Does Irritable Bowel Syndrome Exist? Identifiable and Treatable Causes of Associated Symptoms Suggest It May Not


BCNH College of Nutrition and Health, London NW3 5HT, UK
Gastrointest. Disord. 2019, 1(3), 314-340; https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord1030027
Submission received: 9 April 2019
/
Revised: 10 July 2019
/
Accepted: 11 July 2019
/
Published: 18 July 2019
Abstract
:Significant shortcomings in irritable bowel syndrome (IBS) diagnosis and treatment may arise from IBS being an “umbrella” diagnosis that clusters several underlying identifiable and treatable causes for the same symptom presentation into one classification. This view is compatible with the emerging understanding that the pathophysiology of IBS is heterogeneous with varied disease mechanisms responsible for the central pathological features. Collectively, these converging views of the pathophysiology, assessment and management of IBS render the traditional diagnosis and treatment of IBS less relevant; in fact, they suggest that IBS is not a disease entity per se and posit the question “does IBS exist?” The aim of this narrative review is to explore identifiable and treatable causes of digestive symptoms, including lifestyle, environmental and nutritional factors, as well as underlying functional imbalances, that may be misinterpreted as being IBS.
1. Introduction
Irritable bowel syndrome (IBS) is one of the most widespread functional digestive disorders with a global prevalence of 11% [1]. IBS represents a substantial burden to health status as well as the economy, with people hospitalized more frequently, consuming more medication, and missing more workdays than people without IBS [2]. Symptoms are also frequent and chronic, with a large survey demonstrating that 50% of people with IBS had had symptoms for more than ten years and 57% experienced symptoms daily [3]. Challenges facing better management of IBS include limitations of diagnostic methods and poor therapeutic options.
Current expert recommendations for the diagnosis of IBS encourage confirmation based on subjective clinical symptoms meeting the Rome IV criteria alone, with no objective evidence of the disease and minimal or no additional testing to exclude other pathology [4]. In clinical practice, however, the diagnostic guideline is often not adopted because physicians believe IBS is a diagnosis by exclusion and frequently order diagnostic tests to rule out alternative diagnoses [5]. Subsequent to diagnosis, the Bristol Stool Form Scale is used to differentiate IBS into various subtypes based on predominant symptoms—IBS with constipation, IBS with diarrhea, or IBS with mixed symptoms of constipation and diarrhea—which are used to direct treatment options [6]. No accepted biomarkers for IBS exist and novel tests have been found to perform only as good as symptom-based criteria, which is moderately well [7].
Treatment is typically based on the prevailing symptoms with antispasmodics and antidepressants used for pain, loperamide and the 5-HT(3) receptor antagonist alosetron for reducing bowel frequency, and soluble fiber for constipation predominant or mixed IBS [8]. Despite their widespread use, these treatments lack strong evidence of efficacy with less than 25% of patients reporting complete relief of any one symptom [9]. Furthermore, they have significant side-effects with many people seeking medical help or missing work, school, or social activities because of adverse events [10]. Probiotics have shown good evidence of efficacy and low incidence of side-effects, however, the number needed to treat (NNT) is 7 [11]. Similarly, psychological therapies including stress reduction and relaxation are beneficial and safe, yet the NNT is 4 [12]. Regardless of therapy, the response rate is typically low and does not completely resolve global symptoms [13].
Significant shortcomings in IBS diagnosis and treatment may arise from IBS being an “umbrella” diagnosis that clusters several underlying identifiable and treatable causes for the same symptom presentation into one classification [14]. This view is compatible with the emerging understanding that the pathophysiology of IBS is heterogeneous with varied disease mechanisms responsible for the central pathological features, namely alterations in gastrointestinal motility and visceral sensory function, responsible for the generation of clinical symptoms [15]. Obtaining a better understanding of each patient’s pathophysiology with clinical and molecular assessments could therefore help improve diagnosis and target different therapies to individuals most likely to benefit [16]. In a clinical setting, this heterogeneous view of IBS could be approached from the framework of functional medicine, which personalizes patient care by focusing investigative and treatment approaches on the unique state of physiological function of an individual rather than traditional histopathological or clinical definitions of disease [17].
Evidence that identification of underlying reasons for IBS-symptoms can improve patient care is provided by a clinical retrospective study that found 98% of 303 patients with diarrhea-predominant IBS (IBS-D) and functional diarrhea had an alternative explanation for their symptoms, including bile acid induced diarrhea, carbohydrate intolerance, gluten enteropathy and non-celiac gluten intolerance, and responded very well to treatments that corresponded with their new diagnosis [14]. Notably, this particular study supported the hypothesis that “IBS-D and functional diarrhea are not true clinical entities as previously thought, but a collection of different, separate medical conditions.” Similarly, another research group conducted a retrospective analysis of a biomarker test that identifies potentially treatable underlying causes of IBS in people that meet Rome III criteria and found that up to 94% have results suggesting a treatable underlying diagnosis or functional problem [18,19]. The same group also demonstrated that such testing significantly reduced medical and gastrointestinal procedural costs by improving patient care [20].
Collectively, these new and converging views of the pathophysiology, assessment and management of IBS render the traditional diagnosis and treatment of IBS less relevant; in fact, they suggest that IBS is not a disease entity per se and posit the question “does IBS exist?” Indeed, it has been proposed that cataloguing unexplained functional gastrointestinal symptoms as a distinct disease “generates lazy thinking and impedes progress” [21]. The aim of this narrative review is to explore identifiable and treatable causes of digestive symptoms, including lifestyle, environmental and nutritional factors, as well as underlying functional imbalances, that may be misinterpreted as being the syndrome of IBS (see Figure 1). Well established differential diagnosis, notably celiac disease, inflammatory bowel disease, microscopic colitis and chronic giardiasis, have been excluded from this review.
2. Lifestyle and Environmental Factors
2.1. Stress
Anxiety and depression are frequent clinical features in people presenting with IBS and may originate from the gastrointestinal disturbance in as many as two-thirds of cases [22,23]. Regardless of whether psychiatric illness precedes or follows the development of functional gastrointestinal illness, there is clearly an important contribution to gastrointestinal symptoms. For example, chronic life stress is a strong predictor of symptom intensity in people diagnosed with IBS and the absence of stress can result in symptomatic improvement over time [24]. Furthermore, low stress resilience has been found to predict IBS symptom severity [25].
Because dysregulation of the brain–gut axis can influence the main pathophysiological features of IBS, including visceral hypersensitivity, colonic motility and alterations in the gut microbiota, it could be central to the development of symptoms in some individuals [26]. Thus, psychiatric illness and chronic stress could be viewed not simply as a comorbid in patients with IBS, but important contributory factors and potential treatment targets [27].
Functional assessments of the stress response and hypothalamic–pituitary–adrenal (HPA) axis activity have been explored in patients with IBS, with some evidence to suggest elevated salivary cortisol levels at awakening [28], and serum neuropeptide Y (NPY) may be useful [29]. A greater frequency of serotonin transporter (SERT) gene variants has been found in IBS patients with a history of either depression or anxiety, and may play a functional role in digestive symptom pathogenesis [30,31]. Furthermore, the presence of at least one allele of the catechol-O-methyltransferase (COMT) Val158Met polymorphism may predict baseline symptom severity and subsequent response to stress-reduction [32,33].
Mind–body therapies such as cognitive behavioral therapy are typically utilized as indiscriminate first-line therapies for IBS, yet are still relatively effective compared to other treatments and directly improve IBS symptoms independent of effects on psychological distress [34]. They may also alter the underlying pathophysiology, with a hypnotherapy and educational intervention found to reduce visceral hypersensitivity [35]. Mind–body therapies could be targeted to patients with clinical or laboratory indicators of a dysregulated stress response, and there is potential for gene variants in SERT and COMT to direct treatment.
2.2. Circadian Disruption
Circadian rhythm disruption can affect several aspects of gastrointestinal function including gastrointestinal motility, visceral sensitivity, immunological function, and barrier integrity [36]. In a subgroup of people presenting with IBS, circadian rhythm disruption could contribute significantly to symptoms. Subjective and objective measures of sleep disruption have been reported to be associated with gastrointestinal symptoms [37,38,39]. Furthermore, circadian disruption due to shift work is associated with IBS severity independent of sleep quality [40].
Urinary 6-hydroxymelatonin, a clinical biomarker of circadian disruption, has been found to be altered in patients with IBS compared to controls and proposed to be a useful biomarker for personalized treatment with melatonin [41,42]. Melatonin therapy has been shown to result in clinical improvement when administered to people presenting with IBS and sleep disorders, independent of its effects on mood and sleep [43]. Clinical trials of melatonin in people with IBS suggest it may improve colonic transit time, reduce abdominal pain, and improve global IBS symptoms [44]. Other methods for restoring circadian disruption and melatonin production have been proposed, but not yet investigated in IBS, such as extending the dark period at night to 9 or 10 h [45].
2.3. Physical Inactivity
Physical inactivity or sedentary behaviour is known to contribute to a wide range of chronic diseases but its contribution to gastrointestinal illness is not as greatly appreciated or understood [46]. A small number of studies suggest that lack of adequate physical activity may play an important role in the development of IBS symptoms and represent an opportunity for therapeutic intervention. Clinical studies have found that increasing physical activity can improve gastric emptying, intestinal gas transit and reduce abdominal distension [47,48,49]. Furthermore, in patients with IBS exercise counselling and subsequent increase in physical activity, was found to significantly reduce gastrointestinal symptoms within 12-weeks and reduce psychological symptoms in the longer term [50]. Similarly, both yoga and walking reduced gastrointestinal and psychological symptoms in people with IBS [51]. Assessment of daily physical activity and the use of exercise as medicine deserves consideration in the management functional gastrointestinal disorders.
3. Nutritional Factors
3.1. Carbohydrate Restriction
Recently, the symptomatic management of IBS with diet has focused on restriction of Fermentable Oligosaccharide, Disaccharide, Monosaccharide, and Polyols in the diet (low FODMAP diet), which works by reducing osmotic load and gas production in the distal small bowel and the proximal colon [52]. Compared to a standard western diet, a low FODMAP diet leads to a significant improvement in symptom severity, suggesting that a subgroup of patients with IBS may benefit from eating less highly fermentable carbohydrates [53]. The low FODMAP diet is typically viewed as being a short-term, second-line dietary treatment option with traditional dietary measures—such as following a regular eating pattern and limiting the intake of potential dietary triggers, such as alcohol, caffeine, spicy foods, and fat—still the first line of dietary therapy [54]. In fact, traditional dietary measures may be just as effective as a low FODMAP diet [55].
The concept of dietary carbohydrate restriction for functional gastrointestinal disorders is not entirely novel. Before the FODMAP approach gained its current popularity, it had been found that restriction of simple sugars and refined carbohydrates could result in important relief of functional digestive symptoms in some people [56,57,58]. Furthermore, the specific carbohydrate diet has also been reported to be of benefit [59]. It is interesting to speculate that higher intake of refined sugar and carbohydrates could contribute to the development of IBS in some individuals. Because refined sugars can be rapidly metabolized by microbiota in the small intestine, they could play a contributory role to the development of changes in the gut microbiome that are implicated in the pathophysiology of IBS [60,61].
Identifying potential responders to carbohydrate restriction remains a challenge. Apart from testing for lactose intolerance, the FODMAP diet is based on clinical response to food elimination and re-introduction [62]. Breath testing may be useful for identifying fructose intolerance [63]. Intolerance to FODMAPs may be secondary to small intestinal bacterial overgrowth (SIBO), as determined by a positive hydrogen breath test, suggesting that a low FODMAP diet may be particularly useful for symptomatic relief in this patient group, although this is yet to be clarified [64,65]. Novel potential biomarkers that could help in the personalisation of carbohydrate restriction include sucrase-isomaltase gene variants [66].
3.2. Lactose Intolerance
Lactose intolerance, defined as gastrointestinal symptoms in an individual with lactose malabsorption, may contribute to IBS-like symptoms but could be overlooked due to challenges related to diagnosis. A higher prevalence of lactose intolerance, but not lactose malabsorption, has generally been reported in patients fulfilling criteria of IBS [67,68,69]. This observation was confirmed by a meta-analysis of 14 clinical trials in which lactose intolerance, but not lactose malabsorption, was found to be significantly more frequent in patients with IBS when compared to controls [70].
Identification of lactose intolerance in a clinical setting requires a positive test of lactose malabsorption such as genetic, biopsy, or H2-breath tests and subsequent demonstration of an association between lactose intake and symptoms after an open-label challenge [71]. Detection of lactose malabsorption alone is not sufficient to direct dietary treatment [72]. Confirmation of lactose intolerance, however, is clinically challenging as an open-label lactose challenge may have limited accuracy in individuals with self-reported lactose intolerance [73].
Indiscriminate use of lactase enzyme therapy or a lactose-free diet in patients with IBS has not resulted in positive clinical outcomes when compared to placebo or control groups [74,75]. In contrast, clinical trials of a lactose-free diet that were initiated after identification of lactose malabsorption resulted in significant clinical improvement in some, but not all, studies [76,77,78]. It is possible that lactose intolerance is related to a unique pathophysiological subtype, with one study suggesting that mucosal immune activation and increased visceral sensitivity were features of lactose intolerance in IBS patients [79]. Additionally, it has been proposed that lactose intolerance is a component of a wider spectrum of intolerance to poorly absorbed carbohydrates [80].
3.3. Food Hypersensitivity
Immunologically-mediated food hypersensitivity may play a role in the development of IBS symptoms through mechanisms distinct from classic type-1 immunoglobulin E (IgE)—mediated food allergy, including a local and limited IgE-mediated reaction in the intestinal mucosa and/or IgE—independent mechanisms [81]. Studies of dietary therapy based on the elimination of suspected food sensitives indicate that food hypersensitivity plays a role in a subgroup with IBS [82].
Elimination and re-challenge diets have been studied in patients with IBS, although evidence is mixed with some studies reporting benefit, others reporting benefit limited to subgroups of patients such as diarrhoea predominant IBS, while others have found no benefit [83,84,85,86]. In a meta-analysis of elimination and re-challenge diets, the positive clinical response ranged from 15% to 71%, however, due to limitations in study design more research is needed to clarify the role of elimination and re-challenge diets [87]. A more recent systematic review found moderate evidence for targeted elimination diets (removal of suspected symptom-provoking foods), and low evidence for generalized elimination and re-challenge diets [88].
IgG-mediated immune reactions have been proposed to play a role in the development of IBS symptoms and at least six clinical studies have found that IgG antibody-guided exclusion diets can result in modest clinical improvements in symptoms [89,90,91,92,93,94]. In contrast, one study found no benefit, although diagnostic methods varied and the diet duration was relatively short [95]. Elevated serum IgG antibodies to foods commonly associated with atopic conditions have been observed in IBS [96], although studies attempting to correlate antibodies with symptom severity [97,98], or contrast them to controls have found no association [99]. Despite controversy around the use of IgG antibody-guided exclusion diets, they appear to be a clinically useful way to identify a potential cause of symptoms and personalize dietary therapy [100].
3.4. Non-Celiac Gluten Sensitivity
Non-celiac gluten sensitivity (NCGS) is characterized by intestinal and extra-intestinal symptoms related to the ingestion of gluten-containing food in people without celiac disease or wheat allergy, and classically mimics symptoms of IBS [101]. It is unclear if it is gluten that contributes to gastrointestinal symptoms in NCGS or if symptoms are generated by other components of wheat [102]. Regardless of the underlying mechanism, a subgroup of IBS patients exhibit NCGS and experience intestinal and extra-intestinal symptoms after wheat ingestion [103,104].
A controlled trial of a gluten-containing vs. gluten-free diet in patients with diarrhea-predominant IBS without celiac disease found that exposure to gluten increases bowel movement frequency and small bowel permeability, and that this impact is greater in HLA-DQ2/8-positive genotypes [105]. Furthermore, a prospective study of a gluten-free diet in diarrhea-predominant IBS patients without celiac disease found that 71% responded well to the intervention, with greater benefit in HLA-DQ2/8-positive subjects [106]. Further supporting a role of NCGS in IBS, gluten re-challenge after a gluten-free diet was found to significantly worsen symptoms within 1 week [107].
Evidence that gluten can cause functional gastrointestinal symptoms that mimic IBS has led to the proposal that a diagnosis of IBS may delay the identification of NCGS and effective dietary therapy [108]. Clinically, NCGS currently lacks a direct biomarker and diagnosis is based on a clinical rating scale, response to a gluten-free diet, and double-placebo controlled gluten challenge [109].
3.5. Nickel-Related Intestinal Mucositis
Sensitivity to dietary nickel has been recently proposed as a cause of IBS symptoms. In a clinical study, IBS patients with a positive nickel patch test were found to respond well to a low nickel diet with significant reductions in gastrointestinal symptoms [110]. It was hypothesized by the study investigators that dietary nickel may contribute to IBS symptoms by inducing a pro-inflammatory state. In support of this theory, a low nickel diet was found to reduce inflammatory cytokines in people with gastrointestinal and cutaneous symptoms of nickel sensitivity [111].
Diagnosis of dietary nickel sensitivity can be performed with a skin or oral mucosa patch test [110,112]. All patients reporting to a gastroenterology unit with IBS symptoms and suspected sensitivity to nickel containing foods had a positive response to an oral mucosa patch test characterized by local hyperemia and/or edema, compared to no response in a control group [113]. Beyond implementation of a low nickel diet, nutritional detoxification strategies have been proposed but currently lack clinical evidence [114].
3.6. Vitamin D Deficiency
Adults and children with IBS have a high prevalence of vitamin D deficiency when compared to IBS-free controls [115,116]. Vitamin D deficiency could play a contributory role in the development of IBS due to its impact on various aspects of gastrointestinal function including mucosal inflammation [117], epithelial cell integrity [118], and the composition of the gut microbiome [119]. A case report provided initial evidence that treating vitamin D deficiency could improve gastrointestinal symptoms in IBS [120]. Subsequently, a randomized double-blind clinical trial found a significantly greater improvement in IBS symptoms in those receiving vitamin D when compared to placebo [121]. Routinely testing for and treating vitamin D deficiency would be a logical course of action in people presenting with IBS.
4. Functional Imbalances
4.1. Exocrine Pancreatic Insufficiency
A subgroup of patients presenting with IBS have exocrine pancreatic insufficiency and respond well to treatment with digestive enzyme therapy. In a group of patients meeting criteria for diarrhea-predominant IBS exocrine pancreatic insufficiency, defined as fecal elastase-1 (FE-1) less than 100 µg/g, was present in 6.1% of patients, and subsequent pancreatic enzyme supplementation resulted in significant improvement in symptoms [122]. In this study, diarrhea-predominant IBS patients without exocrine pancreatic insufficiency were used as a control group and, in contrast, were found not to benefit from enzyme supplementation. A similar prevalence of exocrine pancreatic insufficiency of 4.1% (FE-1 <100 µg/g) was found in another study across IBS subtypes [19]. A good response to enzyme supplementation in diarrhea-predominant, and galacto-oligosaccharide intolerant IBS has been reported by other investigators [123,124].
4.2. Low-Grade Inflammation
Inflammatory biomarkers, especially C-reactive protein (CRP) and calprotectin, can be used to exclude the presence of inflammatory bowel disease (IBD) in patients presenting with symptoms consistent with IBS [125]. However, a subgroup of patients with IBS may have intestinal inflammation in the absence of IBD [126]. Low-grade intestinal inflammation is thought to play a key role in the pathophysiology of IBS, contributing to altered permeability, hypersensitivity of enteric nerves and changes in serotonin signaling [127].
Calprotectin has been proposed as a biomarker of intestinal inflammation in patients with IBS with a level higher than 50 µg/g, the absence of anti-neutrophil cytoplasmic antibodies (ANCA) and anti-Saccharomyces cerevisiae antibodies (ASCA), antibodies and a normal small bowel examination indicating an inflammatory IBS subtype [128].
Anti-inflammatory therapies have recently been explored in IBS, but not yet targeted to inflammatory subtypes. Clinical trials of the drug mesalazine have generally produced disappointing results, however, a subgroup of patients did appear to respond well [129,130]. In contrast, a histamine receptor H1 antagonist and extract of the anti-inflammatory herb Boswellia serrata have preliminary evidence of substantial clinical benefit [131,132]. Because food antigens are known to trigger intestinal inflammation in IBS, there is potential for the development of novel anti-inflammatory dietary interventions for patients with elevated inflammatory biomarkers, such as calprotectin. Although this concept has not yet been explored, the identification and dietary elimination of food antigens using confocal laser endomicroscopy to visualize real-time food-associated changes in the intestinal mucosa was associated with good clinical responses in patients with IBS [133].
4.3. Intestinal Permeability
Studies have suggested that a subgroup of patients with IBS have increased intestinal permeability, especially those with diarrhea-predominant symptoms [134,135,136]. In patients with IBS and intestinal permeability, determined by an elevated urinary lactulose/mannitol ratio, it was found that the severity of barrier dysfunction correlated with symptom severity [137]. Intestinal permeability is thought to play a central role in the development of IBS due to its contribution to low-grade intestinal inflammation and increased visceral and pain sensitivity [138].
The integrity of intestinal epithelial barrier has been proposed as a therapeutic target in IBS, although evidence for effective therapeutic interventions is currently lacking [139]. Further, the etiological factors involved in the development or intestinal permeability—such as viral, bacterial, dietary and environmental toxins—may theoretically influence the effectiveness of treatments [140]. Interestingly, there is experimental and clinical evidence to suggest that some probiotics may upregulate tight-junction proteins, improve the integrity of the gut epithelium, and reduce intestinal permeability [141,142]. The impact of probiotics on intestinal permeability in patients with IBS has not been well studied, but one clinical trial did find that a probiotic fermented milk drink decreased small bowel permeability and improved clinical symptoms in patients with diarrhea-predominant IBS [143].
Of clinical relevance, it was recently demonstrated that synthesis of the amino acid glutamine, a primary metabolic fuel for epithelial cells, could be impaired in diarrhea-predominant IBS, leading to reduction in tight-junction proteins and increased gut permeability [144]. Supplementation with glutamine in patients with diarrhea-predominant IBS was subsequently found to significantly reduce intestinal permeability and improved global IBS symptoms, especially diarrhea and abdominal pain [145].
4.4. Bile Acid Diarrhea
Bile acid diarrhea (BAD) is characterized by an increase in fecal excretion and change in the proportion of various bile acids in stool, which contributes to intestinal permeability, water and electrolyte secretion, and increased colonic transit [146]. From 16.9% to 35.3% of patients with IBS-D have BAD [147]. Furthermore, bile acid malabsorption, even in the absence of overt BAD, appears to contribute to diarrhea-predominant IBS [148]. BAD is typically confirmed with a therapeutic trial of bile acid binders, serum levels of 7α-hydroxy-4-cholesten-3-one (C4) or selenium homotaurocholic acid test (SeHCAT), and diagnostic confirmation can direct treatment with bile acid binders [149]. Genes controlling bile acid metabolism (KLB rs17618244) receptor expression (GPBAR1rs11554825) are associated with colonic transit and total fecal bile acid excretion in patients with IBS and may be novel functional biomarkers [150].
Pancreatic enzyme supplementation may reduce bile acid malabsorption and improve fat malabsorption, and has been used to treat IBS-D with marked post-prandial symptoms with striking success in some cases, although the role of this therapy in clearly defined BAD is not yet established [151]. Diet is a well-established modifier of colonic bile acid concentrations, but the potential for nutritional therapy to influence bile acid malabsorption or BAD has not yet been explored [152]. Similarly, gut microbiota influence colonic bile acid concentrations and metabolism, yet gut microbiota-targeted therapies, such as probiotics and prebiotics, have not yet been studied in the clinical management of BAD [153]. More research on the therapeutic role of diet, pancreatic enzyme supplementation, probiotics and prebiotics in BAD is needed.
4.5. Chronic Constipation
Although classically differentiated from IBS, chronic constipation may mimic IBS symptoms including intermittent diarrhoea. Functional constipation and IBS have overlapping clinical symptoms and share common pathophysiological mechanisms, including visceral sensitivity and alterations in serotonin signaling [154]. Fecal retention or chronic “hidden” constipation characterized by normal transit time with significantly increased fecal load in the colon has been proposed to be a cause of IBS symptoms in a subgroup of patients [155]. In a study of 252 patients with functional digestive symptoms, in particular pain, bloating and constipation with or without diarrhea, 90 were identified as having fecal loading and subsequently responded well to prokinetic treatment, diet therapy, and exercise [156]. Similarly, a clinical research group proposed that some IBS patients more correctly have “overload and overflow syndrome,” which they defined as a predominant problem of constipation with bouts of diarrhea occurring when fecal loading of the bowel reached a critical level [157]. Subgrouping IBS patients into this underlying classification using the Bristol Stool Scale and clinical symptoms was found to be a useful way to target laxative and fiber therapy and improve treatment [157].
4.6. Dysbiosis
Alterations in the gastrointestinal microbiota are central to the development of IBS and play a fundamental role in pathophysiology by activation of mucosal innate immune responses which increase epithelial permeability, initiate nociceptive sensory pathways and dysregulate the enteric nervous system [158]. The microbiota has emerged as a therapeutic target in IBS but there is no characteristic compositional microbial alteration across patients with IBS and there is currently no well-established way to personalize gut microbiota-targeted therapies [159].
Subgrouping patients with IBS by symptoms has found some correlations with distinct microbial subtypes [160,161]. However, the association between microbial changes in IBS and its pathophysiology are not fully understood and proposing diagnostic or prognostic roles to microbiota is controversial [162]. It is interesting to speculate, however, that selectively targeting low Bifidobacteria species with prebiotics could benefit patients presenting with this microbial signature [163]. Bifidobacteria tend to be lower in patients with IBS compared to healthy controls [160,163], and declines in this species have been found to correlate with digestive symptoms, especially abdominal pain [164,165,166]. Clinical studies of prebiotic galactooligosaccharides [167], short-chain fructo-oligosaccharides [168,169], and partially hydrolyzed guar gum [170,171,172,173] in patients with IBS have suggested they may increase Bifidobacteria and reduce clinical symptoms.
Probiotics have been proposed as an approach for improving gut microbial composition, however a meta-analysis found no effect of probiotics on measures of composition such as α-diversity, richness, or evenness [174]. It has been suggested that the health effects of probiotics may be due to their ability to influence the metabolic function of the gut microbiota or stabilize, rather than alter, its composition [175]. Gaps in our understanding of probiotic effects are reflected in the imprecision of their clinical use, with best practice guidelines recommending that probiotic strains and dose are based on evidence of symptomatic benefit from randomized controlled trials, with a therapeutic trial for 4 weeks, and then subsequently stopping therapy and trialing another probiotic if there is a lack of clinical response [176]. Challenges facing the evolution of probiotics as a more precise therapy for IBS include the delineation of clear IBS subtypes and corresponding probiotic treatments supported by mechanism of action studies in humans and high-quality clinical trials [177]. Gene expression profiling of the peripheral blood leucocytes has recently emerged as a novel way to predict clinical probiotic response, but this technique is in its infancy [178].
Diet has a rapid and strong influence on the composition and metabolic function of the human gastrointestinal microbiota, as evidenced by associations with various dietary patterns and findings from intervention studies [179]. The low FODMAP diet has been shown to impact the gastrointestinal microbiota and related metabolome in patients with IBS. Paradoxically, the low FODMAP diet exacerbates alterations in gastrointestinal microbiota that are associated with IBS symptoms, including reduced Bifidobacteria counts [180]. However, a reduction in bacterial abundance, especially microbiota with saccharolytic potential and thus fermentation of carbohydrates, has been proposed as a central mechanism for the low FODMAP diet’s clinical effects [181]. Interestingly, the low FODMAP diet was recently shown to reduce relative abundance of bacteria involved in gas consumption, as well as an eight-fold reduction in histamine, a novel finding that may also help explain the benefits of this dietary approach [182]. Beyond the low FODMAP diet, there is a notable lack of studies of gut microbiota-targeted dietary interventions in IBS, despite their theoretical potential [183].
4.7. Small Intestinal Bacterial Overgrowth
Small intestinal bacterial overgrowth (SIBO) is defined as an abnormally high number and/or type of bacteria in the small bowel. This overgrowth is typically colonic Gram-negative aerobes and anaerobic species that ferment carbohydrate and play a role in the development of symptoms characteristic of SIBO including bloating, flatulence, abdominal discomfort and changes in stool form [184]. Perhaps not surprisingly, SIBO can mimic symptoms of IBS and case-control studies have generally found a higher prevalence of SIBO among patients with IBS (19% to 37%) compared to healthy controls (0% to 12%) [185]. This association has been suggested to be important clinically as empirical evidence suggests that treating SIBO may relieve symptoms consistent with IBS in some patients [186]. However, the link between SIBO and IBS is controversial for several reasons, including important limitations in the reliability and accuracy of clinical diagnostic methods (breath testing), a lack of robust data demonstrating that eradication of SIBO is clinically effective in the long term, and evidence that the efficacy of antibiotic therapy is independent of the presence of SIBO and may be due to non-antibiotic mechanisms [187]. The clinical management of SIBO in patients with IBS is therefore largely empirical and not currently well supported by evidence.
Empirical management of SIBO is typically based on antibiotic therapy, of which a variety have been used, and result in an overall rate of breath test normalization in 50% of subjects, compared with 10% for placebo [188]. Alternatives and/or adjuvants to antibiotics include dietary therapy, probiotics and herbal therapy.
There are associations between SIBO prevalence and higher intake of carbohydrates and refined sugar and lower intake of dietary fiber, especially insoluble fiber [60,61]. Because refined sugars can be rapidly metabolized by microbiota in the small intestine they could play a contributory role to the development of SIBO. Importantly, carbohydrate intolerance (lactose, fructose and sorbitol) is common among patients with SIBO and may improve after eradication of bacterial overgrowth [64,189]. A low-fermentable carbohydrate diet such as the low FODMAP diet, or restriction of refined carbohydrates, sugars and gas-producing foods could be clinically useful [190].
A medical food-based elemental diet has been used for SIBO, but this approach is limited by poor adherence and long-term safety [191]. In a retrospective study, treatment of people with IBS and SIBO with an elemental diet (Vivonex, Nestlé Health Science) for 2 weeks normalized breath tests in 80% of people, and in non-responders a further 1 week of treatment resulted in a total response rate of 85%. At 1-month follow-up, those who normalized their breath test showed a 66% improvement in symptoms, compared to 11.9% in non-responders [192].Although elemental diets limit the availability of fermentable substrate to microbiota, they may have other effects that explain their benefits such as reducing dietary antigen exposure and improving immunological tolerance [193].
Herbal medicines have been used as alternatives to antibiotic therapy for SIBO and appear to be better tolerated and safer. Although herbs do have antimicrobial effects, they have several other mechanisms of action that may explain any observed improvement in clinical symptoms such as anti-spasmodic, pro-kinetic, immunomodulatory, anti-inflammatory, and antidiarrheal properties. Enteric-coated peppermint oil (0.2 mL three times daily) was shown in a case-report to normalize hydrogen breath test results and reduce IBS-like symptoms after 20 days treatment [194]. In a retrospective study, people with SIBO treated with herbal therapy (one of several different products) were more likely to have successful treatment response, as confirmed with a negative breath-test when compared to treatment with rifaximin (46% for herbal therapy vs. 34% for rifaximin) [195]. Additionally, people who did not respond to rifimaxin were offered either a stronger course of antibiotics or herbal therapy, which were equally effective at eradicating SIBO (both about a 60% successful treatment). Side-effects were fewer and less severe in those receiving herbal therapy. In addition, a novel herbal complex containing quebrach, horse chestnut and peppermint leaf (Atrantil™, USA) developed for the management of SIBO characterized by high methane production and IBS-C was found to improve constipation, bloating and abdominal pain [196,197]. However, these studies did not measure the impact of treatment on bacterial overgrowth or methane production; only clinical symptoms were reported [196,197].
A review and meta-analysis including 22 studies of probiotic therapy for SIBO found that they were effective overall for reducing SIBO, decreasing breath hydrogen concentration, and relieving abdominal pain [198]. Adjuvant probiotic therapy may also improve antibiotic treatment, with one study showing that the addition of a probiotic resulted in better resolution of SIBO compared to antibiotic therapy alone (a negative hydrogen breath test in 93.3% with probiotics vs. 66.7% without) as well as superior symptomatic improvement [199].
4.8. Parasitic Infection
Parasitic infection is a differential diagnosis for IBS, however, there is evidence to suggest that Blastocystis species infection may be overlooked as a cause of IBS symptoms in some individuals. [200]. A higher prevalence of Blastocystis has been observed in people with IBS compared to controls in some [201,202,203], but not all studies [204], and Blastocystis species is frequently present in asymptomatic individuals. A potential reason for why Blastocystis might contribute to symptoms in some people but not others is that there are nine subtypes of the parasite that infect humans, some of which may be pathogenic in certain individuals [205]. Specific subtypes of Blastocystis may have effects that play a causative role in IBS, such as contribution to gastrointestinal dysbiosis, upregulation of pro-inflammatory cytokines, and degradation of tight junction proteins and increased intestinal permeability [206].In support of differential associations with pathogenic Blastocystis subtypes, a recent meta-analysis found associations between two particular subtypes and risk for IBS symptoms [207].
Treatment of Blastocystis infection is controversial, with a lack of clinical trials demonstrating a resolution of symptoms after eradication in Blastocystis-infected IBS patients. Furthermore, there is speculation that Blastocystis is not a cause of IBS but an indicator of intestinal dysfunction or dysbiosis [208]. Conventional treatment of Blastocystis infection is typically antibiotic monotherapy with the success in eradicating the parasite ranging from anywhere between 0% and 100% in various studies, and there are no trials in patients with IBS [209]. One group reported 60% eradication and an improvement in IBS symptoms with a unique antibiotic therapy regime in a pilot study [210]. Furthermore, there is some clinical evidence that herbal therapy with emulsified oil of Oregano (Origanum vulgare) [211], and the probiotic Saccharomyces boulardii [212] may eradicate Blastocystis infection but they have not yet been investigated in Blastocystis-infected patients with IBS.
It is probable that several other parasites, as well as bacteria and viruses, could contribute to symptoms of IBS but clear evidence of causal roles is often lacking for candidate pathogens and requires more research [213].Similar to Blastocystis, there is some evidence, albeit conflicting, to suggest Dientamoeba fragilis may be an overlooked and treatable cause of IBS-like symptoms. Although a statistically significant association has not been reported between D. fragilis and IBS [204] there are prospective studies and case reports of D. fragilis eradication resulting in clinical improvement in patients previously diagnosed with IBS and presenting with typical symptoms of diarrhea, constipation, abdominal pain, bloating, and flatulence [214,215,216].In contrast, one study found no association between eradication of D. fragilis and clinical response in IBS patients [217]. The data implicating D. fragilis in IBS is thus limited to a small number of conflicting studies and requires clarification [218].
5. Discussion
The available evidence suggests that the symptoms of IBS are frequently due to identifiable and treatable underlying causes including lifestyle, environmental and nutritional factors, as well as underlying functional imbalances, that may be misinterpreted as being the syndrome of IBS. IBS, therefore, could be considered a set of symptoms that require further investigation and not a disease per se. This view is consistent with the heterogeneous pathophysiology of IBS in that different causative factors would influence different physiological mechanisms, although the resultant symptoms may still be consistent with classification as IBS. Compatible with this view is the notion that an individual’s genetics, including the genetics of their microbiome, may interact with lifestyle, environmental and nutritional factors in unique ways that give rise to the symptoms of IBS.
Creating a distinction between the symptom-based diagnosis of IBS and the underlying causes that give rise to those symptoms may aid progress in disentangling the clinical overlap between IBS and other functional gastrointestinal disorders such as gastroesophageal reflux disease (GERD) and functional dyspepsia (FD). Overlap between these conditions is very common, yet pathophysiological reasons for their co-occurrence in the same patient are not well understood [219]. A better understanding of the pathophysiological origin of functional gastrointestinal symptoms related to IBS, GERD and FD may help improve treatment options [220]. In support of this hypothesis, there is empirical evidence to suggest that identification and treatment of a shared pathophysiological origin, H. pylori infection, may resolve overlapping symptoms of IBS, GERD, FD and/or erosive esophagitis in some cases [221]. It seems reasonable to suggest that personalized treatment of underlying pathophysiological causes of functional gastrointestinal symptoms could improve outcomes across a wide range of symptom-based diagnosis, not only IBS.
In a clinical setting, the identification of the underlying causes of symptoms in a person with IBS would help personalize treatment and target therapies to those most likely to respond (Table 1), although it should be emphasized that many of the clinical and biochemical investigations and management approaches discussed require clarification before translation to clinical practice. Also, of relevance to clinical trials, patient subgroups based on clinical and biochemical assessments could help direct personalised therapies or identify treatment responders. Importantly, multiple factors may be involved in the development of IBS symptoms and these will vary from person to person, thus a comprehensive, systems-based approach to management that leverages guidance from individual clinical presentations and laboratory biomarkers may represent the best path forward [222].
Funding
The author received no grants or other financial support for this review.
Acknowledgments
The author thanks Deanna Minich for valuable comments on the draft manuscript and the anonymous peer-reviewers for their important and helpful critique.
Conflicts of Interest
The author has received consultancy fees from Pure Encapsulations (Sudbury, MA, USA).
References
- Lovell, R.M.; Ford, A.C. Global prevalence of and risk factors for irritable bowel syndrome: A meta-analysis. Clin. Gastroenterol. Hepatol. 2012, 10, 712–721. [Google Scholar] [CrossRef]
- Spiegel, B.M. The burden of IBS: Looking at metrics. Curr. Gastroenterol. Rep. 2009, 11, 265–269. [Google Scholar] [CrossRef]
- Silk, D.B. Impact of irritable bowel syndrome on personal relationships and working practices. Eur. J. Gastroenterol. Hepatol. 2001, 13, 1327–1332. [Google Scholar] [CrossRef]
- Ford, A.C.; Moayyedi, P.; Lacy, B.E.; Lembo, A.J.; Saito, Y.A.; Schiller, L.R.; Soffer, E.E.; Spiegel, B.M.; Quigley, E.M. Task Force on the Management of Functional Bowel Disorders. American College of Gastroenterology monograph on the management of irritable bowel syndrome and chronic idiopathic constipation. Am. J. Gastroenterol. 2014, 109 (Suppl. 1), S2–S26. [Google Scholar] [CrossRef]
- Spiegel, B.M.; Farid, M.; Esrailian, E.; Talley, J.; Chang, L. Is irritable bowel syndrome a diagnosis of exclusion?: A survey of primary care providers, gastroenterologists, and IBS experts. Am. J. Gastroenterol. 2010, 105, 848–858. [Google Scholar] [CrossRef]
- Ford, A.C.; Lacy, B.E.; Talley, N.J. Irritable Bowel Syndrome. N. Engl. J. Med. 2017, 376, 2566–2578. [Google Scholar] [CrossRef] [Green Version]
- Sood, R.; Gracie, D.J.; Law, G.R.; Ford, A.C. Systematic review with meta-analysis: The accuracy of diagnosing irritable bowel syndrome with symptoms, biomarkers and/or psychological markers. Aliment. Pharmacol. Ther. 2015, 42, 491–503. [Google Scholar] [CrossRef]
- Cremonini, F.; Talley, N.J. Diagnostic and therapeutic strategies in the irritable bowel syndrome. Minerva Med. 2004, 95, 427–441. [Google Scholar]
- Tack, J.; Fried, M.; Houghton, L.A.; Spicak, J.; Fisher, G. Systematic review: The efficacy of treatments for irritable bowel syndrome—A European perspective. Aliment. Pharmacol. Ther. 2006, 24, 183–205. [Google Scholar] [CrossRef]
- Lembo, A. Irritable bowel syndrome medications side effects survey. J. Clin. Gastroenterol. 2004, 38, 776–781. [Google Scholar] [CrossRef]
- Ford, A.C.; Quigley, E.M.; Lacy, B.E.; Lembo, A.J.; Saito, Y.A.; Schiller, L.R.; Soffer, E.E.; Spiegel, B.M.; Moayyedi, P. Efficacy of prebiotics, probiotics, and synbiotics in irritable bowel syndrome and chronic idiopathic constipation: Systematic review and meta-analysis. Am. J. Gastroenterol. 2014, 109, 1547–1561. [Google Scholar] [CrossRef]
- Ford, A.C.; Quigley, E.M.; Lacy, B.E.; Lembo, A.J.; Saito, Y.A.; Schiller, L.R.; Soffer, E.E.; Spiegel, B.M.; Moayyedi, P. Effect of antidepressants and psychological therapies, including hypnotherapy, in irritable bowel syndrome: Systematic review and meta-analysis. Am. J. Gastroenterol. 2014, 109, 1350–1365. [Google Scholar] [CrossRef]
- Bellini, M.; Gambaccini, D.; Stasi, C.; Urbano, M.T.; Marchi, S.; Usai-Satta, P. Irritable bowel syndrome: A disease still searching for pathogenesis, diagnosis and therapy. World J. Gastroenterol. 2014, 20, 8807–8820. [Google Scholar]
- Habba, S.F. Diarrhea Predominant Irritable Bowel Syndrome (IBS-D): Fact or fiction. Med. Hypotheses 2011, 76, 97–99. [Google Scholar] [CrossRef]
- Holtmann, G.J.; Ford, A.C.; Talley, N.J. Pathophysiology of irritable bowel syndrome. Lancet Gastroenterol. Hepatol. 2016, 1, 133–146. [Google Scholar] [CrossRef]
- Enck, P.; Aziz, Q.; Barbara, G.; Farmer, A.D.; Fukudo, S.; Mayer, E.A.; Niesler, B.; Quigley, E.M.; Rajilić-Stojanović, M.; Schemann, M.; et al. Irritable bowel syndrome. Nat. Rev. Dis. Primers 2016, 2, 16014. [Google Scholar] [CrossRef]
- Bland, J. Defining Function in the Functional Medicine Model. Integr. Med. Encinitas 2017, 16, 22–25. [Google Scholar]
- Goepp, J.; Fowler, E.; McBride, T.; Landis, D. Frequency of abnormal fecal biomarkers in irritable bowel syndrome. Glob. Adv. Health Med. 2014, 3, 9–15. [Google Scholar] [CrossRef]
- Emmanuel, A.; Landis, D.; Peucker, M.; Hungin, A.P. Faecal biomarker patterns in patients with symptoms of irritable bowel syndrome. Frontline Gastroenterol. 2016, 7, 275–282. [Google Scholar] [CrossRef] [Green Version]
- Parsons, K.; Goepp, J.; Dechairo, B.; Fowler, E.; Markward, N.; Hanaway, P.; McBride, T.; Landis, D. Novel Testing Enhances Irritable Bowel Syndrome Medical Management: The IMMINENT Study. Glob. Adv. Health Med. 2014, 3, 25–32. [Google Scholar] [CrossRef]
- Quigley, E.M.; Shanahan, F. The language of medicine: Words as servants and scoundrels. Clin. Med. 2009, 9, 131–135. [Google Scholar] [CrossRef]
- Lee, C.; Doo, E.; Choi, J.M.; Jang, S.H.; Ryu, H.S.; Lee, J.Y.; Oh, J.H.; Park, J.H.; Kim, Y.S.; Brain-Gut Axis Research Group of Korean Society of Neurogastroenterology and Motility. The Increased Level of Depression and Anxiety in Irritable Bowel Syndrome Patients Compared with Healthy Controls: Systematic Review and Meta-analysis. J. Neurogastroenterol. Motil. 2017, 23, 349–362. [Google Scholar] [CrossRef] [Green Version]
- Koloski, N.A.; Jones, M.; Talley, N.J. Evidence that independent gut-to-brain and brain-to-gut pathways operate in the irritable bowel syndrome and functional dyspepsia: A 1-year population-based prospective study. Aliment. Pharmacol. Ther. 2016, 44, 592–600. [Google Scholar] [CrossRef]
- Bennett, E.J.; Tennant, C.C.; Piesse, C.; Badcock, C.A.; Kellow, J.E. Level of chronic life stress predicts clinical outcome in irritable bowel syndrome. Gut 1998, 43, 256–261. [Google Scholar] [CrossRef] [Green Version]
- Park, S.H.; Naliboff, B.D.; Shih, W.; Presson, A.P.; Videlock, E.J.; Ju, T.; Kilpatrick, L.; Gupta, A.; Mayer, E.A.; Chang, L. Resilience is decreased in irritable bowel syndrome and associated with symptoms and cortisol response. Neurogastroenterol. Motil. 2017. [Google Scholar] [CrossRef]
- Muscatello, M.R.; Bruno, A.; Scimeca, G.; Pandolfo, G.; Zoccali, R.A. Role of negative affects in pathophysiology and clinical expression of irritable bowel syndrome. World J. Gastroenterol. 2014, 20, 7570–7586. [Google Scholar] [CrossRef]
- Konturek, P.C.; Brzozowski, T.; Konturek, S.J. Stress and the gut: Pathophysiology, clinical consequences, diagnostic approach and treatment options. J. Physiol. Pharmacol. 2011, 62, 591–599. [Google Scholar]
- Suárez-Hitz, K.A.; Otto, B.; Bidlingmaier, M.; Schwizer, W.; Fried, M.; Ehlert, U. Altered psychobiological responsiveness in women with irritable bowel syndrome. Psychosom. Med. 2012, 74, 221–231. [Google Scholar] [CrossRef]
- Stasi, C.; Bellini, M.; Gambaccini, D.; Duranti, E.; de Bortoli, N.; Fani, B.; Albano, E.; Russo, S.; Sudano, I.; Laffi, G.; et al. Neuroendocrine Dysregulation in Irritable Bowel Syndrome Patients: A Pilot Study. J. Neurogastroenterol. Motil. 2017, 23, 428–434. [Google Scholar] [CrossRef] [Green Version]
- Kohen, R.; Tracy, J.H.; Haugen, E.; Cain, K.C.; Jarrett, M.E.; Heitkemper, M.M. Rare Variants of the Serotonin Transporter Are Associated With Psychiatric Comorbidity in Irritable Bowel Syndrome. Biol. Res. Nurs. 2016, 18, 394–400. [Google Scholar] [CrossRef] [Green Version]
- Jin, D.C.; Cao, H.L.; Xu, M.Q.; Wang, S.N.; Wang, Y.M.; Yan, F.; Wang, B.M. Regulation of the serotonin transporter in the pathogenesis of irritable bowel syndrome. World J. Gastroenterol. 2016, 22, 8137–8148. [Google Scholar] [CrossRef] [PubMed]
- Karling, P.; Danielsson, Å.; Wikgren, M.; Söderström, I.; Del-Favero, J.; Adolfsson, R.; Norrback, K.F. The relationship between the val158met catechol-O-methyltransferase (COMT) polymorphism and irritable bowel syndrome. PLoS ONE 2011, 6, e18035. [Google Scholar] [CrossRef] [PubMed]
- Han, C.J.; Kohen, R.; Jun, S.; Jarrett, M.E.; Cain, K.C.; Burr, R.; Heitkemper, M.M. COMT Val158Met Polymorphism and Symptom Improvement Following a Cognitively Focused Intervention for Irritable Bowel Syndrome. Nurs. Res. 2017, 66, 75–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballou, S.; Keefer, L. Psychological Interventions for Irritable Bowel Syndrome and Inflammatory Bowel Diseases. Clin. Transl. Gastroenterol. 2017, 8, e214. [Google Scholar] [CrossRef] [PubMed]
- Lowén, M.B.; Mayer, E.A.; Sjöberg, M.; Tillisch, K.; Naliboff, B.; Labus, J.; Lundberg, P.; Ström, M.; Engström, M.; Walter, S.A. Effect of hypnotherapy and educational intervention on brain response to visceral stimulus in the irritable bowel syndrome. Aliment. Pharmacol. Ther. 2013, 37, 1184–1197. [Google Scholar] [CrossRef] [PubMed]
- Konturek, P.C.; Brzozowski, T.; Konturek, S.J. Gut clock: Implication of circadian rhythms in the gastrointestinal tract. J. Physiol. Pharmacol. 2011, 62, 139–150. [Google Scholar] [PubMed]
- Rotem, A.Y.; Sperber, A.D.; Krugliak, P.; Freidman, B.; Tal, A.; Tarasiuk, A. Polysomnographic and actigraphic evidence of sleep fragmentation in patients with irritable bowel syndrome. Sleep 2003, 26, 747–752. [Google Scholar] [CrossRef]
- Buchanan, D.T.; Cain, K.; Heitkemper, M.; Burr, R.; Vitiello, M.V.; Zia, J.; Jarrett, M. Sleep measures predict next-day symptoms in women with irritable bowel syndrome. J. Clin. Sleep Med. 2014, 10, 1003–1009. [Google Scholar] [CrossRef]
- Patel, A.; Hasak, S.; Cassell, B.; Ciorba, M.A.; Vivio, E.E.; Kumar, M.; Gyawali, C.P.; Sayuk, G.S. Effects of disturbed sleep on gastrointestinal and somatic pain symptoms in irritable bowel syndrome. Aliment. Pharmacol. Ther. 2016, 44, 246–258. [Google Scholar] [CrossRef]
- Nojkov, B.; Rubenstein, J.H.; Chey, W.D.; Hoogerwerf, W.A. The impact of rotating shift work on the prevalence of irritable bowel syndrome in nurses. Am. J. Gastroenterol. 2010, 105, 842–847. [Google Scholar] [CrossRef]
- Wisniewska-Jarosinska, M.; Chojnacki, J.; Konturek, S.; Brzozowski, T.; Smigielski, J.; Chojnacki, C. Evaluation of urinary 6-hydroxymelatonin sulphate excretion in women at different age with irritable bowel syndrome. J. Physiol. Pharmacol. 2010, 61, 295–300. [Google Scholar] [PubMed]
- Radwan, P.; Skrzydlo-Radomanska, B.; Radwan-Kwiatek, K.; Burak-Czapiuk, B.; Strzemecka, J. Is melatonin involved in the irritable bowel syndrome? J. Physiol. Pharmacol. 2009, 60 (Suppl. 3), 67–70. [Google Scholar] [PubMed]
- Song, G.H.; Leng, P.H.; Gwee, K.A.; Moochhala, S.M.; Ho, K.Y. Melatonin improves abdominal pain in irritable bowel syndrome patients who have sleep disturbances: A randomised, double blind, placebo controlled study. Gut 2005, 54, 1402–1407. [Google Scholar] [CrossRef] [PubMed]
- Mozaffari, S.; Rahimi, R.; Abdollahi, M. Implications of melatonin therapy in irritable bowel syndrome: A systematic review. Curr. Pharm. Des. 2010, 16, 3646–3655. [Google Scholar] [CrossRef] [PubMed]
- Stevens, R.G. Light-at-night, circadian disruption and breast cancer: Assessment of existing evidence. Int. J. Epidemiol. 2009, 38, 963–970. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.K.; Saltin, B. Exercise as medicine-evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci Sports 2015, 25 (Suppl. 3), 1–72. [Google Scholar] [CrossRef] [PubMed]
- Dainese, R.; Serra, J.; Azpiroz, F.; Malagelada, J.R. Effects of physical activity on intestinal gas transit and evacuation in healthy subjects. Am. J. Med. 2004, 116, 536–539. [Google Scholar] [CrossRef]
- De Schryver, A.M.; Keulemans, Y.C.; Peters, H.P.; Akkermans, L.M.; Smout, A.J.; De Vries, W.R.; van Berge-Henegouwen, G.P. Effects of regular physical activity on defecation pattern in middle-aged patients complaining of chronic constipation. Scand. J. Gastroenterol. 2005, 40, 422–429. [Google Scholar] [CrossRef]
- Matsuzaki, J.; Suzuki, H.; Masaoka, T.; Tanaka, K.; Mori, H.; Kanai, T. Influence of regular exercise on gastric emptying in healthy men: A pilot study. J. Clin. Biochem. Nutr. 2016, 59, 130–133. [Google Scholar] [CrossRef]
- Johannesson, E.; Ringström, G.; Abrahamsson, H.; Sadik, R. Intervention to increase physical activity in irritable bowel syndrome shows long-term positive effects. World J. Gastroenterol. 2015, 21, 600–608. [Google Scholar] [CrossRef]
- Shahabi, L.; Naliboff, B.D.; Shapiro, D. Self-regulation evaluation of therapeutic yoga and walking for patients with irritable bowel syndrome: A pilot study. Psychol. Health Med. 2016, 21, 176–188. [Google Scholar] [CrossRef] [PubMed]
- Nanayakkara, W.S.; Skidmore, P.M.; O’Brien, L.; Wilkinson, T.J.; Gearry, R.B. Efficacy of the low FODMAP diet for treating irritable bowel syndrome: The evidence to date. Clin. Exp. Gastroenterol. 2016, 9, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Marsh, A.; Eslick, E.M.; Eslick, G.D. Does a diet low in FODMAPs reduce symptoms associated with functional gastrointestinal disorders? A comprehensive systematic review and meta-analysis. Eur. J. Nutr. 2016, 55, 897–906. [Google Scholar] [CrossRef] [PubMed]
- Cozma-Petruţ, A.; Loghin, F.; Miere, D.; Dumitraşcu, D.L. Diet in irritable bowel syndrome: What to recommend, not what to forbid to patients! World J. Gastroenterol. 2017, 23, 3771–3783. [Google Scholar] [CrossRef]
- Böhn, L.; Störsrud, S.; Liljebo, T.; Collin, L.; Lindfors, P.; Törnblom, H.; Simrén, M. Diet low in FODMAPs reduces symptoms of irritable bowel syndrome as well as traditional dietary advice: A randomized controlled trial. Gastroenterology 2015, 149, 1399–1407. [Google Scholar] [CrossRef] [PubMed]
- Hurst, A.; Knott, F. Intestinal carbohydrate dyspepsia. QJM 1931, 94, 171–179. [Google Scholar] [CrossRef]
- Ledochowski, M.; Widner, B.; Bair, H.; Probst, T.; Fuchs, D. Fructose- and sorbitol-reduced diet improves mood and gastrointestinal disturbances in fructose malabsorbers. Scand. J. Gastroenterol. 2000, 35, 1048–1052. [Google Scholar] [CrossRef]
- Austin, G.L.; Dalton, C.B.; Hu, Y.; Morris, C.B.; Hankins, J.; Weinland, S.R.; Westman, E.C.; Yancy, W.S., Jr.; Drossman, D.A. A very low-carbohydrate diet improves symptoms and quality of life in diarrhea-predominant irritable bowel syndrome. Clin. Gastroenterol. Hepatol. 2009, 7, 706–708. [Google Scholar] [CrossRef]
- O’Dwyer, D.D.; Darville, R.L. Specific carbohydrate diet: Irritable bowel syndrome patient case study. Nutr. Food Sci. 2015, 45, 859–872. [Google Scholar] [CrossRef]
- Ierardi, E.; Losurdo, G.; Sorrentino, C.; Giorgio, F.; Rossi, G.; Marinaro, A.; Romagno, K.R.; Di Leo, A.; Principi, M. Macronutrient intakes in obese subjects with or without small intestinal bacterial overgrowth: An alimentary survey. Scand. J. Gastroenterol. 2016, 51, 277–280. [Google Scholar] [CrossRef]
- Parlesak, A.; Klein, B.; Schecher, K.; Bode, J.C.; Bode, C. Prevalence of small bowel bacterial overgrowth and its association with nutrition intake in nonhospitalized older adults. J. Am. Geriatr. Soc. 2003, 51, 768–773. [Google Scholar] [CrossRef] [PubMed]
- Barrett, J.S. How to institute the low-FODMAP diet. J. Gastroenterol. Hepatol. 2017, 32 (Suppl. 1), 8–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fedewa, A.; Rao, S.S. Dietary fructose intolerance, fructan intolerance and FODMAPs. Curr. Gastroenterol. Rep. 2014, 16, 370. [Google Scholar] [CrossRef] [PubMed]
- Nucera, G.; Gabrielli, M.; Lupascu, A.; Lauritano, E.C.; Santoliquido, A.; Cremonini, F.; Cammarota, G.; Tondi, P.; Pola, P.; Gasbarrini, G.; et al. Abnormal breath tests to lactose, fructose and sorbitol in irritable bowel syndrome may be explained by small intestinal bacterial overgrowth. Aliment. Pharmacol. Ther. 2005, 21, 1391–1395. [Google Scholar] [CrossRef] [PubMed]
- Kwiatkowski, L.; Rice, E.; Langland, J. Integrative Treatment of Chronic Abdominal Bloating and Pain Associated With Overgrowth of Small Intestinal Bacteria: A Case Report. Altern. Ther. Health Med. 2017, 23, 56–61. [Google Scholar]
- Henström, M.; Diekmann, L.; Bonfiglio, F.; Hadizadeh, F.; Kuech, E.M.; von Köckritz-Blickwede, M.; Thingholm, L.B.; Zheng, T.; Assadi, G.; Dierks, C.; et al. Functional variants in the sucrase-isomaltase gene associate with increased risk of irritable bowel sydrome. Gut 2018, 67, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Farup, P.G.; Monsbakken, K.W.; Vandvik, P.O. Lactose malabsorption in a population with irritable bowel syndrome: Prevalence and symptoms. A case-control study. Scand. J. Gastroenterol. 2004, 39, 645–649. [Google Scholar] [CrossRef]
- Gupta, D.; Ghoshal, U.C.; Misra, A.; Misra, A.; Choudhuri, G.; Singh, K. Lactose intolerance in patients with irritable bowel syndrome from northern India: A case-control study. J. Gastroenterol. Hepatol. 2007, 22, 2261–2265. [Google Scholar] [CrossRef]
- Xiong, L.; Wang, Y.; Gong, X.; Chen, M. Prevalence of lactose intolerance in patients with diarrhea-predominant irritable bowel syndrome: Data from a tertiary center in southern China. J. Health Popul. Nutr. 2017, 36, 38. [Google Scholar] [CrossRef]
- Varjú, P.; Gede, N.; Szakács, Z.; Hegyi, P.; Cazacu, I.M.; Pécsi, D.; Fábián, A.; Szepes, Z.; Vincze, Á.; Tenk, J.; et al. Lactose intolerance but not lactose maldigestion is more frequent in patients with irritable bowel syndrome than in healthy controls: A meta-analysis. Neurogastroenterol. Motil. 2019, 31, e13527. [Google Scholar] [CrossRef]
- Misselwitz, B.; Pohl, D.; Frühauf, H.; Fried, M.; Vavricka, S.R.; Fox, M. Lactos malabsorption and intolerance: Pathogenesis, diagnosis and treatment. United Eur. Gastroenterol. J. 2013, 1, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Tolliver, B.A.; Jackson, M.S.; Jackson, K.L.; Barnett, E.D.; Chastang, J.F.; DiPalma, J.A. Does lactose maldigestion really play a role in the irritable bowel? J. Clin. Gastroenterol. 1996, 23, 15–17. [Google Scholar] [CrossRef] [PubMed]
- Suarez, F.L.; Savaiano, D.A.; Levitt, M.D. A comparison of symptoms after the consumption of milk or lactose-hydrolyzed milk by people with self-reported severe lactose intolerance. N. Engl. J. Med. 1995, 333, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Lisker, R.; Solomons, N.W.; Pérez Briceño, R.; Ramírez Mata, M. Lactase and placebo in the management of the irritable bowel syndrome: A double-blind, cross-over study. Am. J. Gastroenterol. 1989, 84, 756–762. [Google Scholar] [PubMed]
- Moritz, K.; Hemmer, W.; Jung, P.; Sesztak-Greinecker, G.; Götz, M.; Jarisch, R.; Wantke, F. Effect of a fructose and lactose elimination diet in patients with irritable bowel syndrome: A randomized double-blind placebo-controlled study. J. Gastroenterol. Hepatol. Res. 2013, 2, 833–839. [Google Scholar]
- Vernia, P.; Ricciardi, M.R.; Frandina, C.; Bilotta, T.; Frieri, G. Lactose malabsorption and irritable bowel syndrome. Effect of a long-term lactose-free diet. Ital. J. Gastroenterol. 1995, 27, 117–121. [Google Scholar] [PubMed]
- Böhmer, C.J.; Tuynman, H.A. The clinical relevance of lactose malabsorption inirritable bowel syndrome. Eur. J. Gastroenterol. Hepatol. 1996, 8, 1013–1016. [Google Scholar] [CrossRef] [PubMed]
- Parker, T.J.; Woolner, J.T.; Prevost, A.T.; Tuffnell, Q.; Shorthouse, M.; Hunter, J.O. Irritable bowel syndrome: Is the search for lactose intolerance justified? Eur. J. Gastroenterol. Hepatol. 2001, 13, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Fox, M.; Cong, Y.; Chu, H.; Zheng, X.; Long, Y.; Fried, M.; Dai, N. Lactose intolerance in irritable bowel syndrome patients with diarrhoea: The roles of anxiety, activation of the innate mucosal immune system and visceral sensitivity. Aliment. Pharmacol. Ther. 2014, 39, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Misselwitz, B.; Dai, N.; Fox, M. Lactose Intolerance in Adults: Biological Mechanism and Dietary Management. Nutrients 2015, 7, 8020–8035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mansueto, P.; D’Alcamo, A.; Seidita, A.; Carroccio, A. Food allergy in irritable bowel syndrome: The case of non-celiac wheat sensitivity. World J. Gastroenterol. 2015, 21, 7089–7109. [Google Scholar] [CrossRef] [PubMed]
- Choung, R.S.; Talley, N.J. Food Allergy and Intolerance in IBS. Gastroenterol. Hepatol. 2006, 2, 756–760. [Google Scholar]
- Nanda, R.; James, R.; Smith, H.; Dudley, C.R.; Jewell, D.P. Food intolerance and the irritable bowel syndrome. Gut 1989, 30, 1099–1104. [Google Scholar] [CrossRef]
- Jones, V.A.; McLaughlan, P.; Shorthouse, M.; Workman, E.; Hunter, J.O. Food intolerance: A major factor in the pathogenesis of irritable bowel syndrome. Lancet 1982, 2, 1115–1117. [Google Scholar] [CrossRef]
- Bentley, S.J.; Pearson, D.J.; Rix, K.J. Food hypersensitivity in irritable bowel syndrome. Lancet 1983, 2, 295–297. [Google Scholar] [CrossRef]
- McKee, A.M.; Prior, A.; Whorwell, P.J. Exclusion diets in irritable bowel syndrome: Are they worthwhile? J. Clin. Gastroenterol. 1987, 9, 526–528. [Google Scholar] [CrossRef] [PubMed]
- Niec, A.M.; Frankum, B.; Talley, N.J. Are adverse food reactions linked to irritable bowel syndrome? Am. J. Gastroenterol. 1998, 93, 2184–2190. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Salem, A.; Nanavati, J.; Mullin, G.E. The Role of Diet in the Treatment of Irritable Bowel Syndrome: A Systematic Review. Gastroenterol. Clin. North. Am. 2018, 47, 107–137. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, W.; Sheldon, T.A.; Shaath, N.; Whorwell, P.J. Food elimination based on IgG antibodies in irritable bowel syndrome: A randomised controlled trial. Gut 2004, 53, 1459–1464. [Google Scholar] [CrossRef]
- Zar, S.; Mincher, L.; Benson, M.J.; Kumar, D. Food-specific IgG4 antibody-guided exclusion diet improves symptoms and rectal compliance in irritable bowel syndrome. Scand. J. Gastroenterol. 2005, 40, 800–807. [Google Scholar] [CrossRef]
- Drisko, J.; Bischoff, B.; Hall, M.; McCallum, R. Treating irritable bowel syndrome with a food elimination diet followed by food challenge and probiotics. J. Am. Coll. Nutr. 2006, 25, 514–522. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.M.; Li, Y.Q. The therapeutic effects of eliminating allergic foods according to food-specific IgG antibodies in irritable bowel syndrome. Zhonghua Nei Ke Za Zhi 2007, 46, 641–643. (In Chinese) [Google Scholar] [PubMed]
- Guo, H.; Jiang, T.; Wang, J.; Chang, Y.; Guo, H.; Zhang, W. The value of eliminating foods according to food-specific immunoglobulin G antibodies in irritable bowel syndrome with diarrhoea. J. Int. Med. Res. 2012, 40, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Aydinlar, E.I.; Dikmen, P.Y.; Tiftikci, A.; Saruc, M.; Aksu, M.; Gunsoy, H.G.; Tozun, N. IgG-based elimination diet in migraine plus irritable bowel syndrome. Headache 2013, 53, 514–525. [Google Scholar] [CrossRef] [PubMed]
- Zwetchkenbaum, J.; Burakoff, R. The irritable bowel syndrome and food hypersensitivity. Ann. Allergy. 1988, 61, 47–49. [Google Scholar] [PubMed]
- Zar, S.; Benson, M.J.; Kumar, D. Food-specific serum IgG4 and IgE titers to common food antigens in irritable bowel syndrome. Am. J. Gastroenterol. 2005, 100, 1550–1557. [Google Scholar] [CrossRef] [PubMed]
- Zuo, X.L.; Li, Y.Q.; Li, W.J.; Guo, Y.T.; Lu, X.F.; Li, J.M.; Desmond, P.V. Alterations of food antigen-specific serum immunoglobulins G and E antibodies in patients with irritable bowel syndrome and functional dyspepsia. Clin. Exp. Allergy 2007, 37, 823–830. [Google Scholar] [CrossRef]
- Kennedy, D.A.; Lewis, E.; Cooley, K.; Fitz, H. An exploratory comparative investigation of Food Allergy/Sensitivity Testing in IBS (The FAST Study): A comparison between various laboratory methods and an elimination diet. Adv. Integr. Med. 2014, 1, 124–130. [Google Scholar] [CrossRef]
- Ligaarden, S.C.; Lydersen, S.; Farup, P.G. IgG and IgG4 antibodies in subjects with irritable bowel syndrome: A case control study in the general population. BMC Gastroenterol. 2012, 12, 166. [Google Scholar] [CrossRef]
- Mullin, G.E.; Swift, K.M.; Lipski, L.; Turnbull, L.K.; Rampertab, S.D. Testing for food reactions: The good, the bad, and the ugly. Nutr. Clin. Pract. 2010, 25, 192–198. [Google Scholar] [CrossRef]
- Catassi, C.; Bai, J.C.; Bonaz, B.; Bouma, G.; Calabrò, A.; Carroccio, A.; Castillejo, G.; Ciacci, C.; Cristofori, F.; Dolinsek, J.; et al. Non-Celiac Gluten sensitivity: The new frontier of gluten related disorders. Nutrients 2013, 5, 3839–3853. [Google Scholar] [CrossRef] [PubMed]
- Volta, U.; Pinto-Sanchez, M.I.; Boschetti, E.; Caio, G.; De Giorgio, R.; Verdu, E.F. Dietary Triggers in Irritable Bowel Syndrome: Is There a Role for Gluten? J. Neurogastroenterol. Motil. 2016, 22, 547–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biesiekierski, J.R.; Newnham, E.D.; Irving, P.M.; Barrett, J.S.; Haines, M.; Doecke, J.D.; Shepherd, S.J.; Muir, J.G.; Gibson, P.R. Gluten causes gastrointestinal symptoms in subjects without celiac disease: A double-blind randomized placebo-controlled trial. Am. J. Gastroenterol. 2011, 106, 508–514. [Google Scholar] [CrossRef] [PubMed]
- Carroccio, A.; Mansueto, P.; Iacono, G.; Soresi, M.; D’Alcamo, A.; Cavataio, F.; Brusca, I.; Florena, A.M.; Ambrosiano, G.; Seidita, A.; et al. Non-celiac wheat sensitivity diagnosed by double-blind placebo-controlled challenge: Exploring a new clinical entity. Am. J. Gastroenterol. 2012, 107, 1898–1906. [Google Scholar] [CrossRef] [PubMed]
- Vazquez-Roque, M.I.; Camilleri, M.; Smyrk, T.; Murray, J.A.; Marietta, E.; O’Neill, J.; Carlson, P.; Lamsam, J.; Janzow, D.; Eckert, D.; et al. A controlled trial of gluten-free diet in patients with irritable bowel syndrome-diarrhea: Effects on bowel frequency and intestinal function. Gastroenterology 2013, 144, 903–911. [Google Scholar] [CrossRef] [PubMed]
- Aziz, I.; Trott, N.; Briggs, R.; North, J.R.; Hadjivassiliou, M.; Sanders, D.S. Efficacy of a Gluten-Free Diet in Subjects with Irritable Bowel Syndrome-Diarrhea Unaware of Their HLA-DQ2/8 Genotype. Clin. Gastroenterol. Hepatol. 2016, 14, 696–703. [Google Scholar] [CrossRef]
- Zanwar, V.G.; Pawar, S.V.; Gambhire, P.A.; Jain, S.S.; Surude, R.G.; Shah, V.B.; Contractor, Q.Q.; Rathi, P.M. Symptomatic improvement with gluten restriction in irritable bowel syndrome: A prospective, randomized, double blinded placebo controlled trial. Intest. Res. 2016, 14, 343–350. [Google Scholar] [CrossRef]
- Shahbazkhani, B.; Sadeghi, A.; Malekzadeh, R.; Khatavi, F.; Etemadi, M.; Kalantri, E.; Rostami-Nejad, M.; Rostami, K. Non-Celiac Gluten Sensitivity Has Narrowed the Spectrum of Irritable Bowel Syndrome: A Double-Blind Randomized Placebo-Controlled Trial. Nutrients 2015, 7, 4542–4554. [Google Scholar] [CrossRef] [Green Version]
- Catassi, C.; Elli, L.; Bonaz, B.; Bouma, G.; Carroccio, A.; Castillejo, G.; Cellier, C.; Cristofori, F.; de Magistris, L.; Dolinsek, J.; et al. Diagnosis of non-celiac gluten sensitivity (NCGS): The salerno experts’ criteria. Nutrients 2015, 7, 4966–4977. [Google Scholar] [CrossRef]
- Rizzi, A.; Nucera, E.; Laterza, L.; Gaetani, E.; Valenza, V.; Corbo, G.M.; Inchingolo, R.; Buonomo, A.; Schiavino, D.; Gasbarrini, A. Irritable Bowel Syndrome and Nickel Allergy: What Is the Role of the Low Nickel Diet? J. Neurogastroenterol. Motil. 2017, 23, 101–108. [Google Scholar] [CrossRef] [Green Version]
- Minelli, M.; Schiavino, D.; Musca, F.; Bruno, M.E.; Falagiani, P.; Mistrello, G.; Riva, G.; Braga, M.; Turi, M.C.; Di Rienzo, V.; et al. Oral hyposensitization to nickel induces clinical improvement and a decrease in TH1 and TH2 cytokines in patients with systemic nickel allergy syndrome. Int. J. Immunopathol. Pharmacol. 2010, 23, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Picarelli, A.; Di Tola, M.; Vallecoccia, A.; Libanori, V.; Magrelli, M.; Carlesimo, M.; Rossi, A. Oral mucosa patch test: A new tool to recognize and study the adverse effects of dietary nickel exposure. Biol. Trace Elem. Res. 2011, 139, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Borghini, R.; Puzzono, M.; Rosato, E.; Di Tola, M.; Marino, M.; Greco, F.; Picarelli, A. Nickel-Related Intestinal Mucositis in IBS-Like Patients: Laser Doppler Perfusion Imaging and Oral Mucosa Patch Test in Use. Biol. Trace Elem. Res. 2016, 173, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Borghini, R.; Donato, G.; Alvaro, D.; Picarelli, A. New insights in IBS-like disorders: Pandora’s box has been opened; a review. Gastroenterol. Hepatol. Bed Bench 2017, 10, 79–89. [Google Scholar] [PubMed]
- Khayyat, Y.; Attar, S. Vitamin D Deficiency in Patients with Irritable Bowel Syndrome: Does it Exist? Oman Med. J. 2015, 30, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Nwosu, B.U.; Maranda, L.; Candela, N. Vitamin D status in pediatric irritable bowel syndrome. PLoS ONE 2017, 12, e0172183. [Google Scholar]
- Li, Y.C.; Chen, Y.; Du, J. Critical roles of intestinal epithelial vitamin D receptor signaling in controlling gut mucosal inflammation. J. Steroid Biochem. Mol. Biol. 2015, 148, 179–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cantorna, M.T.; McDaniel, K.; Bora, S.; Chen, J.; James, J. Vitamin D, immune regulation, the microbiota, and inflammatory bowel disease. Exp. Biol. Med. 2014, 239, 1524–1530. [Google Scholar] [CrossRef] [Green Version]
- Bashir, M.; Prietl, B.; Tauschmann, M.; Mautner, S.I.; Kump, P.K.; Treiber, G.; Wurm, P.; Gorkiewicz, G.; Högenauer, C.; Pieber, T.R. Effects of high doses of vitamin D3 on mucosa-associated gut microbiome vary between regions of the human gastrointestinal tract. Eur. J. Nutr. 2016, 55, 1479–1489. [Google Scholar] [CrossRef]
- Sprake, E.F.; Grant, V.A.; Corfe, B.M. Vitamin D3 as a novel treatment for irritable bowel syndrome: Single case leads to critical analysis of patient-centred data. BMJ Case Rep. 2012, 2012. [Google Scholar] [CrossRef]
- Abbasnezhad, A.; Amani, R.; Hajiani, E.; Alavinejad, P.; Cheraghian, B.; Ghadiri, A. Effect of vitamin D on gastrointestinal symptoms and health-related quality of life in irritable bowel syndrome patients: A randomized double-blind clinical trial. Neurogastroenterol. Motil. 2016. [Google Scholar] [CrossRef] [PubMed]
- Leeds, J.S.; Hopper, A.D.; Sidhu, R.; Simmonette, A.; Azadbakht, N.; Hoggard, N.; Morley, S.; Sanders, D.S. Some patients with irritable bowel syndrome may have exocrine pancreatic insufficiency. Clin. Gastroenterol. Hepatol. 2010, 8, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Money, M.E.; Walkowiak, J.; Virgilio, C.; Talley, N.J. Pilot study: A randomised, double blind, placebo controlled trial of pancrealipase for the treatment of postprandial irritable bowel syndrome-diarrhoea. Frontline Gastroenterol. 2011, 2, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Tuck, C.J.; Taylor, K.M.; Gibson, P.R.; Barrett, J.S.; Muir, J.G. Increasing Symptoms in Irritable Bowel Symptoms With Ingestion of Galacto-Oligosaccharides Are Mitigated by α-Galactosidase Treatment. Am. J. Gastroenterol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Menees, S.B.; Powell, C.; Kurlander, J.; Goel, A.; Chey, W.D. A meta-analysis of the utility of C-reactive protein, erythrocyte sedimentation rate, fecal calprotectin, and fecal lactoferrin to exclude inflammatory bowel disease in adults with IBS. Am. J. Gastroenterol. 2015, 110, 444–454. [Google Scholar] [CrossRef] [PubMed]
- Martin-Viñas, J.J.; Quigley, E.M. Immune response in irritable bowel syndrome: A systematic review of systemic and mucosal inflammatory mediators. J. Dig. Dis. 2016, 17, 572–581. [Google Scholar] [CrossRef] [PubMed]
- Spiller, R. Irritable bowel syndrome: New insights into symptom mechanisms and advances in treatment. F1000Research 2016, 5. [Google Scholar] [CrossRef]
- Melchior, C.; Aziz, M.; Aubry, T.; Gourcerol, G.; Quillard, M.; Zalar, A.; Coëffier, M.; Dechelotte, P.; Leroi, A.M.; Ducrotté, P. Does calprotectin level identify a subgroup among patients suffering from irritable bowel syndrome? Results of a prospective study. United Eur. Gastroenterol. J. 2017, 5, 261–269. [Google Scholar] [CrossRef]
- Barbara, G.; Cremon, C.; Annese, V.; Basilisco, G.; Bazzoli, F.; Bellini, M.; Benedetti, A.; Benini, L.; Bossa, F.; Buldrini, P.; et al. Randomised controlled trial of mesalazine in IBS. Gut 2016, 65, 82–90. [Google Scholar] [CrossRef]
- Lam, C.; Tan, W.; Leighton, M.; Hastings, M.; Lingaya, M.; Falcone, Y.; Zhou, X.; Xu, L.; Whorwell, P.; Walls, A.F.; et al. A mechanistic multicentre, parallel group, randomised placebo-controlled trial of mesalazine for the treatment of IBS with diarrhoea (IBS-D). Gut 2016, 65, 91–99. [Google Scholar] [CrossRef]
- Wouters, M.M.; Balemans, D.; Van Wanrooy, S.; Dooley, J.; Cibert-Goton, V.; Alpizar, Y.A.; Valdez-Morales, E.E.; Nasser, Y.; Van Veldhoven, P.P.; Vanbrabant, W.; et al. Histamine Receptor H1-Mediated Sensitization of TRPV1 Mediates Visceral Hypersensitivity and Symptoms in Patients with Irritable Bowel Syndrome. Gastroenterology 2016, 150, 875–887. [Google Scholar] [CrossRef] [PubMed]
- Belcaro, G.; Gizzi, G.; Pellegrini, L.; Corsi, M.; Dugall, M.; Cacchio, M.; Feragalli, B.; Togni, S.; Riva, A.; Eggenhoffner, R.; et al. Supplementation with a lecithin-based delivery form of Boswellia serrata extract (Casperome®) controls symptoms of mild irritable bowel syndrome. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 2249–2254. [Google Scholar] [PubMed]
- Fritscher-Ravens, A.; Schuppan, D.; Ellrichmann, M.; Schoch, S.; Röcken, C.; Brasch, J.; Bethge, J.; Böttner, M.; Klose, J.; Milla, P.J. Confocal endomicroscopy shows food-associated changes in the intestinal mucosa of patients with irritable bowel syndrome. Gastroenterology 2014, 147, 1012–1020. [Google Scholar] [CrossRef] [PubMed]
- Piche, T.; Barbara, G.; Aubert, P.; Bruley des Varannes, S.; Dainese, R.; Nano, J.L.; Cremon, C.; Stanghellini, V.; De Giorgio, R.; Galmiche, J.P.; et al. Impaired intestinal barrier integrity in the colon of patients with irritable bowel syndrome: Involvement of soluble mediators. Gut 2009, 58, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Zhang, B.; Verne, G.N. Intestinal membrane permeability and hypersensitivity in the irritable bowel syndrome. Pain 2009, 146, 41–46. [Google Scholar] [CrossRef] [Green Version]
- Vazquez-Roque, M.I.; Camilleri, M.; Smyrk, T.; Murray, J.A.; O’Neill, J.; Carlson, P.; Lamsam, J.; Eckert, D.; Janzow, D.; Burton, D.; et al. Association of HLA-DQ gene with bowel transit, barrier function, and inflammation in irritable bowel syndrome with diarrhea. Am. J. Physiol.-Gastrointest. Liver Physiol. 2012, 303, G1262–G1269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shulman, R.J.; Jarrett, M.E.; Cain, K.C.; Broussard, E.K.; Heitkemper, M.M. Associations among gut permeability, infl ammatory markers, and symptoms in patients with irritable bowel syndrome. J. Gastroenterol. 2014, 49, 1467–1476. [Google Scholar] [CrossRef]
- Camilleri, M.; Lasch, K.; Zhou, W. Irritable bowel syndrome: Methods, mechanisms, and pathophysiology. The confluence of increased permeability, inflammation, and pain in irritable bowel syndrome. Am. J. Physiol.-Gastrointest. Liver Physiol. 2012, 303, G775–G785. [Google Scholar] [CrossRef]
- Barbara, G.; Zecchi, L.; Barbaro, R.; Cremon, C.; Bellacosa, L.; Marcellini, M.; De Giorgio, R.; Corinaldesi, R.; Stanghellini, V. Mucosal permeability and immune activation as potential therapeutic targets of probiotics in irritable bowel syndrome. J. Clin. Gastroenterol. 2012, 46, S52–S55. [Google Scholar] [CrossRef]
- Bischoff, S.C.; Barbara, G.; Buurman, W.; Ockhuizen, T.; Schulzke, J.D.; Serino, M.; Tilg, H.; Watson, A.; Wells, J.M. Intestinal permeability—A new target for disease prevention and therapy. BMC Gastroenterol. 2014, 14, 189. [Google Scholar] [CrossRef]
- Ahrne, S.; Hagslatt, M.L. Effect of lactobacilli on paracellular permeability in the gut. Nutrients 2011, 3, 104–117. [Google Scholar] [CrossRef] [PubMed]
- Michielan, A.; D’Incà, R. Intestinal Permeability in Inflammatory Bowel Disease: Pathogenesis, Clinical Evaluation, and Therapy of Leaky Gut. Mediat. Inflamm. 2015, 2015, 628157. [Google Scholar] [CrossRef] [PubMed]
- Zeng, J.; Li, Y.Q.; Zuo, X.L.; Zhen, Y.B.; Yang, J.; Liu, C.H. Clinical trial: Effect of active lactic acid bacteria on mucosal barrier function in patients with diarrhoea-predominant irritable bowel syndrome. Aliment. Pharmacol. Ther. 2008, 28, 994–1002. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Costinean, S.; Croce, C.M.; Brasier, A.R.; Merwat, S.; Larson, S.A.; Basra, S.; Verne, G.N. MicroRNA 29 targets nuclear factor-κB-repressing factor and Claudin 1 to increase intestinal permeability. Gastroenterology 2015, 148, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Verne, M.L.; Fields, J.Z.; Lefante, J.J.; Basra, S.; Salameh, H.; Verne, G.N. Randomised placebo-controlled trial of dietary glutamine supplements for postinfectious irritable bowel syndrome. Gut. 2019, 68, 996–1002. [Google Scholar]
- Camilleri, M. Bile Acid diarrhea: Prevalence, pathogenesis, and therapy. Gut Liver 2015, 9, 332–339. [Google Scholar] [CrossRef]
- Slattery, S.A.; Niaz, O.; Aziz, Q.; Ford, A.C.; Farmer, A.D. Systematic review with meta-analysis: The prevalence of bile acid malabsorption in the irritable bowel syndrome with diarrhoea. Aliment. Pharmacol. Ther. 2015, 42, 3–11. [Google Scholar] [CrossRef]
- Peleman, C.; Camilleri, M.; Busciglio, I.; Burton, D.; Donato, L.; Zinsmeister, A.R. Colonic Transit and Bile Acid Synthesis or Excretion in Patients with Irritable Bowel Syndrome-Diarrhea Without Bile Acid Malabsorption. Clin. Gastroenterol. Hepatol. 2017, 15, 720–727. [Google Scholar] [CrossRef]
- Camilleri, M. Advances in understanding of bile acid diarrhea. Expert Rev. Gastroenterol. Hepatol. 2014, 8, 49–61. [Google Scholar] [CrossRef]
- Camilleri, M.; Shin, A.; Busciglio, I.; Carlson, P.; Acosta, A.; Bharucha, A.E.; Burton, D.; Lamsam, J.; Lueke, A.; Donato, L.J.; et al. Genetic variation in GPBAR1 predisposes to quantitative changes in colonic transit and bile acid excretion. Am. J. Physiol.-Gastrointest. Liver Physiol. 2014, 307, G508–G516. [Google Scholar] [CrossRef] [Green Version]
- Money, M.E.; Camilleri, M. Review: Management of postprandial diarrhea syndrome. Am. J. Med. 2012, 125, 538–544. [Google Scholar] [CrossRef] [PubMed]
- O’Keefe, S.J. Diet, microorganisms and their metabolites, and colon cancer. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 691–706. [Google Scholar] [CrossRef] [PubMed]
- Joyce, S.A.; Gahan, C.G. Bile Acid Modifications at the Microbe-Host Interface: Potential for Nutraceutical and Pharmaceutical Interventions in Host Health. Annu. Rev. Food Sci. Technol. 2016, 7, 313–333. [Google Scholar] [CrossRef] [PubMed]
- Shekhar, C.; Monaghan, P.J.; Morris, J.; Issa, B.; Whorwell, P.J.; Keevil, B.; Houghton, L.A. Rome III functional constipation and irritable bowel syndrome with constipation are similar disorders within the spectrum of sensitization, regulated by serotonin. Gastroenterology 2013, 145, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Raahave, D.; Loud, F.B. Additional faecal reservoirs or hidden constipation: A link between functional and organic bowel disease. Dan. Med. Bull. 2004, 51, 422–425. [Google Scholar] [PubMed]
- Raahave, D.; Christensen, E.; Loud, F.B.; Knudsen, L.L. Correlation of bowel symptoms with colonic transit, length, and faecal load in functional faecal retention. Dan. Med. Bull. 2009, 56, 83–88. [Google Scholar]
- Wiesner, M.; Naylor, S.J.; Copping, A.; Furlong, A.; Lynch, A.G.; Parkes, M.; Hunter, J.O. Symptom classification in irritable bowel syndrome as a guide to treatment. Scand. J. Gastroenterol. 2009, 44, 796–803. [Google Scholar] [CrossRef]
- Simrén, M.; Barbara, G.; Flint, H.J.; Spiegel, B.M.; Spiller, R.C.; Vanner, S.; Verdu, E.F.; Whorwell, P.J.; Zoetendal, E.G.; Rome Foundation Committee. Intestinal microbiota in functional bowel disorders: A Rome foundation report. Gut 2013, 62, 159–176. [Google Scholar]
- Fan, W.T.; Ding, C.; Xu, N.N.; Zong, S.; Ma, P.; Gu, B. Close association between intestinal microbiota and irritable bowel syndrome. Eur. J. Clin. Microbiol. Infect. Dis. 2017. [Google Scholar] [CrossRef]
- Lyra, A.; Rinttilä, T.; Nikkilä, J.; Krogius-Kurikka, L.; Kajander, K.; Malinen, E.; Mättö, J.; Mäkelä, L.; Palva, A. Diarrhoea-predominant irritable bowel syndrome distinguishable by 16S rRNA gene phylotype quantification. World J. Gastroenterol. 2009, 15, 5936–5945. [Google Scholar] [CrossRef]
- Liu, H.N.; Wu, H.; Chen, Y.Z.; Chen, Y.J.; Shen, X.Z.; Liu, T.T. Altered molecular signature of intestinal microbiota in irritable bowel syndrome patients compared with healthy controls: A systematic review and meta-analysis. Dig. Liver Dis. 2017, 49, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Jeffery, I.B.; Quigley, E.M.; Öhman, L.; Simrén, M.; O’Toole, P.W. The microbiota link to irritable bowel syndrome: An emerging story. Gut Microbes 2012, 3, 572–576. [Google Scholar] [CrossRef] [PubMed]
- Rivière, A.; Selak, M.; Lantin, D.; Leroy, F.; De Vuyst, L. Bifidobacteria and Butyrate-Producing Colon Bacteria: Importance and Strategies for Their Stimulation in the Human Gut. Front. Microbiol. 2016, 7, 979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parkes, G.C.; Rayment, N.B.; Hudspith, B.N.; Petrovska, L.; Lomer, M.C.; Brostoff, J.; Whelan, K.; Sanderson, J.D. Distinct microbial populations exist in the mucosa-associated microbiota of sub-groups of irritable bowel syndrome. Neurogastroenterol. Motil. 2012, 24, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Quigley, E.M. Do patients with functional gastrointestinal disorders have an altered gut flora? Ther. Adv. Gastroenterol. 2009, 2, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Jalanka-Tuovinen, J.; Salonen, A.; Nikkil, J.; Immonen, O.; Kekkonen, R.; Lahti, L.; Palva, A.; de Vos, W.M. Intestinal microbiota in healthy adults: Temporal analysis reveals individual and common core and relation to intestinal symptoms. PLoS ONE 2011, 6, e23035. [Google Scholar] [CrossRef]
- Rajilic-Sotjanovic, M.; Biagi, E.; Heilig, H.G.; Kajander, K.; Kekkonen, R.A.; Tims, S.; de Vos, W.M. Global and deep molecular analysis of microbiota signatures in faecal samples from patients with irritable bowel syndrome. Gastroenterology 2011, 141, 1737–1801. [Google Scholar]
- Silk, D.B.; Davis, A.; Vulevic, J.; Tzortzis, G.; Gibson, G.R. Clinical trial: The effects of a trans-galactooligosaccharide prebiotic on faecal microbiota and symptoms in irritable bowel syndrome. Aliment. Pharmacol. Ther. 2009, 29, 508–518. [Google Scholar] [CrossRef]
- Paineau, D.; Payen, F.; Panserieu, S.; Coulombier, G.; Sobaszek, A.; Lartigau, I.; Brabet, M.; Galmiche, J.P.; Tripodi, D.; Sacher-Huvelin, S.; et al. The effects of regular consumption of short-chain fructo-oligosaccharides on digestive comfort of subjects with minor functional bowel disorders. Br. J. Nutr. 2008, 99, 311–318. [Google Scholar] [CrossRef] [Green Version]
- Azpiroz, F.; Dubray, C.; Bernalier-Donadille, A.; Cardot, J.M.; Accarino, A.; Serra, J.; Wagner, A.; Respondek, F.; Dapoigny, M. Effects of scFOS on the composition of fecal microbiota and anxiety in patients with irritable bowel syndrome: A randomized, double blind, placebo controlled study. Neurogastroenterol. Motil. 2017, 29, e12911. [Google Scholar] [CrossRef]
- Giannini, E.G.; Mansi, C.; Dulbecco, P.; Savarino, V. Role of partially hydrolyzed guar gum in the treatment of irritable bowel syndrome. Nutrition 2006, 22, 334–342. [Google Scholar] [CrossRef] [PubMed]
- Russo, L.; Andreozzi, P.; Zito, F.P.; Vozzella, L.; Savino, I.G.; Sarnelli, G.; Cuomo, R. Partially hydrolyzed guar gum in the treatment of irritable bowel syndrome with constipation: Effects of gender, age, and body mass index. Saudi J. Gastroenterol. 2015, 21, 104–110. [Google Scholar] [PubMed]
- Niv, E.; Halak, A.; Tiommny, E.; Yanai, H.; Strul, H.; Naftali, T.; Vaisman, N. Randomized clinical study: Partially hydrolyzed guar gum (PHGG) versus placebo in the treatment of patients with irritable bowel syndrome. Nutr. Metab. 2016, 13, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kristensen, N.B.; Bryrup, T.; Allin, K.H.; Nielsen, T.; Hansen, T.H.; Pedersen, O. Alterations in fecal microbiota composition by probiotic supplementation in healthy adults: A systematic review of randomized controlled trials. Genome Med. 2016, 8, 52. [Google Scholar] [CrossRef] [PubMed]
- Sanders, S.E. Probiotics and microbiota composition. BMC Med. 2016, 14, 82. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, Y.A.; Alder, A.; Anderson, W.; Wills, A.; Goddard, L.; Gulia, P.; Jankovich, E.; Mutch, P.; Reeves, L.B.; Singer, A.; et al. British Dietetic Association evidence-based guidelines for the dietary management of irritable bowel syndrome in adults. J. Hum. Nutr. Diet. 2012, 25, 260–274. [Google Scholar] [CrossRef]
- Allen, A.P.; Clarke, G.; Cryan, J.F.; Quigley, E.M.M.; Dinan, T.G. Bifidobacterium infantis 35624 and other probiotics in the management of irritable bowel syndrome. Strain specificity, symptoms, and mechanisms. Curr. Med. Res. Opin. 2017, 33, 1349–1351. [Google Scholar] [CrossRef]
- Nobutani, K.; Sawada, D.; Fujiwara, S.; Kuwano, Y.; Nishida, K.; Nakayama, J.; Kutsumi, H.; Azuma, T.; Rokutan, K. The effects of administration of the Lactobacillus gasseri strain CP2305 on quality of life, clinical symptoms and changes in gene expression in patients with irritable bowel syndrome. J. Appl. Microbiol. 2017, 122, 212–224. [Google Scholar] [CrossRef]
- Power, S.E.; O’Toole, P.W.; Stanton, C.; Ross, R.P.; Fitzgerald, G.F. Intestinal microbiota, diet and health. Br. J. Nutr. 2014, 111, 387–402. [Google Scholar] [CrossRef]
- Staudacher, H.M.; Lomer, M.C.; Anderson, J.L.; Barrett, J.S.; Muir, J.G.; Irving, P.M.; Whelan, K. Fermentable carbohydrate restriction reduces luminal bifidobacteria and gastrointestinal symptoms in patients with irritable bowel syndrome. J. Nutr. 2012, 142, 1510–1518. [Google Scholar] [CrossRef]
- Hill, P.; Muir, J.G.; Gibson, P.R. Controversies and Recent Developments of the Low-FODMAP Diet. Gastroenterol. Hepatol. 2017, 13, 36–45. [Google Scholar]
- McIntosh, K.; Reed, D.E.; Schneider, T.; Dang, F.; Keshteli, A.H.; De Palma, G.; Madsen, K.; Bercik, P.; Vanner, S. FODMAPs alter symptoms and the metabolome of patients with IBS: A randomised controlled trial. Gut 2017, 66, 1241–1251. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Choi, J.K.; Ryu, H.S.; Choi, C.H.; Kang, E.H.; Park, K.S.; Min, Y.W.; Hong, K.S. Therapeutic Modulation of Gut Microbiota in Functional Bowel Disorders. J. Neurogastroenterol. Motil. 2017, 23, 9–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sachdev, A.H.; Pimentel, M. Gastrointestinal bacterial overgrowth: Pathogenesis and clinical significance. Ther. Adv. Chronic Dis. 2013, 4, 223–231. [Google Scholar] [CrossRef]
- Ghoshal, U.C.; Shukla, R.; Ghoshal, U. Small Intestinal Bacterial Overgrowth and Irritable Bowel Syndrome: A Bridge between Functional Organic Dichotomy. Gut Liver 2017, 11, 196–208. [Google Scholar] [CrossRef] [PubMed]
- Pimentel, M. Review article: Potential mechanisms of action of rifaximin in the management of irritable bowel syndrome with diarrhoea. Aliment. Pharmacol. Ther. 2016, 43 (Suppl. 1), 37–49. [Google Scholar] [CrossRef] [PubMed]
- Aziz, I.; Törnblom, H.; Simrén, M. Small intestinal bacterial overgrowth as a cause for irritable bowel syndrome: Guilty or not guilty? Curr. Opin. Gastroenterol. 2017, 33, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.C.; Day, L.W.; Somsouk, M.; Sewell, J.L. Meta-analysis: Antibiotic therapy for small intestinal bacterial overgrowth. Aliment. Pharmacol. Ther. 2013, 38, 925–934. [Google Scholar] [CrossRef] [PubMed]
- Enko, D.; Halwachs-Baumann, G.; Stolba, R.; Mangge, H.; Kriegshäuser, G. Refining small intestinal bacterial overgrowth diagnosis by means of carbohydrate specificity: A proof-of-concept study. Ther. Adv. Gastroenterol. 2016, 9, 265–272. [Google Scholar] [CrossRef]
- Rezaie, A.; Pimentel, M.; Rao, S.S. How to Test and Treat Small Intestinal Bacterial Overgrowth: An Evidence-Based Approach. Curr. Gastroenterol. Rep. 2016, 18, 8. [Google Scholar] [CrossRef]
- Ciampa, B.P.; Reyes Ramos, E.; Borum, M.; Doman, D.B. The Emerging Therapeutic Role of Medical Foods for Gastrointestinal Disorders. Gastroenterol. Hepatol. 2017, 13, 104–115. [Google Scholar]
- Pimentel, M.; Constantino, T.; Kong, Y.; Bajwa, M.; Rezaei, A.; Park, S. A 14-day elemental diet is highly effective in normalizing the lactulose breath test. Dig. Dis. Sci. 2004, 49, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Hunter, J. Elemental diet and the nutritional treatment of Crohn’s disease. Gastroenterol. Hepatol. Bed Bench 2015, 8, 4–5. [Google Scholar] [PubMed]
- Logan, A.C.; Beaulne, T.M. The treatment of small intestinal bacterial overgrowth with enteric-coated peppermint oil: A case report. Altern. Med. Rev. 2002, 7, 410–417. [Google Scholar] [PubMed]
- Chedid, V.; Dhalla, S.; Clarke, J.O.; Roland, B.C.; Dunbar, K.B.; Koh, J.; Justino, E.; Tomakin, E.; Mullin, G.E. Herbal therapy is equivalent to rifaximin for the treatment of small intestinal bacterial overgrowth. Glob. Adv. Health Med. 2014, 3, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.; Scott-Hoy, B.; Jennings, L. Efficacy of a Quebracho, Conker Tree, and M. balsamea Willd blended extract in patients with irritable bowel syndrome with constipation. J. Gasterenterol. Hepatol. Res. 2015, 4, 1762–1767. [Google Scholar] [CrossRef]
- Brown, K.; Scott-Hoy, B.; Jennings, L.W. Response of irritable bowel syndrome with constipation patients administered a combined quebracho/conker tree/M. balsamea Willd extract. World J. Gastrointest. Pharmacol. Ther. 2016, 7, 463–468. [Google Scholar] [CrossRef]
- Zhong, C.; Qu, C.; Wang, B.; Liang, S.; Zeng, B. Probiotics for Preventing and Treating Small Intestinal Bacterial Overgrowth: A Meta-Analysis and Systematic Review of Current Evidence. J. Clin. Gastroenterol. 2017, 51, 300–311. [Google Scholar] [CrossRef]
- Khalighi, A.R.; Khalighi, M.R.; Behdani, R.; Jamali, J.; Khosravi, A.; Kouhestani, S.H.; Radmanesh, H.; Esmaeelzadeh, S.; Khalighi, N. Evaluating the efficacy of probiotic on treatment in patients with small intestinal bacterial overgrowth (SIBO)—A pilot study. Indian J. Med. Res. 2014, 140, 604–608. [Google Scholar]
- Poirier, P.; Wawrzyniak, I.; Vivarès, C.P.; Delbac, F.; El Alaoui, H. New insights into Blastocystis spp.: A potential link with irritable bowel syndrome. PLoS Pathog. 2012, 8, e1002545. [Google Scholar] [CrossRef]
- Yakoob, J.; Jafri, W.; Jafri, N.; Khan, R.; Islam, M.; Beg, M.A.; Zaman, V. Irritable bowel syndrome: In search of an etiology: Role of Blastocystis hominis. Am. J. Trop. Med. Hyg. 2004, 70, 383–385. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-González, D.E.; Martínez-Flores, W.A.; Reyes-Gordillo, J.; Ramírez-Miranda, M.E.; Arroyo-Escalante, S.; Romero-Valdovinos, M.; Stark, D.; Souza-Saldivar, V.; Martinez-Hernandez, F.; Flisser, A.; et al. Blastocystis infection is associated with irritable bowel síndrome in a Mexican patient population. Parasitol. Res. 2012, 110, 1269–1275. [Google Scholar] [CrossRef] [PubMed]
- Nourrisson, C.; Scanzi, J.; Pereira, B.; NkoudMongo, C.; Wawrzyniak, I.; Cian, A.; Viscogliosi, E.; Livrelli, V.; Delbac, F.; Dapoigny, M.; et al. Blastocystis is associated with decrease of fecal microbiota protective bacteria: Comparative analysis between patients with irritable bowel syndrome and control subjects. PLoS ONE 2014, 9, e111868. [Google Scholar] [CrossRef] [PubMed]
- Krogsgaard, L.R.; Engsbro, A.L.; Stensvold, C.R.; Nielsen, H.V.; Bytzer, P. The prevalence of intestinal parasites is not greater among individuals with irritable bowel syndrome: A population-based case-control study. Clin. Gastroenterol. Hepatol. 2015, 13, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Ragavan, N.D.; Govind, S.K.; Chye, T.T.; Mahadeva, S. Phenotypic variation in Blastocystis sp. ST3. Parasites Vectors 2014, 7, 404. [Google Scholar] [CrossRef]
- Vargas-Sanchez, G.B.; Romero-Valdovinos, M.; Ramirez-Guerrero, C.; Vargas-Hernandez, I.; Ramirez-Miranda, M.E.; Martinez-Ocaña, J.; Valadez, A.; Ximenez, C.; Lopez-Escamilla, E.; Hernandez-Campos, M.E.; et al. Blastocystis Isolates from Patients with Irritable Bowel Syndrome and from Asymptomatic Carriers Exhibit Similar Parasitological Loads, but Significantly Different Generation Times and Genetic Variability across Multiple Subtypes. PLoS ONE 2015, 10, e0124006. [Google Scholar] [CrossRef] [PubMed]
- Rostami, A.; Riahi, S.M.; Haghighi, A.; Saber, V.; Armon, B.; Seyyedtabaei, S.J. The role of Blastocystis sp. and Dientamoeba fragilis in irritable bowel syndrome: A systematic review and meta-analysis. Parasitol. Res. 2017. [Google Scholar] [CrossRef]
- Coyle, C.M.; Varughese, J.; Weiss, L.M.; Tanowitz, H.B. Blastocystis: To treat or not to treat... Clin. Infect. Dis. 2012, 54, 105–110. [Google Scholar] [CrossRef]
- Stensvold, C.R.; Smith, H.V.; Nagel, R.; Olsen, K.E.; Traub, R.J. Eradication of Blastocystis carriage with antimicrobials: Reality or delusion? J. Clin. Gastroenterol. 2010, 44, 85–90. [Google Scholar] [CrossRef]
- Nagel, R.; Bielefeldt-Ohmann, H.; Traub, R. Clinical pilot study: Efficacy of triple antibiotic therapy in Blastocystis positive irritable bowel syndrome patients. Gut Pathog. 2014, 6, 34. [Google Scholar] [CrossRef]
- Force, M.; Sparks, W.S.; Ronzio, R.A. Inhibition of enteric parasites by emulsified oil of oregano in vivo. Phytother. Res. 2000, 14, 213–214. [Google Scholar] [CrossRef]
- Dinleyici, E.C.; Eren, M.; Dogan, N.; Reyhanioglu, S.; Yargic, Z.A.; Vandenplas, Y. Clinical efficacy of Saccharomyces boulardii or metronidazole in symptomatic nchildren with Blastocystis hominis infection. Parasitol. Res. 2011, 108, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Shariati, A.; Fallah, F.; Pormohammad, A.; Taghipour, A.; Safari, H.; Chirani, A.S.; Sabour, S.; Alizadeh-Sani, M.; Azimi, T. The possible role of bacteria, viruses, and parasites in initiation and exacerbation of irritable bowel syndrome. J. Cell. Physiol. 2019, 234, 8550–8569. [Google Scholar] [CrossRef] [PubMed]
- Lagacé-Wiens, P.R.; VanCaeseele, P.G.; Koschik, C. Dientamoeba fragilis: An emerging role in intestinal disease. CMAJ 2006, 175, 468–469. [Google Scholar] [CrossRef] [PubMed]
- Borody, T.; Warren, A.; Wettstein, G.; Robertson, G.; Recabarren, P.; Fontela, A.; Herdman, K.; Surace, R. Eradication of Dientamoeba fragilis can resolve IBS-like symptoms. J. Gastroenterol. Hepatol. 2002, 17, A103. [Google Scholar]
- Ali, S.; Khetpal, N.; Khan, M.T.; Rasheed, M.; Asad-Ur-Rahman, F.; Echeverria-Beltran, K. A Mexican Honeymoon Marred by Gastrointestinal Upset: A Case of Dientamoeba fragilis Causing Post-infectious Irritable Bowel Syndrome. Cureus 2017, 9, e1992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engsbro, A.L.; Stensvold, C.R.; Nielsen, H.V.; Bytzer, P. Treatment of Dientamoeba fragilis in patients with irritable bowel syndrome. Am. J. Trop. Med. Hyg. 2012, 87, 1046–1052. [Google Scholar] [CrossRef]
- Stark, D.; Barratt, J.; Chan, D.; Ellis, J.T. Dientamoeba fragilis, the Neglected Trichomonad of the Human Bowel. Clin. Microbiol. Rev. 2016, 29, 553–580. [Google Scholar] [CrossRef] [Green Version]
- Hsu, C.S.; Liu, T.T.; Wen, S.H.; Wang, C.C.; Yi, C.H.; Chen, J.H.; Lei, W.Y.; Orr, W.C.; Fabio, P.; Chen, C.L. Clinical, metabolic, and psychological characteristics in patients with gastroesophageal reflux disease overlap with irritable bowel syndrome. Eur. J. Gastroenterol. Hepatol. 2015, 27, 516–522. [Google Scholar] [CrossRef]
- De Bortoli, N.; Tolone, S.; Frazzoni, M.; Martinucci, I.; Sgherri, G.; Albano, E.; Ceccarelli, L.; Stasi, C.; Bellini, M.; Savarino, V.; et al. Gastroesophageal reflux disease, functional dyspepsia and irritable bowel syndrome: Common overlapping gastrointestinal disorders. Ann. Gastroenterol. 2018, 31, 639–648. [Google Scholar] [CrossRef]
- Kountouras, J.; Doulberis, M.; Papaefthimiou, A.; Polyzos, S.A. Gastroesophageal reflux disease, irritable bowel syndrome and functional dyspepsia as overlapping conditions: Focus on effect of trimebutine. Ann. Gastroenterol. 2019, 32, 318. [Google Scholar] [CrossRef] [PubMed]
- Davis, S. Reversal of Irritable Bowel Syndrome, Sleep Disturbance, and Fatigue with an Elimination Diet, Lifestyle Modification, and Dietary Supplements: A Case Report. Integr. Med. Encinitas 2016, 15, 60–66. [Google Scholar] [PubMed]
Figure 1.
Underlying causes of irritable bowel symptoms.
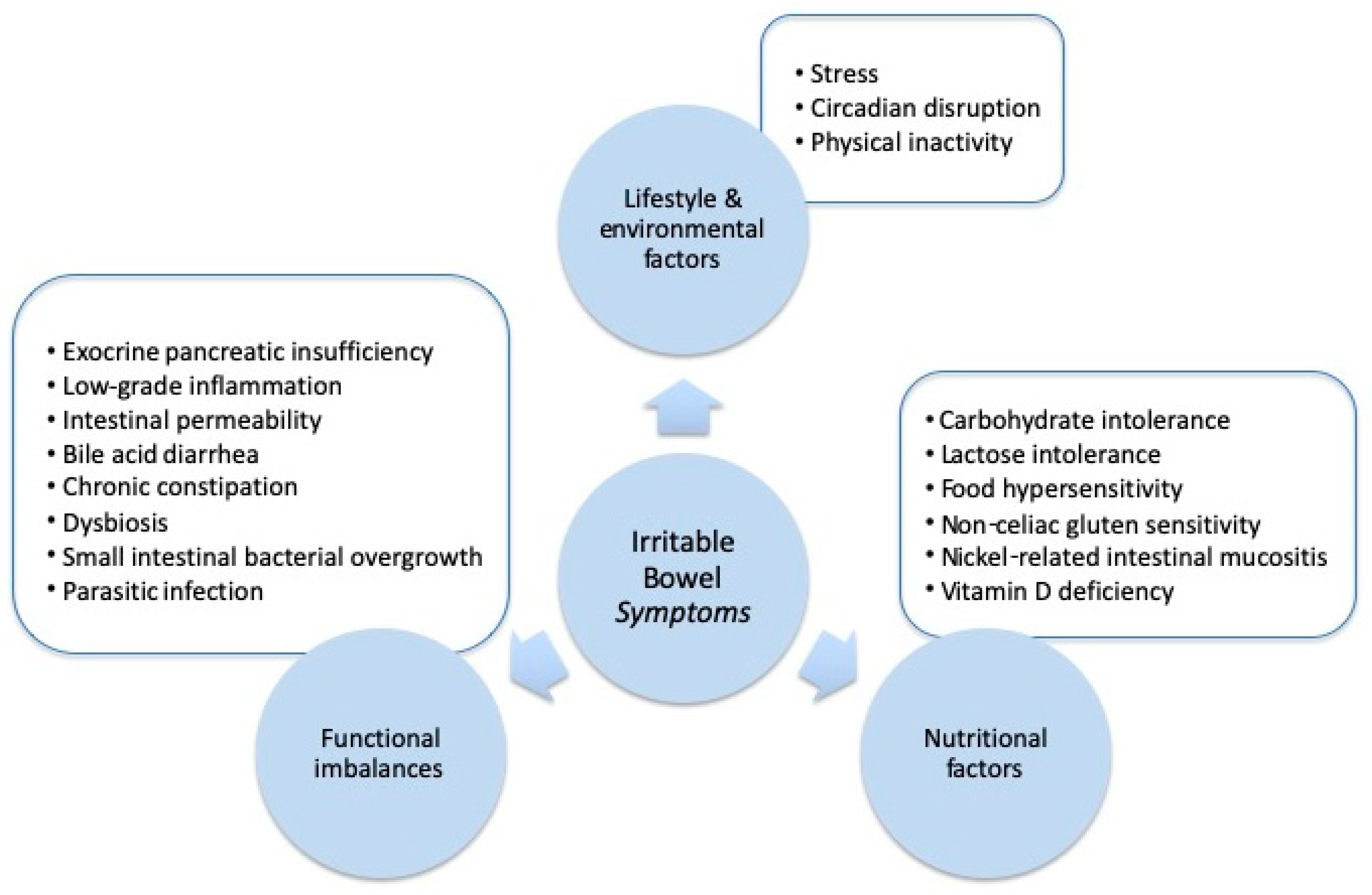

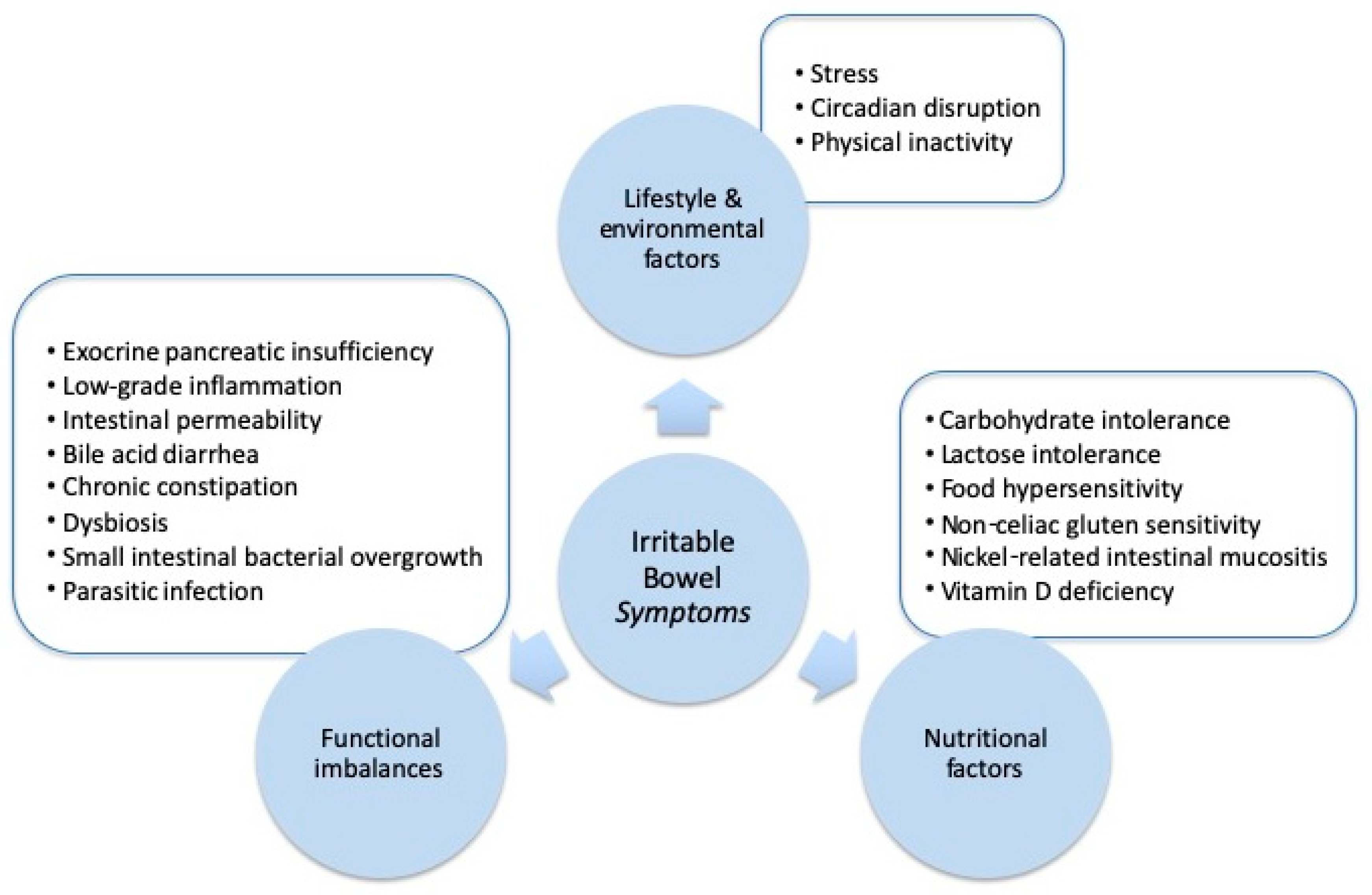{kind=link}
Table 1.
Summary of factors that may explain irritable bowel symptoms.
| Contributing Factor | Mechanisms | Clinical and Biochemical Investigations | Potential Management and Treatment Approaches |
|---|---|---|---|
| Stress | Dysregulation of the brain–gut axis can influence the main pathophysiological features of IBS, including visceral hypersensitivity, colonic motility and alterations in the gut microbiota. | Clinical symptom severity. Salivary diurnal and/or waking cortisol. Serum neuropeptide Y. Serotonin transporter gene variants. Catechol-O-methyltransferase Val158Met gene variants. | Mind–body therapies. Cognitive behavioral therapy. Hypnotherapy. Educational interventions. |
| Circadian disruption | Circadian rhythm disruption can affect several aspects of gastrointestinal function including gastrointestinal motility, visceral sensitivity, immunological function, and barrier integrity. | Questioning around sleep patterns and electric light-at-night exposure. Salivary melatonin. | Extending the dark period. Regular sleep patterns. |
| Physical inactivity | Clinical studies have found that increasing physical activity can improve gastric emptying, intestinal gas transit and reduce abdominal distension. | Tracking physical activity levels. Activity tracker step count. | Exercise counselling. Yoga. Walking. |
| Carbohydrate intolerance | Fermentable carbohydrates may increase osmotic load and gas production in the distal small bowel and the proximal colon. | Breath testing for lactose and fructose intolerance. Breath testing for small intestinal bacterial overgrowth. Genetic testing for sucrase-isomaltase gene variants. | Reduce intake of refined sugar and carbohydrates. Low FODMAP diet. |
| Lactose intolerance | Unabsorbed lactose in the intestine can increase osmotic load and intestinal water content in addition to undergoing fermentation to produce short chain fatty acids and gas including hydrogen and methane, which may cause or aggravate symptoms in susceptible individuals. | Positive test of lactose malabsorption (genetic, biopsy, or H2-breath test) and subsequent open-label lactose challenge. | Lactase enzyme therapy. Low-lactose or lactose-free diet. |
| Food hypersensitivity | Immunologically mediated food hypersensitivity may play a role in the development of gastrointestinal symptoms via a local and limited IgE-mediated reaction in the intestinal mucosa and/or IgE-independent mechanisms. | Dietary elimination and re-challenge. IgG antibodies to foods. | Elimination and re-challenge diet. IgG antibody-guided exclusion diet. |
| Non-celiac gluten sensitivity | People with NCGS have evidence of immune activation (measured with increased serum levels of soluble CD14), leaky gut (lipopolysaccharide-binding protein and antibody reactivity to bacterial LPS and flagellin) and intestinal damage (fatty acid-binding protein 2). | Clinical rating scale, response to a gluten-free diet, and double-placebo controlled gluten challenge. HLA-DQ2/8 gene variants. | Gluten-free diet. |
| Nickel-related intestinal mucositis | In nickel sensitive people, exposure results in elevated levels of IFNy, IL-5, and IL-13 in the supernatants of peripheral blood mononuclear cell cultures stimulated with nickel, suggesting a pro-inflammatory effect. | Positive nickel patch test. | Low nickel diet. |
| Vitamin D deficiency | Vitamin D deficiency could contribute to mucosal inflammation, impaired epithelial cell integrity, and the alterations in the composition of the gut microbiome. | Serum 25-hydroxy vitamin D. | Sunlight exposure. Vitamin D3 supplementation. |
| Exocrine pancreatic insufficiency | Impaired digestion of food may increase antigenic load and/or contribute to postprandial osmotic diarrhoea. | Clinical symptoms of postprandial osmotic diarrhoea, or galacto-oligosaccharide intolerance. Fecal elastase-1 (FE-1). | Digestive enzyme therapy. |
| Low-grade inflammation | Low-grade intestinal inflammation contributes to altered permeability, hypersensitivity of enteric nerves and changes in serotonin signaling. | Fecal calprotectin. | Low antigenic/elimination diet. Anti-inflammatory diet. Anti-inflammatory herbal medicines, such as Boswellia serrata. |
| Intestinal permeability | Intestinal permeability contributes to low-grade intestinal inflammation and increased visceral and pain sensitivity. | Intestinal permeability (lactulose/mannitol). Serum lipopolysaccharide binding protein. | Probiotics. Glutamine. |
| Bile acid malabsorption | An increase in the fecal excretion and change in the proportion of the various bile acids in stool contributes to intestinal permeability, water and electrolyte secretion, and increased colonic transit. | Therapeutic trial of bile acid binders. Serum 7α-hydroxy-4-cholesten-3-one. Selenium homotaurocholic acid test. KLB rs17618244 and GPBAR1rs11554825 gene variants. | Bile acid binders. Pancreatic enzyme therapy. Diet that minimizes bile acid production and/or excretion. Probiotics. Prebiotics. |
| Chronic constipation | Functional constipation is associated with visceral sensitivity and alterations in serotonin signaling. | The Bristol Stool Scale. | Laxatives. Fiber therapy. |
| Dysbiosis | Alterations in the gastrointestinal microbiota activate mucosal innate immune responses which increase epithelial permeability, initiate nociceptive sensory pathways and dysregulate the enteric nervous system. | Comprehensive stool microbiology. Breath testing for small intestinal bacterial overgrowth. | Gut-microbiota-targeted dietary interventions. Probiotics. Prebiotics. |
| Small intestinal bacterial overgrowth | Colonic gram-negative aerobes and anaerobic species overgrow in the small intestine where they ferment carbohydrate and contribute to digestive symptoms. | Breath testing for small intestinal bacterial overgrowth. | Antibiotics. Medical food-based elemental diet. Herbal medicine. Probiotics. |
| Parasitic infection or overgrowth | Specific subtypes of Blastocystis species may contribute to dysbiosis, upregulate pro-inflammatory cytokines, and degrade tight junction proteins and increase intestinal permeability. D. fragilis-infection may result in inflammatory changes and intestinal permeability in the gut mucosa. | Comprehensive stool parasitology, including Blastocystis species and D. fragilis. | Antibiotic therapy. Emulsified oil of Oregano. Saccharomyces boulardii. |
© 2019 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Brown, B.I. Does Irritable Bowel Syndrome Exist? Identifiable and Treatable Causes of Associated Symptoms Suggest It May Not. Gastrointest. Disord. 2019, 1, 314-340. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord1030027
AMA Style
Brown BI. Does Irritable Bowel Syndrome Exist? Identifiable and Treatable Causes of Associated Symptoms Suggest It May Not. Gastrointestinal Disorders. 2019; 1(3):314-340. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord1030027
Chicago/Turabian StyleBrown, Benjamin I. 2019. "Does Irritable Bowel Syndrome Exist? Identifiable and Treatable Causes of Associated Symptoms Suggest It May Not" Gastrointestinal Disorders 1, no. 3: 314-340. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord1030027