
Prevalence and Factors Associated with Hygiene Behaviours among In-School Adolescents in Ghana

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Variables
2.2.1. Outcome Variables
2.2.2. Explanatory Variables
2.3. Statistical Analyses
2.4. Ethical Clearance
3. Results
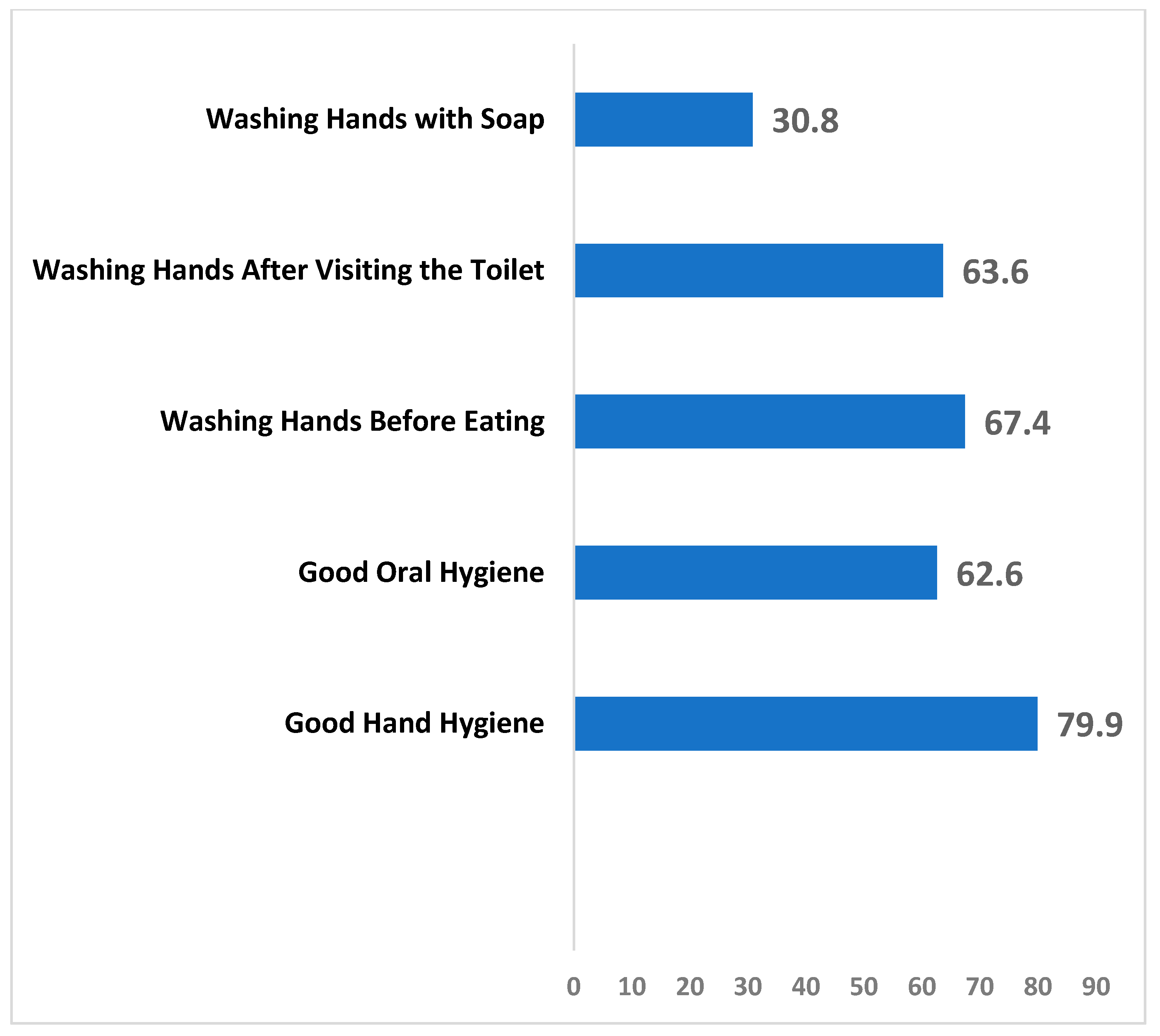
3.1. Descriptive Analysis on the Prevalence of Hygiene Behaviours
3.2. Relationship between Hygiene Behaviours and Explanatory Variables
3.3. Predictors of Hand Hygiene among In-School Adolescents
3.4. Predictors of Oral Hygiene among In-School Adolescents
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| COR | Crude Odds Ratio |
| AOR | Adjusted Odds Ratio |
| CI | Confidence Interval |
| WHO | World Health Organisation |
| CDC | Centers for Disease Control |
| STROBE | Strengthening the Reporting of Observational Studies in Epidemiology |
| GSHS | Ghana Global School-Based Health Survey |
| VIF | Variance Inflation Factor |
| GES | Ghana Education Service |
| WASH | Water, Sanitation, and Hygiene |
References
- WHO/UNICEF Joint Water Supply Sanitation Monitoring Programme. Progress on Drinking Water and Sanitation: 2014 Update; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Curtis, V.; Cairncross, S. Effect of washing hands with soap on diarrhoea risk in the community: A systematic review. Lancet Infect. Dis. 2003, 3, 275–281. [Google Scholar] [CrossRef]
- Curtis, V.; Schmidt, W.-P.; Luby, S.; Florez, R.; Touré, O.; Biran, A. Hygiene: New hopes, new horizons. Lancet Infect. Dis. 2011, 11, 312–321. [Google Scholar] [CrossRef]
- Dobe, M.; Mandal, R.N.; Jha, A. Social Determinants of Good Hand-Washing Practice (GHP) Among Adolescents in a Rural Indian Community. Fam. Community Health 2013, 36, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Pengpid, S.; Peltzer, K. Hygiene Behaviour and Associated Factors among In-School Adolescents in Nine African Countries. Int. J. Behav. Med. 2011, 18, 150–159. [Google Scholar] [CrossRef]
- Peltzer, K.; Pengpid, S. Oral and Hand Hygiene Behaviour and Risk Factors among In-School Adolescents in Four Southeast Asian Countries. Int. J. Environ. Res. Public Health 2014, 11, 2780–2792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anand, D.; Prakash, S. Assessment of the hygiene and sanitation practices of students of class VI to IX in urban government inter college at Allahabad district, India. Int. J. Community Med Public Health 2018, 5, 3870–3875. [Google Scholar] [CrossRef]
- Ranasinghe, S.; Ramesh, S.; Jacobsen, K.H. Hygiene and mental health among middle school students in India and 11 other countries. J. Infect. Public Health 2016, 9, 429–435. [Google Scholar] [CrossRef] [Green Version]
- Cruz, J.P.; Bashtawi, M.A. Predictors of hand hygiene practice among Saudi nursing students: A cross-sectional self-reported study. J. Infect. Public Health 2016, 9, 485–493. [Google Scholar] [CrossRef] [Green Version]
- Kassak, K.M.; Dagher, R.; Doughan, B. Oral hygiene and lifestyle cor-2. relates among new undergraduate university students in Leba-non. J. Am. Coll. Health 2001, 50, 15–20. [Google Scholar] [CrossRef]
- Kakudate, N.; Morita, M.; Sugai, M.; Kawanami, M. Systematic cognitive behavioral approach for oral hygiene instruction: A short-term study. Patient Educ. Couns. 2009, 74, 191–196. [Google Scholar] [CrossRef]
- Liu, Z.; Zhang, W.; Zhang, J.; Zhou, X.; Zhang, L.; Song, Y.; Wang, Z. Oral hygiene, periodontal health and chronic obstructive pulmonary disease exacerbations. J. Clin. Periodontol. 2011, 39, 45–52. [Google Scholar] [CrossRef]
- Honkala, S.; Honkala, E.; Al-Sahli, N. Do life-or school-satisfaction and self-esteem indicators explain the oral hygiene habits of schoolchildren? Community Dent. Oral Epidemiol. 2007, 35, 337–347. [Google Scholar] [CrossRef]
- Polk, D.E.; Weyant, R.J.; Manz, M.C. Socioeconomic factors in adolescents’ oral health: Are they mediated by oral hygiene behaviors or preventive interventions? Community Dent. Oral Epidemiol. 2010, 38, 1–9. [Google Scholar] [CrossRef]
- Siziya, S.; Muula, A.S.; Rudatsikira, E. Self-reported poor oral hygiene among in-school adolescents in Zambia. BMC Res. Notes 2011, 4, 255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maes, L.; Vereecken, C.; Vanobbergen, J.; Honkala, S. Tooth brushing and social characteristics of families in 32 countries. Int. Dent. J. 2006, 56, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Zhou, G.; Jiang, T.; Knoll, N.; Schwarzer, R. Improving hand hygiene behaviour among adolescents by a planning intervention. Psychol. Health Med. 2015, 20, 824–831. [Google Scholar] [CrossRef]
- Mastin, D.F.; Bryson, J.; Corwyn, R. Assessment of Sleep Hygiene Using the Sleep Hygiene Index. J. Behav. Med. 2006, 29, 223–227. [Google Scholar] [CrossRef]
- Vivas, A.P.; Gelaye, B.; Aboset, N.; Kumie, A.; Berhane, Y.; Williams, M.A. Knowledge, attitudes and practices (KAP) of hygiene among school children in Angolela, Ethiopia. J. Prev. Med. Hyg. 2010, 51, 73. [Google Scholar]
- Okemwa, K.A.; Gatongi, P.M.; Rotich, J.K. The oral health knowledge and hygiene practices among primary school children aged 5–17 years in a rural area of Uasin Gishu District, Kenya. J. Dent. Oral Hyg. 2010, 7, 187–196. [Google Scholar]
- Blay, D.; Åstrøm, A.N.; Haugejorden, O. Oral hygiene and sugar consumption among urban and rural adolescents in Ghana. Community Dent. Oral Epidemiol. 2000, 28, 443–450. [Google Scholar] [CrossRef]
- Danquah, L.; Awuah, E.; Mensah, C.M.; Agyemang, S. Sanitation and hygiene practices in relation to childhood diarrhoea prevalence: The case of households with children under-five years in Ghana. Sci. J. Public Health 2014, 2, 19–125. [Google Scholar]
- George Amponsah, A.; Ekua Anamoaba, B. Evaluation of food hygiene knowledge attitudes and practices of food handlers in food businesses in Accra, Ghana. Food and Nutrition sciences. Food Nutr. Sci. 2011, 17, 317–322. [Google Scholar]
- Yawson, A.E.; Hesse, A.A.J. Hand hygiene practices and resources in a teaching hospital in Ghana. J. Infect. Dev. Ctries. 2013, 7, 338–347. [Google Scholar] [CrossRef] [Green Version]
- Mariwah, S.; Hampshire, K.; Kasim, A. The impact of gender and physical environment on the handwashing behaviour of university students in Ghana. Trop. Med. Int. Health 2012, 17, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Monney, I.; Agyei, D.; Ewoenam, B.S.; Priscilla, C.; Nyaw, S. Food hygiene and safety practices among street food vendors: An assessment of compliance, institutional and legislative framework in Ghana. Food Public Health 2014, 4, 306–315. [Google Scholar]
- Scott, B.; Curtis, V.; Rabie, T.; Garbrah-Aidoo, N. Health in our hands, but not in our heads: Understanding hygiene motivation in Ghana. Heal. Policy Plan. 2007, 22, 225–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control (CDC). Global School-Based Student Health Survey. 2015. Available online: https://www.cdc.gov/gshs/index.htm (accessed on 27 January 2021).
- Asante, K.O.; Kugbey, N.; Osafo, J.; Quarshie, E.N.-B.; Sarfo, J.O. The prevalence and correlates of suicidal behaviours (ideation, plan and attempt) among adolescents in senior high schools in Ghana. SSM Popul. Health 2017, 3, 427–434. [Google Scholar] [CrossRef]
- Ray, S.K.; Amarchand, R.; Srikanth, J.; Majumdar, K.K. A study on prevalence of bacteria in the hands of children and their perception on hand washing in two schools of Bangalore and Kolkata. Indian J. Public Health 2011, 55, 293. [Google Scholar] [CrossRef]
- Yao, K.; Yao, Y.; Shen, X.; Lu, C.; Guo, Q. Assessment of the oral health behavior, knowledge and status among dental and medical undergraduate students: A cross-sectional study. BMC Oral Health 2019, 19, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghana Education Service. School Health Education Programme Unit: WASH in School; Annual Report; Ghana Education Service: Accra, Ghana, 2012. [Google Scholar]
- Mooijman, A.; Esseku, H.; Tay, V. National Implementation Model: WASH in Schools; Ghana Education Service: Accra, Ghana, 2013. [Google Scholar]
- McMichael, C. Water, Sanitation and Hygiene (WASH) in Schools in Low-Income Countries: A Review of Evidence of Impact. Int. J. Environ. Res. Public Health 2019, 16, 359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development; United Nations: New York, NY, USA, 2015. [Google Scholar]
- Mbawalla, H.S.; Masalu, J.R.; Åstrøm, A.N. Socio-demographic and behavioural correlates of oral hygiene status and oral health related quality of life, the Limpopo-Arusha school health project (LASH): A cross-sectional study. BMC Paediatr. 2010, 10, 87. [Google Scholar] [CrossRef] [Green Version]
- Che Salleh, N.; Mohamad Anuar, M.F.; Abdullah, N.A.; Yaw, S.L.; Ibrahim Wong, N.; Teck Pei, T.; Awaluddin, S.M.; Aris, T. Prevalence and Factors Associated With Oral and Hand Hygiene Practices Among Adolescents in Malaysia: Findings From the National Health and Morbidity Survey 2017. Asia Pac. J. Public Health 2019, 31, 97S–104S. [Google Scholar] [CrossRef]
- Garbutt, C.; Simmons, G.; Patrick, D.; Miller, T. The public hand hygiene practices of New Zealanders: A national survey. N. Z. Med. J. 2007, 120, 1265. [Google Scholar]
- Pickering, A.J.; Blum, A.G.; Breiman, R.F.; Ram, P.K.; Davis, J. Video Surveillance Captures Student Hand Hygiene Behavior, Reactivity to Observation, and Peer Influence in Kenyan Primary Schools. PLoS ONE 2014, 9, e92571. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Outcome Variables | Questions | Coding |
|---|---|---|
| Oral Hygiene | During the past 30 days, how many times per day did you usually clean or brush your teeth? | 1 = I did not clean or brush my teeth during the past 30 days 2 = less than 1 time per day 3 = 1 time per day 4 = 2 times per day 5 = 3 times per day 6 = 4 or more times per day (coded 1–3 = 0, 4–6 = 1) |
| Handwashing | During the past 30 days, how often did you wash your hands before eating? (a) | 1 = never, 2 = rarely, 3 = sometimes, 4 = most of the times, 5 = always (coded 1–4 = 0, 5 = 1) |
| Handwashing with soap | During the past 30 days, how often did you use soap when washing your hands? (b) | 1 = never, 2 = rarely, 3 = sometimes, 4 = most of the times, 5 = always (coded 1–4 = 0, 5 = 1) |
| Hand washing after toilet | During the past 30 days, how often did you wash your hands after using the toilet or latrine? (c) | 1 = never, 2 = rarely, 3 = sometimes, 4 = most of the times, 5 = always (coded 1–4 = 0, 5 = 1) |
| Hand hygiene | Hand hygiene created from a–c | Coded as 1 = Always for those who indicated always to all three questions and 0 otherwise |
| Explanatory variables | ||
| Suicidal ideation | During the past 12 months, did you ever seriously consider attempting suicide? | 1 = Yes 0 = No coded (1 = Yes and 0 = No) |
| Suicide plan | During the past 12 months, did you make a plan about how you would attempt suicide? | 1 = Yes 0 = No coded (1 = Yes and 0 = No) |
| Suicidal Attempt | During the past 12 months, how many times did you actually attempt suicide? | During the past 12 months, how many times did you actually attempt suicide? |
| Age | Custom age | 1 = 12, 2 = 13, 3 = 14, 4 = 15, 5 = 16, 6 = 17, 7 = 18 years (coded 0 = 12–17, 18 years = 1) |
| Sex | Sex | 1 = male, 2 = female |
| Grade | In what grade are you? | 1 = SHS1, 2 = SHS2, 3 = SHS3, 4 = SHS4 |
| Hunger | Went hungry past 30 days | 1 = never, 2 = rarely, 3 = sometimes, 4 = most of the times, 5 = always (coded 1–3 = 0, 4–5 = 1) |
| Tobacco use | During the past 30 days, on how many days did you use any other form of tobacco, such as chewing tobacco leaves? | 1 = 0 days; to 7 = all 30 days (coded 1 = 0; and 2–7 = 1) |
| Alcohol use | During the past 30 days, on how many days did you have at least one drink containing alcohol? | 1 = 0 days to 7 = All 30 days (coded 1 = 0; and 2–7 = 1) |
| Truancy | During the past 30 days, on how many days did you miss classes or school without permission? | 1 = 0 days,2= 1 or 2 days, 3 = 3 to 5 days, 4 = 6 to 9 days, 5= 10 or more (coded 1 = 0 and 2–5 = 1) |
| Fighting | During the past 12 months, how many times were you in a physical fight? | 1 = 0 times; to 8 = 12 or more times (coded 1 = 0; and 2–8 = 1) |
| Bullied | During the past 30 days, how were you bullied most often? | 1 = 0 times; to 8 = 12 or more times (coded 1 = 0; and 2–7 = 1) |
| Attacked | During the past 12 months, how many times were you physically attacked? | 1 = 0 days,2= 1 or 2 days, 3 = 3 to 5 days, 4 = 6 to 9 days, 5= 10 or more (coded 1 = 0 and 2–5 = 1) |
| Injury | During the past 12 months, how many times were you seriously injured?’ | 1 = 0 times to 8 = 12 or more times (coded as 1 = 0 and 2–8 = 1) |
| Close friends | How many close friends do you have? | 1 = 0 to 4 = 3 or more (coded 1 = 0, 1–2 = 1, 3 or more = 2) |
| Loneliness | During the past 12 months, how many times have you felt lonely? | 1 = never, 2 = rarely, 3 = sometimes, 4 = most of the time to 5 = always (coded 1 = 0 and 4–5 = 1) |
| Peer Support | During the past 30 days, how often were most of the students in your school kind and helpful? | 1 = never, 2 = rarely, 3 = sometimes, 4 = most of the time, 5 = always (coded 1–3 = 0; and 4–5 = 1) |
| Parents check homework (Parental Supervision) | During the past 30 days, how often did your parents or guardians check to see if your homework was done? | 1 = never, 2 = rarely, 3 = sometimes, 4 = most of the time, 5 = always (coded 1–3 = 0; and 4–5 = 1) |
| Understand problems (Parental Connectedness | During the past 30 days, how often did your parents or guardians understand your problems and worries? | 1 = never, 2 = rarely, 3 = sometimes, 4 = most of the time, 5 = always (coded 1–3 = 0; and 4–5 = 1) |
| Know what adolescents do in their free time (Parental or Guardian Bonding) | During the past 30 days, how often did your parents or guardians really know what you were doing with your free time? | 1 = never, 2 = rarely, 3 = sometimes, 4 = most of the time, 5 = always (coded 1–3 = 0; and 4–5 = 1) |
| Parental Intrusion | During the past 30 days, how often did your parents or guardians go through your things without your approval? | 1 = never, 2 = rarely, 3 = sometimes, 4 = most of the time, 5 = always (coded 1–3 = 0; and 4–5 = 1) |
| Variables | Weighted N | Weighted % | Good Oral Hygiene | p-Value | Good Hand Hygiene | p-Value |
|---|---|---|---|---|---|---|
| Age | 0.835 | 0.011 | ||||
| 12–17 years | 606 | 44.9 | 79.6 | 58.1 | ||
| 18 years | 742 | 55.1 | 79.2 | 64.9 | ||
| Sex | 0.246 | 0.250 | ||||
| Male | 690 | 51.2 | 78.2 | 60.4 | ||
| Female | 658 | 48.8 | 80.8 | 63.4 | ||
| Grade | 0.570 | 0.605 | ||||
| SHS1 | 332 | 24.6 | 78.8 | 62.6 | ||
| SHS2 | 351 | 26.0 | 81.6 | 64.1 | ||
| SHS3 | 370 | 27.5 | 80.1 | 59.3 | ||
| SHS4 | 295 | 21.9 | 76.9 | 62.1 | ||
| Ever Went Hungry | 0.032 | 0.790 | ||||
| No | 544 | 40.3 | 82.2 | 61.3 | ||
| Yes | 804 | 59.7 | 77.4 | 62.0 | ||
| Suicidal Ideation | 0.695 | 0.136 | ||||
| No | 1132 | 84.0 | 79.6 | 60.9 | ||
| Yes | 216 | 16.0 | 78.4 | 66.4 | ||
| Suicidal Plan | 0.683 | <0.001 | ||||
| No | 1063 | 78.9 | 79.6 | 58.8 | ||
| Yes | 285 | 21.1 | 78.5 | 72.8 | ||
| Suicidal Attempt | 0.782 | <0.001 | ||||
| No | 1080 | 80.1 | 79.2 | 59.1 | ||
| Yes | 268 | 19.9 | 80.0 | 72.7 | ||
| Tobacco Use | 0.046 | 0.268 | ||||
| No | 1279 | 94.9 | 79.9 | 61.4 | ||
| Yes | 69 | 5.2 | 69.7 | 68.2 | ||
| Alcohol Use | <0.001 | 0.229 | ||||
| No | 1184 | 87.8 | 81.1 | 62.3 | ||
| Yes | 164 | 12.2 | 66.7 | 57.4 | ||
| Ever Engaged in a Fight | 0.001 | 0.581 | ||||
| No | 968 | 71.8 | 81.6 | 61.3 | ||
| Yes | 380 | 28.2 | 73.7 | 62.9 | ||
| Truancy | <0.001 | 0.002 | ||||
| No | 921 | 68.3 | 82.7 | 64.5 | ||
| Yes | 427 | 31.7 | 71.9 | 55.5 | ||
| Ever Experienced Bullying | 0.001 | 0.005 | ||||
| No | 776 | 57.6 | 82.4 | 58.6 | ||
| Yes | 572 | 42.4 | 75.1 | 66.1 | ||
| Attacked Colleagues | 0.008 | 0.178 | ||||
| No | 853 | 63.3 | 81.6 | 60.4 | ||
| Yes | 495 | 36.7 | 75.5 | 64.1 | ||
| Sustained an Injury | 0.011 | 0.396 | ||||
| No | 633 | 47.0 | 82.3 | 60.6 | ||
| Yes | 715 | 53.0 | 76.7 | 62.8 | ||
| Have Close Friends | 0.156 | 0.866 | ||||
| No | 178 | 13.2 | 83.4 | 61.1 | ||
| Yes | 1170 | 86.8 | 78.8 | 61.8 | ||
| Feeling Lonely | 0.211 | 0.573 | ||||
| No | 1098 | 81.4 | 80.0 | 62.1 | ||
| Yes | 250 | 18.6 | 76.5 | 60.2 | ||
| Peer Support | 0.428 | 0.985 | ||||
| No | 243 | 18.1 | 77.5 | 61.7 | ||
| Yes | 1105 | 82.0 | 79.8 | 61.7 | ||
| Parents Checking Homework (Parental Supervision) | <0.001 | <0.001 | ||||
| No | 785 | 58.2 | 73.3 | 52.6 | ||
| Yes | 563 | 41.8 | 87.9 | 74.5 | ||
| Parents or Guardians Understand Problems (Parental Connectedness) | 0.001 | 0.003 | ||||
| No | 744 | 55.2 | 76.0 | 58.2 | ||
| Yes | 604 | 44.8 | 83.5 | 66.0 | ||
| Parents or Guardians Know What Adolescent Does in Their Free Time (Parental Bonding) | <0.001 | <0.001 | ||||
| No | 811 | 60.2 | 75.3 | 56.3 | ||
| Yes | 537 | 39.8 | 85.6 | 70.0 | ||
| Parents Going Through Things Without Adolescents’ Approval (Parental Intrusion at Home) | 0.187 | 0.002 | ||||
| No | 1132 | 84.0 | 78.8 | 60.0 | ||
| Yes | 216 | 16.0 | 82.8 | 71.3 | ||
| Variable | Model I COR (95% CI) | Model II AOR (95% CI) |
|---|---|---|
| Ever Went Hungry | ||
| No | Ref | Ref |
| Yes | * 0.74 (0.57–0.98) | 0.96 (0.72–1.28) |
| Truancy | ||
| No | Ref | Ref |
| Yes | * 0.53 (0.41–0.70) | * 0.69 (0.51–0.92) |
| Ever Experienced Bullying | ||
| No | Ref | Ref |
| Yes | * 0.64 (0.49–0.84) | * 0.70 (0.52–0.94) |
| Parents Checking Homework (Parental Supervision) | ||
| No | Ref | Ref |
| Yes | *** 2.63 (1.96–3.56) | *** 2.30 (1.64–2.31) |
| Parents or Guardians Know What Adolescent Does in Their Free Time (Parental Bonding) | ||
| No | Ref | Ref |
| Yes | ** 1.94 (1.46–2.60) | 1.34 (0.98–1.89) |
| Parents or Guardians Understand Problems (Parental Connectedness) | ||
| No | Ref | Ref |
| Yes | ** 1.60 (1.22–2.10) | 1.06 (0.78–1.43) |
| Experiencing an Attack | ||
| No | Ref | Ref |
| Yes | ** 0.70 (0.53–0.91) | 0.87 (0.64–1.16) |
| Sustaining an Injury | ||
| No | Ref | Ref |
| Yes | ** 0.71 (0.54–0.93) | 0.90 (0.66–1.21) |
| Tobacco Use | ||
| No | Ref | Ref |
| Yes | * 0.58 (0.33–0.99) | 0.84 (0.48–1.46) |
| Engaging in a Fight | ||
| No | Ref | Ref |
| Yes | ** 0.63 (0.48–0.84) | 0.79 (0.58–1.07) |
| N | 1348 | 1348 |
| R2 | 0.058 | |
| Variable | Model I COR (95% CI) | Model II AOR (95% CI) |
|---|---|---|
| Age | ||
| 12–17 years | Ref | Ref |
| 18 years | *** 1.33 (1.07–1.66) | 1.67 *** (1.32–2.12) |
| Truancy | ||
| No | Ref | Ref |
| Yes | ** 0.69 (0.54–0.87) | 0.72 * (0.56–0.92) |
| Ever Experienced Bullying | ||
| No | Ref | Ref |
| Yes | ** 1.38 (1.10–1.72) | 1.26 (0.987–1.61) |
| Suicidal Plan | ||
| No | Ref | Ref |
| Yes | 1.87 (1.40–2.50) | 1.56 * (1.08–2.25) |
| Suicidal Attempt | ||
| No | Ref | Ref |
| Yes | 1.84 (1.37–2.48) | 1.42 (0.96–2.09) |
| Parents Checking Homework (Parental supervision) | ||
| No | Ref | Ref |
| Yes | *** 2.63 (2.08–3.33) | 2.34 *** (1.80–3.04) |
| Parents or Guardians Know What Adolescent Does in Their Free Time (Parental Bonding) | ||
| No | Ref | Ref |
| Yes | *** 1.82 (1.44–2.29) | 1.35 * (1.04–1.75) |
| Parents Going Through Things Without Adolescents’ Approval (Parental Intrusion at Home) | ||
| No | Ref | Ref |
| Yes | 1.66 (1.20–2.29) | 1.18 (0.84–1.66) |
| N | 1348 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seidu, A.-A.; Amu, H.; Salihu, T.; Hagan, J.E., Jr.; Agbaglo, E.; Amoah, A.; Abodey, E.; Boateng, M.A.; Ahinkorah, B.O. Prevalence and Factors Associated with Hygiene Behaviours among In-School Adolescents in Ghana. J 2021, 4, 169-181. https://0-doi-org.brum.beds.ac.uk/10.3390/j4020014
Seidu A-A, Amu H, Salihu T, Hagan JE Jr., Agbaglo E, Amoah A, Abodey E, Boateng MA, Ahinkorah BO. Prevalence and Factors Associated with Hygiene Behaviours among In-School Adolescents in Ghana. J. 2021; 4(2):169-181. https://0-doi-org.brum.beds.ac.uk/10.3390/j4020014
Chicago/Turabian StyleSeidu, Abdul-Aziz, Hubert Amu, Tarif Salihu, John Elvis Hagan, Jr., Ebenezer Agbaglo, Abigail Amoah, Eric Abodey, Margaret Abokoma Boateng, and Bright Opoku Ahinkorah. 2021. "Prevalence and Factors Associated with Hygiene Behaviours among In-School Adolescents in Ghana" J 4, no. 2: 169-181. https://0-doi-org.brum.beds.ac.uk/10.3390/j4020014