
Usefulness of Circulating CYFRA21-1 in Patients as a Biomarker in Patients Taking Sorafenib or Lenvatinib for Unresectable Hepatocellular Carcinoma

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Administration of SOR/LEN
2.3. Measurement of Serum CYFRA21-1
2.4. Follow-Up after Administration
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
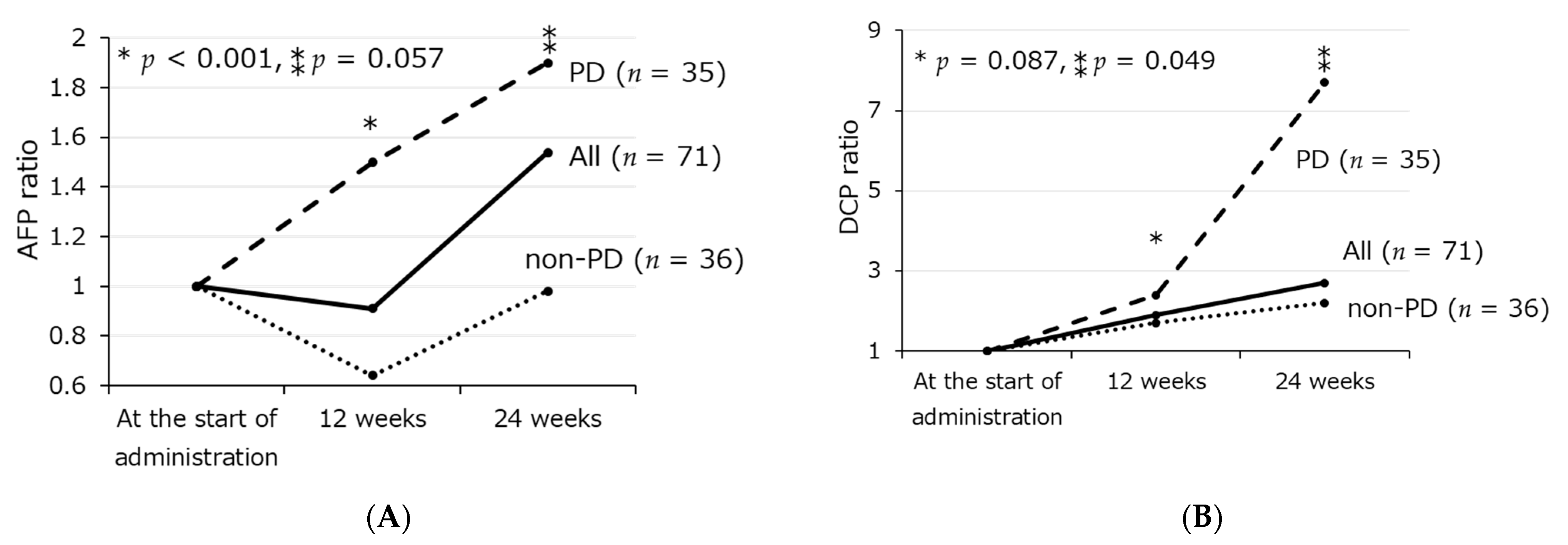
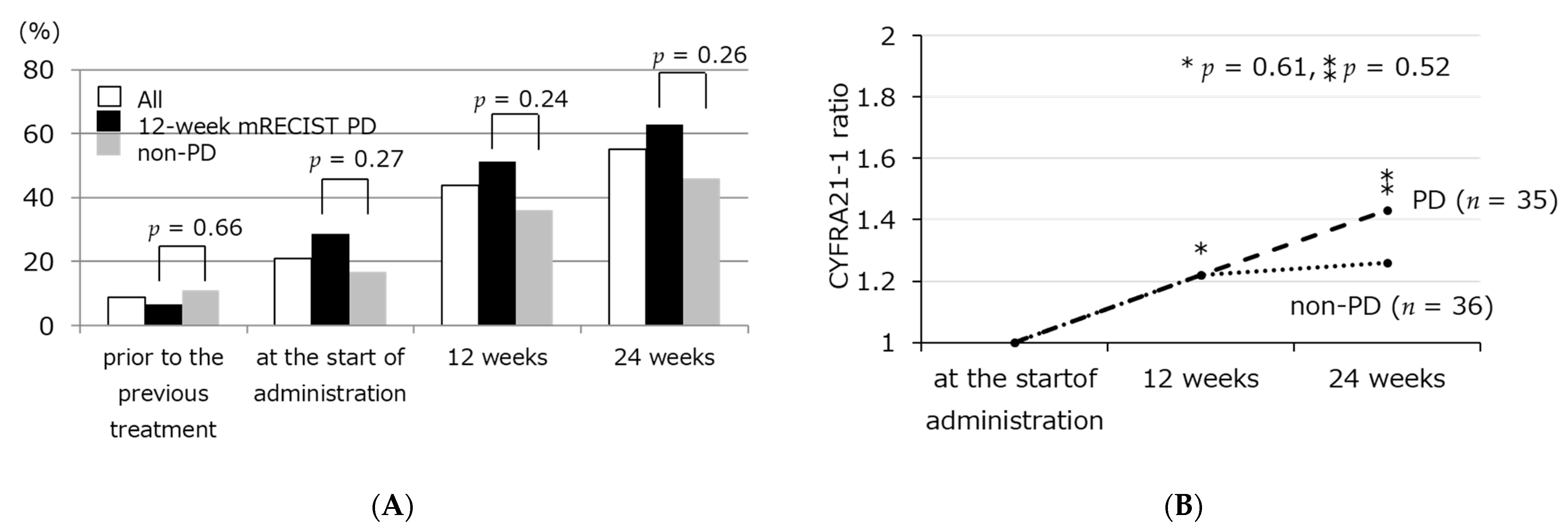
3.2. Transition of Tumor Markers Including Serum CYFRA21-1 Level
3.3. Factors Relating to Survival after SOR/LEN Administration
3.4. Characteristics in Patients with High CYFRA 21-1 Level
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Me, J.F.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; De Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in Advanced Hepatocellular Carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.-H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.-W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef] [Green Version]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.-H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 389, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Abou-Alfa, G.K.; Meyer, T.; Cheng, A.-L.; El-Khoueiry, A.B.; Rimassa, L.; Ryoo, B.-Y.; Cicin, I.; Merle, P.; Chen, Y.; Park, J.-W.; et al. Cabozantinib in Patients with Advanced and Progressing Hepatocellular Carcinoma. N. Engl. J. Med. 2018, 379, 54–63. [Google Scholar] [CrossRef]
- Zhu, A.X.; Kang, Y.-K.; Yen, C.-J.; Finn, R.S.; Galle, P.R.; Llovet, J.M.; Assenat, E.; Brandi, G.; Pracht, M.; Lim, H.Y.; et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased α-fetoprotein concentrations (REACH-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 282–296. [Google Scholar] [CrossRef]
- Kudo, M.; Okusaka, T.; Motomura, K.; Ohno, I.; Morimoto, M.; Seo, S.; Wada, Y.; Sato, S.; Yamashita, T.; Furukawa, M.; et al. Ramucirumab after prior sorafenib in patients with advanced hepatocellular carcinoma and elevated alpha-fetoprotein: Japanese subgroup analysis of the REACH-2 trial. J. Gastroenterol. 2020, 55, 627–639. [Google Scholar] [CrossRef] [Green Version]
- Zhu, A.X.; Park, J.O.; Ryoo, B.-Y.; Yen, C.-J.; Poon, R.; Pastorelli, D.; Blanc, J.-F.; Chung, H.; Baron, A.D.; Pfiffer, T.E.F.; et al. Ramucirumab versus placebo as second-line treatment in patients with advanced hepatocellular carcinoma following first-line therapy with sorafenib (REACH): A randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol. 2015, 16, 859–870. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.-Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Ricci-Vitiani, L.; Lombardi, D.G.; Pilozzi, E.; Biffoni, M.; Todaro, M.; Peschle, C.; De Maria, R. Identification and expansion of human colon-cancer-initiating cells. Nature 2007, 445, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Al-Hajj, M.; Wicha, M.S.; Benito-Hernandez, A.; Morrison, S.J.; Clarke, M.F. Prospective identification of tumorigenic breast cancer cells. Proc. Natl. Acad. Sci. USA 2003, 100, 3983–3988. [Google Scholar] [CrossRef] [Green Version]
- Kawai, T.; Yasuchika, K.; Ishii, T.; Katayama, H.; Yoshitoshi, E.Y.; Ogiso, S.; Minami, T.; Miyauchi, Y.; Kojima, H.; Yamaoka, R.; et al. Identification of keratin 19-positive cancer stem cells associating human hepatocellular carcinoma using CYFRA 21-1. Cancer Med. 2017, 6, 2531–2540. [Google Scholar] [CrossRef] [Green Version]
- Kawai, T.; Yasuchika, K.; Ishii, T.; Katayama, H.; Yoshitoshi, E.Y.; Ogiso, S.; Kita, S.; Yasuda, K.; Fukumitsu, K.; Mizumoto, M.; et al. Keratin 19, a Cancer Stem Cell Marker in Human Hepatocellular Carcinoma. Clin. Cancer Res. 2015, 21, 3081–3091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Medical Association. Declaration of Helsinki. Law Med. Health Care 1991, 19, 264–265. [Google Scholar] [CrossRef]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of Liver Function in Patients With Hepatocellular Carcinoma: A New Evidence-Based Approach—The ALBI Grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) Assessment for Hepatocellular Carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef] [Green Version]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [Green Version]
- Kudo, M.; Han, K.-H.; Ye, S.-L.; Zhou, J.; Huang, Y.-H.; Lin, S.-M.; Wang, C.-K.; Ikeda, M.; Chan, S.L.; Choo, S.P.; et al. A Changing Paradigm for the Treatment of Intermediate-Stage Hepatocellular Carcinoma: Asia-Pacific Primary Liver Cancer Expert Consensus Statements. Liver Cancer 2020, 9, 245–260. [Google Scholar] [CrossRef] [PubMed]
- Kew, M.C. Hepatocellular carcinoma in developing countries: Prevention, diagnosis and treatment. World J. Hepatol. 2012, 4, 99–104. [Google Scholar] [CrossRef]
- Ueshima, K.; Kudo, M.; Takita, M.; Nagai, T.; Tatsumi, C.; Ueda, T.; Kitai, S.; Ishikawa, E.; Yada, N.; Inoue, T.; et al. Des-γ-Carboxyprothrombin May Be a Promising Biomarker to Determine the Therapeutic Efficacy of Sorafenib for Hepatocellular Carcinoma. Dig. Dis. 2011, 29, 321–325. [Google Scholar] [CrossRef]
- Miyahara, K.; Nouso, K.; Morimoto, Y.; Tomoda, T.; Kobayashi, S.; Takeuchi, Y.; Hagihara, H.; Kuwaki, K.; Ohnishi, H.; Ikeda, F.; et al. Evaluation of the effect of sorafenib using serum NX-des-γ-carboxyprothrombin in patients with hepatocellular carcinoma. Hepatol. Res. 2012, 43, 1064–1070. [Google Scholar] [CrossRef]
- Kuzuya, T.; Asahina, Y.; Tsuchiya, K.; Tanaka, K.; Suzuki, Y.; Hoshioka, T.; Tamaki, S.; Kato, T.; Yasui, Y.; Hosokawa, T.; et al. Early Decrease in α-Fetoprotein, but Not Des-γ-Carboxy Prothrombin, Predicts Sorafenib Efficacy in Patients with Advanced Hepatocellular Carcinoma. Oncology 2011, 81, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, H.; Ohno, S.; Miyazaki, M.; Hashimoto, K.; Egashira, A.; Saeki, H.; Watanabe, M.; Sugimachi, K. CYFRA 21-1 determination in patients with esophageal squamous cell carcinoma. Cancer 2000, 89, 1413–1417. [Google Scholar] [CrossRef]
- Anfuso, B.; El-Khobar, K.E.; Sukowati, C.; Tiribelli, C. The multiple origin of cancer stem cells in hepatocellular carcinoma. Clin. Res. Hepatol. Gastroenterol. 2015, 39, S92–S97. [Google Scholar] [CrossRef]
- Komuta, M.; Spee, B.; Borght, S.V.; De Vos, R.; Verslype, C.; Aerts, R.; Yano, H.; Suzuki, T.; Matsuda, M.; Fujii, H.; et al. Clinicopathological study on cholangiolocellular carcinoma suggesting hepatic progenitor cell origin. Hepatology 2008, 47, 1544–1556. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.-S.; Heo, J.; Libbrecht, L.; Chu, I.-S.; Kaposi-Novak, P.; Calvisi, D.F.; Mikaelyan, A.; Roberts, L.; Demetris, A.J.; Sun, Z.; et al. A novel prognostic subtype of human hepatocellular carcinoma derived from hepatic progenitor cells. Nat. Med. 2006, 12, 410–416. [Google Scholar] [CrossRef]
- Dean, M.; Fojo, T.; Bates, S.E. Tumour stem cells and drug resistance. Nat. Rev. Cancer 2005, 5, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Caviglia, G.P.; Ciruolo, M.; Olivero, A.; Carucci, P.; Rolle, E.; Rosso, C.; Abate, M.L.; Risso, A.; Ribaldone, D.G.; Tandoi, F.; et al. Prognostic Role of Serum Cytokeratin-19 Fragment (CYFRA 21-1) in Patients with Hepatocellular Carcinoma. Cancers 2020, 12, 2776. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.; Fujita, J.; Murota, M.; Li, J.-Q.; Ishida, T.; Nishioka, M.; Imaida, Y.; Kuriyama, S. CYFRA 21-1 is released in TNF-α-induced apoptosis in the hepatocellular carcinoma cell line HuH-7. Int. J. Oncol. 2002, 21, 441–445. [Google Scholar] [CrossRef] [PubMed]
- Ding, S.-J.; Li, Y.; Tan, Y.-X.; Jiang, M.-R.; Tian, B.; Liu, Y.-K.; Shao, X.-X.; Ye, S.-L.; Wu, J.-R.; Zeng, R.; et al. From proteomic analysis to clinical significance: Overexpression of cytokeratin 19 correlates with hepatocellular carcinoma metastasis. Mol. Cell. Proteom. 2004, 3, 73–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsuchiya, K.; Komuta, M.; Yasui, Y.; Tamaki, N.; Hosokawa, T.; Ueda, K.; Kuzuya, T.; Itakura, J.; Nakanishi, H.; Takahashi, Y.; et al. Expression of Keratin 19 Is Related to High Recurrence of Hepatocellular Carcinoma after Radiofrequency Ablation. Oncology 2011, 80, 278–288. [Google Scholar] [CrossRef]
- Uenishi, T.; Kubo, S.; Yamamoto, T.; Shuto, T.; Ogawa, M.; Tanaka, H.; Tanaka, S.; Kaneda, K.; Hirohashi, K. Cytokeratin 19 expression in hepatocellular carcinoma predicts early postoperative recurrence. Cancer Sci. 2003, 94, 851–857. [Google Scholar] [CrossRef] [PubMed]
- Uenishi, T.; Yamazaki, O.; Yamamoto, T.; Hirohashi, K.; Tanaka, H.; Tanaka, S.; Hai, S.; Ono, K.; Kubo, S. Clinical significance of serum cytokeratin-19 fragment (CYFRA 21-1) in hepatocellular carcinoma. J. Hepato-Biliary-Pancreat. Surg. 2006, 13, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Govaere, O.; Komuta, M.; Berkers, J.; Spee, B.; Janssen, C.; De Luca, F.; Katoonizadeh, A.; Wouters, J.; van Kempen, L.; Durnez, A.; et al. Keratin 19: A key role player in the invasion of human hepatocellular carcinomas. Gut 2013, 63, 674–685. [Google Scholar] [CrossRef] [Green Version]
- Durnez, A.; Verslype, C.; Nevens, F.; Fevery, J.; Aerts, R.; Pirenne, J.; Lesaffre, E.; Libbrecht, L.; Desmet, V.; Roskams, T. The clinicopathological and prognostic relevance of cytokeratin 7 and 19 expression in hepatocellular carcinoma. A possible progenitor cell origin. Histopathology 2006, 49, 138–151. [Google Scholar] [CrossRef]
- Ku, N.-O.; Strnad, P.; Bantel, H.; Omary, B. Keratins: Biomarkers and modulators of apoptotic and necrotic cell death in the liver. Hepatology 2016, 64, 966–976. [Google Scholar] [CrossRef] [Green Version]
- Zen, C.; Zen, Y.; Mitry, R.R.; Corbeil, D.; Karbanova, J.; O’Grady, J.; Karani, J.; Kane, P.; Heaton, N.; Portmann, B.C.; et al. Mixed phenotype hepatocellular carcinoma after transarterial chemoembolization and liver transplantation. Liver Transplant. 2011, 17, 943–954. [Google Scholar] [CrossRef]
- Zeng, Z.; Ren, J.; O’Neil, M.; Zhao, J.; Bridges, B.; Cox, J.; Abdulkarim, B.; Schmitt, T.M.; Kumer, S.C.; Weinman, S.A. Impact of stem cell marker expression on recurrence of TACE-treated hepatocellular carcinoma post liver transplantation. BMC Cancer 2012, 12, 584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terashima, T.; Yamashita, T.; Takata, N.; Nakagawa, H.; Toyama, T.; Arai, K.; Kitamura, K.; Yamashita, T.; Sakai, Y.; Mizukoshi, E.; et al. Post-progression survival and progression-free survival in patients with advanced hepatocellular carcinoma treated by sorafenib. Hepatol. Res. 2015, 46, 650–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiraoka, A.; Kumada, T.; Kariyama, K.; Takaguchi, K.; Itobayashi, E.; Shimada, N.; Tajiri, K.; Tsuji, K.; Ishikawa, T.; Ochi, H.; et al. Therapeutic potential of lenvatinib for unresectable hepatocellular carcinoma in clinical practice: Multicenter analysis. Hepatol. Res. 2019, 49, 111–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomonari, T.; Sato, Y.; Tani, J.; Hirose, A.; Ogawa, C.; Morishita, A.; Tanaka, H.; Tanaka, T.; Taniguchi, T.; Okamoto, K.; et al. Comparison of therapeutic outcomes of sorafenib and lenvatinib as primary treatments for hepatocellular carcinoma with a focus on molecular-targeted agent sequential therapy: A propensity score-matched analysis. Hepatol. Res. 2020, 51, 472–481. [Google Scholar] [CrossRef]
- Takada, H.; Kurosaki, M.; Tsuchiya, K.; Komiyama, Y.; Itakura, J.; Takahashi, Y.; Nakanishi, H.; Yasui, Y.; Tamaki, N.; Maeyashiki, C.; et al. Baseline and Early Predictors of Good Patient Candidates for Second-Line after Sorafenib Treatment in Unresectable Hepatocellular Carcinoma. Cancers 2019, 11, 1256. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.-K.; Yen, C.-L.; Shiu, S.-I.; Lee, S.-W.; Chang, P.-Y.; Yeh, H.-Z.; Lee, T.-Y. Transcatheter arterial chemoembolization after stopping sorafenib therapy for advanced hepatocellular carcinoma. PLoS ONE 2017, 12, e0188999. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| All (n = 71) | SOR (n = 36) | LEN (n = 35) | p Value | |
|---|---|---|---|---|
| Male gender, n (%) | 62 (87) | 31 (86) | 31 (89) | 1.0 |
| Etiology: HBV/HCV/others, n (%) | 13/33/25 (18/47/35) | 7/19/10 (19/53/28) | 6/14/15 (17/40/43) | 0.42 |
| At the time of administration of SOR/LEN Age (years), median(range) | 70 (52–91) | 69 (56–91) | 70 (52–83) | 0.92 |
| Tumor diameter (mm), median(range) | 27 (8.4–180) | 29 (8.4–160) | 27 (12–180) | 0.85 |
| Tumor number, median(range) | 6 (1–10) | 10 (1–10) | 6 (1–10) | 0.046 |
| Portal vein tumor thrombosis (Vp 2/3), n (%) | 16 (22) | 8 (22) | 8 (23) | 1.0 |
| Extrahepatic metastasis, n (%) | 29 (41) | 19 (53) | 10 (29) | 0.054 |
| ALBI grade 1/2/3, n (%) | 20/48/3 (28/68/4) | 10/24/2 (28/67/5) | 10/24/1 (29/68/3) | 1.0 |
| BCLC stage B/C, n (%) | 32/39 (45/55) | 13/23 (36/64) | 19/16 (54/46) | 0.16 |
| AFP (ng/mL), median(range) | 143 (1.8–421,248) | 238 (1.8–421,248) | 143 (4.0–146,670) | 0.48 |
| AFP L3 index (%), median(range) | 18 (0.5–94) | 29 (0.5–87) | 15 (0.5–94) | 0.31 |
| DCP (mAU/mL), median(range) | 939 (15–616,708) | 1671 (15–616,708) | 513 (25–501,890) | 0.41 |
| CYFRA21-1 (ng/mL), median(range) | 2.6 (0.76–10.6) | 2.5 (0.76–10.6) | 2.7 (1.1–8.9) | 0.63 |
| Administration dose, reduction/full dose, n (%) | 16/55 (22/78) | 32/4 (89/11) | 12/23 (34/66) | 0.001 |
| Administration duration (weeks), median(range) | 17 (4–95) | 16 (4–95) | 21 (4–88) | 0.30 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| HR | p Value | HR | 95%CI | p Value | ||
| At the start of administration | Tumor diameter ≥ 70 mm | 3.4 | <0.001 | 2.3 | 0.97–5.3 | 0.059 |
| Tumor number ≥ 4 | 1.3 | 0.44 | ||||
| Portal vein tumor thrombosis (Vp 2/3) | 1.7 | 0.097 | ||||
| Extrahepatic metastasis | 2.0 | 0.031 | 1.6 | 0.81–3.0 | 0.19 | |
| ALBI grade 2/3 | 1.5 | 0.24 | ||||
| AFP ≥ 2000 ng/ml | 3.7 | <0.001 | 2.0 | 0.91–4.6 | 0.079 | |
| AFP-L3 index ≥ 15% | 2.2 | 0.020 | 2.2 | 1.1–4.6 | 0.030 | |
| DCP ≥ 1000 mAU/ml | 4.9 | 0.0025 | 1.3 | 0.55–2.9 | 0.59 | |
| CYFRA21-1 ≥ 3.5 ng/ml | 2.1 | 0.024 | 2.1 | 0.99–4.6 | 0.051 | |
| After the start of administration | 12-week mRECIST PD | 1.9 | 0.042 | 1.7 | 1.01–3.7 | 0.019 |
| 12-week AFP ratio ≥ 0.8 | 1.9 | 0.051 | ||||
| 12-week DCP ratio ≥ 4 | 3.0 | 0.018 | 2.5 | 1.1–6.3 | 0.047 | |
| 12-week CYFRA21-1 ratio ≥ 2 | 2.4 | 0.0025 | 3.6 | 1.2–11 | 0.023 | |
| Administration period < 12 weeks | 2.4 | 0.0071 | 2.4 | 1.1–5.7 | 0.046 | |
| ALBI grade 3 at PD | 3.9 | 0.0020 | 2.3 | 0.86–6.4 | 0.097 | |
| No additional treatment after discontinuation of SOR/LEN | 2.0 | 0.041 | 2.5 | 1.1–6.1 | 0.036 | |
| Baseline < 3.5 ng/mL and 12-Week CYFRA21-1 Ratio < 2 (n = 46) | Baseline ≥ 3.5 ng/mL or 12-Week CYFRA21-1 Ratio ≥ 2 (n = 25) | p Value | |
|---|---|---|---|
| Male gender, n (%) | 41 (89%) | 21 (84%) | 0.71 |
| At the time of administration of SOR/LEN Age (years), median(range) | 69 (52–86) | 72 (52–91) | 0.47 |
| Tumor size ≥70 mm, n (%) | 7 (15%) | 7 (28%) | 0.22 |
| Tumor number ≥4, n (%) | 38 (83%) | 17 (68%) | 0.23 |
| up to 7 out, n (%) | 37 (80%) | 21 (84%) | 1.0 |
| Portal vein thrombosis (Vp 2/3), n (%) | 11 (24%) | 5 (20%) | 0.78 |
| Extrahepatic metastasis, n (%) | 16 (35%) | 13 (52%) | 0.21 |
| ALBI grade 2or3, n (%) | 34 (74) | 17 (68) | 0.59 |
| AFP ≥2000 ng/mL, n (%) | 7 (15%) | 12 (48%) | 0.005 |
| AFP L3 index ≥ 15%, n (%) | 24 (52%) | 18 (72%) | 0.13 |
| DCP ≥ 1000 mAU/mL, n (%) | 19 (42%) | 15 (63%) | 0.13 |
| 12-week mRECIST PD, n (%) | 21 (47%) | 12 (52%) | 0.80 |
| TACE unsuitable pattern, n (%) | 19 (41%) | 19 (76%) | 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takada, H.; Osawa, L.; Komiyama, Y.; Kato, R.; Nakakuki, N.; Muraoka, M.; Suzuki, Y.; Tatsumi, A.; Sato, M.; Takahashi, E.; et al. Usefulness of Circulating CYFRA21-1 in Patients as a Biomarker in Patients Taking Sorafenib or Lenvatinib for Unresectable Hepatocellular Carcinoma. Reports 2021, 4, 25. https://0-doi-org.brum.beds.ac.uk/10.3390/reports4030025
Takada H, Osawa L, Komiyama Y, Kato R, Nakakuki N, Muraoka M, Suzuki Y, Tatsumi A, Sato M, Takahashi E, et al. Usefulness of Circulating CYFRA21-1 in Patients as a Biomarker in Patients Taking Sorafenib or Lenvatinib for Unresectable Hepatocellular Carcinoma. Reports. 2021; 4(3):25. https://0-doi-org.brum.beds.ac.uk/10.3390/reports4030025
Chicago/Turabian StyleTakada, Hitomi, Leona Osawa, Yasuyuki Komiyama, Ryoh Kato, Natsuko Nakakuki, Masaru Muraoka, Yuichiro Suzuki, Akihisa Tatsumi, Mitsuaki Sato, Ei Takahashi, and et al. 2021. "Usefulness of Circulating CYFRA21-1 in Patients as a Biomarker in Patients Taking Sorafenib or Lenvatinib for Unresectable Hepatocellular Carcinoma" Reports 4, no. 3: 25. https://0-doi-org.brum.beds.ac.uk/10.3390/reports4030025