
An Unusual Femoral Sheath Severing with Successful Recapture: A Case Report



1
Department of Cardiology, University Hospital of Split, Spinčićeva 1, 21000 Split, Croatia
2
Department of Cardiology, Ljubljana University Medical Centre, Zaloska Cesta 7, 1000 Ljubljana, Slovenia
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to the work.
Reports 2021, 4(4), 34; https://0-doi-org.brum.beds.ac.uk/10.3390/reports4040034
Submission received: 16 August 2021
/
Revised: 27 September 2021
/
Accepted: 5 October 2021
/
Published: 8 October 2021
{kind=link}
{kind=link}
{kind=link}
Abstract
:This study presents a case of a successful severed femoral sheath recapture during transfemoral transcatheter aortic valve replacement (TAVR). During skin tunneling with a scalpel, the discontinuity of the femoral sheath occurred. Grasping of the distal sheath with the surgical hemostat was attempted unsuccessfully. A proximal part of the severed sheath was removed and Medtronic Sentrant introducer sheath (14 French) was then placed over the existing Confida wire which permanently remained in position, followed by the introduction of the Amplatz Left 2 (AL2) catheter which pushed the severed sheath in the ascending aorta over the Confida wire. The crucial maneuver was the entanglement of the severed sheath in the aortic non-coronary cusp which allowed for its entrapment by the AL2 catheter. This allowed for the coronary guidewire BMW Universal (0.014″) placement and a slow balloon retrieval (SeQuent NEO 2.5 × 25 mm2) of the severed sheath into the introducer sheath. The guidewire/balloon catheter was then exchanged for the support wire (0.035″) followed by the removal of the introducer sheath, AL2 catheter and the severed sheath. In conclusion, sheath severing is a complex accidental event during TAVR, which can be solved by intra-aortic recapture and retraction.
1. Introduction
Transcatheter aortic valve replacement (TAVR) is increasingly utilized for the treatment of severe aortic stenosis (AS) [1]. According to the latest guidelines of the American College of Cardiology, TAVR is primarily recommended for symptomatic patients with severe AS who have a prohibitive risk for surgical aortic valve replacement (SAVR) with a predicted post-TAVR survival of >12 months, or those who are older than 80 years or for younger patients with a life expectancy of <10 years and no anatomic contraindication [2]. Recent years have seen an increased use of femoral access for TAVR and a decreased occurrence of access-related complications such as bleeding, vascular occlusion with peripheral ischemia, and embolization [3,4].
However, owing to the global expansion of percutaneous procedures, different unpredictable accidental events still occur on a daily basis. As such, equipment-related events represent an important issue which have a rare occurrence but require extremely delicate management and the operators must be familiar with various solving methods. The frailty and complexity of patients additionally increase the vascular access-related risks, especially including large-bore equipment [5]. To the best of our knowledge, none of the studies reported femoral sheath severing with successful intra-aortic recapture and retraction.
2. Case Presentation Section
This study presents an 86-year-old patient who underwent TAVR due to low-flow low-gradient severe symptomatic AS. In-hospital echocardiographic measurements showed a mean transvalvular pressure gradient of 29 mmHg, aortic valve area (AVA) ≤1 cm2 and a peak velocity of 3.8 m/s with reduced ejection fraction (Simpson biplane LVEF ~25%). Chronic heart failure (ACCF/AHA C; NYHA 4) was accompanied with permanent atrial fibrillation and chronic coronary syndrome, leading to several repeated hospitalizations. In one of the preceding hospitalizations, the patient underwent balloon aortic valvuloplasty as a bridge to TAVR (due to institutional conditions). Prior to the TAVR procedure, multi-slice computed tomography (MSCT) of the aorta and its branches showed acceptable vessel calibers for a femoral approach. The timeline of clinical events is presented in Supplementary Figure S1.
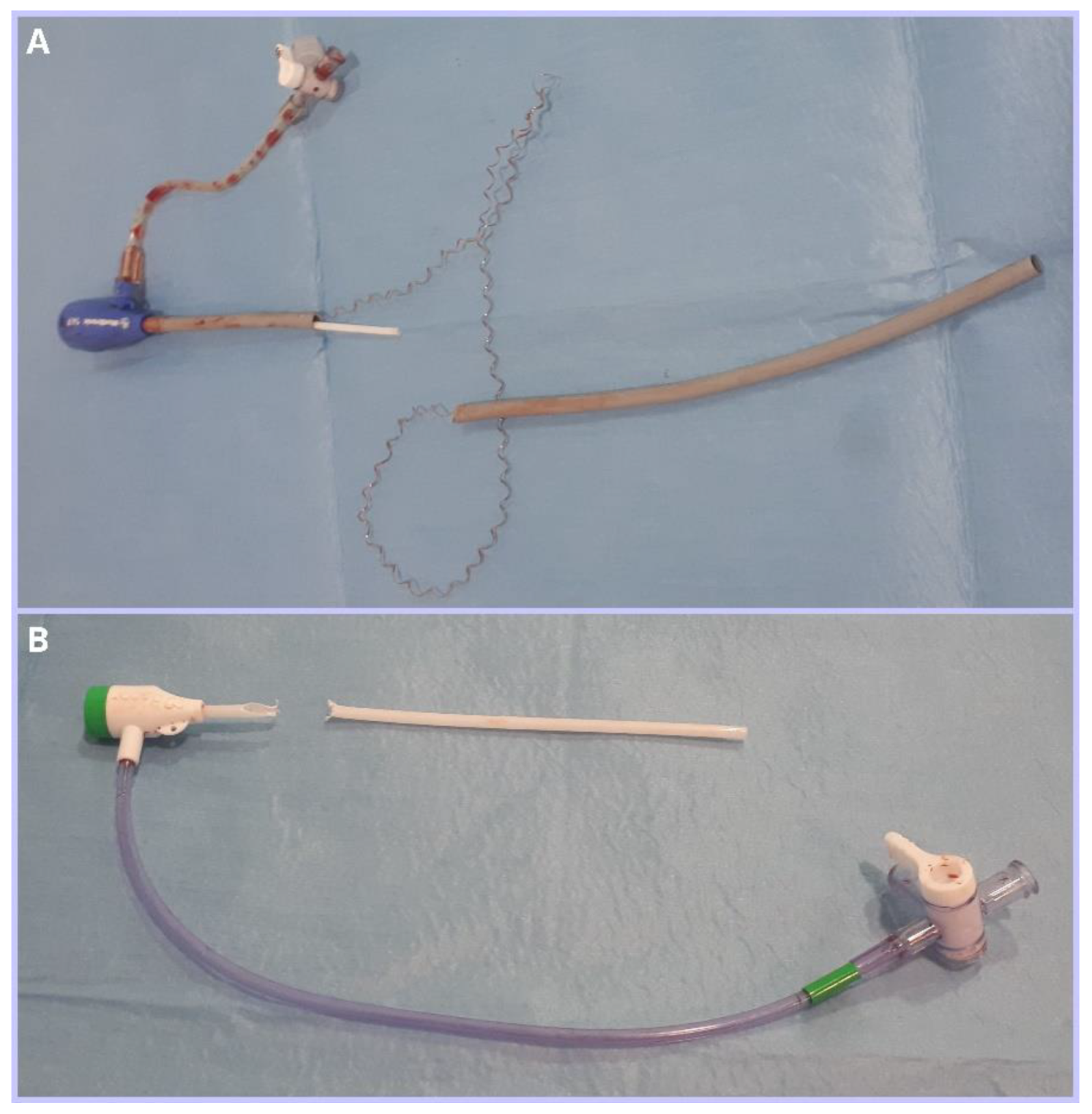
The procedure was introduced by the insertion of bilateral femoral sheaths (6 French). The pigtail catheter was placed in the non-coronary cusp over the left femoral approach, while a right-sided bore access served for the ventricular placement of support wire Confida (Medtronic™, Dublin, Ireland). Following this, right-side femoral access was additionally prepared for the placement of the EnVeo PRO delivery system (ENVPRO-16 Medtronic™, Dublin, Ireland), including a skin tunnel expansion by scalpel. However, at the moment of the 6 French sheath removal, the operator noticed an active local bleeding with discontinuity of the proximal and distal part of the femoral sheath (Figure 1).
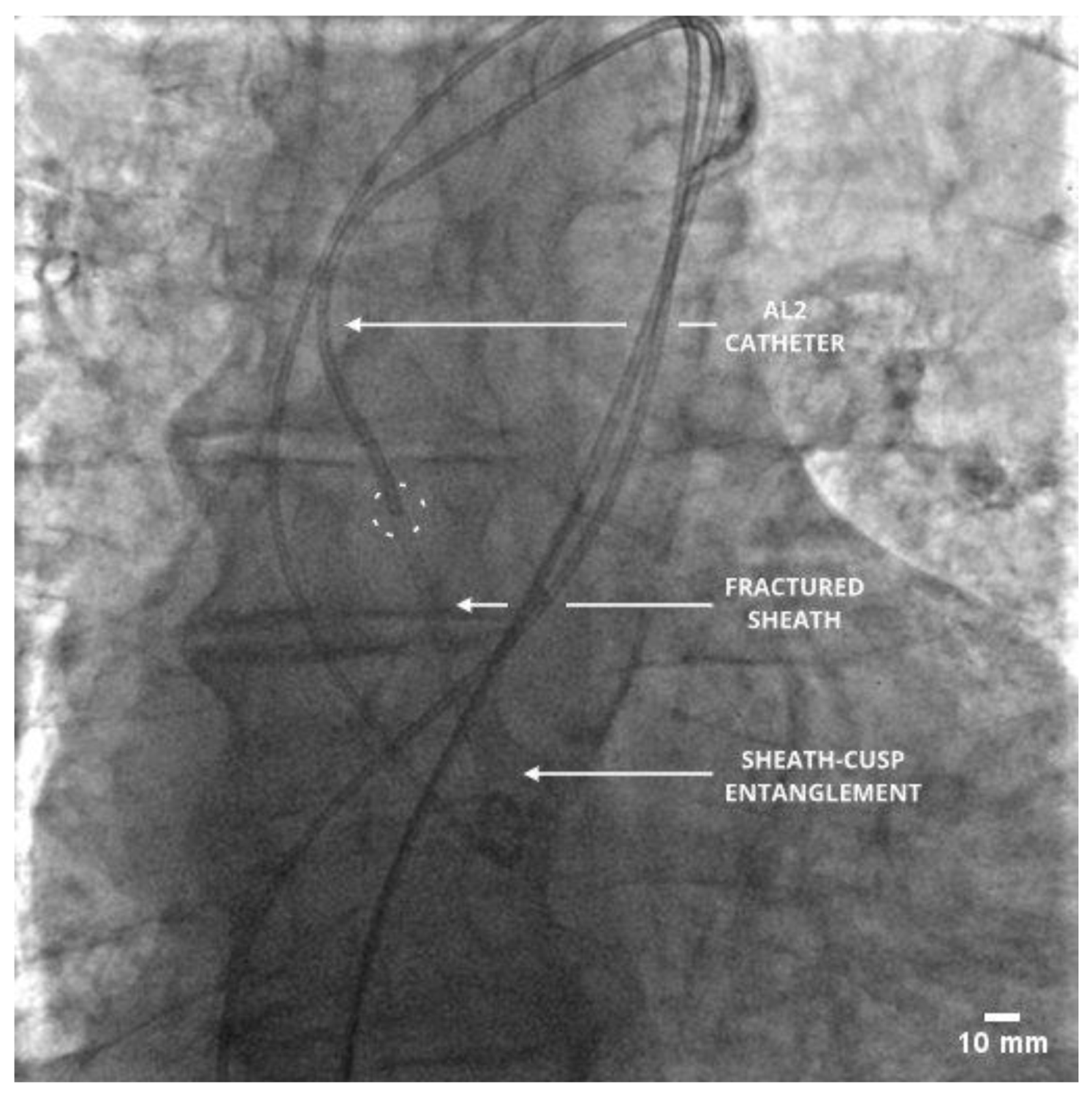
An immediate hemostatic control was established with the team strategy planning according to the Situation, Background, Assessment and Recommendation (SBAR) technique. Several unsuccessful attempts of grasping the distal sheath part with the surgical hemostat were performed. Therefore, a proximal part of the severed sheath was removed and a Medtronic Sentrant (Medtronic™, Dublin, Ireland) introducer sheath (14 French) was placed over the existing Confida wire. The Confida wire permanently remained in position with only a careful transfer from the left ventricle into the aortic bulb. This was followed by the introduction of the Amplatz Left 2 (AL2; Boston Scientific™, Marlborough, MS, USA) catheter which pushed the severed sheath in the ascending aorta over the Confida wire. The crucial step of this maneuver was the entanglement of the severed sheath in the aortic non-coronary cusp which allowed for its entrapment by the AL2 catheter (Figure 2).
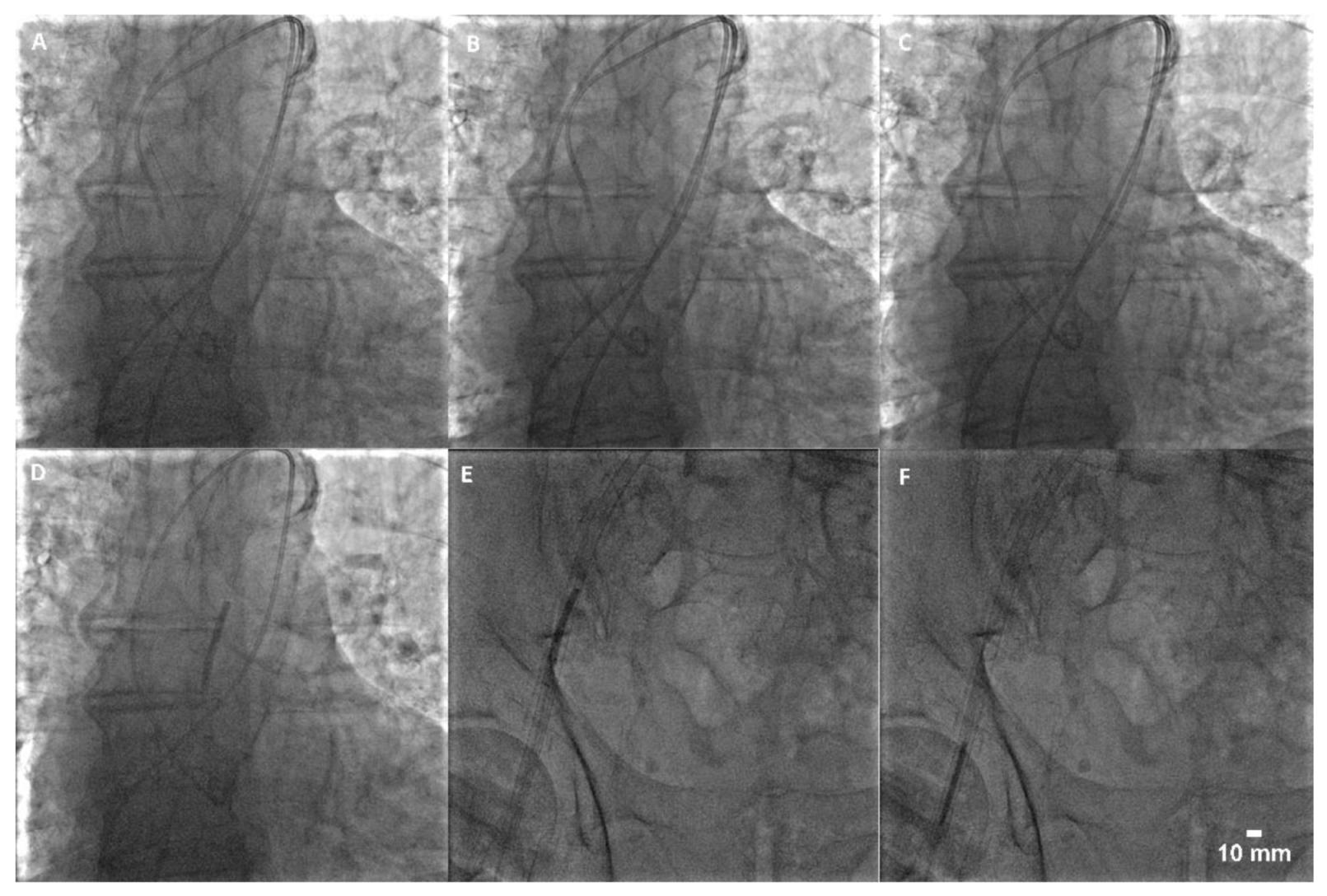
This satisfied the prerequisite for the Confida wire removal and the introduction of coronary guidewire BMW Universal (0.014”; Abbott™, Abbott Park, IL, USA) along with the rapid exchange balloon catheter SeQuent NEO (2.5 × 25 mm2; Bbraun™, Melsungen, Germany), which were placed over the severed sheath. The balloon was then inflated and slowly moved into the Medtronic Sentrant introducer sheath under the fluoroscopic guidance. The balloon was then deflated and together with the guidewire removed out of the sheath. This was followed by the introduction of the standard support J-wire (0.035″) and conjoint removal of the introducer sheath, AL2 catheter and the severed sheath (Figure 3). The introducer sheath was thereafter intersected to visualize the distal part of the severed femoral sheath (Figure 1).
Finally, a novel Medtronic Sentrant introducer sheath was placed in the right femoral artery over the standard support J-wire. Balloon predilatation (Z Med II Braun™; 28 × 40 mm; Bbraun, Melsungen, Germany) was first applied after which a successful implantation of the self-expanding valve Evolut R 34 (Medtronic™, Dublin, Ireland) was performed (Supplementary Figure S2). The access site was closed using a vascular closure device (VCD), namely Perclose Proglide (Abbott™, Abbott Park, IL, United States) and Angio-Seal VIP (Terumo™, Tokyo, Japan) (Supplementary Figure S3). Patient follow-up showed minimal paravalvular leak and did not reveal any access site complication. However, clinical impairment persisted with several subsequent hospitalizations due to acute decompensation of the chronic heart failure. There were no signs of clinically significant endovascular damage during the procedure itself and the follow-up period.
3. Discussion
This case report presents an unusual accidental event during peripheral large bore access which can develop in any percutaneous procedure and reveals a successful method for the recapture of the severed sheath. There are rare reports of sheath fracture during coronary angiography due to radial spasm [6] or catheter fracture due to excessive manipulation during femoral [7] and radial approaches [8]. Similar retrieval technique by a larger sheath were previously presented by Akkus et al. [7]. However, to the best of our knowledge, there are no case reports of successful a recapture of the severed sheath in the ascending aorta during TAVR procedure.
A post-procedural debriefing of the TAVR team detected that scalpel manipulation during skin tunneling probably caused accidental damage of the 6 French femoral sheath. This could therefore occur with any procedure that involves scalpel use for “tunnel” creation and is not restricted to TAVR. It must be emphasized that skin tunnelling should preferably be carried out without the sheath in situ (wire only), with the cutting edge of the scalpel facing away from the equipment. However, it is also important to emphasize that other routine actions such as the addition of local anesthetic could damage the sheath and cause local hematoma. Moreover, other emerging techniques such as ipsilateral dual artery sheath placement, or ipsilateral artery and vein puncture increase the risk of sheath damage. Finally, as previously described, this event is possible with sheath manipulation during any cardiac catheterization procedure, such as coronary angiography. Having in mind the complexity and associated risk of similar accidental events, it is important to prevent them. For example, the creation of “skin tunneling” over a micro-puncture access needle on the very initial access site puncture or over the wire can only help to avoid any accidental damage to a guidewire or catheter.
The presented maneuver for the recapture of the severed sheath in the ascending aorta is an unusual method. While the described technique could lead to potentially devastating complications such as intraventricular sheath entrapment, coronary artery embolization and peripheral embolization, the presented fragile patient was spared from the hypothetical surgical operation and sheath evacuation. Even though the sheath was successfully retrieved, it is a potentially risky technique and other standard methods for sheath recapture, such as the snaring technique, should be considered and emphasized. The lack of the vascular snare at the time of the procedure compelled us to carry out this unusual technique.
4. Conclusions
This case report brings out several important issues related to any percutaneous procedure. Firstly, accidental events such as sheath severing are possible and should be avoided by strict preventive measures and procedure standardization. Secondly, if a similar accidental event still occurs, s, the wire should be kept in its place during strategy planning and preferably continuously during the procedure. Having in mind its rare occurrence and extreme complexity, accidental events with equipment damage and/or discontinuity require a highly trained team. Therefore, teamwork when executing the SBAR technique and feedback loop is essential for success with regard to solving intra-procedural complications. Finally, operators performing large bore procedures must be familiar with different standard and bail-out strategies in order to cope with any unexpected accidental event or complication.
In conclusion, rare accidental events such as sheath severing are possible during any percutaneous procedure, and percutaneous recapture of the distal sheath part can be considered at the operator’s discretion. However, excellent knowledge about other standard recapturing methods, such as the snaring technique, is required for all operators performing large bore percutaneous procedures. Preventive measures, safe maneuvers and greater awareness should be encouraged to decrease the rate of similar accidental events.
Supplementary Materials
The following are available online at https://0-www-mdpi-com.brum.beds.ac.uk/article/10.3390/reports4040034/s1, Figure S1: Timeline, Figure S2: Successful implantation of the self-expanding aortic valve: A. implanted valve; B. aortography showing minimal paravalvular leak, Figure S3: Digital subtraction angiography after the application of vascular closure device: A. opacification of the proximal part of common femoral artery; B. opacification of the distal part of common femoral artery.
Author Contributions
Conceptualization: F.R., A.M., M.B. and I.K.; resources: F.R., M.B. and I.K.; writing—original draft: F.R., A.M., M.B., N.C. and I.K.; writing—review and editing: F.R., A.M., M.B., N.C. and I.K.; supervision: F.R., M.B., N.C. and I.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent was obtained from the patient(s) to publish this paper.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Otto, C.M.; Kumbhani, D.J.; Alexander, K.P.; Calhoon, J.H.; Desai, M.Y.; Kaul, S.; Lee, J.C.; Ruiz, C.E.; Vassileva, C.M. 2017 ACC Expert Consensus Decision Pathway for Transcatheter Aortic Valve Replacement in the Management of Adults with Aortic Stenosis. J. Am. Coll. Cardiol. 2017, 69, 1313–1346. [Google Scholar] [CrossRef]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P.; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e35–e71. [Google Scholar] [CrossRef]
- Scarsini, R.; De Maria, G.L.; Joseph, J.; Fan, L.; Cahill, T.J.; Kotronias, R.; Burzotta, F.; Newton, J.D.; Kharbanda, R.; Prendergast, B.; et al. Impact of Complications During Transfemoral Transcatheter Aortic Valve Replacement: How Can They Be Avoided and Managed? J. Am. Heart Assoc. 2019, 8, e013801. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry, M.A.; Sardar, M.R. Vascular complications of transcatheter aortic valve replacement: A concise literature review. World J. Cardiol. 2017, 9, 574–582. [Google Scholar] [CrossRef]
- Holmes, D.R.; Nishimura, R.A.; Grover, F.L.; Brindis, R.G.; Carroll, J.D.; Edwards, F.H.; Peterson, E.D.; Rumsfeld, J.S.; Shahian, D.M.; Thourani, V.H.; et al. Annual Outcomes with Transcatheter Valve Therapy. Ann. Thorac. Surg. 2016, 101, 789–800. [Google Scholar] [CrossRef] [Green Version]
- Athauda-Arachchi, P.; Dorman, S. Retention and fracture of a hydrophilic radial artery sheath due to severe spasm. Interv. Cardiol. 2012, 4, 57–60. [Google Scholar] [CrossRef]
- Akkus, N.I.; Bahadur, F.; Varma, J. Fracture of a guiding catheter in a tortuous iliac artery and its retrieval by a larger sheath. Rev. Port. Cardiol. 2013, 32, 341–344. [Google Scholar] [CrossRef]
- Lee, Y.-P.; Tan, H.-C.; Lee, C.-H. Complete fracture of an Ikari guiding catheter in the axillary artery during transradial coronary intervention. Int. J. Angiol. 2008, 17, 40–42. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Severed femoral sheath and its relation to the Medtronic Sentrant introducer sheath (14 French): (A) position in the introducer sheath; (B) two parts of the severed sheath.
Figure 1.
Severed femoral sheath and its relation to the Medtronic Sentrant introducer sheath (14 French): (A) position in the introducer sheath; (B) two parts of the severed sheath.

Figure 2.
Intra-aortic entrapment of the fractured sheath with the AL2 catheter after the Confida wire removal.
Figure 2.
Intra-aortic entrapment of the fractured sheath with the AL2 catheter after the Confida wire removal.

Figure 3.
Step-by-step recapture of the severed sheath: (A) wiring; (B) balloon crossing; (C) balloon capture; (D) balloon snaring (aorta); (E) balloon snaring (introducer sheath); (F) balloon deflation and evacuation.
Figure 3.
Step-by-step recapture of the severed sheath: (A) wiring; (B) balloon crossing; (C) balloon capture; (D) balloon snaring (aorta); (E) balloon snaring (introducer sheath); (F) balloon deflation and evacuation.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Runjić, F.; Matetic, A.; Bunc, M.; Crnčević, N.; Kristić, I. An Unusual Femoral Sheath Severing with Successful Recapture: A Case Report. Reports 2021, 4, 34. https://0-doi-org.brum.beds.ac.uk/10.3390/reports4040034
AMA Style
Runjić F, Matetic A, Bunc M, Crnčević N, Kristić I. An Unusual Femoral Sheath Severing with Successful Recapture: A Case Report. Reports. 2021; 4(4):34. https://0-doi-org.brum.beds.ac.uk/10.3390/reports4040034
Chicago/Turabian StyleRunjić, Frane, Andrija Matetic, Matjaž Bunc, Nikola Crnčević, and Ivica Kristić. 2021. "An Unusual Femoral Sheath Severing with Successful Recapture: A Case Report" Reports 4, no. 4: 34. https://0-doi-org.brum.beds.ac.uk/10.3390/reports4040034