Quality of Life and Eligibility for Specific Financial Assistance for Medical Expenses: A Cross-Sectional Web-Based Survey among Patients with Inflammatory Bowel Disease in Japan

Abstract
:1. Introduction
2. Results
2.1. The Status of Specific Financial Assistance
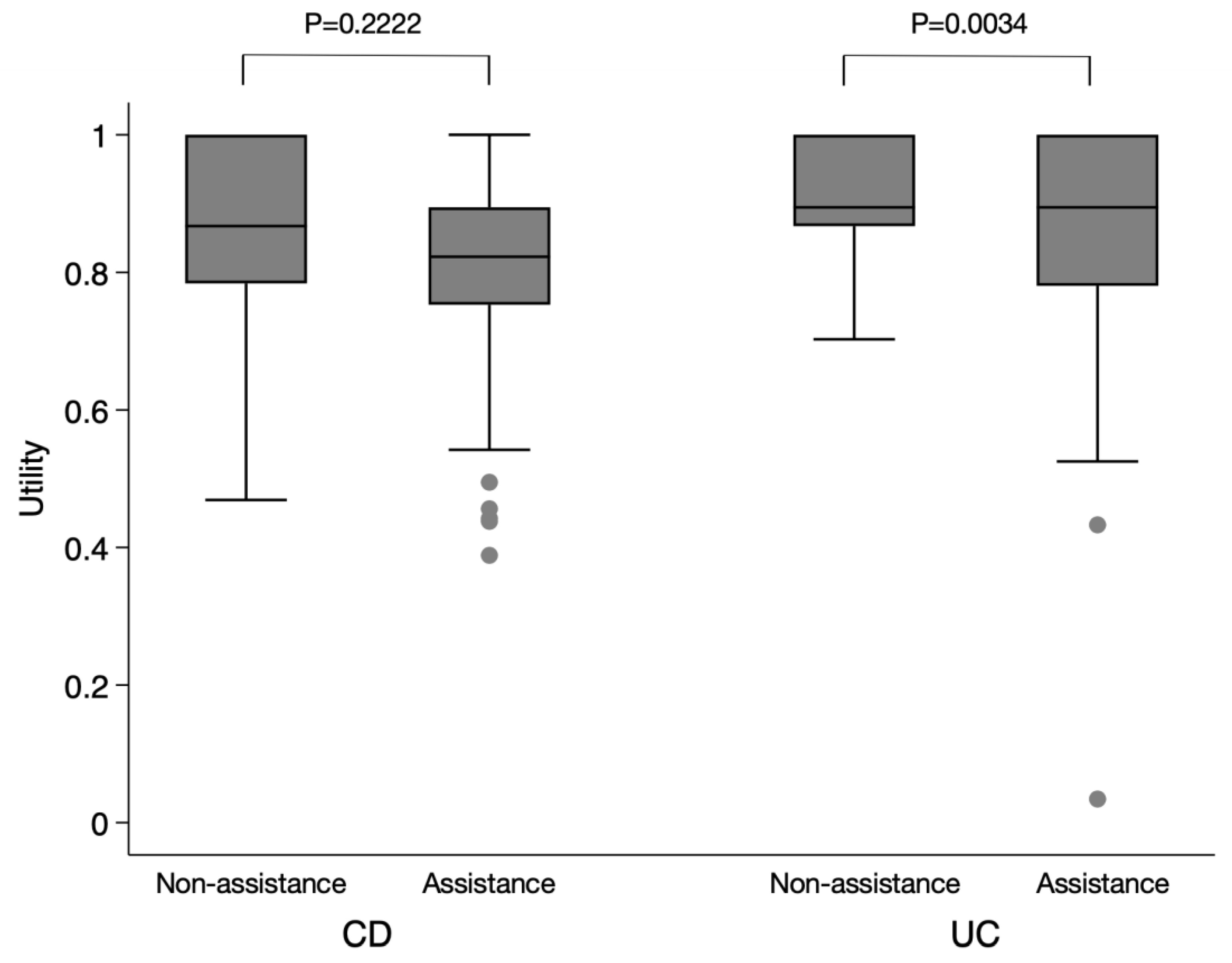
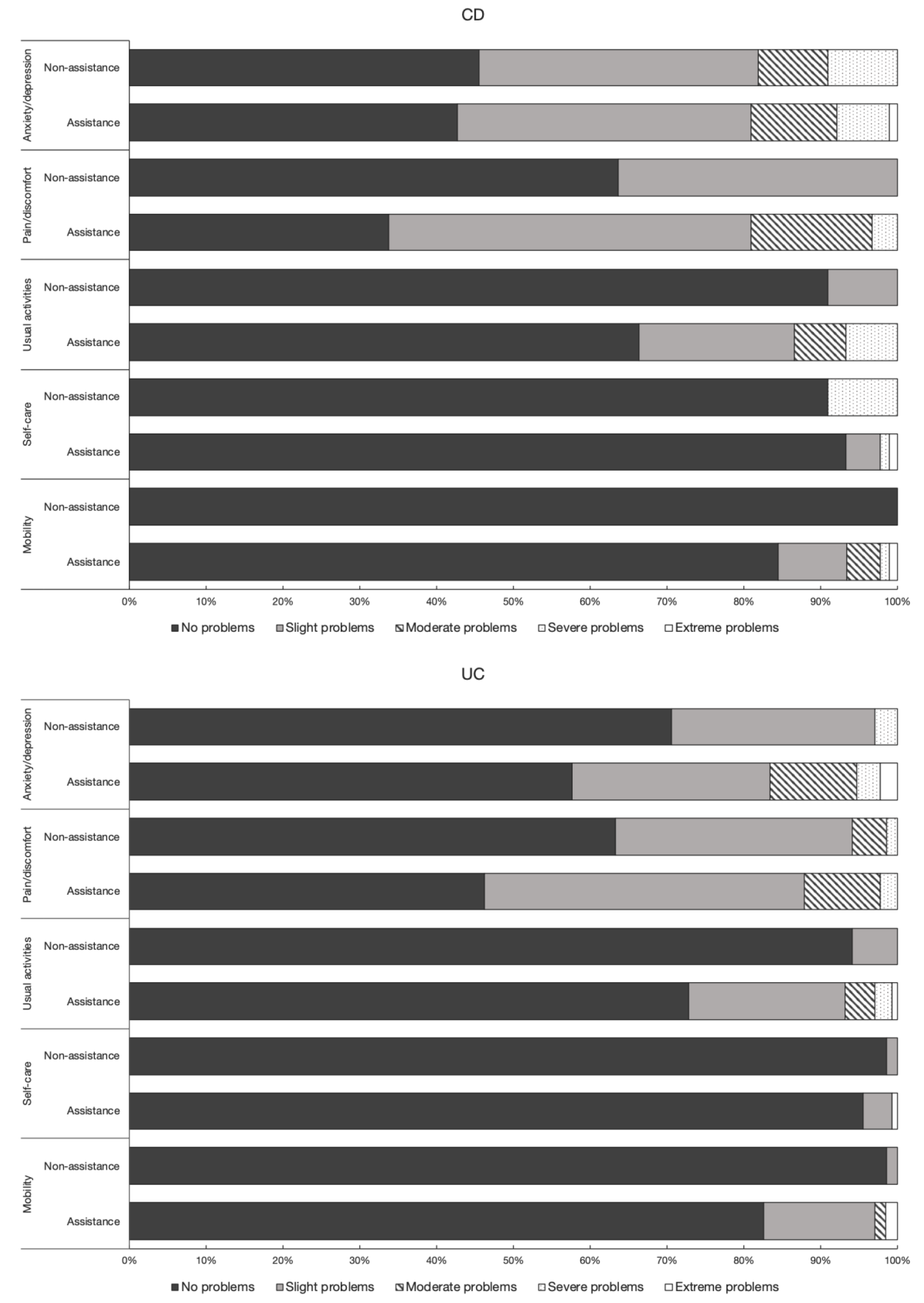
2.2. Quality of Life Indices
3. Discussion
4. Materials and Methods
4.1. Setting and Participants
4.2. Questionnaire
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kaplan, G.G.; Ng, S.C. Understanding and preventing the global increase of inflammatory bowel disease. Gastroenterology 2017, 152, 313–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molodecky, N.A.; Soon, I.S.; Rabi, D.M.; Ghali, W.A.; Ferris, M.; Chernoff, G.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Barkema, H.W.; et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology 2012, 142, 46–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okabayashi, S.; Kobayashi, T.; Hibi, T. Inflammatory bowel disease in Japan-Is it similar to or different from Westerns? J. Anus. Rectum. Colon. 2020, 4, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsumoto, T.; Yanai, S.; Toya, Y.; Ueno, M.; Nakamura, S. Internet-orientated assessment of QOL and actual treatment status in Japanese patients with inflammatory bowel disease: The 3I Survey. J. Crohns Colitis 2015, 9, 477–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamabe, K.; Liebert, R.; Flores, N.; Pashos, C.L. Health-related quality of life outcomes and economic burden of inflammatory bowel disease in Japan. Clin. Outcomes Res. 2019, 11, 221–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ueno, F.; Nakayama, Y.; Hagiwara, E.; Kurimoto, S.; Hibi, T. Impact of inflammatory bowel disease on Japanese patients’ quality of life: Results of a patient questionnaire survey. J. Gastroenterol. 2017, 52, 555–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahlich, J.; Matsuoka, K.; Nakamura, Y.; Sruamsiri, R. The relationship between socio-demographic factors, health status, treatment type, and employment outcome in patients with inflammatory bowel disease in Japan. BMC Public Health 2017, 17, 623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenberg, D.; Schwartz, D.; Vardi, H.; Friger, M.; Sarid, O.; Slonim-Nevo, V.; Odes, S. Health-related utility weights in a cohort of real-world Crohn’s disease patients. J. Crohns Colitis 2015, 9, 1138–1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuwano, T. Establishment of the Intractable/Rare Diseases Act and present government measures against intractable/rare diseases. Iryotosyakai 2018, 28, 17–26, [In Japanese]. [Google Scholar]
- Hashimoto, H.; Green, J.; Iwao, Y.; Sakurai, T.; Hibi, T.; Fukuhara, S. Reliability, validity, and responsiveness of the Japanese version of the Inflammatory Bowel Disease Questionnaire. J. Gastroenterol. 2003, 38, 1138–1143. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.L.; Zhong, L.H.; Wen, Y.; Liu, T.W.; Li, X.Y.; Hou, Z.K.; Hu, Y.; Mo, C.W.; Liu, F.B. Inflammatory bowel disease-specific health-related quality of life instruments: A systematic review of measurement properties. Health Qual. Life Outcomes 2017, 15, 177. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.; Smith, T.C.; Gray, G.C.; Ryan, M.A. When epidemiology meets the Internet: Web-based surveys in the Millennium Cohort Study. Am. J. Epidemiol. 2007, 166, 1345–1354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekman, A.; Dickman, P.W.; Klint, A.; Weiderpass, E.; Litton, J.E. Feasibility of using web-based questionnaires in large population-based epidemiological studies. Eur. J. Epidemiol. 2006, 21, 103–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolters, F.L.; van Zeijl, G.; Sijbrandij, J.; Wessels, F.; O’Morain, C.; Limonard, C.; Russel, M.G.; Stockbrugger, R.W. Internet-based data inclusion in a population-based European collaborative follow-up study of inflammatory bowel disease patients: Description of methods used and analysis of factors influencing response rates. World J. Gastroenterol. 2005, 11, 7152–7158. [Google Scholar] [CrossRef] [PubMed]
- Ueno, F.; Doi, M.; Kawai, Y.; Ukawa, N.; Cammarota, J.; Betts, K.A. Number needed to treat and cost per remitter for biologic treatments of Crohn’s disease in Japan. J. Med. Econ. 2020, 23, 80–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahlich, J.; Matsuoka, K.; Sruamsiri, R. Biologic treatment of Japanese patients with inflammatory bowel disease. BMC Gastroenterol. 2018, 18, 160. [Google Scholar] [CrossRef] [PubMed]
- Saito, S.; Nakazawa, K.; Suzuki, K.; Ishikawa, T.; Akazawa, K. Paradigm shift of healthcare cost for patients with inflammatory bowel diseases: A claims data-based analysis in Japan. Gastrointest. Disord. 2019, 1, 120–128. [Google Scholar] [CrossRef] [Green Version]
- Shiroiwa, T.; Ikeda, S.; Noto, S.; Igarashi, A.; Fukuda, T.; Saito, S.; Shimozuma, K. Comparison of value set based on DCE and/or TTO data: Scoring for EQ-5D-5L health states in Japan. Value Health 2016, 19, 648–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiroiwa, T.; Fukuda, T.; Ikeda, S.; Igarashi, A.; Noto, S.; Saito, S.; Shimozuma, K. Japanese population norms for preference-based measures: EQ-5D-3L, EQ-5D-5L, and SF-6D. Qual. Life Res. 2016, 25, 707–719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuoka, K.; Kobayashi, T.; Ueno, F.; Matsui, T.; Hirai, F.; Inoue, N.; Kato, J.; Kobayashi, K.; Kobayashi, K.; Koganei, K.; et al. Evidence-based clinical practice guidelines for inflammatory bowel disease. J. Gastroenterol. 2018, 53, 305–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Respondent Characteristic | CD | UC | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Eligible for Financial Assistance (n = 89) | Ineligible for Financial Assistance (n = 11) | P-Value | Eligible for Financial Assistance (n = 132) | Ineligible for Financial Assistance (n = 68) | P-Value | |||||
| Number or Median | % or IQR | Number or Median | % or IQR | Number or Median | % or IQR | Number or Median | % or IQR | |||
| Age (in years) | ||||||||||
| 20–29 | 4 | 4.5% | 0 | 0.0% | 0.682 | 7 | 5.3% | 2 | 2.9% | 0.558 |
| 30–39 | 20 | 22.5% | 2 | 18.2% | 22 | 16.7% | 7 | 10.3% | ||
| 40–49 | 29 | 32.6% | 5 | 45.5% | 30 | 22.7% | 14 | 20.6% | ||
| 50–59 | 28 | 31.5% | 2 | 18.2% | 41 | 31.1% | 28 | 41.2% | ||
| ≥ 60 | 8 | 9.0% | 2 | 18.2% | 32 | 24.2% | 17 | 25.0% | ||
| Sex | ||||||||||
| Male | 64 | 71.9% | 8 | 72.7% | 1.000 | 90 | 68.2% | 47 | 69.1% | 0.513 |
| Female | 25 | 28.1% | 3 | 27.3% | 42 | 31.8% | 21 | 30.9% | ||
| Annual income (in Japanese yen) | ||||||||||
| Low (<300 million) | 51 | 57.3% | 7 | 63.6% | 0.400 | 79 | 59.8% | 34 | 50.0% | 0.333 |
| Middle (≥300 million and <500 million) | 14 | 15.7% | 3 | 27.3% | 22 | 16.7% | 12 | 17.6% | ||
| High (≥500 million) | 24 | 27.0% | 1 | 9.1% | 31 | 23.5% | 22 | 32.4% | ||
| Marital status | ||||||||||
| Single | 44 | 49.4% | 4 | 36.4% | 0.529 | 38 | 28.8% | 16 | 23.5% | 0.502 |
| Married * | 45 | 50.6% | 7 | 63.6% | 94 | 71.2% | 52 | 76.5% | ||
| Age at diagnosis (in years) | 27 | 20–34 | 30 | 21–35 | 0.494 | 38 | 26.5–50 | 38.5 | 27.5–52.5 | 0.457 |
| Disease duration (in years) | 17 | 11–24 | 17 | 1–27 | 0.632 | 10 | 5–18 | 9.5 | 3.5–19.5 | 0.555 |
| Previous surgery for IBD | ||||||||||
| Yes | 66 | 74.2% | 7 | 63.6% | 0.482 | 13 | 9.8% | 4 | 5.9% | 0.429 |
| No | 23 | 25.8% | 4 | 36.4% | 119 | 90.2% | 64 | 94.1% | ||
| Hospitalization for IBD in the past year | ||||||||||
| Yes | 23 | 25.8% | 2 | 18.2% | 0.726 | 19 | 14.4% | 4 | 5.9% | 0.101 |
| No | 66 | 74.2% | 9 | 81.8% | 113 | 85.6% | 64 | 94.1% | ||
| Treatment | CD (N = 100) | UC (N = 200) | ||||||
|---|---|---|---|---|---|---|---|---|
| Number | % | Median EQ-5D-5L Score | IQR | Number | % | Median EQ-5D-5L Score | IQR | |
| Treated with 5-ASA | ||||||||
| Yes | 76 | 76.0% | 0.823 | 0.751–0.895 | 164 | 82.0% | 0.895 | 0.823–1 |
| No | 24 | 24.0% | 0.867 | 0.788–0.895 | 36 | 18.0% | 0.883 | 0.780–1 |
| Treated with elemental diet | ||||||||
| Yes | 52 | 52.0% | 0.823 | 0.722–0.880 | 5 | 2.5% | 0.670 | 0.629–0.685 |
| No | 48 | 48.0% | 0.867 | 0.810–1 | 195 | 97.5% | 0.895 | 0.823–1 |
| Treated with steroids | ||||||||
| Yes | 12 | 12.0% | 0.823 | 0.741–0.849 | 18 | 9.0% | 0.823 | 0.676–0.867 |
| No | 88 | 88.0% | 0.833 | 0.772–0.895 | 182 | 91.0% | 0.895 | 0.823–1 |
| Treated with immunomodulators | ||||||||
| Yes | 30 | 30.0% | 0.792 | 0.710–0.895 | 29 | 14.5% | 0.825 | 0.734–0.895 |
| No | 70 | 70.0% | 0.867 | 0.799–0.895 | 171 | 85.5% | 0.895 | 0.823–1 |
| Treated with CAP | ||||||||
| Yes | 1 | 1.0% | 0.469 | 0.469–0.469 | 2 | 1.0% | 0.657 | 0.629–0.685 |
| No | 99 | 99.0% | 0.823 | 0.771–0.895 | 198 | 99.0% | 0.895 | 0.823–1 |
| Treated with biological drugs | ||||||||
| Yes | 60 | 60.0% | 0.823 | 0.751–0.895 | 13 | 6.5% | 0.799 | 0.734–0.895 |
| No | 40 | 40.0% | 0.849 | 0.772–0.947 | 187 | 93.5% | 0.895 | 0.823–1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thi Thanh Tran, H.; Saito, S.; Noto, S.; Suzuki, K. Quality of Life and Eligibility for Specific Financial Assistance for Medical Expenses: A Cross-Sectional Web-Based Survey among Patients with Inflammatory Bowel Disease in Japan. Gastrointest. Disord. 2020, 2, 123-133. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord2020012
Thi Thanh Tran H, Saito S, Noto S, Suzuki K. Quality of Life and Eligibility for Specific Financial Assistance for Medical Expenses: A Cross-Sectional Web-Based Survey among Patients with Inflammatory Bowel Disease in Japan. Gastrointestinal Disorders. 2020; 2(2):123-133. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord2020012
Chicago/Turabian StyleThi Thanh Tran, Huyen, Shota Saito, Shinichi Noto, and Kenji Suzuki. 2020. "Quality of Life and Eligibility for Specific Financial Assistance for Medical Expenses: A Cross-Sectional Web-Based Survey among Patients with Inflammatory Bowel Disease in Japan" Gastrointestinal Disorders 2, no. 2: 123-133. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord2020012