Standardization of a Radiofrequency Ablation Tool in an Ex-Vivo Porcine Liver Model

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animal Model
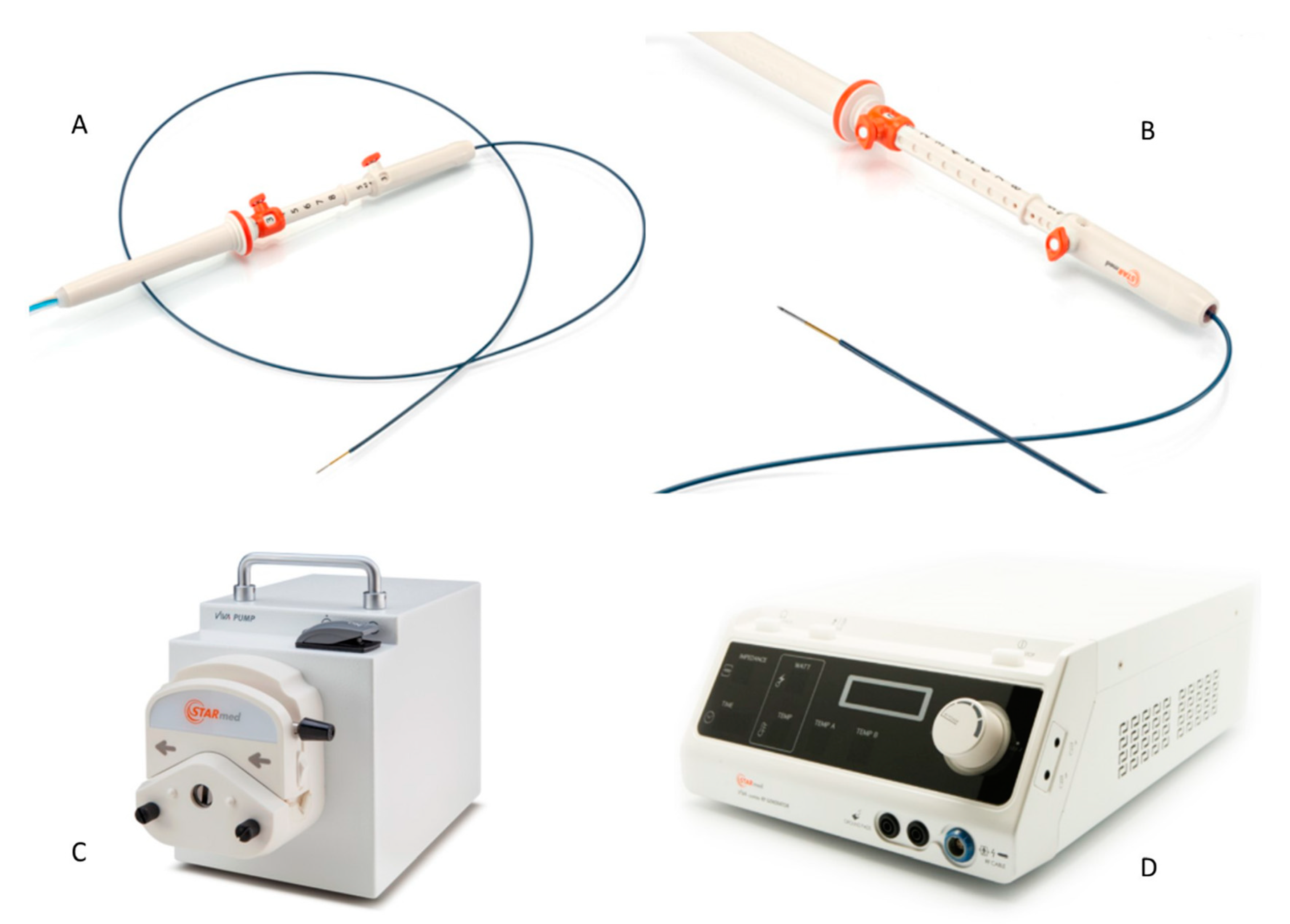
2.2. RFA System
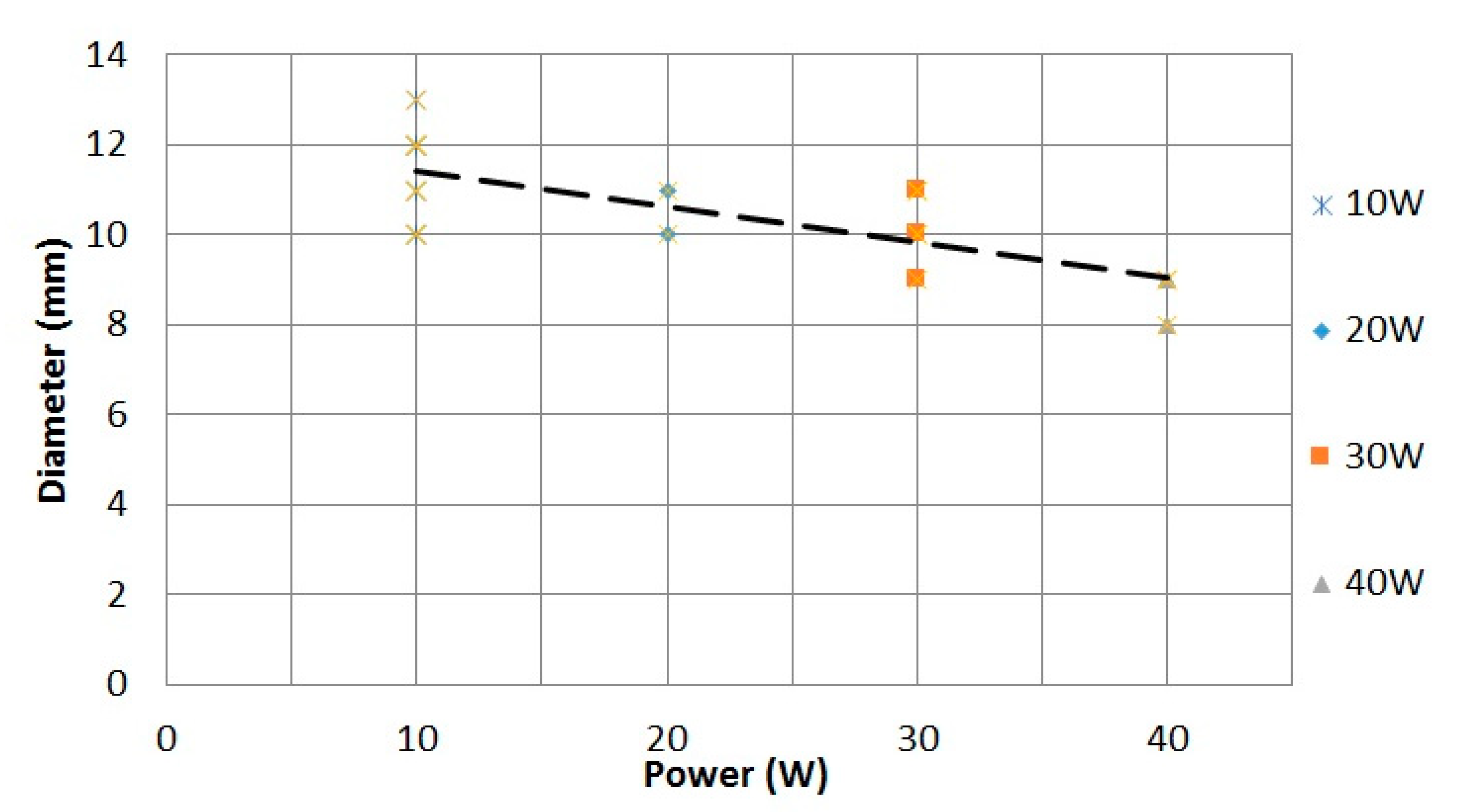
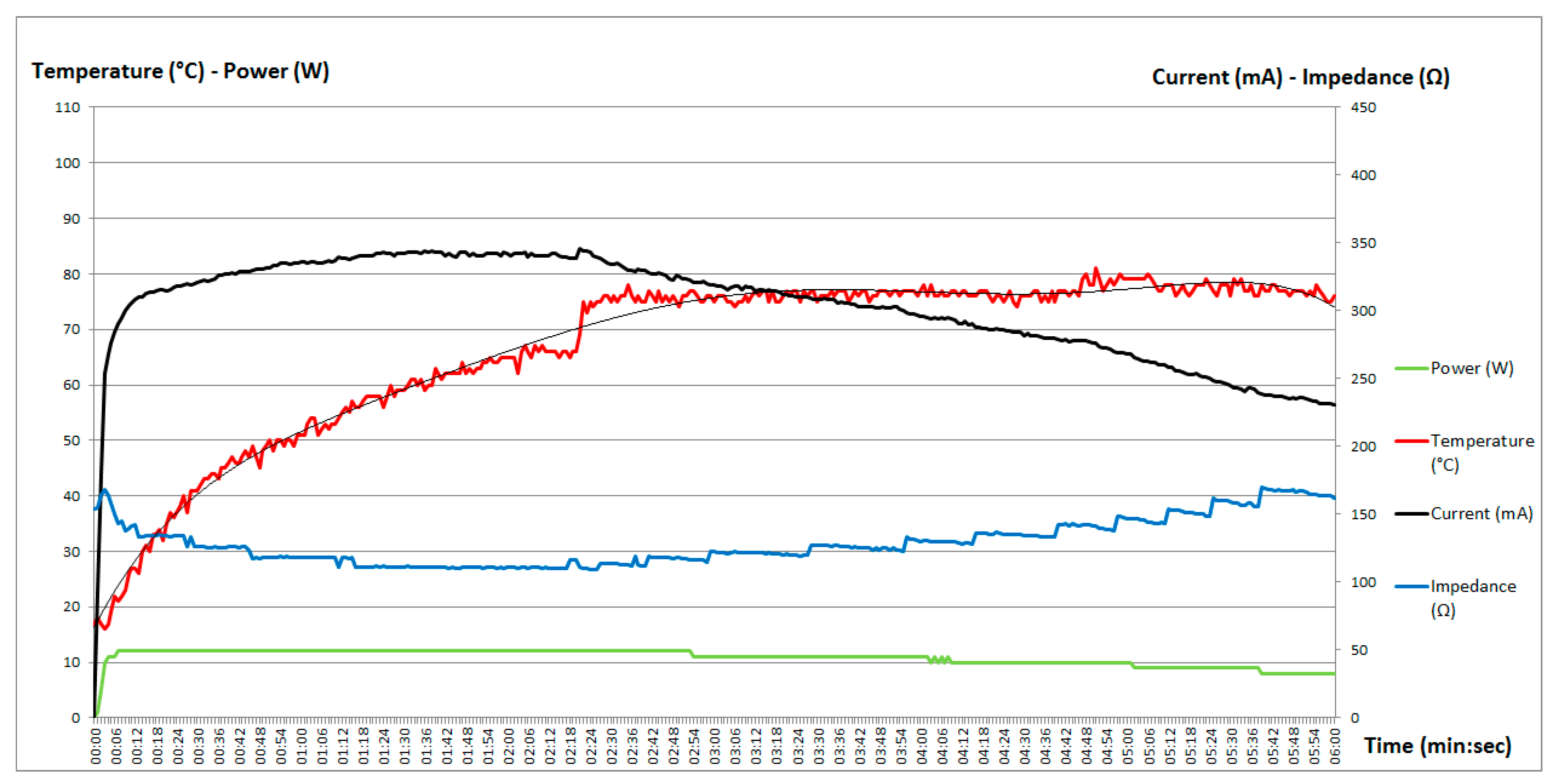
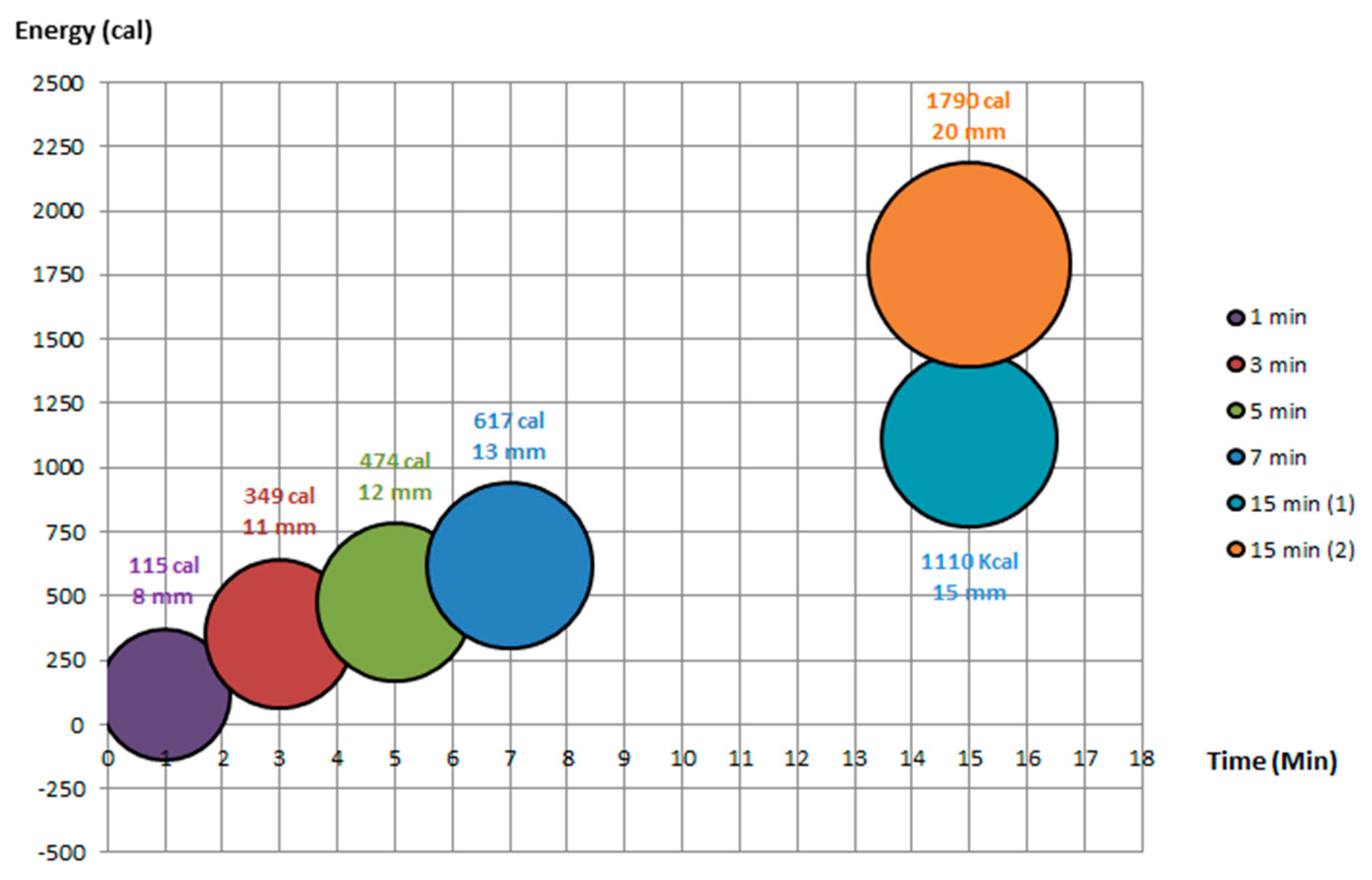
2.3. Ablation Setting
2.4. Statistics
3. Results
3.1. Total Ablated Area
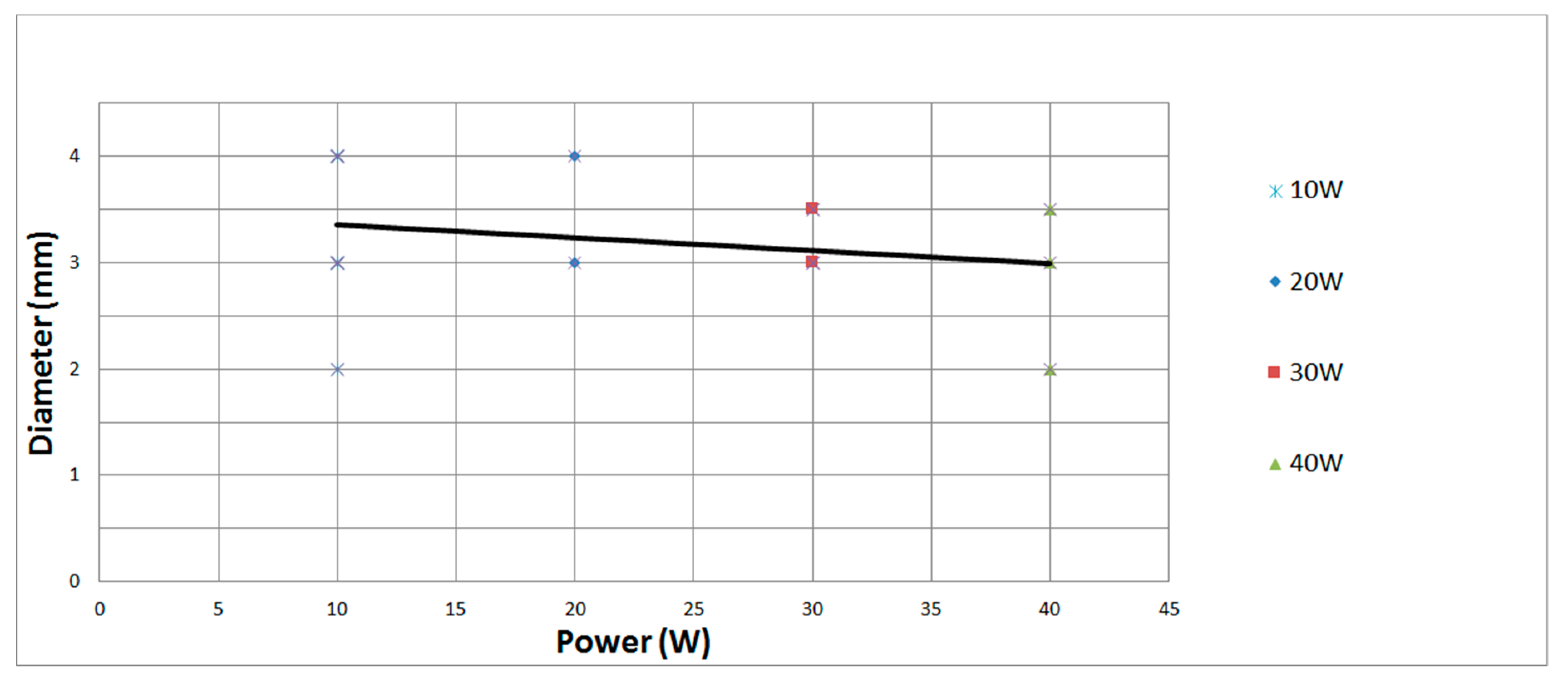
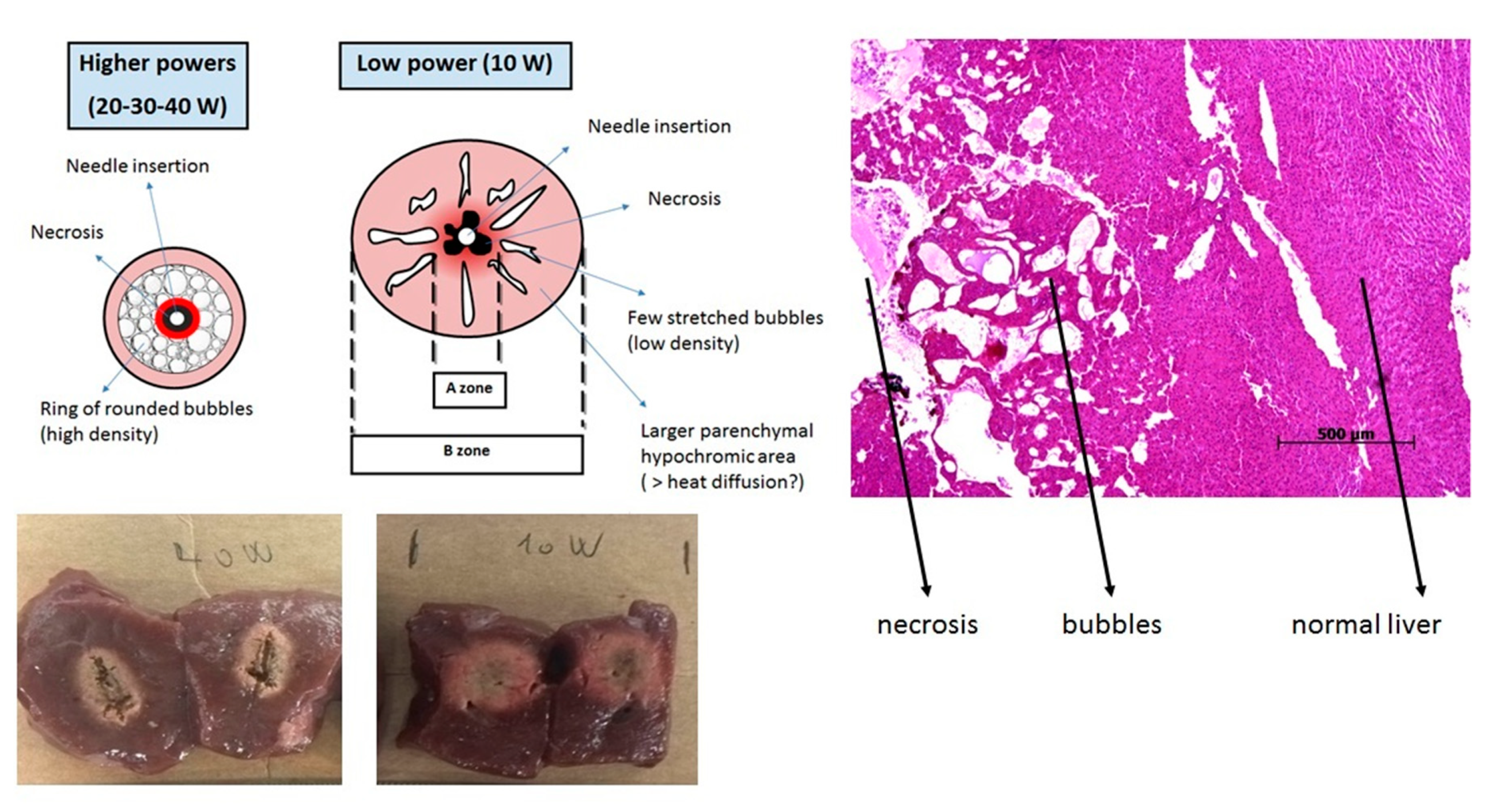
3.2. Area of Coagulative Necrosis
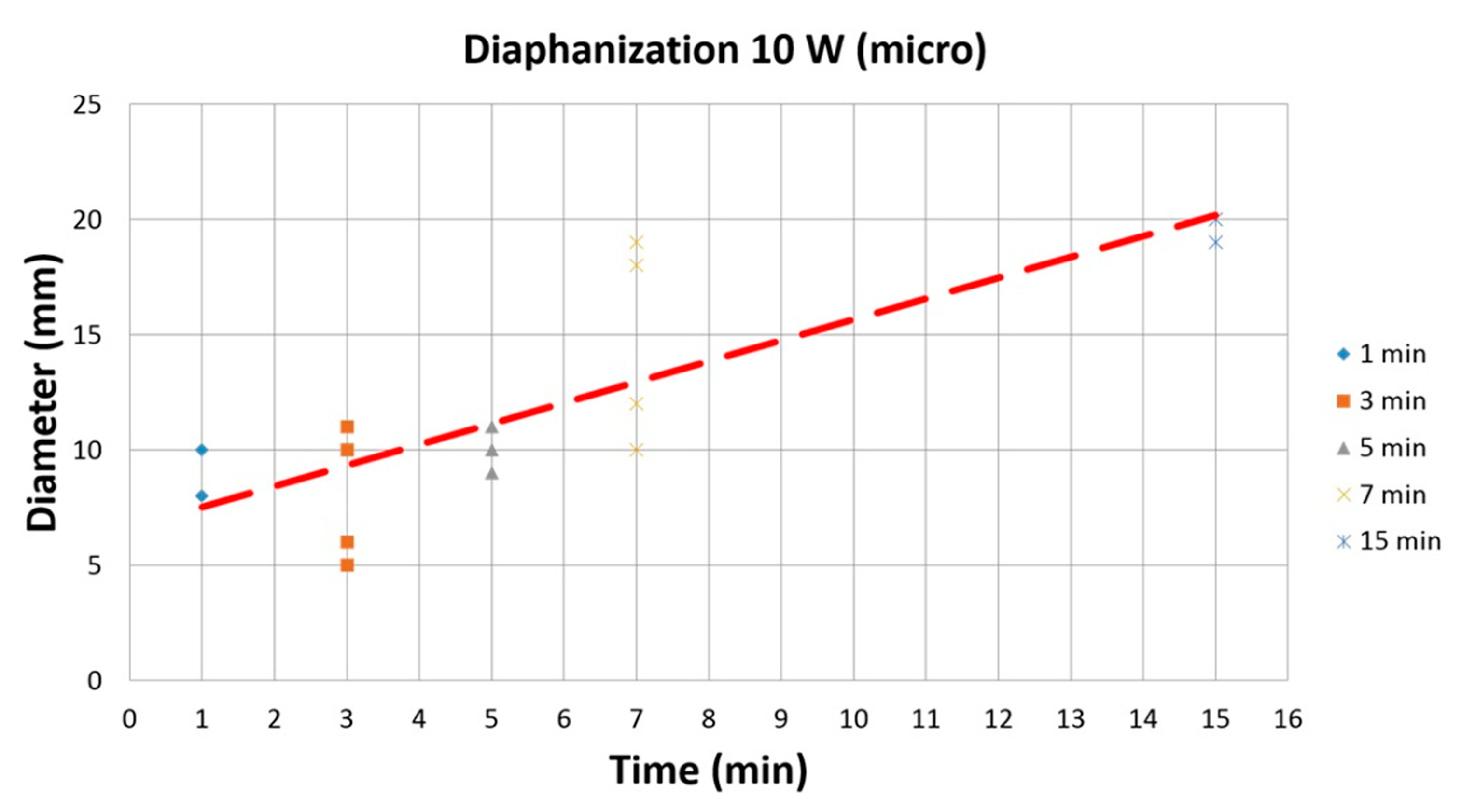
3.3. Diaphanization Area
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Paiella, S.; Salvia, R.; Ramera, M.; Girelli, R.; Frigerio, I.; Giardino, A.; Allegrini, V.; Bassi, C. Local Ablative Strategies for Ductal Pancreatic Cancer (Radiofrequency Ablation, Irreversible Electroporation): A Review. Gastroenterol. Res. Pract. 2016, 2016, 4508376. [Google Scholar] [CrossRef] [Green Version]
- Chu, K.F.; Dupuy, D.E. Thermal ablation of tumours: Biological mechanisms and advances in therapy. Nat. Rev. Cancer 2014, 14, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Wright, A.S.; Sampson, L.A.; Warner, T.F.; Mahvi, D.M.; Lee, F.T., Jr. Radiofrequency versus microwave ablation in a hepatic porcine model. Radiology 2005, 236, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Signoretti, M.; Valente, R.; Repici, A.; Fave, G.D.; Capurso, G.; Carrara, S. Endoscopy-guided ablation of pancreatic lesions: Technical possibilities and clinical outlook. World J. Gastrointest. Endosc. 2017, 9, 41–54. [Google Scholar] [CrossRef]
- Kim, H.J.; Seo, D.W.; Hassanuddin, A.; Kim, S.-H.; Chae, H.J.; Jang, J.W.; Park, D.H.; Lee, S.S.; Lee, S.-K.; Kim, M.-H. EUS-guided radiofrequency ablation of the porcine pancreas. Gastrointest. Endosc. 2012, 76, 1039–1043. [Google Scholar] [CrossRef] [PubMed]
- Song, T.J.; Seo, D.W.; Lakhtakia, S.; Reddy, N.; Oh, D.W.; Park, D.H.; Lee, S.S.; Lee, S.K.; Kim, M.-H. Initial experience of EUS-guided radiofrequency ablation of unresectable pancreatic cancer. Gastrointest. Endosc. 2016, 83, 440–443. [Google Scholar] [CrossRef]
- Lakhtakia, S.; Ramchandani, M.; Galasso, D.; Gupta, R.; Venugopal, S.; Kalpala, R.; Reddy, D.N. EUS-guided radiofrequency ablation for management of pancreatic insulinoma by using a novel needle electrode (with videos). Gastrointest. Endosc. 2016, 83, 234–239. [Google Scholar] [CrossRef]
- Armellini, E.; Crinò, S.F.; Ballarè, M.; Occhipinti, P. Endoscopic ultrasound-guided radiofrequency ablation of a pancreatic neuroendocrine tumor. Endoscopy 2015, 47. [Google Scholar] [CrossRef] [Green Version]
- Crinò, S.F.; D’Onofrio, M.; Bernardoni, L.; Frulloni, L.; Iannelli, M.; Malleo, G.; Paiella, S.; Larghi, A.; Gabbrielli, A. EUS-guided Radiofrequency Ablation (EUS-RFA) of Solid Pancreatic Neoplasm Using an 18-gauge Needle Electrode: Feasibility, Safety, and Technical Success. J. Gastrointest. Liver Dis. 2018, 27, 67–72. [Google Scholar] [CrossRef] [Green Version]
- Scopelliti, F.; Pea, A.; Conigliaro, R.; Butturini, G.; Frigerio, I.; Regi, P.; Giardino, A.; Bertani, H.; Paini, M.; Pederzoli, P.; et al. Technique, safety, and feasibility of EUS-guided radiofrequency ablation in unresectable pancreatic cancer. Surg. Endosc. 2018, 32, 4022–4028. [Google Scholar] [CrossRef]
- Barthet, M.; Giovannini, M.; Lesavre, N.; Boustiere, C.; Napoleon, B.; Koch, S.; Gasmi, M.; Vanbiervliet, G.; Gonzalez, J.-M. Endoscopic ultrasound-guided radiofrequency ablation for pancreatic neuroendocrine tumors and pancreatic cystic neoplasms: A prospective multicenter study. Endoscopy 2019, 51, 836–842. [Google Scholar] [CrossRef] [PubMed]
- Carrara, S.; Arcidiacono, P.G.; Albarello, L.; Addis, A.; Enderle, M.D.; Boemo, C.; Campagnol, M.; Ambrosi, A.; Doglioni, C.; Testoni, P.A. Endoscopic ultrasound-guided application of a new hybrid cryotherm probe in porcine pancreas: A preliminary study. Endoscopy 2008, 40, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Carrara, S.; Arcidiacono, P.G.; Albarello, L.; Addis, A.; Enderle, M.D.; Boemo, C.; Neugebauer, A.; Campagnol, M.; Doglioni, C.; Testoni, P.A. Endoscopic ultrasound-guided application of a new internally gas cooled radiofrequency ablation probe in the liver and spleen of an animal model: A preliminary study. Endoscopy 2008, 40, 759–763. [Google Scholar] [CrossRef] [PubMed]
- Edler, L. Statistical requirements of phase I studies. Onkologie 1990, 13, 90–95. [Google Scholar] [CrossRef]
- Shibata, T.; Niinobu, T.; Ogata, N. Comparison of the effects of in-vivo thermal ablation of pig liver by microwave and radiofrequency coagulation. J. Hepatobiliary Pancreat. Surg. 2000, 7, 592–598. [Google Scholar] [CrossRef]
- Rustagi, T.; Gleeson, F.C.; Abu Dayyeh, B.K.; Topazian, M.D.; Levy, M.J. Evaluation of Effects of Radiofrequency Ablation of Ex vivo Liver Using the 1-Fr Wire Electrode. J. Clin. Gastroenterol. 2018, 52, 168–171. [Google Scholar] [CrossRef]
- Itoi, T.; Isayama, H.; Sofuni, A.; Itokawa, F.; Tamura, M.; Watanabe, Y.; Moriyasu, F.; Kahaleh, M.; Habib, N.; Nagao, T.; et al. Evaluation of effects of a novel endoscopically applied radiofrequency ablation biliary catheter using an ex-vivo pig liver. J. Hepatobiliary Pancreat. Sci. 2012, 19, 543–547. [Google Scholar] [CrossRef]
- Carrara, S.; Petrone, M.C.; Testoni, P.A.; Arcidiacono, P.G. Tumors and new endoscopic ultrasound-guided therapies. World J. Gastrointest. Endosc. 2013, 5, 141–147. [Google Scholar] [CrossRef]
- Petrone, M.C.; Arcidiacono, P.G.; Carrara, S.; Albarello, L.; Enderle, M.D.; Neugebauer, A.; Boemo, C.; Doglioni, C.; Testoni, P.A. US-guided application of a new hybrid probe in human pancreatic adenocarcinoma: An ex vivo study. Gastrointest. Endosc. 2010, 71, 1294–1297. [Google Scholar] [CrossRef]
- Arcidiacono, P.G.; Carrara, S.; Reni, M.; Petrone, M.C.; Cappio, S.; Balzano, G.; Boemo, C.; Cereda, S.; Nicoletti, R.; Enderle, M.D.; et al. Feasibility and safety of EUS-guided cryothermal ablation in patients with locally advanced pancreatic cancer. Gastrointest. Endosc. 2012, 76, 1142–1151. [Google Scholar] [CrossRef]
- Barret, M.; Leblanc, S.; Rouquette, A.; Chaussade, S.; Terris, B.; Prat, F. EUS-guided pancreatic radiofrequency ablation: Preclinical comparison of two currently available devices in a pig model. Endosc. Int. Open 2019, 7, E138–E143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haen, S.P.; Pereira, P.L.; Salih, H.R.; Rammensee, H.-G.; Gouttefangeas, C. More than just tumor destruction: Immunomodulation by thermal ablation of cancer. Clin. Dev. Immunol. 2011, 2011, 160250. [Google Scholar] [CrossRef] [PubMed]
- Giardino, A.; Innamorati, G.; Ugel, S.; Perbellini, O.; Girelli, R.; Frigerio, I.; Regi, P.; Scopelliti, F.; Butturini, G.; Paiella, S.; et al. Immunomodulation after radiofrequency ablation of locally advanced pancreatic cancer by monitoring the immune response in 10 patients. Pancreatology 2017, 17, 962–966. [Google Scholar] [CrossRef] [PubMed]







© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rossi, G.; Petrone, M.C.; Capurso, G.; Albarello, L.; Testoni, S.G.G.; Archibugi, L.; Schiavo Lena, M.; Doglioni, C.; Arcidiacono, P.G. Standardization of a Radiofrequency Ablation Tool in an Ex-Vivo Porcine Liver Model. Gastrointest. Disord. 2020, 2, 300-309. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord2030027
Rossi G, Petrone MC, Capurso G, Albarello L, Testoni SGG, Archibugi L, Schiavo Lena M, Doglioni C, Arcidiacono PG. Standardization of a Radiofrequency Ablation Tool in an Ex-Vivo Porcine Liver Model. Gastrointestinal Disorders. 2020; 2(3):300-309. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord2030027
Chicago/Turabian StyleRossi, Gemma, Maria Chiara Petrone, Gabriele Capurso, Luca Albarello, Sabrina Gloria Giulia Testoni, Livia Archibugi, Marco Schiavo Lena, Claudio Doglioni, and Paolo Giorgio Arcidiacono. 2020. "Standardization of a Radiofrequency Ablation Tool in an Ex-Vivo Porcine Liver Model" Gastrointestinal Disorders 2, no. 3: 300-309. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord2030027