
A Comparison of Post-Operative Occlusion with 3-D vs. 2-D Miniplate Fixation in the Management of Isolated Mandibular Angle Fractures


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maurer, P.; Eckert, A.W.; Kriwalsky, M.S.; Schubert, J. Scope and limitations of methods of mandibular reconstruction: A long-term follow-up. Br. J. Oral Maxillofac. Surg. 2010, 48, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Qiamuddin. Analysis of 362 cases of maxillofacial injuries in northern region of Pakistan. Pak. Oral Dent. J. 1991, 11, 35–43. [Google Scholar]
- Kim, K.; Ibrahim, A.M.S.; Koolen, P.G.L.; Lee, B.T.; Lin, S.J. Trends in Facial Fracture Treatment Using the American College of Surgeons National Surgical Quality Improvement Program Database. Plast. Reconstr. Surg. 2014, 133, 627–638. [Google Scholar] [CrossRef] [PubMed]
- Vyas, A.; Mazumdar, U.; Khan, F.; Mehra, M.; Parihar, L.; Purohit, C. A study of mandibular fractures over a 5-year period of time: A retrospective study. Contemp. Clin. Dent. 2014, 5, 452–455. [Google Scholar] [CrossRef]
- Sehgal, S.; Ramanujam, L.; Prasad, K.; Krishnappa, R. Three-dimensional v/s standard titanium miniplate fixation in the management of mandibular fractures–A randomized clinical study. J. Cranio-Maxillofac. Surg. 2015, 42, 1292–1299. [Google Scholar] [CrossRef]
- Amjad, S.; Adnan Ali, S.; Abdus, S. Pattern and management of mandibular fractures: A study conducted on 264 patients. Pak. Oral Dent. J. 2007, 27, 103–106. [Google Scholar]
- Gadicherla, S.; Sasikumar, P.; Gill, S.S.; Bhagania, M.; Kamath, A.T.; Pentapati, K.C. Mandibular Fractures and Associated Factors at a Tertiary Care Hospital. Arch. Trauma Res. 2016, 5, e30574. [Google Scholar] [CrossRef] [Green Version]
- Tiwari, A.; Lata, J.; Mishra, M. Influence of the impacted mandibular third molars on fractures of the mandibular angle and condyle—A prospective clinical study. J. Oral Biol. Craniofacial Res. 2016, 6, 227–230. [Google Scholar] [CrossRef] [Green Version]
- Al-Moraissi, E.A.; Ellis, E. What Method for Management of Unilateral Mandibular Angle Fractures Has the Lowest Rate of Postoperative Complications? A Systematic Review and Meta-Analysis. J. Oral Maxillofac. Surg. 2014, 72, 2197–2211. [Google Scholar] [CrossRef]
- Lee, J.-H. Treatment of Mandibular Angle Fractures. Arch. Craniofacial Surg. 2017, 18, 73–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zanakis, S.; Tasoulas, J.; Angelidis, I.; Dendrinos, C. Tooth in the line of angle fractures: The impact in the healing process. A retrospective study of 112 patients. J. Cranio-Maxillofac. Surg. 2015, 43, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Danda, A.K. Comparison of a Single Noncompression Miniplate Versus 2 Noncompression Miniplates in the Treatment of Mandibular Angle Fractures: A Prospective, Randomized Clinical Trial. J. Oral Maxillofac. Surg. 2010, 68, 1565–1567. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, J.O.; Jensen, S.S.; Kofod, T.; Schwartz, O.; Hillerup, S. Open or closed repositioning of mandibular fractures: Is there a difference in healing outcome? A systematic review. Int. Assoc. Dent. Traumatol. 2008, 24, 17–21. [Google Scholar] [CrossRef]
- Tams, J.; van Loon, J.-P.; Otten, B.; Bos, R.R. A computer study of biodegradable plates for internal fixation of mandibular angle fractures. J. Oral Maxillofac. Surg. 2001, 59, 404–407. [Google Scholar] [CrossRef]
- Zhu, W. Failure Analysis of the Superior Lateral Plate Technique for Mandibular Angle Fractures. J. Oral Maxillofac. Surg. 2019, 77, 107–108. [Google Scholar] [CrossRef]
- Champy, M.; Loddé, J.; Schmitt, R.; Jaeger, J.; Muster, D. Mandibular osteosynthesis by miniature screwed plates via a buccal approach. J. Maxillofac. Surg. 1978, 6, 14–21. [Google Scholar] [CrossRef]
- Yazdani, J.; Talesh, K.T.; Hosein, M.; Motamedi, K.; Fekri, S.; Hajmohammadi, S. Mandibular Angle Fractures: Comparison of One Miniplate vs. Two Mini- plates. Trauma Mon. 2013, 18, 17–20. [Google Scholar] [CrossRef]
- Alkan, A.; Çelebi, N.; Özden, B.; Baş, B.; Inal, S. Biomechanical comparison of different plating techniques in repair of mandibular angle fractures. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2007, 104, 752–756. [Google Scholar] [CrossRef]
- Sadhwani, B.S.; Anchlia, S. Conventional 2.0 mm miniplates versus 3-D plates in mandibular fractures. Ann. Maxillofac. Surg. 2013, 3, 154–159. [Google Scholar] [CrossRef] [Green Version]
- Farmand, M.; Dupoirieux, L. The value of 3-dimensional plates in maxillofacial surgery. Rev. De Stomatol. Et De Chir. Maxillo-Faciale 1992, 93, 353–357. [Google Scholar]
- Singh, R.K.; Chand, S.; Pal, U.S.; Das, S.K.; Sinha, V.P. Matrix miniplate versus locking miniplate in the management of displaced mandibular angle fractures. Natl. J. Maxillofac. Surg. 2013, 4, 225–228. [Google Scholar] [CrossRef] [Green Version]
- Wusiman, P.; Taxifulati, D.; Weidong, L.; Moming, A. Three-dimensional versus standard miniplate, lag screws versus miniplates, locking plate versus non-locking miniplates: Management of mandibular fractures, a systematic review and meta-analysis. J. Dent. Sci. 2019, 14, 66–80. [Google Scholar] [CrossRef]
- Bohner, L.; Beiglboeck, F.; Schwipper, S.; Lustosa, R.M.; Segura, C.P.M.; Kleinheinz, J.; Jung, S. Treatment of Mandible Fractures Using a Miniplate System: A Retrospective Analysis. J. Clin. Med. 2020, 9, 2922. [Google Scholar] [CrossRef] [PubMed]
- Erdmann, D.; Follmar, K.E.; DeBruijn, M.; Bruno, A.D.; Jung, S.-H.; Edelman, D.; Mukundan, S.; Marcus, J.R. A Retrospective Analysis of Facial Fracture Etiologies. Ann. Plast. Surg. 2008, 60, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Gutta, R.; Tracy, K.; Johnson, C.; James, L.E.; Krishnan, D.G.; Marciani, R.D. Outcomes of Mandible Fracture Treatment at an Academic Tertiary Hospital: A 5-Year Analysis. J. Oral Maxillofac. Surg. 2014, 72, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Schierle, H.P.; Schmelzeisen, R.; Rahn, B. Experimental studies of the biomechanical stability of different miniplate configurations for the mandibular angle. Kiefer Gesichts-Chir. 1996, 41, 166–170. [Google Scholar]
- Vineeth, K.; Lalitha, R.M.; Prasad, K.; Ranganath, K.; Shwetha, V.; Singh, J. “A comparative evaluation between single noncompression titanium miniplate and three dimensional titanium miniplate in treatment of mandibular angle fracture”—A randomized prospective study. J. Cranio-Maxillofac. Surg. 2013, 41, 103–109. [Google Scholar] [CrossRef]
- Al-Tairi, N.; Shoushan, M.; Khedr, M.S.; Abd-Alal, S. Comparison of three-dimensional plate versus double miniplate osteosynthesis for treatment of unfavorable mandibular angle fractures. Tanta Dent. J. 2015, 12, 89–98. [Google Scholar] [CrossRef]
- Al-Moraissi, E.; Mounair, R.; El-Sharkawy, T.; El-Ghareeb, T. Comparison between three-dimensional and standard miniplates in the management of mandibular angle fractures: A prospective, randomized, double-blind, controlled clinical study. Int. J. Oral Maxillofac. Surg. 2015, 44, 316–321. [Google Scholar] [CrossRef]
- Wusiman, P.; Nie, B.; Li, W.D.; Moming, A. Management of mandibular angle fractures using 3- dimensional or standard miniplates: A systematic review and meta-analysis. J. Cranio-Maxillofac. Surg. 2019, 47, 622–628. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Patients above 16 years diagnosed with isolated mandibular angle fractures | Previously treated mandibular angle fractures |
| Infected fractures | |
| Comminuted fractures | |
| Completely edentulous patients | |
| Medically compromised patients |
| Gender Distribution | ||||
|---|---|---|---|---|
| Group A | Group B | Total | p-Value | |
| Males | 30 (57.7%) | 42 (80.8%) | 72 (69.2%) | 0.02 |
| Females | 22 (42.3% | 10 (19.2%) | 32 (30.8) | |
| Etiology of Fractures | ||||
| Fall | 28 (53.8%) | 8 (15.4%) | 36 (34.6%) | 0.01 |
| RTA | 20 (38.5) | 38 (73.1%) | 58 (55.8%) | |
| Assault | 4 (7.7%) | 6 (11.5%) | 10 (9.6%) | |
| Age Group | ||||
| 16–30 | 27 (51.9%) | 43 (82.7%) | 70 (67.8%) | 0.01 |
| 31–40 | 22 (42.3%) | 7 (13.5%) | 29 (27.9) | |
| 41–60 | 3 (5.8%) | 2 (3.8%) | 5 (4.8%) | |
| Total | 52 (100%) | 52 (100%) | 104 (100%) | |
| Group A | Group B | Total | p-Value | |
|---|---|---|---|---|
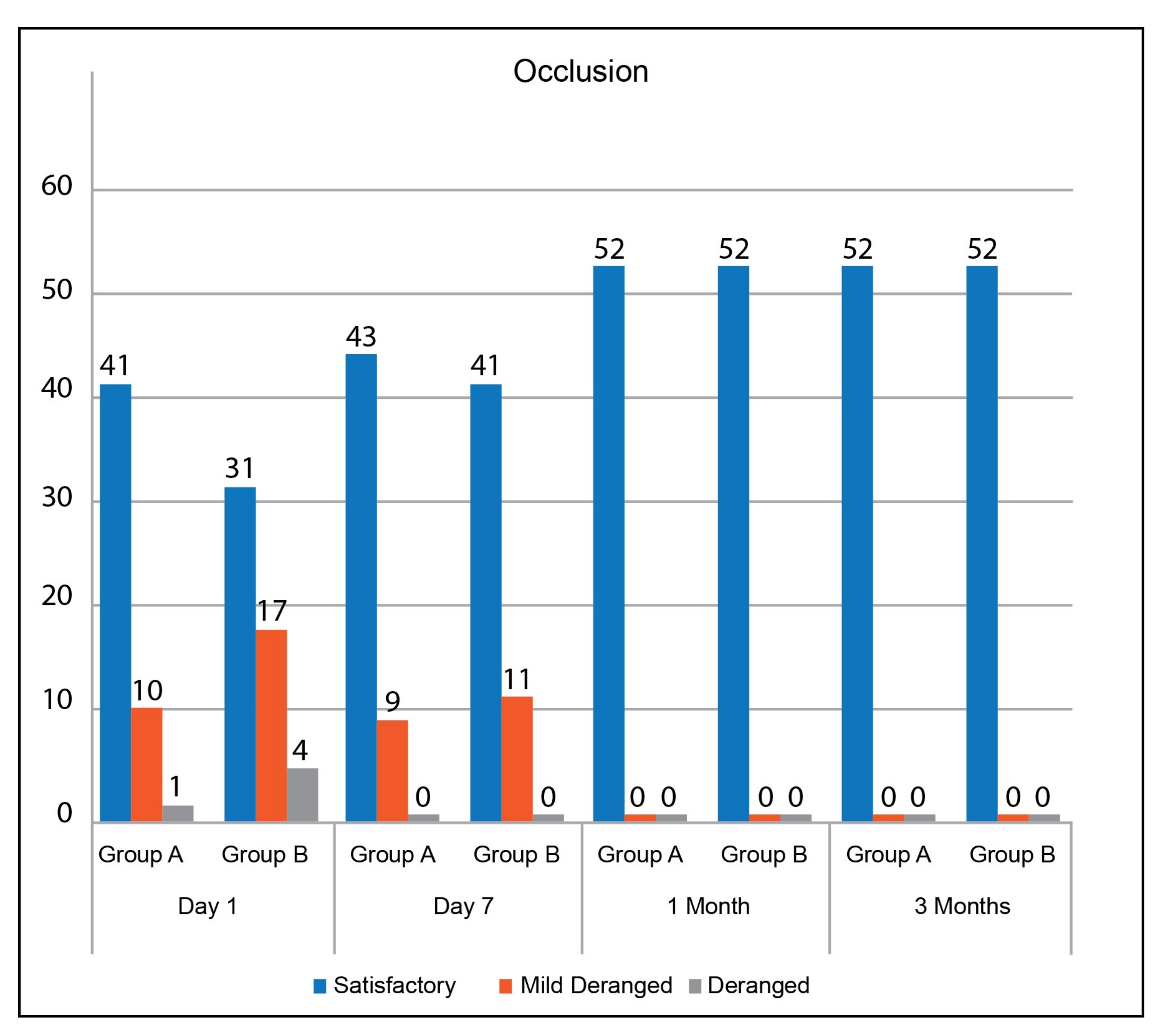
| Occlusion Day 1 | ||||
| Satisfactory | 41 (78.8%) | 31 (59.6%) | 72 (69.2%) | 0.11 |
| Mildly Deranged | 10 (19.2%) | 17 (32.7%) | 27 (26.0%) | |
| Deranged | 1 (1.9%) | 4 (7.7%) | 5 (4.8%) | |
| Occlusion Day 7 | ||||
| Satisfactory | 43 (82.7%) | 41 (78.8%) | 84 (80.8%) | 0.62 |
| Mildly Deranged | 9 (17.3%) | 11 (21.2%) | 20 (19.2%) | |
| Deranged | 0 | 0 | 0 | |
| Total | 52 (100%) | 52 (100%) | 104 (100%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mujtaba, A.; Malik, N.R.; Umer, M.F.; Mujtaba, H.; Zofeen, S.; Rana, Z.A. A Comparison of Post-Operative Occlusion with 3-D vs. 2-D Miniplate Fixation in the Management of Isolated Mandibular Angle Fractures. J 2022, 5, 107-113. https://0-doi-org.brum.beds.ac.uk/10.3390/j5010008
Mujtaba A, Malik NR, Umer MF, Mujtaba H, Zofeen S, Rana ZA. A Comparison of Post-Operative Occlusion with 3-D vs. 2-D Miniplate Fixation in the Management of Isolated Mandibular Angle Fractures. J. 2022; 5(1):107-113. https://0-doi-org.brum.beds.ac.uk/10.3390/j5010008
Chicago/Turabian StyleMujtaba, Anosha, Namrah Rafiq Malik, Muhammad Farooq Umer, Hasan Mujtaba, Shumaila Zofeen, and Zahoor Ahmad Rana. 2022. "A Comparison of Post-Operative Occlusion with 3-D vs. 2-D Miniplate Fixation in the Management of Isolated Mandibular Angle Fractures" J 5, no. 1: 107-113. https://0-doi-org.brum.beds.ac.uk/10.3390/j5010008