
A Case Report of Primordial Odontogenic Tumor That Required Distinction from a Dentigerous Cyst

 ,
,
Abstract
:1. Introduction
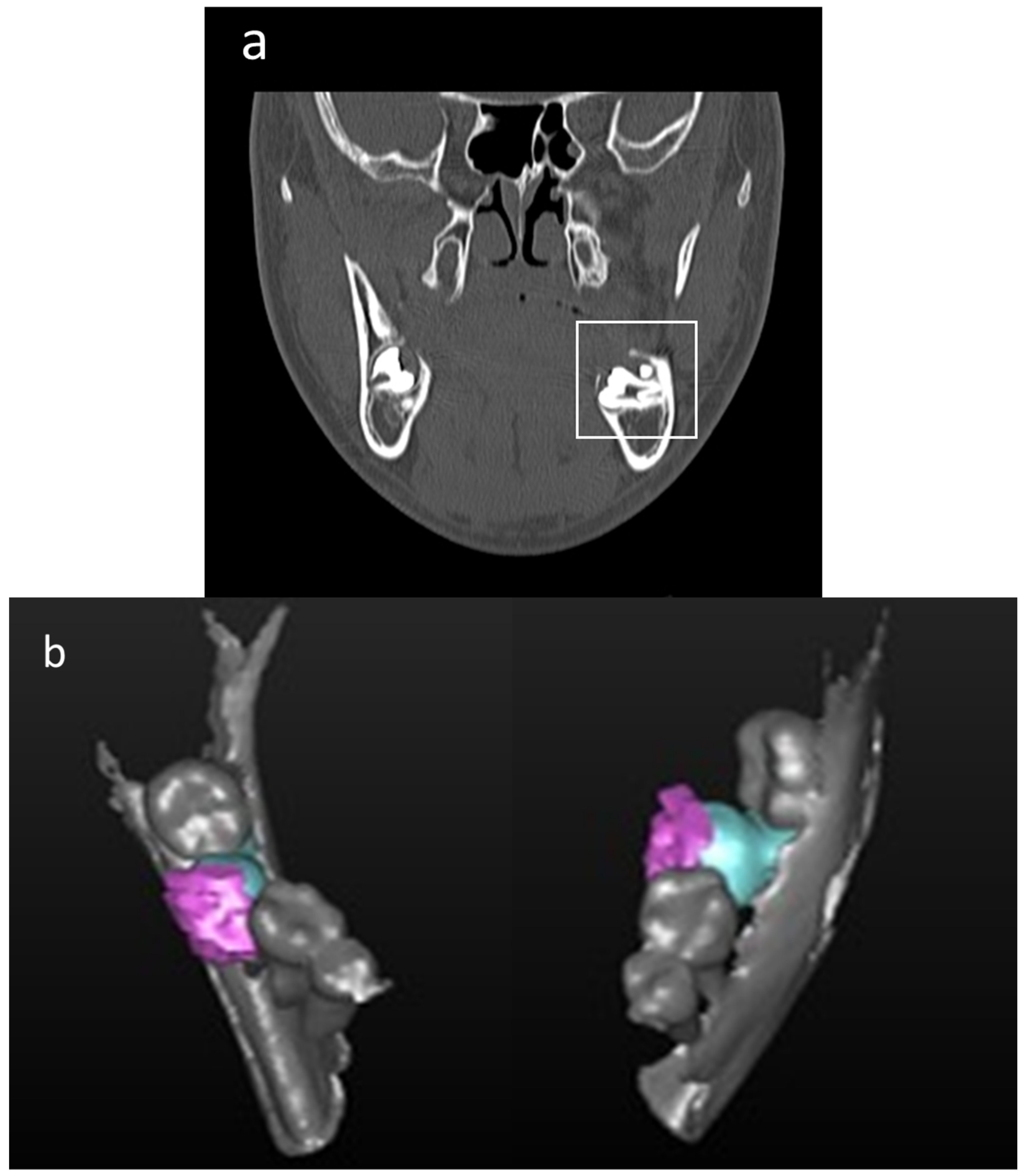
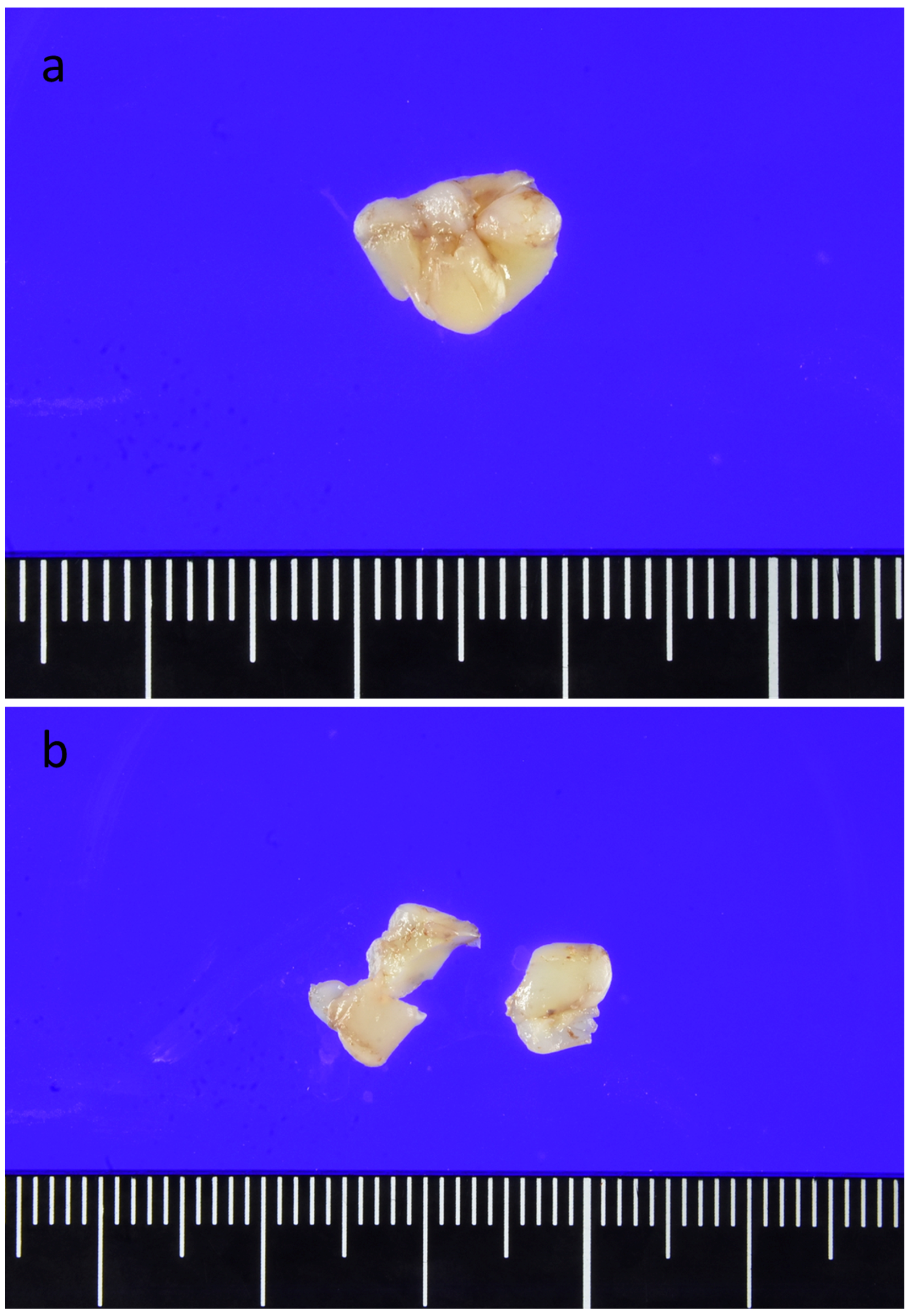
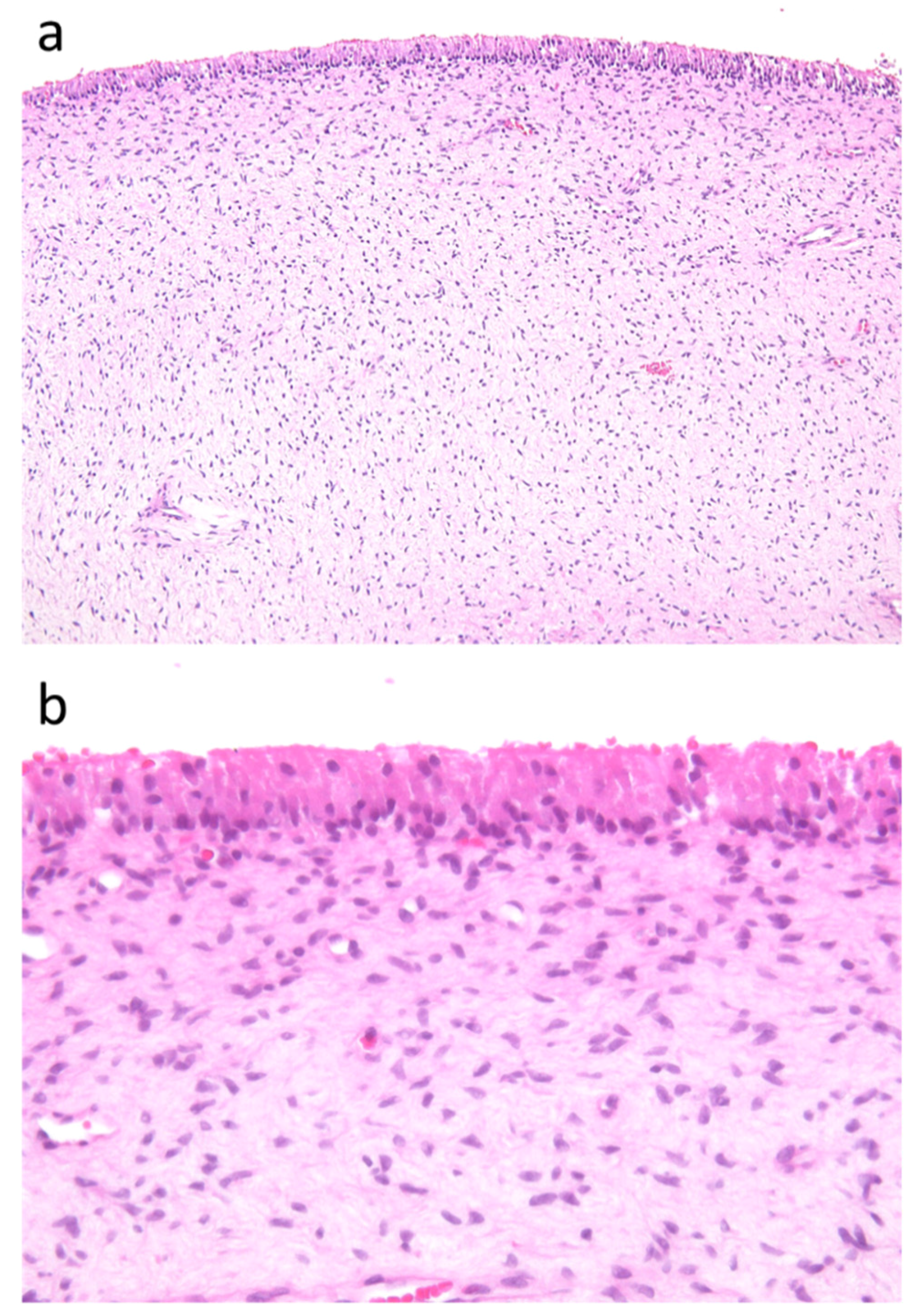
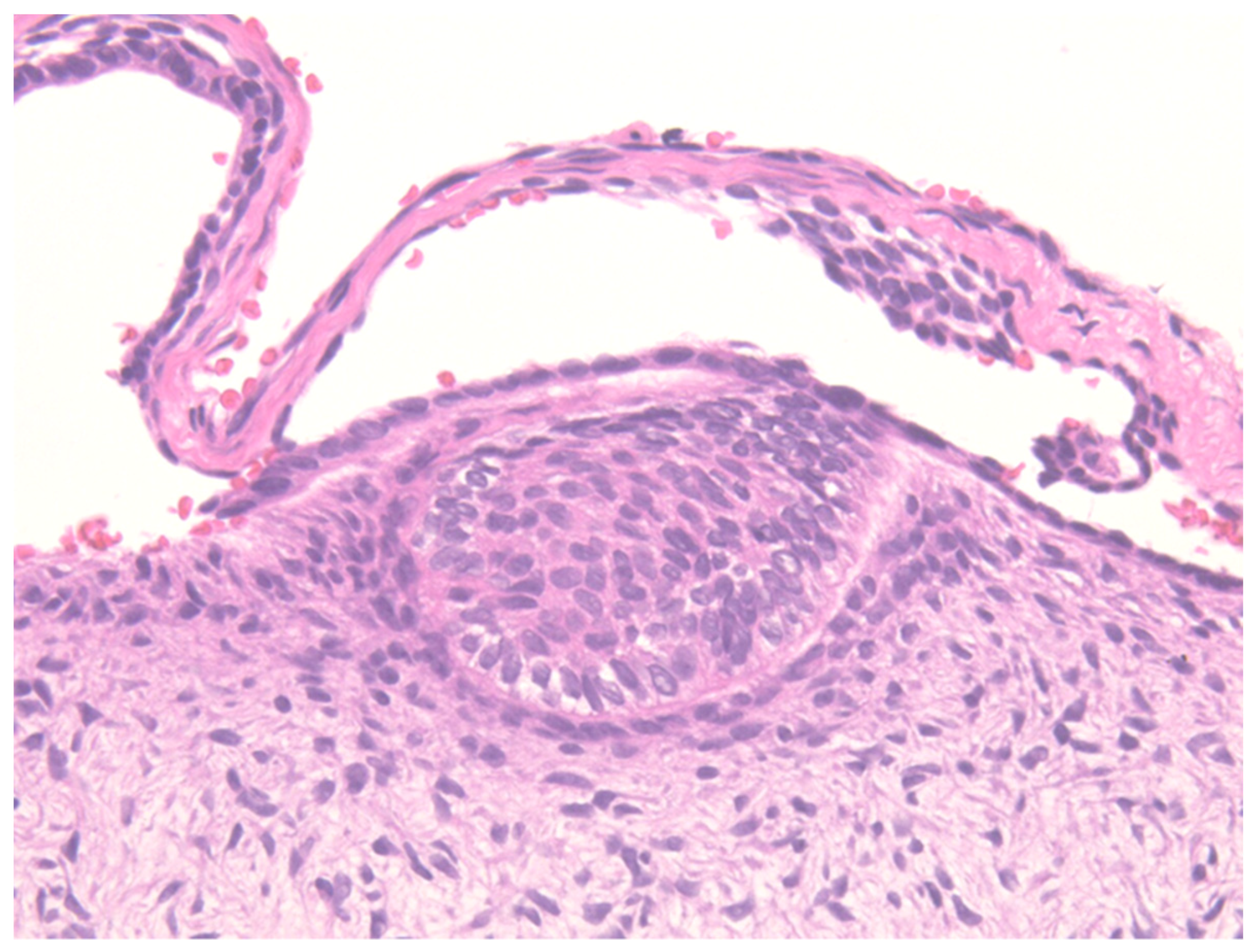
2. Case Report
3. Discussion

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Age (Years) | Gender | Site | Radiographic Findings | Involved Teeth | Size (mm) | Clinical or Radiographic Diagmosis | Cut Surface | Recurrence, Follow-Up |
|---|---|---|---|---|---|---|---|---|---|
| Mosqueda Taylor et al. (2014) [2] | 3 | F | Mand | well-defined, biloculated | D, E, 6 | 90 × 70 | benign odontogenic tumor | solid mass | No, 9 years |
| 3 | F | Max | well-defined | E, 6 | 35 × 30 | benign odontogenic tumor | solid mass | No, 6 months | |
| 13 | F | Mand | well-defined, biloculated | 6,7,8 | 80 × 50 | benign odontogenic tumor | solid mass | No, 3 years | |
| 16 | M | Mand | well-defined | 8 | 55 × 50 | benign odontogenic tumor | solid mass | lost of follow up | |
| 16 | M | Mand | well-defined | 8 | 65 × 50 | benign odontogenic tumor | solid mass | No, 10 years | |
| 18 | M | Mand | well-defined | 8 | 45 × 40 | benign odontogenic tumor | solid mass | No, 20 years | |
| Slater LJ et al. (2016) [11] | 19 | M | Mand | well-defined | 8 | 25 × 19 | unknown | solid mass | No, 7 months |
| Ando et al. (2017) [8] | 8 | F | Max | well-defined | D | 16 × 15 | DC, benign odontogenic tumor | solid mass | No, 16 months |
| Mikami et al. (2017) [9] | 5 | M | Mand | well-defined | D, E | 80 × 80 | unknown | solid mass | No, 7 months |
| Bajpai and Pardhe (2018) [12] | 17 | M | Mand | well-defined, multilocular | 5, 6, 7, 8 | 30 × 20 | benign odontogenic tumor | unknown | No, 6 months |
| Almazyad A et al. (2018) [13] | 15 | F | Mand | well-defined, multilocular | 8 | 35 × 20 | DC | unknown | No, 3 months |
| 18 | M | Mand | well-defined | 8 | 12 × 7 | DC | a yellow–tan mass | No, 20 months | |
| Hatem Amer et al. (2018) [10] | 2 | M | Mand | well-defined, multilocular | impacted tooth | 30 × 40 | unknown | cystic lesion | No, 2 years |
| Bomfim B B et al. (2018) [14] | 4 | M | Mand | well-defined | D, E | 30 × 20 | unknown | solid mass | lost of follow up |
| Teixeira L N et al. (2019) [15] | 13 | F | Mand | well-defined | 8 | unknown | DC | unknown | No, 13 years |
| Poomsawat S et al. (2019) [16] | 17 | F | Mand | well-defined | 8 | 25 × 34 | other odontogenic cyst | unknown | No, 18 months |
| Wilson A. Delgado-Azañero et al. (2020) [17] | 12 | F | Mand | well-defined, unilocular | 5 | 30 × 25 | benign odontogenic tumor and DC | solid mass | No, 15 months |
| 13 | F | Mand | well-defined, unilocular | 8 | unknown | DC | solid mass | No, 60 months | |
| Naina S. et al. (2020) [3] | 14 | M | Max | well-defined, unilocular | impacted tooth | 30 × 20 | benign odontogenic tumor and DC | white nodule | No, 36 months |
| Kayamori K. et al. (2020) [18] | 10 | M | Max | well-defined, unilocular | D | 17 × 15 | benign odontogenic tumor | solid mass | No, 30 months |
| Present case | 14 | M | Mand | well-defined | 7 | 10 × 8 | DC | solid mass | No, 11 months |
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- El-Naggar, A.K.; Chan, J.K.C.; Grandis, J.R.; Takata, T.; Slootweg, P.J. WHO Classification of Head and Neck Tumours, 4th ed.; WHO: Geneva, Switzerland, 2017; Volume 9, pp. 223–224. [Google Scholar]
- Mosqueda-Taylor, A.; Pires, F.R.; Aguirre-Urízar, J.M.; Carlos-Bregni, R.; de la Piedra-Garza, J.M.; Martínez-Conde, R.; Martínez-Mata, G.; Carreño-Álvarez, S.J.; da Silveira, H.M.; de Barros Dias, B.S.; et al. Primordial odontogenic tumour: Clinicopathologica analysis of six cases of a previously undescribed entity. Histopathology 2014, 65, 606–612. [Google Scholar] [CrossRef] [PubMed]
- Naina, S.; Narwal, A.; Devi, A.; Kamboj, M.; Pandiar, D. Primordial Odontogenic Tumor of Anterior Maxilla in a Young Male: A Case Report and an Updated Review of Literature. Pediatr. Dev. Pathol. 2021, 24, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Sudhakara, M.; Rudrayya, S.P.; Vanaki, S.S.; Bhullar, R.K.; Shivakumar, M.S.; Hosur, M. Expression of CK14 and vimentin in adenomatoid odontogenic tumor and dentigerous cyst. J. Oral Maxillofac. Pathol. 2016, 20, 369–376. [Google Scholar] [PubMed] [Green Version]
- Bologna-Molina, R.; Mikami, T.; Pereira-Prado, V.; Pires, F.R.; Carlos-Bregni, R.; Mosqueda-Taylor, A. Primordial odontogenic tumor: An immunohistochemical profile. Med. Oral Patol. Oral Cir. Bucal. 2017, 22, e314–e323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nadalin, M.R.; Fregnani, E.R.; Silva-Sousa, Y.T.C.; Perez, D.E.D.C. Syndecan-1 (CD138) and Ki-67 expression in odontogenic cystic lesions. Braz. Dent. J. 2011, 22, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Rahman, F.; Bhargava, A.; Tippu, S.R.; Kalra, M.; Bhargava, N.; Kaur, I.; Srivastava, S. Analysis of the immunoexpression of Ki-67 and Bcl-2 in the pericoronal tissues of impacted teeth, dentigerous cysts and gingiva using software image analysis. Dent. Res. J. 2013, 10, 31–37. [Google Scholar]
- Ando, T.; Shrestha, M.; Nakamoto, T.; Uchisako, K.; Yamasaki, S.; Koizumi, K.; Ogawa, I.; Miyauchi, M.; Takata, T. A case of primordial odontogenic tumor: A new entity in the latest WHO classification (2017). Pathol. Int. 2017, 67, 365–369. [Google Scholar] [CrossRef] [PubMed]
- Mikami, T.; Ohashi, Y.; Bologna-Molina, R.; Mosqueda-Taylor, A.; Fujiwara, N.; Tsunoda, N.; Yamada, H.; Takeda, Y. Primordial Odontogenic Tumor: A case report with histopathological analyses. Pathol. Int. 2017, 67, 638–643. [Google Scholar] [CrossRef] [PubMed]
- Hafed, L.; Amer, H.; Ibrahim, S. Case Report: A Primordial odontogenic tumor [version 1; referees: 3 approved]. F1000Research 2018, 7, 1. [Google Scholar]
- Slater, L.J.; Eftimie, L.F.; Herford, A.S. Primordial Odontogenic Tumor: Report of a Case. J. Oral Maxillofac. Surg. 2016, 74, 547–551. [Google Scholar] [CrossRef] [PubMed]
- Pardhe, N.; Bajpai, M. Primordial odontogenic tumor of mandible; a case with proposed diagnostic criteria. Iran. J. Med. Sci. 2018, 43, 97–99. [Google Scholar] [PubMed]
- Almazyad, A.; Li, C.C.; Tapia, R.O.; Robertson, J.P.; Collette, D.; Woo, S.B. Primordial odontogenic tumour: Report of two cases. Histopathology 2018, 72, 1221–1227. [Google Scholar] [CrossRef] [PubMed]
- Bomfim, B.B.; Prado, R.; Sampaio, R.K.; Conde, D.C.; de Andrade, B.A.B.; Agostini, M.; Romañach, M.J. Primordial Odontogenic Tumor: Report of a New Case and Literature Review. Head Neck Pathol. 2019, 13, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, L.N.; Furuse, C.; Santos, F.P.; Soares, A.B.; de Oliveira, E.M.F.; de Araújo, N.S.; de Araújo, V.C. The challenging diagnosis of primordial odontogenic tumor. Case Rep. Dent. 2019, 2019, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Poomsawat, S.; Ngamsom, S.; Nonpassopon, N. Primordial odontogenic tumor with prominent calcifications: A rare case report. J. Clin. Exp. Dent. 2019, 11, e952–e956. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Azañero, W.A.; de Almeida, O.P.; Pereira, A.A.C.; de Oliveira, C.E.; Dias, M.A.; Florez-Valderrama, G.; de Lima Morais, T.M.; Mariz, B.A.L.A.; Mosqueda-Taylor, A. Primordial odontogenic tumor: Report of 2 new cases. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 20, 31126–31133. [Google Scholar] [CrossRef] [PubMed]
- Kayamori, K.; Tsuchiya, M.; Michi, Y.; Kuribayashi, A.; Mikami, T.; Sakamoto, K.; Yoda, T.; Ikeda, T. Primordial odontogenic tumor occurred in the maxilla with unique calcifications and its crucial points for differential diagnosis. Pathol. Int. 2021, 71, 80–87. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ono, S.; Kawai, H.; Sukegawa, S.; Takabatake, K.; Nakano, K.; Nagatsuka, H.; Yoshino, T. A Case Report of Primordial Odontogenic Tumor That Required Distinction from a Dentigerous Cyst. Reports 2021, 4, 4. https://0-doi-org.brum.beds.ac.uk/10.3390/reports4010004
Ono S, Kawai H, Sukegawa S, Takabatake K, Nakano K, Nagatsuka H, Yoshino T. A Case Report of Primordial Odontogenic Tumor That Required Distinction from a Dentigerous Cyst. Reports. 2021; 4(1):4. https://0-doi-org.brum.beds.ac.uk/10.3390/reports4010004
Chicago/Turabian StyleOno, Sawako, Hotaka Kawai, Shintaro Sukegawa, Kiyofumi Takabatake, Keisuke Nakano, Hitoshi Nagatsuka, and Tadashi Yoshino. 2021. "A Case Report of Primordial Odontogenic Tumor That Required Distinction from a Dentigerous Cyst" Reports 4, no. 1: 4. https://0-doi-org.brum.beds.ac.uk/10.3390/reports4010004