Concordance of Chronotype Categorisations Based on Dim Light Melatonin Onset, the Morningness-Eveningness Questionnaire, and the Munich Chronotype Questionnaire



Abstract
:1. Introduction
2. Results
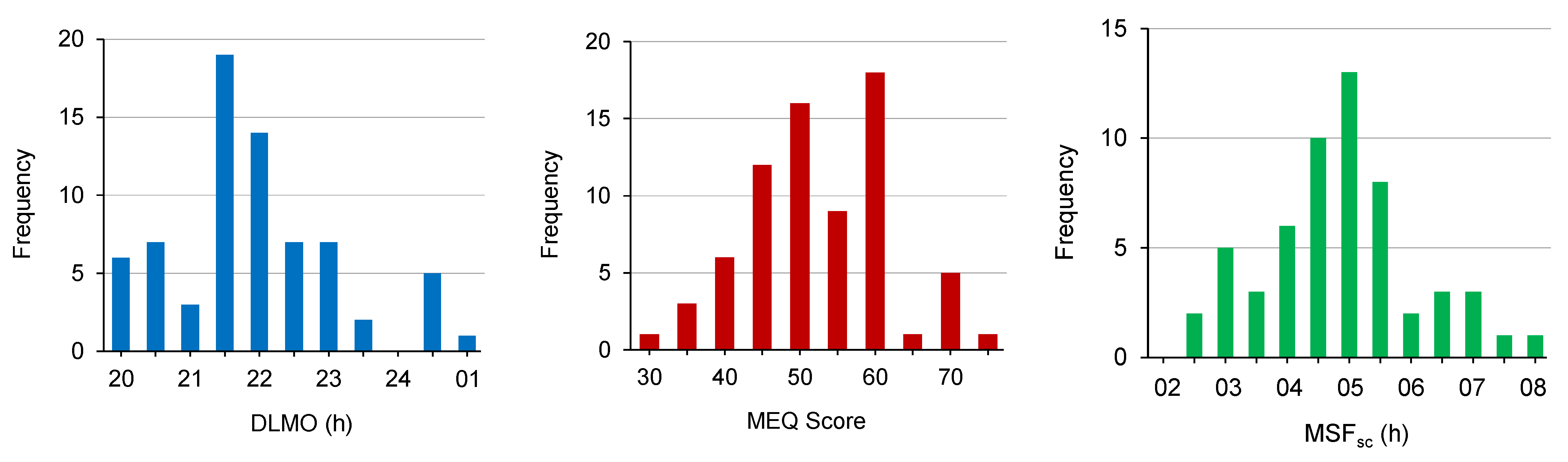
2.1. DLMO, MEQ Score and MSFsc
2.2. DLMO-CT Categories
2.3. MEQ-CT and MSFsc-CT Categories
2.4. Concordance of Categorisations
3. Discussion
4. Materials and Methods
4.1. Participants
4.2. Procedure
4.3. Measures
4.3.1. Dim Light Melatonin Onset (DLMO)
4.3.2. Morningness-Eveningness Questionnaire
4.3.3. Munich Chronotype Questionnaire
4.4. Statistical Analyses
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Levandovski, R.; Sasso, E.; Hidalgo, M.P. Chronotype: A review of the advances, limits and applicability of the main instruments used in the literature to assess human phenotype. Trends Psychiatry Psychother 2013, 35, 3–11. [Google Scholar] [CrossRef] [Green Version]
- Kantermann, T.; Sung, H.; Burgess, H.J. Comparing the Morningness-Eveningness Questionnaire and Munich ChronoType Questionnaire to the Dim Light Melatonin Onset. J. Biol. Rhythms 2015, 30, 449–453. [Google Scholar] [CrossRef] [Green Version]
- Adan, A.; Archer, S.N.; Hidalgo, M.P.; Di Milia, L.; Natale, V.; Randler, C. Circadian typology: A comprehensive review. Chronobiol. Int. 2012, 29, 1153–1175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fabbian, F.; Zucchi, B.; De Giorgi, A.; Tiseo, R.; Boari, B.; Salmi, R.; Cappadona, R.; Gianesini, G.; Bassi, E.; Signani, F.; et al. Chronotype, gender and general health. Chronobiol. Int. 2016, 33, 863–882. [Google Scholar] [CrossRef]
- Juda, M.; Vetter, C.; Roenneberg, T. Chronotype modulates sleep duration, sleep quality, and social jet lag in shift-workers. J. Biol. Rhythms 2013, 28, 141–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burgess, H.J.; Eastman, C.I. The dim light melatonin onset following fixed and free sleep schedules. J. Sleep Res. 2005, 14, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Horne, J.A.; Ostberg, O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int. J. Chronobiol. 1976, 4, 97–110. [Google Scholar] [PubMed]
- Roenneberg, T.; Wirz-Justice, A.; Merrow, M. Life between clocks: Daily temporal patterns of human chronotypes. J. Biol. Rhythms 2003, 18, 80–90. [Google Scholar] [CrossRef] [Green Version]
- Roenneberg, T. Having trouble typing? What on earth is chronotype? J. Biol. Rhythms 2015, 30, 487–491. [Google Scholar] [CrossRef] [Green Version]
- Ritchie, H.K.; Burke, T.M.; Dear, T.B.; McHill, A.W.; Axelsson, J.; Wright, K.P., Jr. Impact of sleep inertia on visual selective attention for rare targets and the influence of chronotype. J. Sleep Res. 2017, 26, 551–558. [Google Scholar] [CrossRef] [Green Version]
- Hida, A.; Kitamura, S.; Ohsawa, Y.; Enomoto, M.; Katayose, Y.; Motomura, Y.; Moriguchi, Y.; Nozaki, K.; Watanabe, M.; Aritake, S.; et al. In vitro circadian period is associated with circadian/sleep preference. Sci. Rep. 2013, 3, 2074. [Google Scholar] [CrossRef] [Green Version]
- Brown, S.A.; Kunz, D.; Dumas, A.; Westermark, P.O.; Vanselow, K.; Tilmann-Wahnschaffe, A.; Herzel, H.; Kramer, A. Molecular insights into human daily behavior. Proc. Natl. Acad. Sci. 2008, 105, 1602–1607. [Google Scholar] [CrossRef] [Green Version]
- Ferrante, A.; Gellerman, D.; Ay, A.; Woods, K.P.; Filipowicz, A.M.; Jain, K.; Bearden, N.; Ingram, K.K. Diurnal preference predicts phase differences in expression of human peripheral circadian clock genes. J. Circadian Rhythms 2015, 13. [Google Scholar] [CrossRef] [Green Version]
- Kitamura, S.; Hida, A.; Aritake, S.; Higuchi, S.; Enomoto, M.; Kato, M.; Vetter, C.; Roenneberg, T.; Mishima, K. Validity of the Japanese version of the Munich ChronoType Questionnaire. Chronobiol. Int. 2014, 31, 845–850. [Google Scholar] [CrossRef] [PubMed]
- Ritonja, J.; Tranmer, J.; Aronson, K.J. The relationship between night work, chronotype, and cardiometabolic risk factors in female hospital employees. Chronobiol. Int. 2019, 36, 616–628. [Google Scholar] [CrossRef]
- Vetter, C.; Fischer, D.; Matera, J.L.; Roenneberg, T. Aligning work and circadian time in shift workers improves sleep and reduces circadian disruption. Curr. Biol. 2015, 25, 907–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caci, H.; Deschaux, O.; Adan, A.; Natale, V. Comparing three morningness scales: Age and gender effects, structure and cut-off criteria. Sleep Med. 2009, 10, 240–245. [Google Scholar] [CrossRef]
- Kervezee, L.; Gonzales-Aste, F.; Boudreau, P.; Boivin, D.B. The relationship between chronotype and sleep behavior during rotating shift work: A field study. Sleep 2021. [Google Scholar] [CrossRef]
- Breithaupt, H.; Hildebrandt, G.; D HRE, D.; Josch, R.; Sieber, U.; Werner, M. Tolerance to shift of sleep, as related to the individual’s circadian phase position. Ergonomics 1978, 21, 767–774. [Google Scholar] [CrossRef] [PubMed]
- Facer-Childs, E.R.; Middleton, B.; Bagshaw, A.P.; Skene, D.J. Human Circadian Phenotyping and Diurnal Performance Testing in the Real World. JoVE 2020, e60448. [Google Scholar] [CrossRef]
- Smith, C.S.; Reilly, C.; Midkiff, K. Evaluation of three circadian rhythm questionnaires with suggestions for an improved measure of morningness. J. Appl. Psychol. 1989, 74, 728. [Google Scholar] [CrossRef]
- Di Milia, L.; Adan, A.; Natale, V.; Randler, C. Reviewing the psychometric properties of contemporary circadian typology measures. Chronobiol. Int. 2013, 30, 1261–1271. [Google Scholar] [CrossRef]
- Sack, R.L.; Auckley, D.; Auger, R.R.; Carskadon, M.A.; Wright, K.P., Jr.; Vitiello, M.V.; Zhdanova, I.V.; American Academy of Sleep, M. Circadian rhythm sleep disorders: Part I, basic principles, shift work and jet lag disorders. An American Academy of Sleep Medicine review. Sleep 2007, 30, 1460–1483. [Google Scholar] [CrossRef] [Green Version]
- Roenneberg, T.; Pilz, L.K.; Zerbini, G.; Winnebeck, E.C. Chronotype and Social Jetlag: A (Self-) Critical Review. Biology 2019, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roenneberg, T.; Allebrandt, K.V.; Merrow, M.; Vetter, C. Social jetlag and obesity. Curr Biol 2012, 22, 939–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, J.M.; Kern, P.A.; Bush, H.M.; McQuerry, K.J.; Black, W.S.; Clasey, J.L.; Pendergast, J.S. Circadian rhythm phase shifts caused by timed exercise vary with chronotype. JCI Insight 2020, 5. [Google Scholar] [CrossRef] [Green Version]
- Ghotbi, N.; Pilz, L.K.; Winnebeck, E.C.; Vetter, C.; Zerbini, G.; Lenssen, D.; Frighetto, G.; Salamanca, M.; Costa, R.; Montagnese, S.; et al. The µMCTQ: An Ultra-Short Version of the Munich ChronoType Questionnaire. J. Biol. Rhythms 2020, 35, 98–110. [Google Scholar] [CrossRef]
- MacCallum, R.C.; Zhang, S.; Preacher, K.J.; Rucker, D.D. On the practice of dichotomization of quantitative variables. Psychol. Methods 2002, 7, 19–40. [Google Scholar] [CrossRef] [PubMed]
- Roenneberg, T.; Kuehnle, T.; Juda, M.; Kantermann, T.; Allebrandt, K.; Gordijn, M.; Merrow, M. Epidemiology of the human circadian clock. Sleep Med. Rev. 2007, 11, 429–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voultsios, A.; Kennaway, D.J.; Dawson, D. Salivary melatonin as a circadian phase marker: Validation and comparison to plasma melatonin. J. Biol. Rhythms 1997, 12, 457–466. [Google Scholar] [CrossRef]
- Burgess, H.J.; Kikyo, F.; Valdespino-Hayden, Z.; Rizvydeen, M.; Kimura, M.; Pollack, M.H.; Hobfoll, S.E.; Rajan, K.B.; Zalta, A.K.; Burns, J.W. Do the Morningness-Eveningness Questionnaire and Munich ChronoType Questionnaire Change After Morning Light Treatment? Sleep Sci. Pract. 2018, 2, 12. [Google Scholar] [CrossRef] [PubMed]
- Roenneberg, T.; Keller, L.K.; Fischer, D.; Matera, J.L.; Vetter, C.; Winnebeck, E.C. Human activity and rest in situ. In Methods Enzymol; Elsevier: Amsterdam, The Netherlands, 2015; Volume 552, pp. 257–283. [Google Scholar]



{kind=link}
{kind=link}
| DLMO-CT Category | n | DLMO (hh:mm) M (SD), Range | MEQ Score M (SD), Range | MSFsc (hh:mm) M (SD), Range |
|---|---|---|---|---|
| Early | 19 | 20:25 (0:46), 19:12–21:13 | 54.8 (11.1), 35–71 | 04:01 (1:15), 02:22–06:42 |
| Intermediate | 19 | 21:33 (0:10), 21:16–21:53 | 49.6 (6.5), 39–60 | 04:46 (0:47), 03:20–06:40 |
| Late | 19 | 23:03 (0:53), 22:04–00:47 | 49.2 (10.1), 27–63 | 05:07 (1:13), 03:22–07:45 |
| Overall | 57 | 21:40 (1:16), 19:12–00:47 | 51.2 (9.7), 27–71 | 04:38 (1:11), 02:22–07:45 |
| (a) MEQ-CT | (b) MSFsc-CT | ||
|---|---|---|---|
| MEQ-CT Category | MEQ Score n, M (SD), Range | MSFsc-CT Category | MSFsc (hh:mm) n, M (SD), Range |
| Early | 22, 60.5 (5.3), 56–71 | Early | 19, 03:23 (0:34), 02:22–04:15 |
| Intermediate | 15, 51.4 (2.9), 47–55 | Intermediate | 19, 04:37 (0:12), 04:17–04:52 |
| Late | 20, 40.8 (5.0), 27–46 | Late | 19, 05:55 (0:48), 04:54–07:45 |
| Overall | 57, 51.2 (9.7), 27–71 | Overall | 57, 04:38 (1:11), 02:22–07:45 |
| Part A | ||||||||
| DLMO-CT Category | MEQ-CT Category | MSFsc-CT Category | ||||||
| Early | Intermediate | Late | Total | Early | Intermediate | Late | Total | |
| Early | 9 | 5 | 5 | 19 | 8 | 4 | 7 | 19 |
| Intermediate | 6 | 5 | 8 | 19 | 10 | 5 | 4 | 19 |
| Late | 7 | 5 | 7 | 19 | 1 | 10 | 8 | 19 |
| Total | 22 | 15 | 20 | 57 | 19 | 19 | 19 | 57 |
| Part B | ||||||||
| Concordance 1 | 9 + 5 + 7 = 21 (37%) | 8 + 5 + 8 = 21 (37%) | ||||||
| 1-step errors 2 | 5 + 6 + 8 + 5 = 24 (42%) | 4 + 10 + 4 + 10 = 28 (49%) | ||||||
| 2-step errors 3 | 5 + 7 = 12 (21%) | 7 + 1 = 8 (14%) | ||||||
| Total | 57 (100%) | 57 (100%) | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reiter, A.M.; Sargent, C.; Roach, G.D. Concordance of Chronotype Categorisations Based on Dim Light Melatonin Onset, the Morningness-Eveningness Questionnaire, and the Munich Chronotype Questionnaire. Clocks & Sleep 2021, 3, 342-350. https://0-doi-org.brum.beds.ac.uk/10.3390/clockssleep3020021
Reiter AM, Sargent C, Roach GD. Concordance of Chronotype Categorisations Based on Dim Light Melatonin Onset, the Morningness-Eveningness Questionnaire, and the Munich Chronotype Questionnaire. Clocks & Sleep. 2021; 3(2):342-350. https://0-doi-org.brum.beds.ac.uk/10.3390/clockssleep3020021
Chicago/Turabian StyleReiter, Andrew M., Charli Sargent, and Gregory D. Roach. 2021. "Concordance of Chronotype Categorisations Based on Dim Light Melatonin Onset, the Morningness-Eveningness Questionnaire, and the Munich Chronotype Questionnaire" Clocks & Sleep 3, no. 2: 342-350. https://0-doi-org.brum.beds.ac.uk/10.3390/clockssleep3020021