Cytomorphological Characterization of Individual Metastatic Tumor Cells from Gastrointestinal Cancer Patient Lymph Nodes with Imaging Flow Cytometry


Abstract
:1. Introduction
2. Materials and Methods
2.1. Spiking Experiments
2.2. Human Lymph Node
2.3. Tissue Dissociation
2.4. Immunofluorescent Cellular Staining
2.5. Imaging Flow Cytometry
3. Results
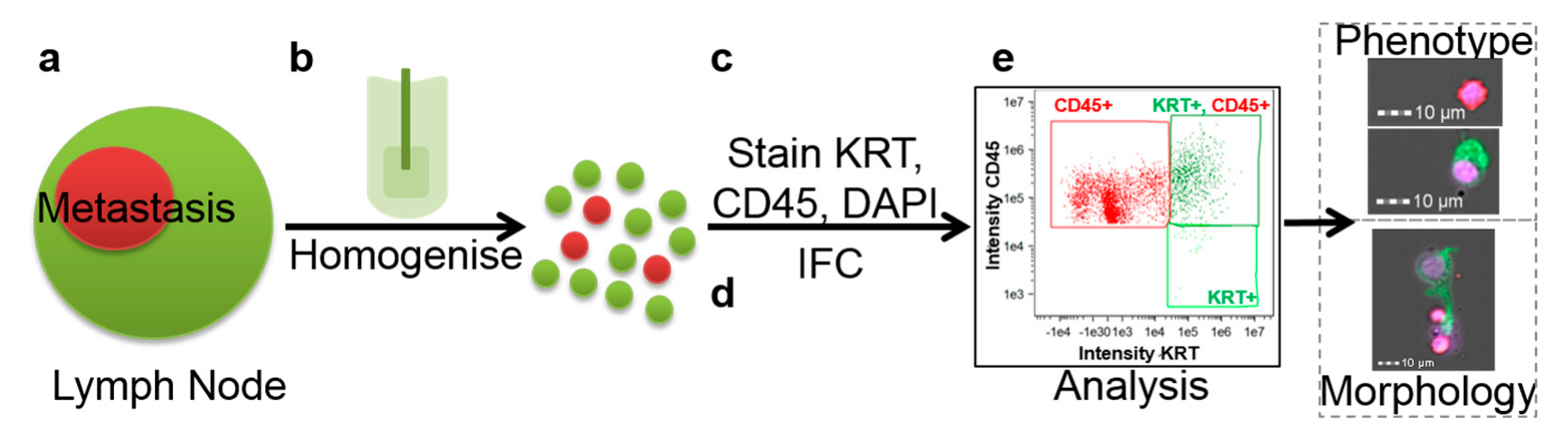
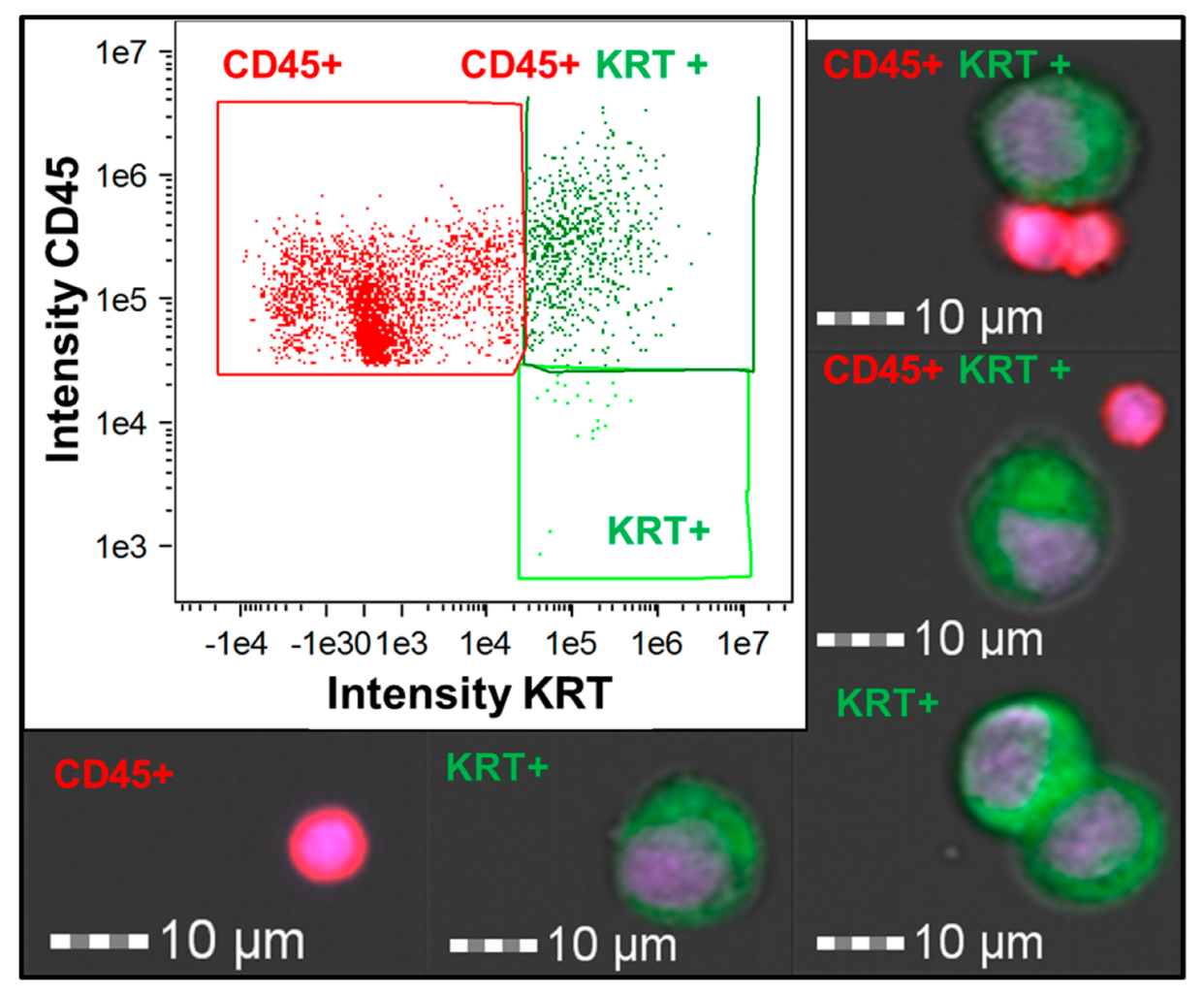
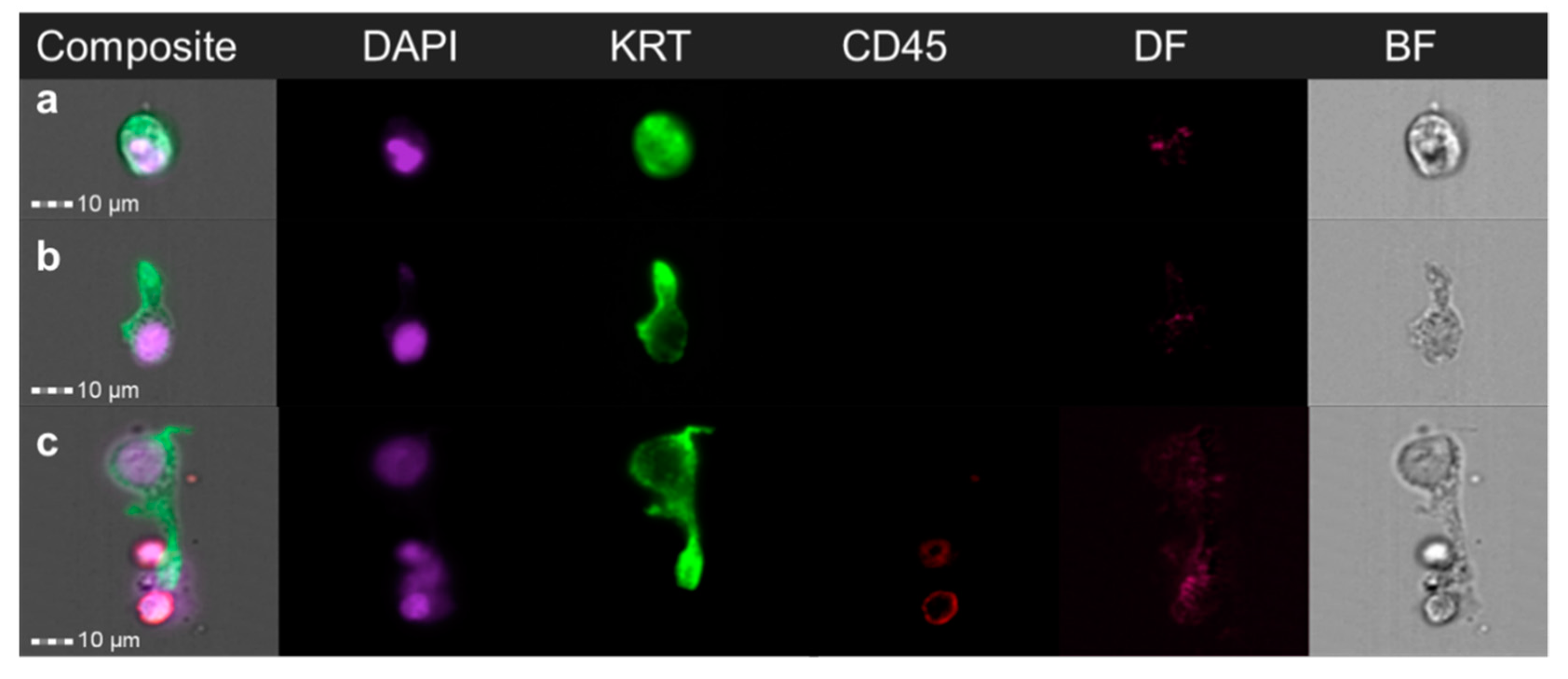
3.1. Identification and Characterization of Cancer Cells in a Lymph Node Spiking Model
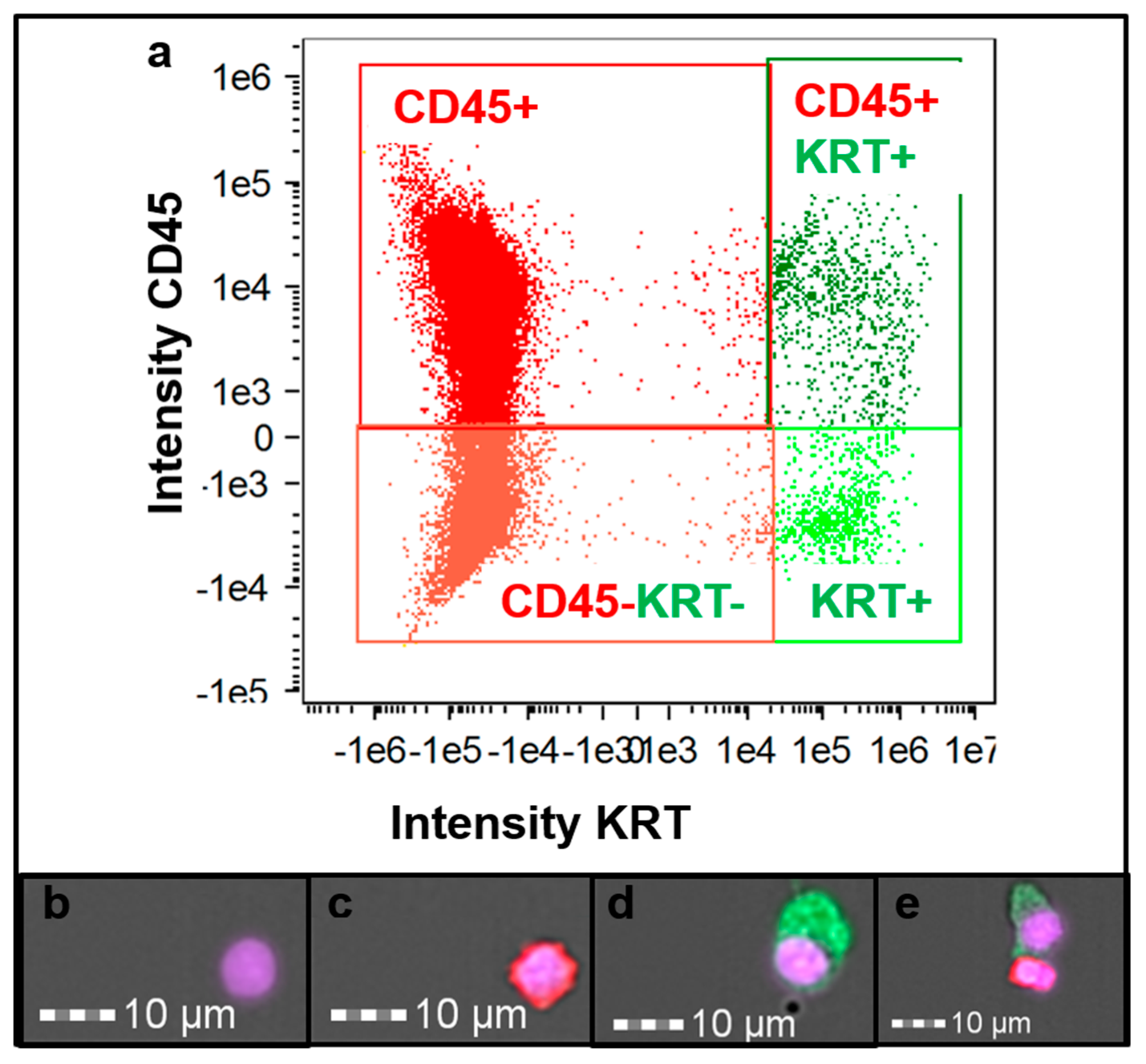
3.2. Cancer Patient Lymph Node Analysis
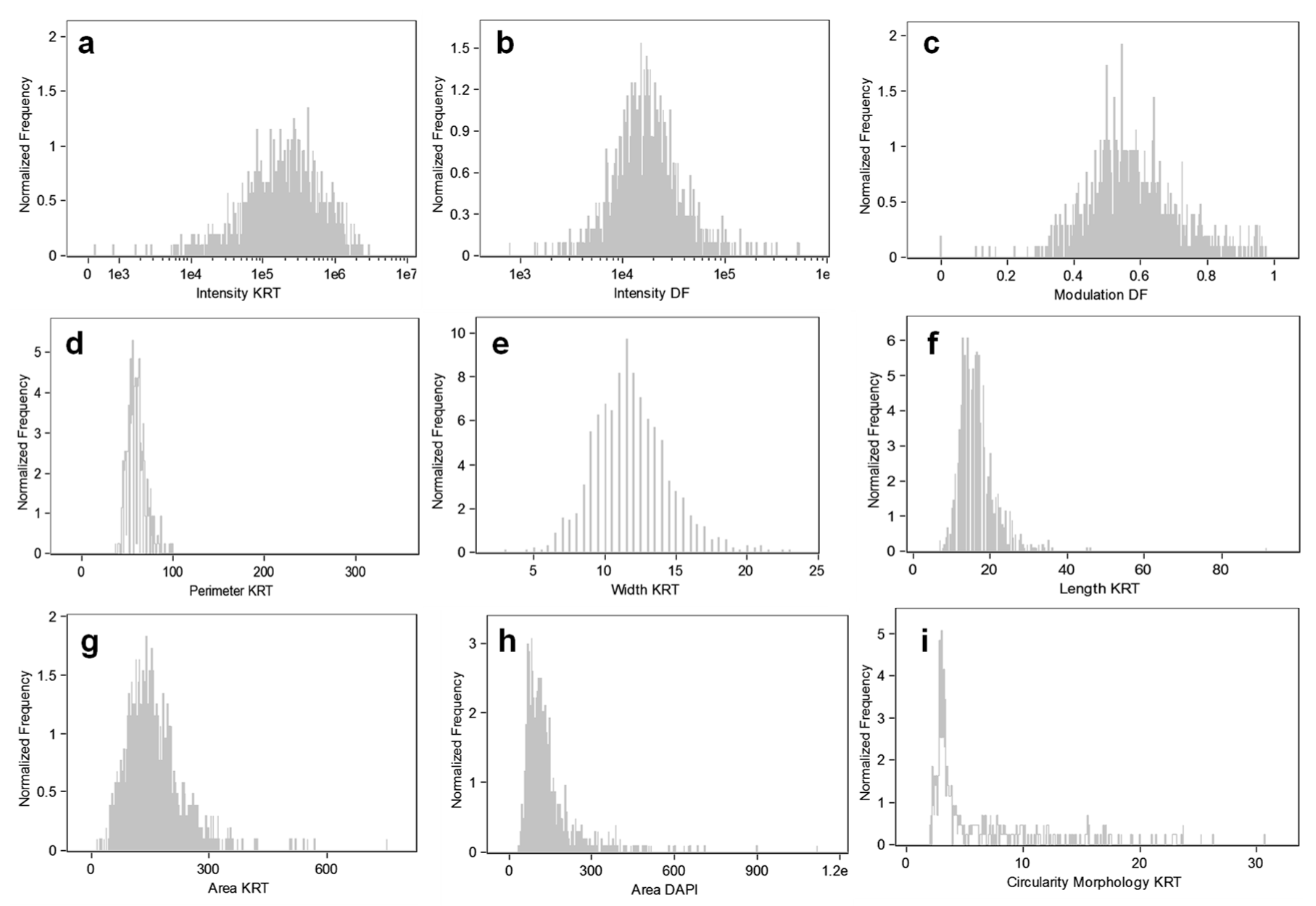
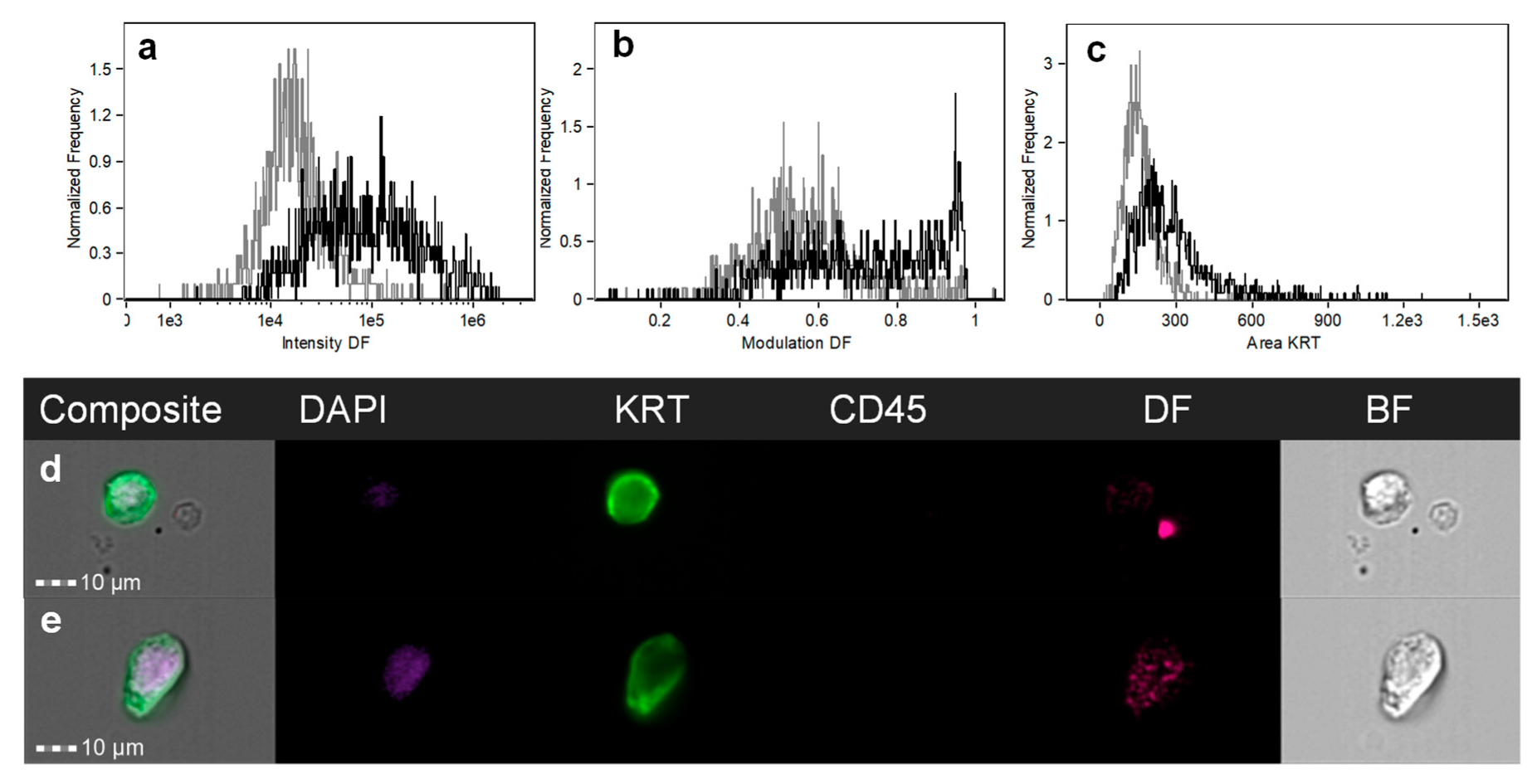
3.3. Tumor Cell Cytomorphological Characterization
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Edge, S.; Byrd, D.; Compton, C.; Fritz, A.; Greene, F.; Trotti, A., III. AJCC Cancer Staging Manual, 7th ed.; Springer: New York, NY, USA, 2010. [Google Scholar]
- Estrada, O.; Pulido, L.; Admella, C.; Hidalgo, L.-A.; Clavé, P.; Sunol, X. Sentinel lymph node biopsy as a prognostic factor in non-metastatic colon cancer: A prospective study. Clin. Transl. Oncol. 2016, 19, 432–439. [Google Scholar] [CrossRef] [PubMed]
- Arigami, T.; Uenosono, Y.; Yanagita, S.; Nakajo, A.; Ishigami, S.; Okumura, H.; Kijima, Y.; Ueno, S.; Natsugoe, S. Clinical significance of lymph node micrometastasis in gastric cancer. Ann. Surg. Oncol. 2012, 20, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.L.; Hoehne, F.M.; Giuliano, A.E. The prognostic significance of micrometastases in breast cancer: A seer population-based analysis. Ann. Surg. Oncol. 2007, 14, 3378–3384. [Google Scholar] [CrossRef] [PubMed]
- Patani, N.; Mokbel, K. Clinical significance of sentinel lymph node isolated tumour cells in breast cancer. Breast Cancer Res. Treat. 2011, 127, 325–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.; Mittendorf, E.A.; Kelten, C.; Tucker, S.L.; Wei, W.; Middleton, L.P.; Broglio, K.; Buchholz, T.A.; Hunt, K.K.; Sahin, A.A. Occult axillary lymph node metastasis do not have prognostic significance in early stage breast cancer. Cancer 2011, 118, 1507–1514. [Google Scholar] [CrossRef] [PubMed]
- Murali, R.; DeSilva, C.; McCarthy, S.W.; Thompson, J.F.; Scolyer, R.A. Sentinel lymph nodes containing very small (<0.1 mm) deposits of metastatic melanoma cannot be safely regarded as tumor-negative. Ann. Surg. Oncol. 2012, 19, 1089–1099. [Google Scholar] [PubMed]
- Naidoo, K.; Pinder, S.E. Micro-and macro-metastasis in the axillary lymph node: A review. Surgeon 2016, 15, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, A.E.; McCall, L.; Beitsch, P.; Whitworth, P.W.; Blumencranz, P.; Leitch, A.M.; Saha, S.; Hunt, K.K.; Morrow, M.; Ballman, K. Locoregional recurrence after sentinel lymph node dissection with or without axillary dissection in patients with sentinel lymph node metastases: The american college of surgeons oncology group z0011 randomized trial. Ann. Surg. 2010, 252, 426–433. [Google Scholar] [CrossRef]
- Briganti, A.; Passoni, N.M.; Abdollah, F.; Nini, A.; Montorsi, F.; Karnes, R.J. Treatment of lymph node–positive prostate cancer: Teaching old dogmas new tricks. Eur. Urol. 2014, 65, 26–28. [Google Scholar] [CrossRef] [PubMed]
- Winter, M.; Gibson, R.; Ruszkiewicz, A.; Thompson, S.K.; Thierry, B. Beyond conventional pathology: Towards preoperative and intraoperative lymph node staging. Int. J. Cancer 2015, 136, 743–751. [Google Scholar] [CrossRef]
- Grabau, D.; Ryden, L.; Fernö, M.; Ingvar, C. Analysis of sentinel node biopsy—A single-institution experience supporting the use of serial sectioning and immunohistochemistry for detection of micrometastases by comparing four different histopathological laboratory protocols. Histopathology 2011, 59, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Cristofanilli, M.; Hayes, D.F.; Budd, G.T.; Ellis, M.J.; Stopeck, A.; Reuben, J.M.; Doyle, G.V.; Matera, J.; Allard, W.J.; Miller, M.C. Circulating tumor cells: A novel prognostic factor for newly diagnosed metastatic breast cancer. J. Clin. Oncol. 2005, 23, 1420–1430. [Google Scholar] [CrossRef] [PubMed]
- Pilati, P.; Mocellin, S.; Bertazza, L.; Galdi, F.; Briarava, M.; Mammano, E.; Tessari, E.; Zavagno, G.; Nitti, D. Prognostic value of putative circulating cancer stem cells in patients undergoing hepatic resection for colorectal liver metastasis. Ann. Surg. Oncol. 2012, 19, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Banyard, J.; Bielenberg, D.R. The role of emt and met in cancer dissemination. Connect. Tissue Res. 2015, 56, 403–413. [Google Scholar] [CrossRef] [PubMed]
- Haber, D.A.; Velculescu, V.E. Blood-based analyses of cancer: Circulating tumor cells and circulating tumor DNA. Cancer Discov. 2014, 4, 650–661. [Google Scholar] [CrossRef]
- Ligthart, S.T.; Coumans, F.A.; Bidard, F.-C.; Simkens, L.H.; Punt, C.J.; de Groot, M.R.; Attard, G.; de Bono, J.S.; Pierga, J.-Y.; Terstappen, L.W. Circulating tumor cells count and morphological features in breast, colorectal and prostate cancer. PLoS ONE 2013, 8, e67148. [Google Scholar] [CrossRef]
- Marrinucci, D.; Bethel, K.; Bruce, R.H.; Curry, D.N.; Hsieh, B.; Humphrey, M.; Krivacic, R.T.; Kroener, J.; Kroener, L.; Ladanyi, A. Case study of the morphologic variation of circulating tumor cells. Hum. Pathol. 2007, 38, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Marrinucci, D.; Bethel, K.; Lazar, D.; Fisher, J.; Huynh, E.; Clark, P.; Bruce, R.; Nieva, J.; Kuhn, P. Cytomorphology of circulating colorectal tumor cells: A small case series. J. Oncol. 2010, 2010, 861341. [Google Scholar] [CrossRef]
- Park, S.; Ang, R.R.; Duffy, S.P.; Bazov, J.; Chi, K.N.; Black, P.C.; Ma, H. Morphological differences between circulating tumor cells from prostate cancer patients and cultured prostate cancer cells. PLoS ONE 2014, 9, e85264. [Google Scholar] [CrossRef]
- Vona, G.; Estepa, L.; Béroud, C.; Damotte, D.; Capron, F.; Nalpas, B.; Mineur, A.; Franco, D.; Lacour, B.; Pol, S. Impact of cytomorphological detection of circulating tumor cells in patients with liver cancer. Hepatology 2004, 39, 792–797. [Google Scholar] [CrossRef]
- Headland, S.E.; Jones, H.R.; D’Sa, A.S.; Perretti, M.; Norling, L.V. Cutting-edge analysis of extracellular microparticles using imagestreamx imaging flow cytometry. Sci. Rep. 2014, 4, 5237. [Google Scholar] [CrossRef] [PubMed]
- Basiji, D.; O’Gorman, M. Imaging flow cytometry. J. Immunol. Methods 2015, 423, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Goda, K.; Ayazi, A.; Gossett, D.R.; Sadasivam, J.; Lonappan, C.K.; Sollier, E.; Fard, A.M.; Hur, S.C.; Adam, J.; Murray, C. High-throughput single-microparticle imaging flow analyzer. Proc. Natl. Acad. Sci. USA 2012, 109, 11630–11635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reyes, E.E.; VanderWeele, D.J.; Isikbay, M.; Duggan, R.; Campanile, A.; Stadler, W.M.; Vander Griend, D.J.; Szmulewitz, R.Z. Quantitative characterization of androgen receptor protein expression and cellular localization in circulating tumor cells from patients with metastatic castration-resistant prostate cancer. J. Transl. Med. 2014, 12, 313. [Google Scholar] [CrossRef] [PubMed]
- Doan, M.; Vorobjev, I.; Rees, P.; Filby, A.; Wolkenhauer, O.; Goldfeld, A.E.; Lieberman, J.; Barteneva, N.; Carpenter, A.E.; Hennig, H. Diagnostic potential of imaging flow cytometry. Trends Biotechnol. 2018, 36, 649–652. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Winter, M.; Thierry, B. Quasi-spherical microwells on superhydrophobic substrates for long term culture of multicellular spheroids and high throughput assays. Biomaterials 2014, 35, 6060–6068. [Google Scholar] [CrossRef]
- Hennig, H.; Rees, P.; Blasi, T.; Kamentsky, L.; Hung, J.; Dao, D.; Carpenter, A.E.; Filby, A. An open-source solution for advanced imaging flow cytometry data analysis using machine learning. Methods 2017, 112, 201–210. [Google Scholar] [CrossRef]
- Ito, M.; Minamiya, Y.; Kawai, H.; Saito, S.; Saito, H.; Imai, K.; Ogawa, J.-I. Intraoperative detection of lymph node micrometastasis with flow cytometry in non–small cell lung cancer. J. Thorac. Cardiovasc. Surg. 2005, 130, 753–758. [Google Scholar] [CrossRef]
- Leers, M.; Schoffelen, R.; Hoop, J.; Theunissen, P.; Oosterhuis, J.; Rahmy, A.; Tan, W.; Nap, M. Multiparameter flow cytometry as a tool for the detection of micrometastatic tumour cells in the sentinel lymph node procedure of patients with breast cancer. J. Clin. Pathol. 2002, 55, 359–366. [Google Scholar] [CrossRef] [Green Version]
- Hartana, C.A.; Kinn, J.; Rosenblatt, R.; Anania, S.; Alamdari, F.; Glise, H.; Sherif, A.; Winqvist, O. Detection of micrometastases by flow cytometry in sentinel lymph nodes from patients with renal tumours. Br. J. Cancer 2016, 115, 957–966. [Google Scholar] [CrossRef] [Green Version]
- Häyry, V.; Kågedal, Å.; Hjalmarsson, E.; da Silva, P.F.N.; Drakskog, C.; Margolin, G.; Georén, S.K.; Munck-Wikland, E.; Winqvist, O.; Cardell, L.O. Rapid nodal staging of head and neck cancer surgical specimens with flow cytometric analysis. Br. J. Cancer 2018, 118, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Jagric, T.; Mis, K.; Gorenjak, M.; Goropevsek, A.; Kavalar, R.; Mars, T. Can flow cytometry reinvent the sentinel lymph node concept in gastric cancer patients? J. Surg. Res. 2018, 223, 46–57. [Google Scholar] [CrossRef] [PubMed]
- Friedl, P.; Wolf, K. Tumour-cell invasion and migration: Diversity and escape mechanisms. Nat. Rev. Cancer 2003, 3, 362–374. [Google Scholar] [CrossRef]
- Kevans, D.; Wang, L.M.; Sheahan, K.; Hyland, J.; O’Donoghue, D.; Mulcahy, H.; O’Sullivan, J. Epithelial-mesenchymal transition (emt) protein expression in a cohort of stage ii colorectal cancer patients with characterized tumor budding and mismatch repair protein status. Int. J. Surg. Pathol. 2011, 19, 751–760. [Google Scholar] [CrossRef] [PubMed]
- Palmieri, V.; Lucchetti, D.; Maiorana, A.; Papi, M.; Maulucci, G.; Calapà, F.; Ciasca, G.; Giordano, R.; Sgambato, A.; De Spirito, M. Mechanical and structural comparison between primary tumor and lymph node metastases cells in colorectal cancer. Soft Matter 2015, 11, 5719–5726. [Google Scholar] [CrossRef] [PubMed]
- Margheri, F.; Luciani, C.; Taddei, M.L.; Giannoni, E.; Laurenzana, A.; Biagioni, A.; Chillà, A.; Chiarugi, P.; Fibbi, G.; Del Rosso, M. The receptor for urokinase-plasminogen activator (upar) controls plasticity of cancer cell movement in mesenchymal and amoeboid migration style. Oncotarget 2014, 5, 1538–1553. [Google Scholar] [CrossRef]
- Wakamatsu, Y.; Sakamoto, N.; Oo, H.Z.; Naito, Y.; Uraoka, N.; Anami, K.; Sentani, K.; Oue, N.; Yasui, W. Expression of cancer stem cell markers aldh1, cd44 and cd133 in primary tumor and lymph node metastasis of gastric cancer. Pathol. Int. 2012, 62, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Takes, R.P.; de Jong, B.; Robert, J.; Wijffels, K.; Schuuring, E.; Litvinov, S.V.; Hermans, J.; van Krieken, H.J. Expression of genetic markers in lymph node metastases compared with their primary tumours in head and neck cancer. J. Pathol. 2001, 194, 298–302. [Google Scholar] [CrossRef]
- Nishizaki, T.; DeVries, S.; Chew, K.; Goodson, W.H.; Ljung, B.-M.; Thor, A.; Waldman, F.M. Genetic alterations in primary breast cancers and their metastases: Direct comparison using modified comparative genomic hybridization. Genes Chromosomes Cancer 1997, 19, 267–272. [Google Scholar] [CrossRef]
- Takahashi, R.; Nagayama, S.; Furu, M.; Kajita, Y.; Jin, Y.; Kato, T.; Imoto, S.; Sakai, Y.; Toguchida, J. Afap1l1, a novel associating partner with vinculin, modulates cellular morphology and motility, and promotes the progression of colorectal cancers. Cancer Med. 2014, 3, 759–774. [Google Scholar] [CrossRef]
- Riethdorf, S.; Wikman, H.; Pantel, K. Review: Biological relevance of disseminated tumor cells in cancer patients. Int. J. Cancer 2008, 123, 1991–2006. [Google Scholar] [CrossRef] [PubMed]
- Resetkova, E.; Hoda, S.A.; Clarke, J.L.; Rosen, P.P. Benign heterotopic epithelial inclusions in axillary lymph nodes. Arch. Pathol. Lab. Med. 2003, 127, e25–e27. [Google Scholar] [PubMed]
- Dunphy, C.H. Pitfalls of frozen section to intraoperative consultations of evaluating lymph nodes for involvement by metastatic malignancies: Benign processes mimicking metastatic carcinoma. In Frozen Section Library: Lymph Nodes; Springer: Berlin/Heidelberg, Germany, 2012; pp. 95–119. [Google Scholar]
- Rao, R.S.; Taylor, J.; Palmer, J.; Jennings, W.C. Breast cancer pseudometastasis in a sentinel lymph node with cytokeratin-positive debris. Breast J. 2005, 11, 134–137. [Google Scholar] [CrossRef] [PubMed]
- Maiorano, E.; Mazzarol, G.M.; Pruneri, G.; Mastropasqua, M.G.; Zurrida, S.; Orvieto, E.; Viale, G. Ectopic breast tissue as a possible cause of false-positive axillary sentinel lymph node biopsies. Am. J. Surg. Pathol. 2003, 27, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Fellegara, G.; Carcangiu, M.L.; Rosai, J. Benign epithelial inclusions in axillary lymph nodes: Report of 18 cases and review of the literature. Am. J. Surg. Pathol. 2011, 35, 1123–1133. [Google Scholar] [CrossRef] [PubMed]
- Bernet, L.; Cano, R.; Martinez, M.; Dueñas, B.; Matias-Guiu, X.; Morell, L.; Palacios, J.; Rezola, R.; Robles-Frias, M.; Ruiz, I. Diagnosis of the sentinel lymph node in breast cancer: A reproducible molecular method: A multicentric spanish study. Histopathology 2011, 58, 863–869. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | 1 | 2 | 3 |
|---|---|---|---|
| Age | 55 | 64 | 67 |
| Gender | F | M | F |
| Primary Tumor Site | Stomach | Sigmoid Colon | Gall Bladder |
| Positive Nodes | 29 | 0 | 0 |
| Stage | pT3pN3bcM1 Clinical Stage (AJCC) IV | pT2pN0cM0 Clinical Stage (AJCC) I | pT3pN0cM1 Clinical Stage (AJCC) IVB |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Winter, M.; Gibson, R.; Ruszkiewicz, A.; Thierry, B. Cytomorphological Characterization of Individual Metastatic Tumor Cells from Gastrointestinal Cancer Patient Lymph Nodes with Imaging Flow Cytometry. Gastrointest. Disord. 2019, 1, 372-384. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord1040030
Winter M, Gibson R, Ruszkiewicz A, Thierry B. Cytomorphological Characterization of Individual Metastatic Tumor Cells from Gastrointestinal Cancer Patient Lymph Nodes with Imaging Flow Cytometry. Gastrointestinal Disorders. 2019; 1(4):372-384. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord1040030
Chicago/Turabian StyleWinter, Marnie, Rachel Gibson, Andrew Ruszkiewicz, and Benjamin Thierry. 2019. "Cytomorphological Characterization of Individual Metastatic Tumor Cells from Gastrointestinal Cancer Patient Lymph Nodes with Imaging Flow Cytometry" Gastrointestinal Disorders 1, no. 4: 372-384. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord1040030