SF6 to approximately 70% in volume could reduce IOP and retain the efficacy of the tamponade in case 2. Due to prompt surgical management, IOP elevation did not compromise the final BCVA. The better prognosis of case 2 may be attributed to its misidentification as nonplanar DMD because of the unavailability of AS-OCT during surgery. However, immediate SF6 descemetopexy in the same operation may play the most important role in the superior visual acuity in case 2.
The initial treatment for DMD was 20% SF6 descemetopexy in the present cases. Case 3 was of recurrent DMD. There is no consensus on steps for the management of recurrent DMD after failed descemetopexy. Repeat injections of gases has been performed for recurrent DMD after the initial descemetopexy [14,23,24]. Jain and Mohan reported that attached DM was achieved with repeat descemetopexy in 12 of 13 cases of recurrent DMD (92.3%) [14]. In a study, 15% of patients developed recurrent DMD, with no significant correlation with age, cataract score, severity of DMD or preoperative visual acuity, which resolved with repeat descemetopxy [23]. In another study, three eyes that required repeat expandable gas injections had more than 50% of corneal involvement and marked separation of DM from the stroma or curling or folding of DM [24]. Case 3 was of large DMD and partial DM loss during cataract surgery was suspected. Therefore, DSAEK was performed instead of repeat descemetopexy.
5. Conclusions
Our case series analyzed the diversity and different outcomes of 20% SF6 descemetopexy in three patients with DMD. Cases with poor visual outcome but attached DM eventually, avoidance of the pupillary block with elevated IOP and management of recurrent DMD were discussed in this study. Application of a new imaging technique for AS-OCT could precisely diagnose, classify and monitor the anatomical outcome, thereby providing guidance in the treatment decision making.
In conclusion, prompt intervention with descemetopexy using 20% SF6 is often effective and safe in repairing DMD, including a large and central DMD. Pupillary block with elevated IOP is a concern, so prophylactic PI is recommended and proper treatment should be timely initiated. Repeat descemetopexy could be considered in cases of recurrent DMD. However, close monitoring is advocated since secondary management, such as endothelial keratoplasty, may be required.
Author Contributions
Conceptualization, H.-C.H., R.-L.J., F.-T.W. and Y.-S.C.; Data curation, H.-C.H. and C.-Y.L.; Formal analysis, H.-C.H., R.-L.J., F.-T.W. and Y.-S.Ch.; Investigation, H.-C.H., R.-L.J., S.-H.T., F.-T.W. and Y.-S.C.; Methodology, H.-C.H., R.-L.J., S.-H.T., F.-T.W. and Y.-S.C.; Project administration, R.-L.J., F.-T.W. and Y.-S.C.; Resources, F.-T.W. and Y.-S.C.; Software, H.-C.H. and C.-Y.L.; Supervision, S.-H.T., F.-T.W. and Y.-S.C.; Validation, R.-L.J., S.-H.T., F.-T.W. and Y.-S.C.; Visualization, H.-C.H. and R.-L.J.; Writing—original draft, H.-C.H. and C.-Y.L.; Writing—review & editing, R.-L.J., S.-H.T., F.-T.W. and Y.-S.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
Data from the Department of Ophthalmology, Chi Mei Medical Center, Tainan 710, Taiwan.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Marcon, A.S.; Rapuano, C.J.; Jones, M.R.; Laibson, P.R.; Cohen, E.J. Descemet’s Membrane Detachment after Cataract Surgery: Management and Outcome. Ophthalmology 2002, 109, 2325–2330. [Google Scholar] [CrossRef]
- Gorski, M.; Shih, C.; Savoie, B.; Udell, I. Spontaneous Descemet Membrane Detachment 20 Years after Penetrating Keratoplasty for Keratoconus. Cornea 2016, 35, 1023–1025. [Google Scholar] [CrossRef] [PubMed]
- Minkovitz, J.B.; Schrenk, L.C.; Pepose, J.S. Spontaneous Resolution of an Extensive Detachment of Descemet’s Membrane Following Phacoemulsification. Arch. Ophthalmol. 1994, 112, 551–552. [Google Scholar] [CrossRef] [PubMed]
- Agraval, U.; Mantry, S.; Ramaesh, K. Inadvertent Detachment of Descemet Membrane and Spontaneous Reattachment Following Cataract Surgery: An Anterior Segment Optical Coherence Tomography (as Oct) Study. Semin. Ophthalmol. 2017, 32, 529–531. [Google Scholar] [CrossRef] [PubMed]
- Chiu, L.Y.; Tseng, H.Y. Descemet’s Membrane Detachment Following Uneventful Phacoemulsification Surgeries: A Case Report. Medicine (Baltimore) 2018, 97, e0444. [Google Scholar] [CrossRef] [PubMed]
- Chow, V.W.; Agarwal, T.; Vajpayee, R.B.; Jhanji, V. Update on Diagnosis and Management of Descemet’s Membrane Detachment. Curr. Opin. Ophthalmol. 2013, 24, 356–361. [Google Scholar] [CrossRef]
- Garg, J.; Mathur, U.; Acharya, M.C.; Chauhan, L. Outcomes of Descemetopexy with Isoexpansile Perfluoropropane after Cataract Surgery. J. Ophthalmic. Vis. Res. 2016, 11, 168–173. [Google Scholar]
- Sparks, G.M. Descemetopexy. Surgical Reattachment of Stripped Descemet’s Membrane. Arch. Ophthalmol. 1967, 78, 31–34. [Google Scholar] [CrossRef]
- Benatti, C.A.; Tsao, J.Z.; Afshari, N.A. Descemet Membrane Detachment during Cataract Surgery: Etiology and Management. Curr. Opin. Ophthalmol. 2017, 28, 35–41. [Google Scholar] [CrossRef]
- Zusman, N.B.; Waring, G.O., 3rd; Najarian, L.V.; Wilson, L.A. Sulfur Hexafluoride Gas in the Repair of Intractable Descemet’s Membrane Detachment. Am. J. Ophthalmol. 1987, 104, 660–662. [Google Scholar] [CrossRef]
- Chaurasia, S.; Ramappa, M.; Garg, P. Outcomes of Air Descemetopexy for Descemet Membrane Detachment after Cataract Surgery. J. Cataract Refract. Surg. 2012, 38, 1134–1139. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Satya, P.S.; Mayank, S.; Basant, K.S.; Swarnima, A. To Study the Efficacy of Air Descemetopexy in the Management of Various Types of Descemet Membrane Detachment Based on Anterior Segment—Optical Coherence Tomography & to Know the Role of Other Gases Perfluoropropane (14% C3f8) and Sulphur Hexafluoride (20% Sf6) in Failed Cases of Air Descemetopexy. IP Int. J. Ocul. Oncol. Oculoplasty 2019, 5, 124–129. [Google Scholar]
- Gault, J.A.; Raber, I.M. Repair of Descemet’s Membrane Detachment with Intracameral Injection of 20% Sulfur Hexafluoride Gas. Cornea 1996, 15, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Jain, R.; Mohan, N. Outcomes of Repeat Descemetopexy in Post-Cataract Surgery Descemet Membrane Detachment. Am. J. Ophthalmol. 2014, 157, 571–575. [Google Scholar] [CrossRef]
- Mackool, R.J.; Holtz, S.J. Descemet Membrane Detachment. Arch. Ophthalmol. 1977, 95, 459–463. [Google Scholar] [CrossRef]
- Samarawickrama, C.; Beltz, J.; Chan, E. Descemet’s Membrane Detachments Post Cataract Surgery: A Management Paradigm. Int. J. Ophthalmol. 2016, 9, 1839–1842. [Google Scholar]
- Shalchi, Z.; O’Brart, D.P.; Ilari, L. Bilateral Descemet Membrane Detachment Following Cataract Surgery. JAMA Ophthalmol. 2013, 131, 533–535. [Google Scholar] [CrossRef] [Green Version]
- Odayappan, A.; Shivananda, N.; Ramakrishnan, S.; Krishnan, T.; Nachiappan, S.; Krishnamurthy, S. A Retrospective Study on the Incidence of Post-Cataract Surgery Descemet’s Membrane Detachment and Outcome of Air Descemetopexy. Br. J. Ophthalmol. 2018, 102, 182–186. [Google Scholar] [CrossRef]
- Marques, R.E.; Guerra, P.S.; Sousa, D.C.; Ferreira, N.P.; Goncalves, A.I.; Quintas, A.M.; Rodrigues, W. Sulfur Hexafluoride 20% Versus Air 100% for Anterior Chamber Tamponade in Dmek: A Meta-Analysis. Cornea 2018, 37, 691–697. [Google Scholar] [CrossRef]
- Kansal, S.; Sugar, J. Consecutive Descemet Membrane Detachment after Successive Phacoemulsification. Cornea 2001, 20, 670–671. [Google Scholar] [CrossRef]
- Modi, A.; Giridhar, A.; Gopalakrishnan, M. Sulfurhexafluoride (Sf6) Versus Perfluoropropane (C3f8) Gas as Tamponade in Macular Hole Surgery. Retina 2017, 37, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Kumar, D.A.; Agarwal, A.; Sivanganam, S.; Chandrasekar, R. Height-, Extent-, Length-, and Pupil-Based (Help) Algorithm to Manage Post-Phacoemulsification Descemet Membrane Detachment. J. Cataract Refract. Surg. 2015, 41, 1945–1953. [Google Scholar] [CrossRef] [PubMed]
- Jain, R.; Murthy, S.I.; Basu, S.; Ali, M.H.; Sangwan, V.S. Anatomic and Visual Outcomes of Descemetopexy in Post-Cataract Surgery Descemet’s Membrane Detachment. Ophthalmology 2013, 120, 1366–1372. [Google Scholar] [CrossRef] [PubMed]
- Sukhija, J.; Ram, J.; Kaushik, S.; Gupta, A. Descemet’s Membrane Detachment Following Phacoemulsification. Ophthalmic Surg. Lasers Imaging 2010, 41, 512–517. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Clinical appearance of the first patient (case 1). (A) The detached Descemet’s membrane on silt-lamp biomicroscopy. (B) The detached Descemet’s membrane on anterior segment optical coherence tomography. (C) The anterior chamber after descemetopexy on silt-lamp biomicroscopy. (D) The anterior chamber after descemetopexy on anterior segment optical coherence tomography. (E) A degraded bubble in the anterior chamber. (F) Decreased cystic edema. (G) The final appearance of the attached Descemet’s membrane on silt-lamp biomicroscopy.
Figure 1.
Clinical appearance of the first patient (case 1). (A) The detached Descemet’s membrane on silt-lamp biomicroscopy. (B) The detached Descemet’s membrane on anterior segment optical coherence tomography. (C) The anterior chamber after descemetopexy on silt-lamp biomicroscopy. (D) The anterior chamber after descemetopexy on anterior segment optical coherence tomography. (E) A degraded bubble in the anterior chamber. (F) Decreased cystic edema. (G) The final appearance of the attached Descemet’s membrane on silt-lamp biomicroscopy.

Figure 2.
Clinical appearance of the second patient (case 2). (A) The anterior chamber one day after descemetopexy on silt-lamp biomicroscopy. (B,C) A degraded bubble in the anterior chamber. (D) The attached Descemet’s membrane on anterior segment optical coherence tomography. (E) The attached Descemet’s membrane on silt-lamp biomicroscopy five months after descemetopexy.
Figure 2.
Clinical appearance of the second patient (case 2). (A) The anterior chamber one day after descemetopexy on silt-lamp biomicroscopy. (B,C) A degraded bubble in the anterior chamber. (D) The attached Descemet’s membrane on anterior segment optical coherence tomography. (E) The attached Descemet’s membrane on silt-lamp biomicroscopy five months after descemetopexy.

Figure 3.
Clinical appearance of the third patient (case 3). (A) The detached Descemet’s membrane on anterior segment optical coherence tomography. (B) The anterior chamber after descemetopexy on silt-lamp biomicroscopy. (C) The anterior chamber after descemetopexy on anterior segment optical coherence tomography. (D) The re-detached Descemet’s membrane on silt-lamp biomicroscopy. (E) The re-detached Descemet’s membrane on anterior segment optical coherence tomography. (F) The re-attached Descemet’s membrane after Descemet’s stripping automated endothelial keratoplasty on silt-lamp biomicroscopy. (G) The re-attached Descemet’s membrane after Descemet’s stripping automated endothelial keratoplasty on anterior segment optical coherence tomography. (H) The final appearance of the attached Descemet’s membrane on silt-lamp biomicroscopy.
Figure 3.
Clinical appearance of the third patient (case 3). (A) The detached Descemet’s membrane on anterior segment optical coherence tomography. (B) The anterior chamber after descemetopexy on silt-lamp biomicroscopy. (C) The anterior chamber after descemetopexy on anterior segment optical coherence tomography. (D) The re-detached Descemet’s membrane on silt-lamp biomicroscopy. (E) The re-detached Descemet’s membrane on anterior segment optical coherence tomography. (F) The re-attached Descemet’s membrane after Descemet’s stripping automated endothelial keratoplasty on silt-lamp biomicroscopy. (G) The re-attached Descemet’s membrane after Descemet’s stripping automated endothelial keratoplasty on anterior segment optical coherence tomography. (H) The final appearance of the attached Descemet’s membrane on silt-lamp biomicroscopy.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Demographics and clinical characteristics of patients with Descemet’s membrane detachment after cataract surgery.
Table 1.
Demographics and clinical characteristics of patients with Descemet’s membrane detachment after cataract surgery.
| Case | Age/Sex | Eye | Surgery | Pre-Cataract Surgery BCVA | BCVA at DMD Diagnosis | DMD Features | Time from Surgery to D-Pexy (D) | Surgical Procedure | Final BCVA |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 81/M | R | Phaco/IOL | 20/200 | 20/800 | Central, nonplanar | 21 | SF6 + PI | 20/200 |
| 2 | 81/F | L | Phaco/IOL | 20/60 | NA | Central, nonplanar | intraoperative | SF6 and then PI | 20/30 |
| 3 | 82/F | L | Phaco/IOL | 20/100 | 20/200 | Central, nonplanar | 22 | SF6+ PI and then DSAEK | 20/50 |
BCVA = best-corrected visual acuity; DMD = Descemet membrane detachment; D-pexy = Descemetopexy; DSAEK = Descemet’s stripping automated endothelial keratoplasty; NA = not available; Phaco/IOL = phacoemulsification and intraocular lens implantation; PI = peripheral iridectomy; SF6 = sulfur hexafluoride.
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Huang, H.-C.; Jan, R.-L.; Tseng, S.-H.; Lee, C.-Y.; Wei, F.-T.; Chang, Y.-S. Management of Descemet’s Membrane Detachment after Cataract Surgery—A Case Series. Reports 2020, 3, 13. https://0-doi-org.brum.beds.ac.uk/10.3390/reports3020013
AMA Style
Huang H-C, Jan R-L, Tseng S-H, Lee C-Y, Wei F-T, Chang Y-S. Management of Descemet’s Membrane Detachment after Cataract Surgery—A Case Series. Reports. 2020; 3(2):13. https://0-doi-org.brum.beds.ac.uk/10.3390/reports3020013
Chicago/Turabian StyleHuang, Heng-Chiao, Ren-Long Jan, Sung-Huei Tseng, Chia-Yi Lee, Fu-Tsung Wei, and Yuh-Shin Chang. 2020. "Management of Descemet’s Membrane Detachment after Cataract Surgery—A Case Series" Reports 3, no. 2: 13. https://0-doi-org.brum.beds.ac.uk/10.3390/reports3020013