Gastroparesis in the Pediatric Patient: Children Are Not Little Adults


Division of Gastroenterology, Hepatology, and Nutrition, Department of Pediatrics, Nationwide Children’s Hospital, Columbus, OH 43205, USA
*
Author to whom correspondence should be addressed.
Gastrointest. Disord. 2020, 2(2), 86-95; https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord2020008
Submission received: 2 March 2020
/
Revised: 7 April 2020
/
Accepted: 16 April 2020
/
Published: 22 April 2020
(This article belongs to the Special Issue Gastroparesis)
Abstract
:Although the definition of gastroparesis in children is the same as in adults, there are key differences between gastroparesis in these two populations in presentation, diagnosis, treatment and outcomes. Infants and younger children with gastroparesis tend to be male, present with vomiting as their primary symptom and are more likely to experience the resolution of their symptoms over time. Adolescents with gastroparesis tend to be female, present with abdominal pain as their primary symptom and have a less favorable short- and medium-term outcome, sharing some similarities with adults with gastroparesis. Despite the fact that validated diagnostic criteria for gastroparesis are lacking in infants and younger children, these age groups make up nearly half of children with gastroparesis in some studies. The diagnosis and treatment of children with gastroparesis has thus far relied heavily on research studies performed in adults, but it is becoming increasingly clear that gastroparesis in children is a distinct entity and there are limitations to the applicability of data obtained from adults to the care of children.
1. Introduction
As it is in adults, gastroparesis in children is defined as a delay in gastric emptying in the absence of mechanical obstruction that is accompanied by corresponding symptoms like nausea, vomiting, early satiety, bloating and abdominal pain [1,2]. This disorder results from neuromuscular dysfunction that can be idiopathic in nature or associated with underlying diseases, medical or surgical interventions or preceding infections. Although the definition and presentation of gastroparesis in adults and children share similarities, even the limited available literature on gastroparesis in children demonstrates key differences between gastroparesis in these two populations. The diagnosis and management of gastroparesis in children has thus far leaned heavily on research performed in adult patients, but it is becoming increasingly clear that gastroparesis in children is a distinct entity and that there are limitations to the applicability of adult research to the care of children [2,3]. In this review, we examined the similarities and differences between gastroparesis in children and adults in clinical presentation, diagnosis, treatment and outcomes.
2. Clinical Presentation
2.1. Epidemiology
Because of challenges both shared with adults and unique to children, the prevalence of gastroparesis in children is unknown. As is the case in adults, the clinical presentation of gastroparesis overlaps with that of other disorders, particularly functional dyspepsia, and therefore the estimates of incidence and prevalence, based on patients who sought care and underwent confirmatory gastric emptying measurement, are likely to be underestimates. In one study using a questionnaire to predict gastric emptying, it was estimated that as many as 1.8% of adults have gastroparesis [4]. Similar estimates are not available in children. The measurement of the prevalence of gastroparesis in children is particularly challenging because of the lack of standardized diagnostic criteria, especially for younger patients. However, although the prevalence of gastroparesis in children remains unknown, the number of hospitalizations required for children with gastroparesis has been rising dramatically over the past decade. The cost of these hospitalizations increased nearly six-fold from 2004–2013 [5]. It is clear that gastroparesis in children is a problem that deserves our attention.
Gastroparesis affects children of all ages but is more frequently diagnosed in infants and young children. In one series of over 200 children with gastroparesis, 40.5% were five years of age or younger [6]. In a review of over 4000 patients of 0–21 years of age with gastroparesis requiring hospitalization, 43.5% of hospitalizations were for children of five years of age or younger [5]. There seems to be a male predominance among infants diagnosed with gastroparesis, with one series finding nearly a 3:1 male-to-female ratio among infants diagnosed by gastric emptying scintigraphy (GES) with a liquid meal [6]. Children with gastroparesis are equally likely to be male or female, but a female predominance develops in adolescence with a 2:1 female-to-male ratio in those >17 years of age [6]. There is a clear female predominance among adults with gastroparesis, with some studies reporting a 4:1 female-to-male ratio [1].
2.2. Etiology
The majority of children with gastroparesis do not have an identifiable etiology and are therefore classified as having idiopathic gastroparesis [6]. Although gastroparesis is often considered idiopathic in adults as well, an identifiable cause is more often found in adults (50%–70%) compared to children (30%) [3,6]. In two larger studies of children with gastroparesis based on GES measurement of liquid or solid emptying, the most common causes of gastroparesis were a preceding infection (5%–18%), medication effect (18%) and a complication of surgery (12.5%) [6,7]. Narcotic use was an uncommon cause of gastroparesis in children [6]. However, comorbidities such as a history of prematurity, cerebral palsy, developmental delay and seizure disorder are relatively common (38.5% in one series), and likely play a role in the presentation of these children [6]. Delayed gastric emptying has been found in 80% of critically ill children starting enteral feeding and 69% of children with mitochondrial disorders [8,9]. Diabetes mellitus is the most common identifiable etiology of gastroparesis in adults, but accounts for only 2%–4% of gastroparesis in children [6,7]. The underlying pathophysiology of gastroparesis in children is not well understood, although there is limited data suggesting an association between antral eosinophils, mast cell degranulation, and delayed gastric emptying [2].
2.3. Symptoms
Children with gastroparesis most commonly present with vomiting (42%–68%) and abdominal pain (35%–51%). Nausea, early satiety and weight loss are reported in about a quarter of children with this diagnosis [6,7]. The presentation of gastroparesis in children is similar to the presentation of functional dyspepsia, and up to half of children with functional dyspepsia have delayed gastric emptying [2]. Presentation can change with age, with infants and children more likely to experience vomiting (69% and 45%, respectively) than adolescents (28%). Adolescents with gastroparesis are most likely to report abdominal pain as a presenting symptom, followed by nausea and then vomiting [7]. In adults with gastroparesis, nausea is the most commonly reported symptom (79%–93%) followed by abdominal pain (73%) and vomiting (41%–68%) [1,10]. Although a subset of adults with gastroparesis have pain-predominant symptoms, nausea/vomiting predominance is more common [11].
Symptom scores validated in adults with gastroparesis have not been able to be validated in children. The Gastroparesis Cardinal Symptom Index (GCSI), a validated symptom severity score used for adults with gastroparesis, is not associated with delayed gastric emptying in children. This was demonstrated in a cohort that consisted primarily of older children and adolescents, who one might presume would be closer in clinical presentation to adults. When each symptom was analyzed individually, only nausea severity was associated with delayed gastric emptying [12].
3. Diagnosis
Similar to adults, the diagnosis of gastroparesis in children requires the demonstration of delayed gastric emptying. However, the method by which to do so is less clear, particularly in younger children. A summary of the more commonly used tests is shown in Table 1.
3.1. Gastric Emptying Scintigraphy
GES remains the standard method for the measurement of gastric emptying [11]. For older children and adolescents, GES is generally performed in a similar manner to how it is performed in adults. GES involves the ingestion of a radiolabeled standard meal followed by serial measurement of radioactivity in the stomach, which correlates directly with the amount of the meal remaining in the stomach. GES is performed after a period of fasting and after the discontinuation of medications that can affect gastric emptying, including prokinetic medications and opiates [13]. In adults, the standard meal consists of the equivalent of two eggs labeled with Tc-99m sulfur colloid along with two slices of white bread, jam, and 120 ml of water. Imaging is usually performed at baseline, 1 hour, 2 hours, and 4 hours after the ingestion of the meal. Delayed gastric emptying is defined as having >90% retention at 1 hour, >60% at 2 hours and >10% at 4 hours [14]. These diagnostic criteria have been directly applied to children and adolescents, as normative data are not available for the pediatric population. Although variability remains in how GES is performed among pediatric institutions, extending the study to 4 hours has been recommended for children as well. In two pediatric studies comparing 2-hour and 4-hour studies, investigators found that extending the study from 2 to 4 hours increased the percentage of abnormal studies from 51% to 62% in one study and 13% to 26% in the other. Despite having normal emptying at 2 hours, another 15%–23% of children will have delayed emptying at 4 hours [15,16]. Much like in adults, symptom severity does not seem to correlate with the presence or degree of delayed gastric emptying in children [3,16].
While limitations to the standard GES protocol have been identified for adults undergoing evaluation for gastroparesis, these limitations are even more significant when the protocol is applied to children [1]. The standard meal is not developmentally appropriate for infants and younger children. Even for older children, it can be challenging to finish the standard meal in a timely manner given the volume of the meal and the types of food in the meal. In one series of children of 4 years of age and older, 13% were unable to complete the ingestion of the standard meal. Children who were younger and physically smaller based on body surface area were less likely to be able to complete the meal [17]. The standard meal may also not be acceptable to children based on dietary restrictions (for example, those with egg or wheat allergies) and if they are not accustomed to a Western diet [18].
Perhaps the most glaring limitation in diagnosing gastroparesis in children is the lack of age and size-based normative values. Age and anthropometric measurements, particularly body surface area, can affect the gastric emptying measurements in children [17]. The relative size and nutritional content of the standard meal are very different for a four-year-old child compared to an adult. However, given the radiation exposure associated with GES testing, investigators have been reluctant to apply the test to large numbers of healthy children to establish normative values [3]. This limitation is even more prominent when we consider infants and younger children, for whom the standard meal is not developmentally appropriate. In this population, clinicians often rely on the measurement of the gastric emptying of liquid (for example, radiolabeled formula), again without established normative data. As noted earlier, 40.5%–43.5% of patients described in studies of children with gastroparesis are infants or children younger than five years of age [5,7].
3.2. Gastric Emptying Breath Testing
Gastric emptying breath testing (GEBT) has been studied in children with suspected gastroparesis, but its clinical use is still not widespread. In prior studies, GEBT has been performed in a manner similar to how it is performed in adults. GEBT is particularly appealing in the pediatric population as it does not involve radiation exposure and can be performed in an office setting. 13C is a stable non-radioactive isotope most commonly administered as 13C-octanoic acid (octanoic acid is a medium-chain fatty acid) or 13C-spirulina (Spirulina platensis is an edible blue-green algae). When ingested with a solid meal (prior studies in children have used eggs, cake, or pancakes), subsequent measurement of 13CO2 in breath samples correlates with the rate of gastric emptying [1,19,20]. Several smaller studies have reported a good correlation between GEBT and GES measurements in children [20,21,22]. Investigators have performed GEBT on healthy children to report normative values, most recently in a larger cohort of 120 children who underwent 13C-octanoic acid breath testing with a pancake meal. In this cohort, the mean gastric half-emptying time was 157.7 +/− 54.0 minutes and decreased with age from 1 to 10 years of age before stabilizing [20]. GEBT results can also be influenced by physical activity and confounding factors like malabsorption, hepatic dysfunction and pulmonary disease [1]. However, particularly if further studies support the correlation between gastric emptying measured by GEBT and GES, GEBT could allow the determination of age and size-based normal gastric emptying values.
3.3. Wireless Motility Capsule
Wireless motility capsule (WMC) testing involves the oral ingestion of a non-digestible capsule that continuously records pH, pressure and temperature as the capsule progresses through the gastrointestinal tract. By measuring the time from capsule ingestion until a sharp rise in pH corresponding to its exit from the acidic environment of the stomach, the investigator is able to calculate gastric emptying time [23]. In adults, studies evaluating the correlation between gastric emptying time as measured by the WMC and gastric emptying as measured by GES have provided mixed results [24,25]. In children, one study found that prolonged gastric emptying time was sensitive (100% sensitivity) but not specific (50% specificity) in identifying delayed gastric emptying as measured by GES [26]. Normative data are not available in the pediatric population. WMC testing is not widely available in pediatric institutions, partially due to limited insurance coverage. The size of the capsule also precludes its use in most children younger than five years of age.
4. Treatment
Treatment for both children and adults with gastroparesis involves addressing fluid, electrolyte, and nutritional needs; treating any identifiable cause of the delayed gastric emptying; and managing symptoms [1]. Adults with gastroparesis are more likely to have an identifiable etiology, particularly one that can be directly treated, like diabetes mellitus. Unfortunately, the majority of children with gastroparesis do not have an identifiable cause, and therefore once fluid, electrolyte, and nutritional issues have been addressed, treatment generally involves managing the child’s symptoms. This begins with dietary modifications both to minimize symptoms and to ensure adequate nutritional support. A summary of treatment options is shown in Table 2. Unlike in adults, there are no pediatric studies demonstrating differences in treatment response based on underlying etiology.
4.1. Dietary Modification
Dietary modifications need to be adapted based on the infant or child’s baseline feeding regimen and developmental age. The goals of dietary modification are to ensure adequate nutritional intake while limiting gastric retention and subsequent associated symptoms. Smaller meals with lower fat and fiber content given more frequently throughout the day can be easier to tolerate for children with gastroparesis. For children with more persistent symptoms, formula supplementation or a trial of a pureed diet may be better tolerated, particularly as liquid emptying is often preserved in gastroparesis. For children with more severe symptoms leading to the intolerance of oral feeding, continuous tube feeding or transpyloric feeding is often needed [23,31]. However, dietary modifications alone are rarely effective. In one series, only 1.5% of children with gastroparesis responded to dietary modification alone [7].
4.2. Pharmacologic Treatment
The majority of children with gastroparesis will therefore receive pharmacologic treatment. Metoclopramide is generally considered first-line treatment for adults with gastroparesis, but its use in children has been limited by concerns regarding neurological side effects like tardive dyskinesia that have led to a black box warning from the United States Food and Drug Administration [1,3]. Metoclopramide is a dopamine D2-receptor antagonist that has both prokinetic and antiemetic properties. In a study of children with gastroparesis reported by Rodriguez et al., metoclopramide was the most commonly used prokinetic medication but only 20% reported a favorable response and 11% had resolution of symptoms. Nearly a quarter of children reported side effects, with behavioral changes, dystonia, insomnia and movement disorders reported most often [7]. The limited data available raises the concern that metoclopramide may be less beneficial for children with gastroparesis compared to adults. Domperidone, another dopamine antagonist with both prokinetic and antiemetic effects, was the most effective prokinetic in the study, with 74% reporting response and 26% reporting the resolution of symptoms. Side effects were reportedly in only 6% of children [7]. Domperidone has previously been shown to be superior to cisapride in improving symptoms and gastric emptying in children with diabetic gastroparesis [27]. Unfortunately, domperidone is currently only available in the United States through the Food and Drug Administration Investigational New Drug application process [3]. Cisapride, a 5-hydroxytryptamine type 4 (HT4) receptor agonist, was previously used for gastroparesis but has been removed from commercial use in the United States because of the risk of ventricular arrhythmias [2].
Erythromycin, a macrolide antibiotic and motilin agonist, has a pure prokinetic effect and is generally well tolerated in children. As is the case in adults, children can experience tachyphylaxis with a decrease in efficacy after as little as 4 weeks [32]. For some children, this can be overcome by alternating between erythromycin treatment and scheduled time off the medication. Given the aforementioned concerns regarding metoclopramide, erythromycin is the most commonly used prokinetic in some studies of children with gastroparesis and has been used for infants, children and adolescents [6]. In the same study by Rodriguez et al., 51% of children responded to erythromycin but only 5% reported a resolution of symptoms. However, side effects were less common than with metoclopramide (10% versus 24%) and included abdominal pain, headache and behavioral changes [7].
Proton pump inhibitors, antiemetics, and neuromodulators are often used for children with gastroparesis as well, particularly given the overlap in the presentations between gastroparesis and functional dyspepsia. Tricyclic antidepressants with a more prominent anticholinergic effect, like amitriptyline, can delay gastric emptying and are generally avoided in children with gastroparesis [23]. However, in the six children in the study by Rodriguez et al. who were treated with amitriptyline, all reported a positive response, perhaps further emphasizing the overlap between gastroparesis and functional dyspepsia [7].
4.3. Pyloric Intervention
When children with gastroparesis continue to experience symptoms impacting their quality of life or nutritional status despite medical treatment with dietary modification and pharmacologic treatment, pyloric intervention should be considered. In a subset of adults with gastroparesis, pyloric sphincter dysfunction and pylorospasm is thought to play a role in impairing gastric emptying. Endoscopic intrapyloric botulinum toxin injection has been used to treat adults with gastroparesis with some benefit, although two controlled studies did not show significant improvement in symptoms compared to placebo [33,34]. In a retrospective review of intrapyloric botulinum toxin injections performed in 45 children with gastroparesis, two-thirds reported some degree of improvement after the procedure with improvement lasting a median of 3 months. Older children and those with vomiting were more likely to respond [28]. Pyloroplasty and pyloromyotomy (including gastric per-oral endoscopic myotomy) have been used in adults with gastroparesis, but the pediatric literature on these interventions remains limited. In the series of children with gastroparesis reported by Rodriguez et al, six children underwent pyloroplasty with some degree of positive response in all six children [7]. In another series of children with gastroesophageal reflux disease and concurrent delayed gastric emptying who underwent pyloromyotomy at the time of fundoplication, investigators found an improvement in gastric emptying during the follow up [35]. Prospective, controlled studies on pyloric interventions for children with refractory gastroparesis are needed.
4.4. Gastric Electrical Stimulation
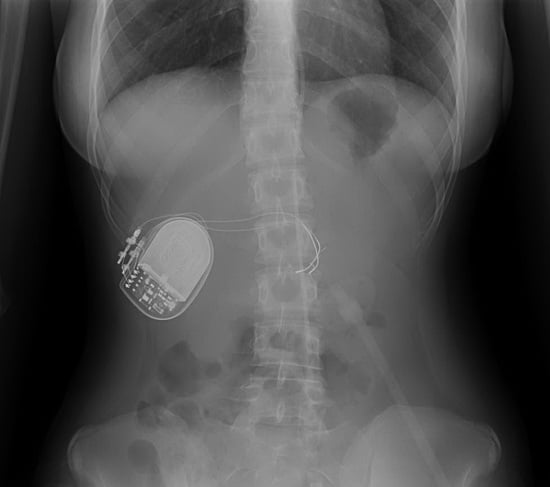
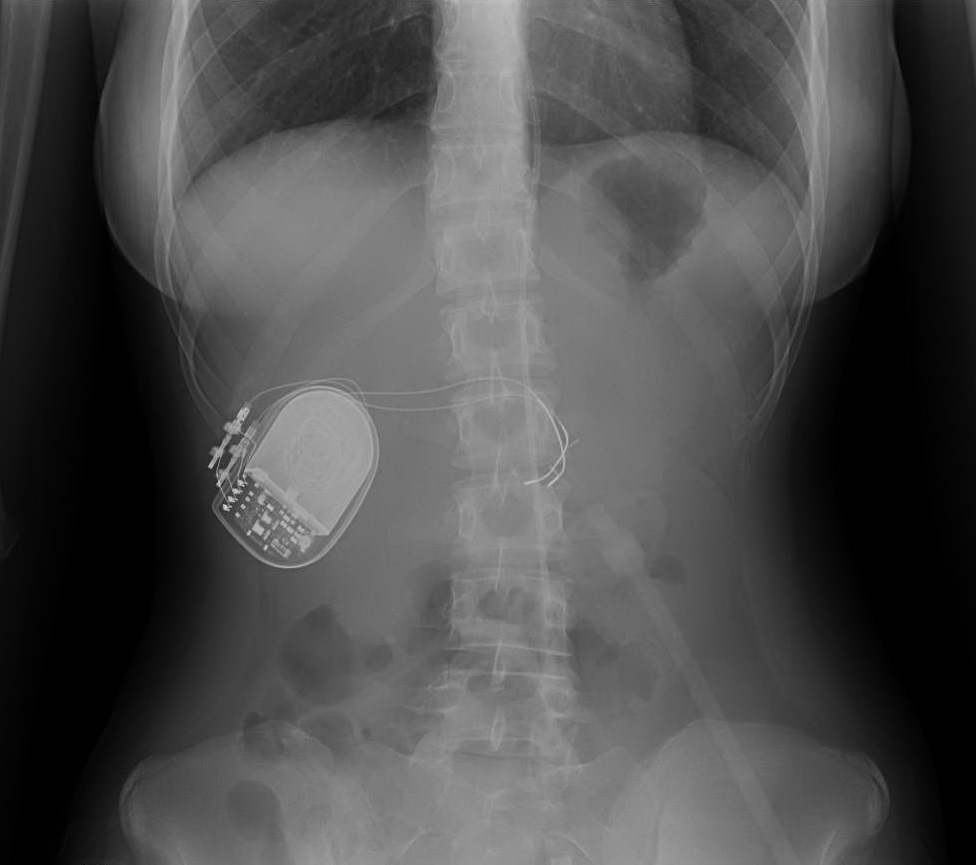
Gastric electrical stimulation is generally reserved for children with debilitating symptoms or long-term dependence on supplemental nutrition (like tube feeding or parenteral nutrition) despite treatment with the therapies previously described. Gastric electrical stimulation involves the application of high-frequency, low-energy electrical stimulation via electrodes implanted along the greater curvature of the stomach. Gastric electrical stimulation has been used for adults with nausea and vomiting refractory to conventional treatment for over two decades and in children for over the past decade [36]. The literature supporting its use in adults has been growing over time, most recently after a randomized controlled trial of 172 patients treated with gastric electrical stimulation demonstrated significantly improved vomiting scores when the stimulator was on compared to off [37]. Gastric electrical stimulation appeared to have several early and late physiological effects, but its beneficial effect on gastric emptying was not consistent. Symptomatic improvement was seen in both patients with and without gastroparesis, and in those with baseline delayed gastric emptying there can be a prokinetic effect as well [38]. Several observational studies of children as young as two years of age with refractory nausea and vomiting (with and without gastroparesis) have found significant and durable improvement in symptom severity, quality of life and feeding tolerance after gastric electrical stimulation treatment. Many pediatric centers proceed with stimulator implantation only after a successful response to a minimally invasive trial of temporary stimulation delivered by a lead placed endoscopically through the nares or pre-existing gastrostomy [29,30,39].
5. Outcomes
Although our understanding of the clinical outcomes for children with gastroparesis is limited, it does appear that the likelihood of symptom improvement and resolution is higher in children than in adults with gastroparesis. The majority of adults with gastroparesis continued to experience symptoms in the long-term, with only 24%–26% experiencing a ≥1 point improvement in GCSI after one year of follow up [40]. In contrast, the majority of children with gastroparesis experience symptom improvement or resolution. In a study of 204 children with gastroparesis, Rodriguez et al. found that 52% experienced resolution of their symptoms after a median follow up of 18 months. The majority of children who experienced symptom resolution had done so prior to 12 months after their diagnosis [7]. In a study of 239 children with gastroparesis, Waseem et al. found significant improvements in nausea, vomiting, abdominal pain, early satiety and weight loss after a mean follow up of 24 months [6]. Clinical outcomes appear to differ based on the child’s age and etiology. In the study by Rodriguez et al., infants and children were more likely to experience a resolution of symptoms than adolescents. Multivariate analysis found that in addition to older age, a longer duration of the symptoms, lack of response to a prokinetic medication and a concurrent diagnosis of mitochondrial disorder led to a lower likelihood of symptom resolution during follow up [7]. In a case series of children with post-viral gastroparesis, all affected patients recovered within 24 months [41].
6. Conclusions
The published literature on gastroparesis in children is limited. Nonetheless, it is clear based on the information we have that gastroparesis in children is distinct from gastroparesis in adults, with key differences in presentation, diagnosis, treatment response and outcome. The toddler with a history of prematurity, cerebral palsy, mitochondrial disorder and delayed gastric emptying is clearly different from the adult with diabetes mellitus, chronic narcotic use and delayed gastric emptying. While both patients share the common finding of delayed gastric emptying, they are otherwise experiencing completely different disorders.
Gastroparesis appears to differ even among different pediatric age groups. Infants and young children with gastroparesis are more likely to be male and to experience resolution of their symptoms within 18–24 months of follow up. Adolescents with gastroparesis are more likely to be female and less likely to experience symptom resolution, perhaps transitioning into a phenotype more similar to adults. Vomiting is the predominant symptom of gastroparesis in younger children compared to abdominal pain in adolescents. These clinical distinctions within the pediatric population argue that appropriate evaluation and management should differ by age group as well.
One of the primary limitations to our understanding of gastroparesis in children is how we evaluate gastric emptying in children. While it may be appropriate to apply adult normative values to adolescents, we have evidence that this is not appropriate for younger and smaller children, even if they are able to complete the standardized meal required for GES. There is growing interest in the use of GEBT in children, which may enable the identification of normative values for gastric emptying across age groups. Another limitation is the lack of clinical measures of gastroparesis severity validated in infants, children, and adolescents. Development of validated symptom scores for each of these populations would facilitate the evaluation of treatment options. These are key steps toward understanding how to best evaluate and treat pediatric patients with gastroparesis.
Further research on gastroparesis specific to children is needed, particularly when we consider the dramatic increase in the number and cost of hospitalizations for gastroparesis in children over the past decade [5]. It is encouraging that attention to this issue is growing, with several other recent publications echoing the distinctions between gastroparesis in children and adults [2,3]. With a new focus on gastroparesis in children and advances in diagnostic testing and treatment, the future is bright.
Conflicts of Interest
The authors declare no conflicts of interest
References
- Camilleri, M.; Chedid, V.; Ford, A.C.; Haruma, K.; Horowitz, M.; Jones, K.L.; Low, P.A.; Park, S.Y.; Parkman, H.P.; Stanghellini, V. Gastroparesis. Nat. Rev. Dis. Primers 2018. [Google Scholar] [CrossRef] [PubMed]
- Kovacic, K.; Elfar, W.; Rosen, J.M.; Yacob, D.; Raynor, J.; Mostamand, S.; Punati, J.; Fortunato, J.E.; Saps, M. Update on pediatric gastroparesis: A review of the published literature and recommendations for future research. Neurogastroenterol. Motil. 2020, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Febo-Rodriguez, L.; Chumpitazi, B.P.; Shulman, R.J. Childhood gastroparesis is a unique entity in need of further investigation. Neurogastroenterol. Motil. 2020, 32. [Google Scholar] [CrossRef] [PubMed]
- Rey, E.; Choung, R.S.; Schleck, C.D.; Zinsmeister, A.R.; Talley, N.J.; Locke, G.R. Prevalence of hidden gastroparesis in the community: The gastroparesis “Iceberg”. J. Neurogastroenterol. Motil. 2012, 18, 34–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, P.L.; Moore-Clingenpeel, M.; Yacob, D.; Di Lorenzo, C.; Mousa, H.M. The rising cost of hospital care for children with gastroparesis: 2004–2013. Neurogastroenterol. Motil. 2016. [Google Scholar] [CrossRef]
- Waseem, S.; Islam, S.; Kahn, G.; Moshiree, B.; Talley, N.J. Spectrum of gastroparesis in children. J. Pediatr. Gastroenterol. Nutr. 2012, 55, 166–172. [Google Scholar] [CrossRef]
- Rodriguez, L.; Irani, K.; Jiang, H.; Goldstein, A.M. Clinical presentation, response to therapy, and outcome of gastroparesis in children. J. Pediatr. Gastroenterol. Nutr. 2012, 55, 185–190. [Google Scholar] [CrossRef]
- Martinez, E.E.; Pereira, L.M.; Gura, K.; Stenquist, N.; Ariagno, K.; Nurko, S.; Mehta, N.M. Gastric emptying in critically III children. J. Parenter. Enter. Nutr. 2017, 41, 1100–1109. [Google Scholar] [CrossRef]
- Bhardwaj, J.; Wan, D.Q.; Koenig, M.K.; Liu, Y.; Hashmi, S.S.; Rhoads, J.M. Impaired gastric emptying and small bowel transit in children with mitochondrial disorders. J. Pediatr. Gastroenterol. Nutr. 2012, 55, 194–199. [Google Scholar] [CrossRef]
- Hasler, W.L.; Wilson, L.A.; Parkman, H.P.; Koch, K.L.; Abell, T.L.; Nguyen, L.; Pasricha, P.J.; Snape, W.J.; McCallum, R.W.; Sarosiek, I.; et al. Factors related to abdominal pain in gastroparesis: contrast to patients with predominant nausea and vomiting. Neurogastroenterol. Motil. 2013, 25, 427-e301. [Google Scholar] [CrossRef] [Green Version]
- Abell, T.L.; Camilleri, M.; Donohoe, K.; Hasler, W.L.; Lin, H.C.; Maurer, A.H.; McCallum, R.W.; Nowak, T.; Nusynowitz, M.L.; Parkman, H.P.; et al. Consensus recommendations for gastric emptying scintigraphy: A joint report of the american neurogastroenterology and motility society and the society of nuclear medicine. Am. J. Gastroenterol. 2008, 103, 753–763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jericho, H.; Adams, P.; Zhang, G.; Rychlik, K.; Saps, M. Nausea predicts delayed gastric emptying in children. J. Pediatr. 2014, 164, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.S.C.; Camilleri, M.; Hasler, W.L.; Maurer, A.H.; Parkman, H.P.; Saad, R.; Scott, M.S.; Simren, M.; Soffer, E.; Szarka, L. Evaluation of gastrointestinal transit in clinical practice: Position paper of the american and european neurogastroenterology and motility societies. Neurogastroenterol. Motil. 2011, 23, 8–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tougas, G. Assessment of gastric emptying using a low fat meal: Establishment of international control values. Am. J. Gastroenterol. 2000, 95, 1456–1462. [Google Scholar] [CrossRef] [PubMed]
- Chogle, A.; Saps, M. Gastroparesis in children. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 439–442. [Google Scholar] [CrossRef] [PubMed]
- Edwards, S.T.; Cocjin, J.; Theut, S.B.; Rivard, D.; Sherman, A.K.; Friesen, C.A. A comparison of the diagnosis of gastroparesis in 4 h pediatric gastric emptying studies versus 2 h studies. BMC Gastroenterol. 2019, 19, 26. [Google Scholar] [CrossRef] [Green Version]
- Wong, G.K.; Shulman, R.J.; Chumpitazi, B.P. Gastric emptying scintigraphy results in children are affected by age, anthropometric factors, and study duration. Neurogastroenterol. Motil. 2015, 27, 356–362. [Google Scholar] [CrossRef] [Green Version]
- Malik, R.; Srivastava, A.; Gambhir, S.; Yachha, S.K.; Siddegowda, M.; Ponnusamy, M.; Poddar, U. Assessment of gastric emptying in children: Establishment of control values utilizing a standardized vegetarian meal. J. Gastroenterol. Hepatol. 2016, 31, 319–325. [Google Scholar] [CrossRef]
- Chitkara, D.K.; Camilleri, M.; Zinsmeister, A.R.; Burton, D.; El-Youssef, M.; Freese, D.; Walker, L.; Stephens, D. Gastric sensory and motor dysfunction in adolescents with functional dyspepsia. J. Pediatr. 2005, 146, 500–505. [Google Scholar] [CrossRef]
- Hauser, B.; Roelants, M.; De Schepper, J.; Veereman, G.; Caveliers, V.; Devreker, T.; De Greef, E.; Vandenplas, Y. Gastric emptying of solids in children: reference values for the 13 c-octanoic acid breath test. Neurogastroenterol. Motil. 2016, 28, 1480–1487. [Google Scholar] [CrossRef]
- Braden, B.; Peterknecht, A.; Piepho, T.; Schneider, A.; Caspary, W.; Hamscho, N.; Ahrens, P. Measuring gastric emptying of semisolids in children using the 13C-acetate breath test: A validation study. Dig. Liver Dis. 2004, 36, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Eradi, B.; Wright, J.; Gibbons, N.J.; Blackshaw, P.E.; Perkins, A.C.; Wakefield, J.; Sithole, J.; Singh, S.J. Validity of 13C octanoic acid breath test for measurement of solid meal gastric emptying time in children. J. Pediatr. Surg. 2006, 41, 2062–2065. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, M.; Parkman, H.P.; Shafi, M.A.; Abell, T.L.; Gerson, L. Clinical guideline: Management of gastroparesis. Am. J. Gastroenterol. 2013, 108, 18–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuo, B.; McCallum, R.W.; Koch, K.L.; Sitrin, M.D.; Wo, J.M.; Chey, W.D.; Hasler, W.L.; Lackner, J.M.; Katz, L.A.; Semler, J.R.; et al. Comparison of gastric emptying of a nondigestible capsule to a radio-labelled meal in healthy and gastroparetic subjects. Aliment. Pharmacol. 2008, 27, 186–196. [Google Scholar] [CrossRef]
- Hasler, W.L.; May, K.P.; Wilson, L.A.; Van Natta, M.; Parkman, H.P.; Pasricha, P.J.; Koch, K.L.; Abell, T.L.; McCallum, R.W.; Nguyen, L.A.; et al. Relating gastric scintigraphy and symptoms to motility capsule transit and pressure findings in suspected gastroparesis. Neurogastroenterol. Motil. 2018, 30, e13196. [Google Scholar] [CrossRef]
- Green, A.D.; Belkind-Gerson, J.; Surjanhata, B.C.; Mousa, H.; Kuo, B.; Di Lorenzo, C. Wireless motility capsule test in children with upper gastrointestinal symptoms. J. Pediatr. 2013, 162, 1181–1187. [Google Scholar] [CrossRef]
- Franzese, A.; Borrelli, O.; Corrado, G.; Rea, P.; Di Nardo, G.; Grandinetti, A.L.; Dito, L.; Cucchiara, S. Domperidone is more effective than cisapride in children with diabetic gastroparesis. Aliment. Pharmacol. 2002, 16, 951–957. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, L.; Rosen, R.; Manfredi, M.; Nurko, S. Endoscopic intrapyloric injection of botulinum toxin A in the treatment of children with gastroparesis: A retrospective, open-label study. Gastrointest. Endosc. 2012, 75, 302–309. [Google Scholar] [CrossRef] [Green Version]
- Lu, P.L.; Teich, S.; Di Lorenzo, C.; Lorenzo, C.D.; Skaggs, B.; Alhajj, M.; Mousa, H.M. Improvement of quality of life and symptoms after gastric electrical stimulation in children with functional dyspepsia. Neurogastroenterol. Motil. 2013, 25, 567-e456. [Google Scholar] [CrossRef]
- Islam, S.; McLaughlin, J.; Pierson, J.; Jolley, C.; Kedar, A.; Abell, T. Long-term outcomes of gastric electrical stimulation in children with gastroparesis. J. Pediatr. Surg. 2016, 51, 67–71. [Google Scholar] [CrossRef]
- Islam, S. Gastroparesis in children. Curr. Opin. Pediatr. 2015, 27, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Richards, R.D.; Davenport, K.; McCallum, R.W. The treatment of idiopathic and diabetic gastroparesis with acute intravenous and chronic oral erythromycin. Am. J. Gastroenterol. 1993, 88, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Arts, J.; Holvoet, L.; Caenepeel, P.; Bisschops, R.; Sifrim, D.; Verbeke, K.; Janssens, J.; Tack, J. Clinical trial: A randomized-controlled crossover study of intrapyloric injection of botulinum toxin in gastroparesis. Aliment. Pharmacol. 2007, 26, 1251–1258. [Google Scholar] [CrossRef] [PubMed]
- Friedenberg, F.K.; Palit, A.; Parkman, H.P.; Hanlon, A.; Nelson, D.B. Botulinum toxin A for the treatment of delayed gastric emptying. Am. J. Gastroenterol. 2008, 103, 416–423. [Google Scholar] [CrossRef]
- Caldaro, T.; Garganese, M.C.; Torroni, F.; Ciofetta, G.; De Angelis, P.; di Abriola, G.F.; Foschia, F.; Rea, F.; Romeo, E.; Dall’Oglio, L. Delayed gastric emptying and typical scintigraphic gastric curves in children with gastroesophageal reflux disease: Could pyloromyotomy improve this condition? J. Pediatr. Surg. 2011, 46, 863–869. [Google Scholar] [CrossRef]
- Lu, P.L.; Di Lorenzo, C. Neurostimulation of the gastrointestinal tract in children. Curr. Opin. Pediatr. 2016, 28, 631–637. [Google Scholar] [CrossRef]
- Ducrotte, P.; Coffin, B.; Bonaz, B.; Fontaine, S.; Bruley Des Varannes, S.; Zerbib, F.; Caiazzo, R.; Grimaud, J.C.; Mion, F.; Hadjadj, S.; et al. Gastric electrical stimulation reduces refractory vomiting in a randomized crossover trial. Gastroenterology 2020, 158, 506–514. [Google Scholar] [CrossRef] [Green Version]
- Abell, T.L.; Kedar, A.; Stocker, A.; Beatty, K.; McElmurray, L.; Hughes, M.; Rashed, H.; Kennedy, W.; Wendelschafer-Crabb, G.; Yang, X.; et al. Gastroparesis syndromes: Response to electrical stimulation. Neurogastroenterol. Motil. 2019, 31, e13534. [Google Scholar] [CrossRef]
- Setya, A.; Nair, P.; Cheng, S. Gastric electrical stimulation: An emerging therapy for children with intractable gastroparesis. World J. Gastroenterol. 2019, 25, 6880–6889. [Google Scholar] [CrossRef]
- Parkman, H.P.; Yamada, G.; Van Natta, M.L.; Yates, K.; Hasler, W.L.; Sarosiek, I.; Grover, M.; Schey, R.; Abell, T.L.; Koch, K.L.; et al. Ethnic, racial, and sex differences in etiology, symptoms, treatment, and symptom outcomes of patients with gastroparesis. Clin. Gastroenterol. Hepatol. 2019, 17, 1489–1499. [Google Scholar] [CrossRef]
- Sigurdsson, L.; Flores, A.; Putnam, P.E.; Hyman, P.E.; Di Lorenzo, C. Postviral gastroparesis: Presentation, treatment, and outcome. J. Pediatr. 1997, 131, 751–754. [Google Scholar] [CrossRef]

{kind=link}
Table 1.
Tests used to measure gastric emptying in children.
| Test | Advantages | Disadvantages |
|---|---|---|
| Gastric emptying scintigraphy (GES) |
|
|
| Gastric emptying breath test (GEBT) |
|
|
| Wireless motility capsule (WMC) |
|
|
Table 2.
Summary of the treatments used for children with gastroparesis.
| Treatment | Description | Outcomes |
|---|---|---|
| Dietary modification |
|
|
| Metoclopramide |
|
|
| Domperidone |
| |
| Erythromycin |
|
|
| Intrapyloric botulinum toxin injection |
|
|
| Gastric electrical stimulation |
|
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Lu, P.L.; Di Lorenzo, C. Gastroparesis in the Pediatric Patient: Children Are Not Little Adults. Gastrointest. Disord. 2020, 2, 86-95. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord2020008
AMA Style
Lu PL, Di Lorenzo C. Gastroparesis in the Pediatric Patient: Children Are Not Little Adults. Gastrointestinal Disorders. 2020; 2(2):86-95. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord2020008
Chicago/Turabian StyleLu, Peter L., and Carlo Di Lorenzo. 2020. "Gastroparesis in the Pediatric Patient: Children Are Not Little Adults" Gastrointestinal Disorders 2, no. 2: 86-95. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord2020008