
Colorectal Cancer Screening: Have We Addressed Concerns and Needs of the Target Population?

 ,
,  ,
,
Abstract
:1. Introduction
2. Results
2.1. Population Preference for CRC Screening Tests
2.1.1. Preference for Colonoscopy
2.1.2. Preference for Stool-Based Tests (FOBT and sDNA)
2.1.3. Preference for Computed Tomography Colonography (CTC)
2.1.4. Preference for Blood Test (SEPT9) and Capsule Colonoscopy (Nanopill)
2.2. Individuals’ Characteristics Influencing Test Preference
2.2.1. Gender
2.2.2. Age
2.2.3. Screening Experience
2.2.4. Ethnicity
2.2.5. Education Level and Belief
2.2.6. Perceived Risk of CRC
2.2.7. Insurance Status
2.2.8. Health Status
2.3. Intention to Participate and Actual Participation in Relation to the Stated Preference
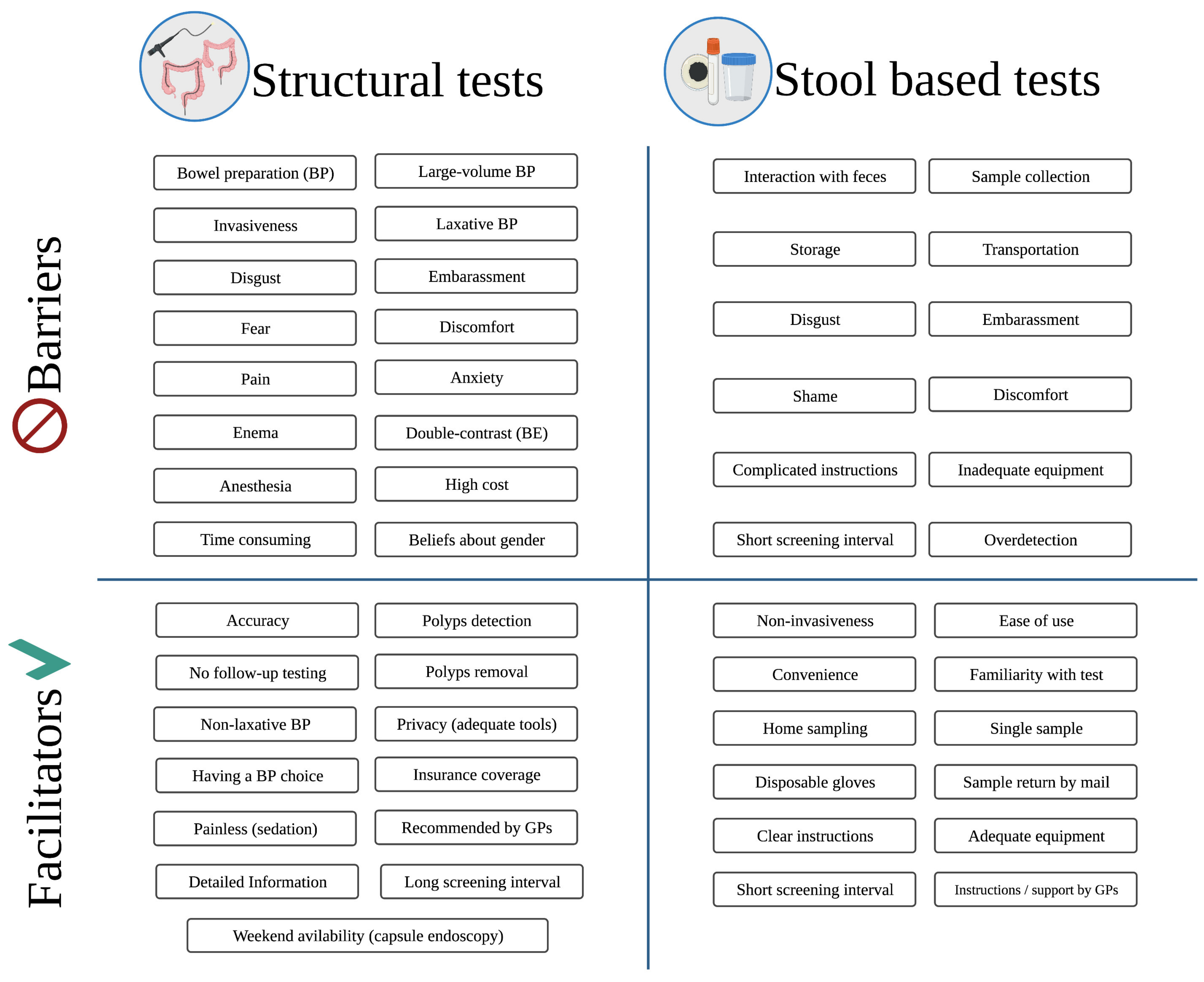
2.4. Barriers to Participation in CRC Screening and Potential Addressing Measures
2.4.1. Visual (or Structural) Tests: Colonoscopy, Sigmoidoscopy, CTC and Capsule Colonoscopy
Barriers to Screening with Visual Tests
Preference for Provider’s Gender
Potential Addressing Measures for Increasing Participation with Visual Tests
2.4.2. Stool-Based Tests: FIT/gFOBT and sDNA Test
Barriers to Screening with Stool-Based Tests
Potential Addressing Measures for Increasing Participation with Stool-Based Tests
2.4.3. General Preferences
Other Barriers to CRC Screening in General
Other Potential Addressing Measures for Increasing Participation in CRC Screening
2.5. Willingness to Pay, Costs and Rewards in CRC Screening
3. Discussion and Conclusions
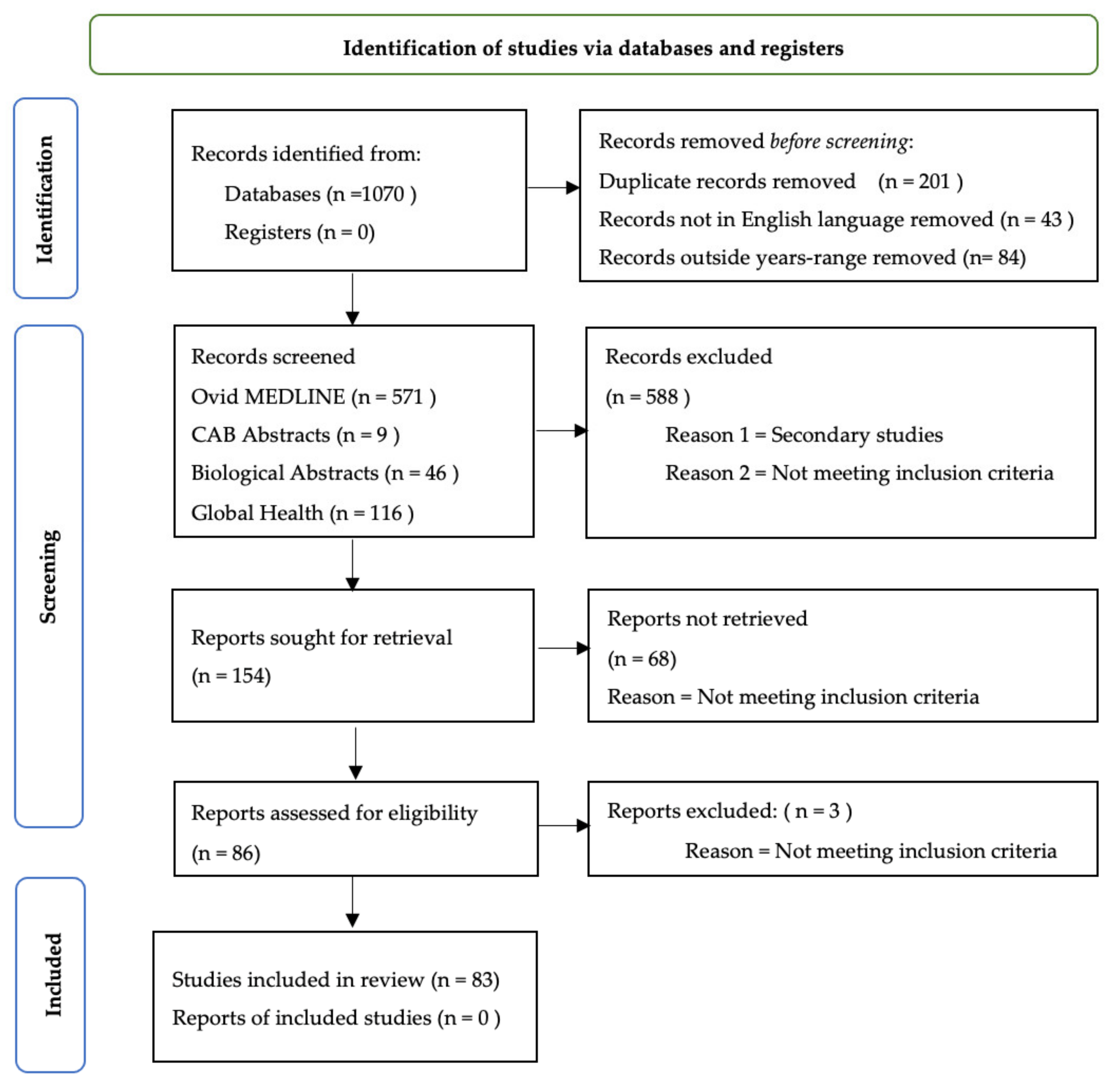
4. Methods
- Ovid MEDLINE® ALL;
- Biological Abstracts;
- CAB Abstracts;
- Global Health
- Population: General population or population at average risk for colorectal cancer (e.g., studies on subjects with genetic/familial risk or cancer patients only were excluded).
- Phenomena of interest: Preference, acceptability, compliance or willingness to undergo one or more screening tests, measured by survey, questionnaire or interview. Only direct measurement of participants’ preferences was taken into consideration (e.g., studies employing methodologies investigating factors associated with uptake as an indirect measurement of participants’ preferences were not included).
- Context: Colorectal cancer screening (i.e., studies on other types of gastrointestinal cancers were excluded).
- Other considerations: We restricted our search to only original articles (reviews, systematic reviews, meta-analyses and other types of secondary research were excluded), written in English and published between January 2005 and July 2021.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Xi, Y.; Xu, P. Global colorectal cancer burden in 2020 and projections to 2040. Transl. Oncol. 2021, 14, 101174. [Google Scholar] [CrossRef] [PubMed]
- Brenner, H.; Stock, C.; Hoffmeister, M. Effect of screening sigmoidoscopy and screening colonoscopy on colorectal cancer incidence and mortality: Systematic review and meta-analysis of randomised controlled trials and observational studies. BMJ 2014, 348, g2467. [Google Scholar] [CrossRef] [Green Version]
- Hewitson, P.; Glasziou, P.; Watson, E.; Towler, B.; Irwig, L. Cochrane systematic review of colorectal cancer screening using the fecal occult blood test (hemoccult): An update. Am. J. Gastroenterol. 2008, 103, 1541–1549. [Google Scholar] [CrossRef] [PubMed]
- Giorgi Rossi, P.; Vicentini, M.; Sacchettini, C.; Di Felice, E.; Caroli, S.; Ferrari, F.; Mangone, L.; Pezzarossi, A.; Roncaglia, F.; Campari, C.; et al. Impact of Screening Program on Incidence of Colorectal Cancer: A Cohort Study in Italy. Am. J. Gastroenterol. 2015, 110, 1359–1366. [Google Scholar] [CrossRef]
- Von Karsa, L.; Patnick, J.; Segnan, N.; Atkin, W.; Halloran, S.; Lansdorp-Vogelaar, I.; Malila, N.; Minozzi, S.; Moss, S.; Quirke, P.; et al. European guidelines for quality assurance in colorectal cancer screening and diagnosis: Overview and introduction to the full Supplement publication. Endoscopy 2013, 45, 51–59. [Google Scholar] [CrossRef] [Green Version]
- Wolf, A.M.D.; Fontham, E.T.H.; Church, T.R.; Flowers, C.R.; Guerra, C.E.; LaMonte, S.J.; Etzioni, R.; McKenna, M.T.; Oeffinger, K.C.; Shih, Y.T.; et al. Colorectal cancer screening for average-risk adults: 2018 guideline update from the American Cancer Society. CA Cancer J. Clin. 2018, 68, 250–281. [Google Scholar] [CrossRef] [PubMed]
- Segnan, N.; Patnick, J.; von Karsa, L. European Guidelines for Quality Assurance in Colorectal Cancer Screening and Diagnosis, 1st ed.; Publications Office of the European Union: Luxembourg, 2010. [Google Scholar]
- Ponti, A.; Anttila, A.; Ronco, G.; Senore, C.; Basu, P.; Segnan, N.; Tomatis, M.; Žakelj, M.P.; Dillner, J.; Fernan, M.; et al. Cancer Screening in the European Union. Report on the Implementation of Council Recommendation on Cancer Screening; European Commission: Brussels, Belgium, 2017; Available online: https://ec.europa.eu/health/sites/health/files/major_chronic_diseases/docs/2017_cancerscreening_2ndreportimplementation_en.pdf (accessed on 16 February 2021).
- Geiger, T.M.; Ricciardi, R. Screening options and recommendations for colorectal cancer. Clin. Colon. Rectal Surg. 2009, 22, 209–217. [Google Scholar] [CrossRef] [Green Version]
- Levin, B.; Lieberman, D.A.; McFarland, B.; Smith, R.A.; Brooks, D.; Andrews, K.S.; Dash, C.; Giardiello, F.M.; Glick, S.; Levin, T.R.; et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: A joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. CA Cancer J. Clin. 2008, 58, 130–160. [Google Scholar] [CrossRef] [Green Version]
- Worthington, J.; Lew, J.B.; Feletto, E.; Holden, C.A.; Worthley, D.L.; Miller, C.; Canfell, K. Improving Australian National Bowel Cancer Screening Program outcomes through increased participation and cost-effective investment. PLoS ONE 2020, 15, e0227899. [Google Scholar] [CrossRef] [Green Version]
- Moutel, G.; Duchange, N.; Lievre, A.; Orgerie, M.B.; Jullian, O.; Sancho-Garnier, H.; Darquy, S. Low participation in organized colorectal cancer screening in France: Underlying ethical issues. Eur. J. Cancer Prev. 2019, 28, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Ni, K.; O’Connell, K.; Anand, S.; Yakoubovitch, S.C.; Kwon, S.C.; de Latour, R.A.; Wallach, A.B.; Sherman, S.E.; Du, M.; Liang, P.S. Low Colorectal Cancer Screening Uptake and Persistent Disparities in an Underserved Urban Population. Cancer Prev. Res. 2020, 13, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Palmer, C.K.; Thomas, M.C.; McGregor, L.M.; von Wagner, C.; Raine, R. Understanding low colorectal cancer screening uptake in South Asian faith communities in England—A qualitative study. BMC Public Health 2015, 15, 998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alberti, L.R.; Garcia, D.P.; Coelho, D.L.; De Lima, D.C.; Petroianu, A. How to improve colon cancer screening rates. World J. Gastrointest. Oncol. 2015, 7, 484–491. [Google Scholar] [CrossRef] [PubMed]
- Dougherty, M.K.; Brenner, A.T.; Crockett, S.D.; Gupta, S.; Wheeler, S.B.; Coker-Schwimmer, M.; Cubillos, L.; Malo, T.; Reuland, D.S. Evaluation of Interventions Intended to Increase Colorectal Cancer Screening Rates in the United States: A Systematic Review and Meta-analysis. JAMA Intern. Med. 2018, 178, 1645–1658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inadomi, J.M.; Vijan, S.; Janz, N.K.; Fagerlin, A.; Thomas, J.P.; Lin, Y.V.; Munoz, R.; Lau, C.; Somsouk, M.; El-Nachef, N.; et al. Adherence to colorectal cancer screening: A randomized clinical trial of competing strategies. Arch. Intern. Med. 2012, 172, 575–582. [Google Scholar]
- Benning, T.M.; Dellaert, B.G.; Dirksen, C.D.; Severens, J.L. Preferences for potential innovations in non-invasive colorectal cancer screening: A labeled discrete choice experiment for a Dutch screening campaign. Acta Oncol. 2014, 53, 898–908. [Google Scholar] [CrossRef] [Green Version]
- Wong, M.C.; Ching, J.Y.; Chan, V.C.; Lam, T.Y.; Luk, A.K.; Ng, S.C.; Ng, S.S.; Sung, J.J. Informed choice vs. no choice in colorectal cancer screening tests: A prospective cohort study in real-life screening practice. Am. J. Gastroenterol. 2014, 109, 1072–1079. [Google Scholar] [CrossRef]
- Marshall, D.A.; Johnson, F.R.; Phillips, K.A.; Marshall, J.K.; Thabane, L.; Kulin, N.A. Measuring patient preferences for colorectal cancer screening using a choice-format survey. Value Health 2007, 10, 415–430. [Google Scholar] [CrossRef] [Green Version]
- Mansfield, C.; Tangka, F.K.; Ekwueme, D.U.; Smith, J.L.; Guy, G.P., Jr.; Li, C.; Hauber, A.B. Stated Preference for Cancer Screening: A Systematic Review of the Literature, 1990–2013. Prev. Chronic Dis. 2016, 13, E27. [Google Scholar] [CrossRef]
- Van Dam, L.; Hol, L.; de Bekker-Grob, E.W.; Steyerberg, E.W.; Kuipers, E.J.; Habbema, J.D.; Essink-Bot, M.L.; van Leerdam, M.E. What determines individuals’ preferences for colorectal cancer screening programmes? A discrete choice experiment. Eur. J. Cancer 2010, 46, 150–159. [Google Scholar] [CrossRef] [Green Version]
- Hol, L.; de Jonge, V.; van Leerdam, M.E.; van Ballegooijen, M.; Looman, C.W.N.; van Vuuren, A.J.; Reijerink, J.C.I.Y.; Habbema, J.D.F.; Essink-Bot, M.L.; Kuipers, E.J. Screening for colorectal cancer: Comparison of perceived test burden of guaiac-based faecal occult blood test, faecal immunochemical test and flexible sigmoidoscopy. Eur. J. Cancer 2010, 46, 2059–2066. [Google Scholar] [CrossRef]
- Cole, S.R.; Zajac, I.; Gregory, T.; Mehaffey, S.; Roosa, N.; Turnbull, D.; Esterman, A.; Young, G.P. Psychosocial variables associated with colorectal cancer screening in South Australia. Int. J. Behav. Med. 2011, 18, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Chapple, A.; Ziebland, S.; Hewitson, P.; McPherson, A. What affects the uptake of screening for bowel cancer using a faecal occult blood test (FOBt): A qualitative study. Soc. Sci. Med. 2008, 66, 2425–2435. [Google Scholar] [CrossRef] [PubMed]
- Wolf, R.L.; Basch, C.E.; Zybert, P.; Basch, C.H.; Ullman, R.; Shmukler, C.; King, F.; Neugut, A.I. Patient Test Preference for Colorectal Cancer Screening and Screening Uptake in an Insured Urban Minority Population. J. Community Health 2016, 41, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Moawad, F.J.; Maydonovitch, C.L.; Cullen, P.A.; Barlow, D.S.; Jenson, D.W.; Cash, B.D. CT colonography may improve colorectal cancer screening compliance. Am. J. Roentgenol. 2010, 195, 1118–1123. [Google Scholar] [CrossRef]
- DeBourcy, A.C.; Lichtenberger, S.; Felton, S.; Butterfield, K.T.; Ahnen, D.J.; Denberg, T.D. Community-based preferences for stool cards versus colonoscopy in colorectal cancer screening. J. Gen. Intern. Med. 2008, 23, 169–174. [Google Scholar] [CrossRef] [Green Version]
- Chatrath, H.; Rex, D.K. Potential screening benefit of a colorectal imaging capsule that does not require bowel preparation. J. Clin. Gastroenterol. 2014, 48, 52–54. [Google Scholar] [CrossRef] [PubMed]
- Schreuders, E.H.; Ruco, A.; Rabeneck, L.; Schoen, R.E.; Sung, J.J.; Young, G.P.; Kuipers, E.J. Colorectal cancer screening: A global overview of existing programmes. Gut 2015, 64, 1637–1649. [Google Scholar] [CrossRef]
- Redwood, D.G.; Blake, I.D.; Provost, E.M.; Kisiel, J.B.; Sacco, F.D.; Ahlquist, D.A. Alaska native patient and provider perspectives on the multitarget stool DNA test compared with colonoscopy for colorectal cancer screening. J. Prim. Care Community Health 2019, 10, 2150132719884295. [Google Scholar] [CrossRef]
- Ling, B.S.; Moskowitz, M.A.; Wachs, D.; Pearson, B.; Schroy, P.C. Attitudes Toward Colorectal Cancer Screening Tests. J. Gen. Intern. Med. 2001, 16, 822–830. [Google Scholar] [CrossRef] [PubMed]
- Schroy, P.C., 3rd; Duhovic, E.; Chen, C.A.; Heeren, T.C.; Lopez, W.; Apodaca, D.L.; Wong, J.B. Risk Stratification and Shared Decision Making for Colorectal Cancer Screening: A Randomized Controlled Trial. Med. Decis. Mak. 2016, 36, 526–535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McQueen, A.; Bartholomew, L.K.; Greisinger, A.J.; Medina, G.G.; Hawley, S.T.; Haidet, P.; Bettencourt, J.L.; Shokar, N.K.; Ling, B.S.; Vernon, S.W. Behind closed doors: Physician-patient discussions about colorectal cancer screening. J. Gen. Intern. Med. 2009, 24, 1228–1235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rimer, B.K.; Briss, P.A.; Zeller, P.K.; Chan, E.C.; Woolf, S.H. Informed decision making: What is its role in cancer screening? Cancer 2004, 101, 1214–1228. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, A.; Neefs, I.; Hoeck, S.; Peeters, M.; Van Hal, G. Towards Novel Non-Invasive Colorectal Cancer Screening Methods: A Comprehensive Review. Cancers 2021, 13, 1820. [Google Scholar] [CrossRef]
- Issa, I.A.; Noureddine, M. Colorectal cancer screening: An updated review of the available options. World J. Gastroenterol. 2017, 23, 5086–5096. [Google Scholar] [CrossRef]
- Bailey, J.R.; Aggarwal, A.; Imperiale, T.F. Colorectal Cancer Screening: Stool DNA and Other Noninvasive Modalities. Gut Liver 2016, 10, 15420. [Google Scholar] [CrossRef]
- Kuipers, E.J.; Rosch, T.; Bretthauer, M. Colorectal cancer screening—Optimizing current strategies and new directions. Nat. Rev. Clin. Oncol. 2013, 10, 130–142. [Google Scholar] [CrossRef]
- Ghanouni, A.; Smith, S.G.; Halligan, S.; Plumb, A.; Boone, D.; Yao, G.L.; Zhu, S.; Lilford, R.; Wardle, J.; von Wagner, C. Public preferences for colorectal cancer screening tests: A review of conjoint analysis studies. Expert Rev. Med. Devices 2013, 10, 489–499. [Google Scholar] [CrossRef] [Green Version]
- Moreno, C.C.; Jarrett, T.; Vey, B.L.; Mittal, P.K.; Krupinski, E.A.; Roberts, D.L. Patient Knowledge Regarding Colorectal Cancer Risk, Opinion of Screening, and Preferences for a Screening Test. Curr. Probl. Diagn. Radiol. 2019, 48, 50–52. [Google Scholar] [CrossRef]
- Cho, Y.H.; Kim, D.H.; Cha, J.M.; Jeen, Y.T.; Moon, J.S.; Kim, J.O.; Lee, S.K.; Cho, Y.K.; Im, J.P.; Jang, J.Y.; et al. Patients’ Preferences for Primary Colorectal Cancer Screening: A Survey of the National Colorectal Cancer Screening Program in Korea. Gut Liver 2017, 11, 821–827. [Google Scholar] [CrossRef] [Green Version]
- Jung, H.S.; Park, D.K.; Kim, M.J.; Yu, S.K.; Kwon, K.A.; Ku, Y.S.; Kim, Y.K.; Kim, J.H. A Comparison of Patient Acceptance and Preferences Between CT Colonography and Conventional Colonoscopy in Colorectal Cancer Screening. Korean J. Intern. Med. 2009, 24, 43–47. [Google Scholar] [CrossRef]
- Imaeda, A.; Bender, D.; Fraenkel, L. What Is Most Important to Patients when Deciding about Colorectal Screening? J. Gen. Intern. Med. 2010, 25, 688–693. [Google Scholar] [CrossRef] [Green Version]
- Omran, S.; Barakat, H.; Muliira, J.K.; Bashaireh, I.; Batiha, A.M. Assessment of Jordanian Patient’s Colorectal Cancer Awareness and Preferences towards CRC Screening: Are Jordanians Ready to Embrace CRC Screening? Asian Pac. J. Cancer Prev. 2015, 16, 4229–4235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calderwood, A.H.; Wasan, S.K.; Heeren, T.C.; Schroy, P.C., 3rd. Patient and Provider Preferences for Colorectal Cancer Screening: How Does CT Colonography Compare to Other Modalities? Int. J. Cancer Prev. 2011, 4, 307–338. [Google Scholar]
- Palmer, R.C.; Midgette, L.A.; Mullan, I.D. Colorectal cancer screening preferences among African Americans: Which screening test is preferred? J. Cancer Educ. 2010, 25, 577–581. [Google Scholar] [CrossRef]
- Sandoval, J.L.; Relecom, A.; Ducros, C.; Bulliard, J.L.; Arzel, B.; Guessous, I. Screening Status as a Determinant of Choice of Colorectal Cancer Screening Method: A Population-Based Informed Survey. Gastrointest. Tumors 2021, 8, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Schroy, P.C., 3rd; Lal, S.; Glick, J.T.; Robinson, P.A.; Zamor, P.; Heeren, T.C. Patient preferences for colorectal cancer screening: How does stool DNA testing fare? Am. J. Manag. Care 2007, 13, 393–400. [Google Scholar]
- Ruffin, M.T.I.; Creswell, J.W.; Jimbo, M.; Fetters, M.D. Factors influencing choices for colorectal cancer screening among previously unscreened African and Caucasian Americans: Findings from a triangulation mixed methods investigation. J. Community Health 2009, 34, 79–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hawley, S.T.; McQueen, A.; Bartholomew, L.K.; Greisinger, A.J.; Coan, S.P.; Myers, R.; Vernon, S.W. Preferences for colorectal cancer screening tests and screening test use in a large multispecialty primary care practice. Cancer 2012, 118, 2726–2734. [Google Scholar] [CrossRef] [Green Version]
- Lachter, J.; Leska-Aharoni, T.; Warum, D.; Eliakim, R. Overcoming barriers to colorectal cancer screening tests. Isr. Med. Assoc. J. 2008, 10, 621–626. [Google Scholar]
- Qumseya, B.J.; Tayem, Y.I.; Dasa, O.Y.; Nahhal, K.W.; Abu-Limon, I.M.; Hmidat, A.M.; Al-Shareif, A.F.; Hamadneh, M.K.; Riegert-Johnson, D.L.; Wallace, M.B. Barriers to colorectal cancer screening in Palestine: A national study in a medically underserved population. Clin. Gastroenterol. Hepatol. 2014, 12, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Parks, P.D.; Weiser, E.; Fischer, K.; Griffin, J.M.; Limburg, P.J.; Rutten, L.J.F. National survey of patient factors associated with colorectal cancer screening preferences. Cancer Prev. Res. 2021, 14, 603–614. [Google Scholar] [CrossRef]
- Bonello, B.; Ghanouni, A.; Bowyer, H.L.; MacRae, E.; Atkin, W.; Halloran, S.P.; Wardle, J.; von Wagner, C. Using a hypothetical scenario to assess public preferences for colorectal surveillance following screening-detected, intermediate-risk adenomas: Annual home-based stool test vs. triennial colonoscopy. BMC Gastroenterol. 2016, 16, 113. [Google Scholar] [CrossRef] [Green Version]
- Brenner, A.; Howard, K.; Lewis, C.; Sheridan, S.; Crutchfield, T.; Hawley, S.; Reuland, D.; Kistler, C.; Pignone, M. Comparing 3 values clarification methods for colorectal cancer screening decision-making: A randomized trial in the US and Australia. J. Gen. Intern. Med. 2014, 29, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Schroy, P.C., 3rd; Heeren, T.C. Patient perceptions of stool-based DNA testing for colorectal cancer screening. Am. J. Prev. Med. 2005, 28, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Phisalprapa, P.; Ngorsuraches, S.; Wanishayakorn, T.; Kositamongkol, C.; Supakankunti, S.; Chaiyakunapruk, N. Estimating the preferences and willingness-to-pay for colorectal cancer screening: An opportunity to incorporate the perspective of population at risk into policy development in Thailand. J. Med. Econ. 2021, 24, 226–233. [Google Scholar] [CrossRef]
- Xu, Y.; Levy, B.T.; Daly, J.M.; Bergus, G.R.; Dunkelberg, J.C. Comparison of patient preferences for fecal immunochemical test or colonoscopy using the analytic hierarchy process. BMC Health Serv. Res. 2015, 15, 175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghanouni, A.; Smith, S.G.; Halligan, S.; Plumb, A.; Boone, D.; Magee, M.S.; Wardle, J.; von Wagner, C. Public perceptions and preferences for CT colonography or colonoscopy in colorectal cancer screening. Patient Educ. Couns. 2012, 89, 116–121. [Google Scholar] [CrossRef]
- Marshall, D.A.; Johnson, F.R.; Kulin, N.A.; Ozdemir, S.; Walsh, J.M.; Marshall, J.K.; Van Bebber, S.; Phillips, K.A. How do physician assessments of patient preferences for colorectal cancer screening tests differ from actual preferences? A comparison in Canada and the United States using a stated-choice survey. Health Econ. 2009, 18, 1420–1439. [Google Scholar] [CrossRef]
- Gwede, C.K.; Koskan, A.M.; Quinn, G.P.; Davis, S.N.; Ealey, J.; Abdulla, R.; Vadaparampil, S.T.; Elliott, G.; Lopez, D.; Shibata, D.; et al. Patients’ perceptions of colorectal cancer screening tests and preparatory education in federally qualified health centers. J. Cancer Educ. 2015, 30, 294–300. [Google Scholar] [CrossRef] [Green Version]
- Berger, B.M.; Schroy, P.C., 3rd; Rosenberg, J.L.; Lai-Goldman, M.; Eisenberg, M.; Brown, T.; Rochelle, R.B.; Billings, P.R. Colorectal cancer screening using stool DNA analysis in clinical practice: Early clinical experience with respect to patient acceptance and colonoscopic follow-up of abnormal tests. Clin. Colorectal Cancer 2006, 5, 338–343. [Google Scholar] [CrossRef]
- Osborne, J.M.; Wilson, C.; Moore, V.; Gregory, T.; Flight, I.; Young, G.P. Sample preference for colorectal cancer screening tests: Blood or stool? Open J. Prev. Med. 2012, 2, 326–331. [Google Scholar] [CrossRef] [Green Version]
- De Bekker-Grob, E.W.; Hol, L.; Donkers, B.; van Dam, L.; Habbema, J.D.; van Leerdam, M.E.; Kuipers, E.J.; Essink-Bot, M.L.; Steyerberg, E.W. Labeled versus unlabeled discrete choice experiments in health economics: An application to colorectal cancer screening. Value Health 2010, 13, 315–323. [Google Scholar] [CrossRef] [Green Version]
- Cantor, S.B.; Volk, R.J.; Cass, A.R.; Gilani, J.; Spann, S.J. Psychological benefits of prostate cancer screening: The role of reassurance. Health Expect. 2002, 5, 104–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramezani Doroh, V.; Delavari, A.; Yaseri, M.; Emamgholipour Sefiddashti, S.; Akbarisari, A. Preferences of Iranian average risk population for colorectal cancer screening tests. Int. J. Health Care Qual. Assur. 2019, 32, 677–687. [Google Scholar] [CrossRef]
- Gareen, I.F.; Siewert, B.; Vanness, D.J.; Herman, B.; Johnson, C.D.; Gatsonis, C. Patient willingness for repeat screening and preference for CT colonography and optical colonoscopy in ACRIN 6664: The National CT Colonography trial. Patient Prefer. Adherence 2015, 9, 1043–1051. [Google Scholar] [CrossRef] [Green Version]
- Vargo, J.J. Doc, can I drive home? Am. J. Gastroenterol. 2009, 104, 1656–1657. [Google Scholar] [CrossRef]
- Riphaus, A.; Gstettenbauer, T.; Frenz, M.B.; Wehrmann, T. Quality of psychomotor recovery after propofol sedation for routine endoscopy: A randomized and controlled study. Endoscopy 2006, 38, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Green, A.R.; Peters-Lewis, A.; Percac-Lima, S.; Betancourt, J.R.; Richter, J.M.; Janairo, M.P.; Gamba, G.B.; Atlas, S.J. Barriers to screening colonoscopy for low-income Latino and white patients in an urban community health center. J. Gen. Intern. Med. 2008, 23, 834–840. [Google Scholar] [CrossRef] [Green Version]
- McLachlan, S.A.; Clements, A.; Austoker, J. Patients’ experiences and reported barriers to colonoscopy in the screening context—A systematic review of the literature. Patient Educ. Couns. 2012, 86, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Iannaccone, R.; Catalano, C.; Mangiapane, F.; Murakami, T.; Lamazza, A.; Fiori, E.; Schillaci, A.; Marin, D.; Nofroni, I.; Hori, M.; et al. Colorectal polyps: Detection with low-dose multi-detector row helical CT colonography versus two sequential colonoscopies. Radiology 2005, 237, 927–937. [Google Scholar] [CrossRef] [PubMed]
- Kato, T.; Muroya, T.; Goda, T.; Takabayashi, K.; Sasaki, K.; Takahashi, T.; Horita, S. Iatrogenic Colonic Perforation due to Computed Tomographic Colonography. Case Rep. Gastroenterol 2015, 9, 171–178. [Google Scholar] [CrossRef]
- Sosna, J.; Blachar, A.; Amitai, M.; Barmeir, E.; Peled, N.; Goldberg, S.N.; Bar-Ziv, J. Colonic perforation at CT colonography: Assessment of risk in a multicenter large cohort. Radiology 2006, 239, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Burling, D.; Halligan, S.; Slater, A.; Noakes, M.J.; Taylor, S.A. Potentially serious adverse events at CT colonography in symptomatic patients: National survey of the United Kingdom. Radiology 2006, 239, 464–471. [Google Scholar] [CrossRef]
- Pickhardt, P.J. Incidence of colonic perforation at CT colonography: Review of existing data and implications for screening of asymptomatic adults. Radiology 2006, 239, 313–316. [Google Scholar] [CrossRef] [PubMed]
- Levin, T.R.; Zhao, W.; Conell, C.; Seeff, L.C.; Manninen, D.L.; Shapiro, J.A.; Schulman, J. Complications of colonoscopy in an integrated health care delivery system. Ann. Intern. Med. 2006, 145, 880–886. [Google Scholar] [CrossRef]
- Zubarik, R.; Fleischer, D.E.; Mastropietro, C.; Lopez, J.; Carroll, J.; Benjamin, S.; Eisen, G. Prospective analysis of complications 30 days after outpatient colonoscopy. Gastrointest. Endosc. 1999, 50, 322–328. [Google Scholar] [CrossRef]
- Anderson, M.L.; Pasha, T.M.; Leighton, J.A. Endoscopic perforation of the colon: Lessons from a 10-year study. Am. J. Gastroenterol. 2000, 95, 3418–3422. [Google Scholar] [CrossRef]
- Laanani, M.; Coste, J.; Blotiere, P.O.; Carbonnel, F.; Weill, A. Patient, Procedure, and Endoscopist Risk Factors for Perforation, Bleeding, and Splenic Injury After Colonoscopies. Clin. Gastroenterol. Hepatol. 2019, 17, 719–727.e713. [Google Scholar] [CrossRef] [Green Version]
- Benazzato, L.; Zorzi, M.; Antonelli, G.; Guzzinati, S.; Hassan, C.; Fantin, A.; the Veneto Screening Endoscopists Working Group. Colonoscopy-related adverse events and mortality in an Italian organized colorectal cancer screening program. Endoscopy 2021, 53, 501–508. [Google Scholar] [CrossRef]
- Pickhardt, P.J.; Choi, J.R.; Hwang, I.; Butler, J.A.; Puckett, M.L.; Hildebrandt, H.A.; Wong, R.K.; Nugent, P.A.; Mysliwiec, P.A.; Schindler, W.R. Computed tomographic virtual colonoscopy to screen for colorectal neoplasia in asymptomatic adults. N. Engl. J. Med. 2003, 349, 2191–2200. [Google Scholar] [CrossRef] [Green Version]
- Johnson, C.D.; Chen, M.H.; Toledano, A.Y.; Heiken, J.P.; Dachman, A.; Kuo, M.D.; Menias, C.O.; Siewert, B.; Cheema, J.I.; Obregon, R.G.; et al. Accuracy of CT colonography for detection of large adenomas and cancers. N. Engl. J. Med. 2008, 359, 1207–1217. [Google Scholar] [CrossRef] [PubMed]
- Van Gelder, R.E.; Birnie, E.; Florie, J.; Schutter, M.P.; Bartelsman, J.F.; Snel, P.; Lameris, J.S.; Bonsel, G.J.; Stoker, J. CT colonography and colonoscopy: Assessment of patient preference in a 5-week follow-up study. Radiology 2004, 233, 328–337. [Google Scholar] [CrossRef] [PubMed]
- Akerkar, G.A.; Yee, J.; Hung, R.; McQuaid, K. Patient experience and preferences toward colon cancer screening: A comparison of virtual colonoscopy and conventional colonoscopy. Gastrointest. Endosc. 2001, 54, 310–315. [Google Scholar] [CrossRef]
- Zajac, I.T.; Duncan, A.; Turnbull, D.; Wilson, C.; Flight, I. Blood-based screening for bowel cancer may not resolve suboptimal screening participation in Australia. Aust. N. Z. J. Public Health 2016, 40, 337–341. [Google Scholar] [CrossRef] [Green Version]
- Osborne, J.M.; Flight, I.; Wilson, C.J.; Chen, G.; Ratcliffe, J.; Young, G.P. The impact of sample type and procedural attributes on relative acceptability of different colorectal cancer screening regimens. Patient Prefer. Adherence 2018, 12, 1825–1836. [Google Scholar] [CrossRef] [Green Version]
- Adler, A.; Geiger, S.; Keil, A.; Bias, H.; Schatz, P.; deVos, T.; Dhein, J.; Zimmermann, M.; Tauber, R.; Wiedenmann, B. Improving compliance to colorectal cancer screening using blood and stool based tests in patients refusing screening colonoscopy in Germany. BMC Gastroenterol. 2014, 14, 183. [Google Scholar] [CrossRef] [Green Version]
- Taber, J.M.; Aspinwall, L.G.; Heichman, K.A.; Kinney, A.Y. Preferences for blood-based colon cancer screening differ by race/ethnicity. Am. J. Health Behav. 2014, 38, 351–361. [Google Scholar] [CrossRef]
- Groothuis-Oudshoorn, C.G.; Fermont, J.M.; van Til, J.A.; Ijzerman, M.J. Public stated preferences and predicted uptake for genome-based colorectal cancer screening. BMC Med. Inform. Decis. Mak. 2014, 14, 18. [Google Scholar] [CrossRef] [Green Version]
- Clarke, N.; Sharp, L.; Osborne, A.; Kearney, P.M. Comparison of uptake of colorectal cancer screening based on fecal immunochemical testing (FIT) in males and females: A systematic review and meta-analysis. Cancer Epidemiol. Biomark. Prev. 2015, 24, 39–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hol, L.; de Bekker-Grob, E.W.; van Dam, L.; Donkers, B.; Kuipers, E.J.; Habbema, J.D.F.; Steyerberg, E.W.; van Leerdam, M.E.; Essink-Bot, M.L. Preferences for colorectal cancer screening strategies: A discrete choice experiment. Br. J. Cancer 2010, 102, 972–980. [Google Scholar] [CrossRef]
- Segnan, N.; Senore, C.; Andreoni, B.; Azzoni, A.; Bisanti, L.; Cardelli, A.; Castiglione, G.; Crosta, C.; Ederle, A.; Fantin, A.; et al. Comparing attendance and detection rate of colonoscopy with sigmoidoscopy and FIT for colorectal cancer screening. Gastroenterology 2007, 132, 2304–2312. [Google Scholar] [CrossRef]
- Denberg, T.D.; Melhado, T.V.; Coombes, J.M.; Beaty, B.L.; Berman, K.; Byers, T.E.; Marcus, A.C.; Steiner, J.F.; Ahnen, D.J. Predictors of nonadherence to screening colonoscopy. J. Gen. Intern. Med. 2005, 20, 989–995. [Google Scholar] [CrossRef] [Green Version]
- Wong, R.K.; Wong, M.L.; Chan, Y.H.; Feng, Z.; Wai, C.T.; Yeoh, K.G. Gender differences in predictors of colorectal cancer screening uptake: A national cross sectional study based on the health belief model. BMC Public Health 2013, 13, 677. [Google Scholar] [CrossRef] [Green Version]
- Shah, S.G.; Brooker, J.C.; Thapar, C.; Williams, C.B.; Saunders, B.P. Patient pain during colonoscopy: An analysis using real-time magnetic endoscope imaging. Endoscopy 2002, 34, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Park, D.I.; Kim, H.J.; Park, J.H.; Cho, Y.K.; Sohn, C.I.; Jeon, W.K.; Kim, B.I.; Ryu, S.H.; Sung, I.K. Factors affecting abdominal pain during colonoscopy. Eur. J. Gastroenterol. Hepatol. 2007, 19, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Ussui, V.M.; Silva, A.L.; Borges, L.V.; Silva, J.G.; Zeitune, J.M.; Hashimoto, C.L. What are the most important factors regarding acceptance to the colonoscopy?: Study of related tolerance parameters. ARQ Gastroenterol. 2013, 50, 23–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azaiza, F.; Cohen, M.; Awad, M.; Daoud, F. Factors associated with low screening for breast cancer in the Palestinian Authority: Relations of availability, environmental barriers, and cancer-related fatalism. Cancer 2010, 116, 4646–4655. [Google Scholar] [CrossRef]
- Jun, J.; Oh, K.M. Asian and Hispanic Americans’ cancer fatalism and colon cancer screening. Am. J. Health Behav. 2013, 37, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Powe, B.D. Fatalism among elderly African Americans. Effects on colorectal cancer screening. Cancer Nurs. 1995, 18, 385–392. [Google Scholar] [CrossRef]
- Ryan, M.; Watson, V.; Entwistle, V. Rationalising the ‘irrational’: A think aloud study of discrete choice experiment responses. Health Econ. 2009, 18, 321–336. [Google Scholar] [CrossRef] [PubMed]
- Van Bebber, S.L.; Liang, S.Y.; Phillips, K.A.; Marshall, D.; Walsh, J.; Kulin, N. Valuing personalized medicine: Willingness to pay for genetic testing for colorectal cancer risk. Pers. Med. 2007, 4, 341–350. [Google Scholar] [CrossRef] [PubMed]
- Howard, K.; Salkeld, G.; Pignone, M.; Hewett, P.; Cheung, P.; Olsen, J.; Clapton, W.; Roberts-Thomson, I.C. Preferences for CT colonography and colonoscopy as diagnostic tests for colorectal cancer: A discrete choice experiment. Value Health 2011, 14, 1146–1152. [Google Scholar] [CrossRef] [Green Version]
- Kroupa, R.; Ondrackova, M.; Kovalcikova, P.; Dastych, M.; Pavlik, T.; Kunovsky, L.; Dolina, J. Viewpoints of the target population regarding barriers and facilitators of colorectal cancer screening in the Czech Republic. World J. Gastroenterol. 2019, 25, 1132–1141. [Google Scholar] [CrossRef]
- Dyer, K.E.; Shires, D.A.; Flocke, S.A.; Hawley, S.T.; Jones, R.M.; Resnicow, K.; Shin, Y.; Lafata, J.E. Patient-Reported Needs Following a Referral for Colorectal Cancer Screening. Am. J. Prev. Med. 2019, 56, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Yusoff, H.M.; Daud, N.; Noor, N.M.; Rahim, A.A. Participation and barriers to colorectal cancer screening in Malaysia. Asian Pac. J. Cancer Prev. 2012, 13, 3983–3987. [Google Scholar] [CrossRef] [Green Version]
- Mansfield, C.; Ekwueme, D.U.; Tangka, F.K.L.; Brown, D.S.; Smith, J.L.; Guy, G.P., Jr.; Li, C.; Hauber, B. Colorectal Cancer Screening: Preferences, Past Behavior, and Future Intentions. Patient Patient-Cent. Outcomes Res. 2018, 11, 599–611. [Google Scholar] [CrossRef]
- Zapatier, J.A.; Kumar, A.R.; Perez, A.; Guevara, R.; Schneider, A. Preferences for ethnicity and sex of endoscopists in a Hispanic population in the United States. Gastrointest. Endosc. 2011, 73, 89–97. [Google Scholar] [CrossRef]
- Nicholson, F.B.; Korman, M.G. Acceptance of flexible sigmoidoscopy and colonoscopy for screening and surveillance in colorectal cancer prevention. J. Med. Screen. 2005, 12, 89–95. [Google Scholar] [CrossRef] [Green Version]
- Menees, S.B.; Inadomi, J.M.; Korsnes, S.; Elta, G.H. Women patients’ preference for women physicians is a barrier to colon cancer screening. Gastrointest. Endosc. 2005, 62, 219–223. [Google Scholar] [CrossRef]
- Zhou, Q.; Li, Y.; Liu, H.; Liang, Y.; Lin, G. Willingness to pay for colorectal cancer screening in Guangzhou. World J. Gastroenterol. 2018, 24, 4708–4715. [Google Scholar] [CrossRef] [PubMed]
- Gordon, N.P.; Green, B.B. Factors associated with use and non-use of the Fecal Immunochemical Test (FIT) kit for Colorectal Cancer Screening in Response to a 2012 outreach screening program: A survey study. BMC Public Health 2015, 15, 546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rex, D.K.; Lieberman, D.A. A survey of potential adherence to capsule colonoscopy in patients who have accepted or declined conventional colonoscopy. J. Clin. Gastroenterol. 2012, 46, 691–695. [Google Scholar] [CrossRef] [PubMed]
- Ghanouni, A.; Halligan, S.; Taylor, S.A.; Boone, D.; Plumb, A.; Stoffel, S.; Morris, S.; Yao, G.L.; Zhu, S.; Lilford, R.; et al. Quantifying public preferences for different bowel preparation options prior to screening CT colonography: A discrete choice experiment. BMJ Open 2014, 4, e004327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassan, C.; East, J.; Radaelli, F.; Spada, C.; Benamouzig, R.; Bisschops, R.; Bretthauer, M.; Dekker, E.; Dinis-Ribeiro, M.; Ferlitsch, M.; et al. Bowel preparation for colonoscopy: European Society of Gastrointestinal Endoscopy (ESGE) Guideline—Update 2019. Endoscopy 2019, 51, 775–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez de Miguel, C.; Serradesanferm, A.; Lopez-Ceron, M.; Carballal, S.; Pozo, A.; Balaguer, F.; Cardenas, A.; Fernandez-Esparrach, G.; Gines, A.; Gonzalez-Suarez, B.; et al. Ascorbic acid PEG-2L is superior for early morning colonoscopies in colorectal cancer screening programs: A prospective non-randomized controlled trial. Gastroenterol. Hepatol. 2015, 38, 62–70. [Google Scholar] [CrossRef]
- ASGE Standards of Practice Committee; Saltzman, J.R.; Cash, B.D.; Pasha, S.F.; Early, D.S.; Muthusamy, V.R.; Khashab, M.A.; Chathadi, K.V.; Fanelli, R.D.; Chandrasekhara, V.; et al. Bowel preparation before colonoscopy. Gastrointest. Endosc. 2015, 81, 781–794. [Google Scholar] [CrossRef]
- Mayo Clinic. Barium Enema. Available online: https://www.mayoclinic.org/tests-procedures/barium-enema/about/pac-20393008 (accessed on 23 August 2021).
- UCSF Department of Radiology & Biomedical Imaging. Prepare for a Virtual CT Colonoscopy Scan. Available online: https://radiology.ucsf.edu/patient-care/prepare/virutal-ct-colonoscopy (accessed on 23 August 2021).
- Chong, V.H. Gender preference and implications for screening colonoscopy: Impact of endoscopy nurses. World J. Gastroenterol. 2012, 18, 3590–3594. [Google Scholar] [CrossRef]
- Khara, H.S.; Suthar, D.; Bergenstock, M.; Berger, A.; McKee, J.L.; Stewart, D.; Theis, S.R.; Komar, M.; Johal, A.S.; Valencia Chavez, D.R.; et al. Identifying Gender Barriers for Colorectal Cancer Screening and Assessing the Need for a Multigender Endoscopy Team: A Prospective Multicenter Study. Am. J. Gastroenterol. 2021, 22, 22. [Google Scholar]
- Dreier, M.; Krueger, K.; Walter, U. Patient-rated importance of key information on screening colonoscopy in Germany: A survey of statutory health insurance members. BMJ Open 2018, 8, e019127. [Google Scholar] [CrossRef] [Green Version]
- Voiosu, A.; Tantau, A.; Garbulet, C.; Tantau, M.; Mateescu, B.; Baicus, C.; Voiosu, R.; Voiosu, T. Factors affecting colonoscopy comfort and compliance: A questionnaire based multicenter study. Rom. J. Intern. Med. 2014, 52, 151–157. [Google Scholar] [PubMed]
- Gurudu, S.R.; Li, F.; Fleischer, D.E.; Sharma, V.K.; Heigh, R.I.; Crowell, M.D.; Lee, M.; Hentz, J.G.; Leighton, J.A. Patient Preference and Acceptance with Sodium Phosphate Tablet Preparation for Colonoscopy. Dig. Dis. Sci. 2009, 54, 1555–1559. [Google Scholar] [CrossRef]
- Pin Erua-Gonsa Lvez, J.F.; Zambrano-Infantino, R.D.C.; Baptista, A.; Sulbaran, M.; Camaray, N. Assessment of tolerance and acceptability between mannitol solution and polyethylene glycol as bowel preparation for colonoscopy: A three-center study. Rev. Gastroenterol. Peru 2020, 40, 7–12. [Google Scholar] [CrossRef]
- Aamar, A.; Butt, Z.; Madhani, K.; Hussain, I.; Garsten, J.; Aslanian, H. Effect of a Novel Patient Garment on Perceived Privacy during Colonoscopy: A Simple Approach to Minimize Embarrassment. Gastroenterol. Res. Pract. 2019, 2019, 2467101. [Google Scholar] [CrossRef]
- Dignity Garments. How to Use Privacy Pants [YouTube Video]. 2016. Available online: https://www.youtube.com/watch?v=tK8QplfW-ME (accessed on 1 September 2021).
- Van den Bruel, A.; Jones, C.; Yang, Y.; Oke, J.; Hewitson, P. People’s willingness to accept overdetection in cancer screening: Population survey. BMJ 2015, 350, h980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bradley, D.T.; Treanor, C.; McMullan, C.; Owen, T.; Graham, A.; Anderson, D. Reasons for non-participation in the Northern Ireland Bowel Cancer Screening Programme: A qualitative study. BMJ Open 2015, 5, e008266. [Google Scholar] [CrossRef] [Green Version]
- Deutekom, M.; Rossum, L.G.M.v.; Rijn, A.F.v.; Laheij, R.J.F.; Fockens, P.; Bossuyt, P.M.M.; Dekker, E.; Jansen, J.B.M.J. Comparison of guaiac and immunological fecal occult blood tests in colorectal cancer screening: The patient perspective. Scand. J. Gastroenterol. 2010, 45, 1345–1349. [Google Scholar] [CrossRef]
- Morling, J.R.; Barke, A.N.; Chapman, C.J.; Logan, R.F. Could stool collection devices help increase uptake in bowel cancer screening programmes? J. Med. Screen. 2018, 25, 174–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pham, R.; Cross, S.; Fernandez, B.; Corson, K.; Dillon, K.; Yackley, C.; Davis, M.M. “Finding the Right FIT”: Rural Patient Preferences for Fecal Immunochemical Test (FIT) Characteristics. J. Am. Board Fam. Med. 2017, 30, 632–644. [Google Scholar] [CrossRef] [Green Version]
- Shin, H.; Suh, M.; Choi, K.; Hwang, S.; Jun, J.; Han, D.; Lee, Y.; Oh, J.; Lee, C.; Lee, D. Higher satisfaction with an alternative collection device for stool sampling in colorectal cancer screening with fecal immunochemical test: A cross-sectional study. BMC Cancer 2018, 18, 365. [Google Scholar] [CrossRef] [Green Version]
- De Klerk, C.M.; Wieten, E.; van der Steen, A.; Ramakers, C.R.; Kuipers, E.J.; Hansen, B.E.; Lansdorp-Vogelaar, I.; Bossuyt, P.M.; Spaander, M.C.W.; Dekker, E. Participation and Ease of Use in Colorectal Cancer Screening: A Comparison of 2 Fecal Immunochemical Tests. Am. J. Gastroenterol. 2019, 114, 511–518. [Google Scholar] [CrossRef]
- Ellis, R.J.B.; Wilson, S.; Holder, R.L.; McManus, R.J. Different faecal sampling methods alter the acceptability of faecal occult blood testing: A cross sectional community survey. Eur. J. Cancer 2007, 43, 1437–1444. [Google Scholar] [CrossRef]
- Stoltzfus, K.C.; Popalis, M.L.; Reiter, P.L.; Moss, J.L. Perspectives on self-sampling for cancer screening among rural and urban women: Multilevel factors related to acceptability. J. Rural Health 2021, 18, 18. [Google Scholar]
- Worthley, D.L.; Cole, S.R.; Esterman, A.; Mehaffey, S.; Roosa, N.M.; Smith, A.; Turnbull, D.; Young, G.P. Screening for colorectal cancer by faecal occult blood test: Why people choose to refuse. Intern. Med. J. 2006, 36, 607–610. [Google Scholar] [CrossRef] [PubMed]
- Benning, T.M.; Dellaert, B.G.; Severens, J.L.; Dirksen, C.D. The effect of presenting information about invasive follow-up testing on individuals’ noninvasive colorectal cancer screening participation decision: Results from a discrete choice experiment. Value Health 2014, 17, 578–587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coughlin, S.S.; Berkowitz, Z.; Hawkins, N.A.; Tangka, F. Breast and colorectal cancer screening and sources of cancer information among older women in the United States: Results from the 2003 Health Information National Trends Survey. Prev. Chronic Dis. 2007, 4, A57. [Google Scholar]
- Albright, K.; Richardson, T.; Kempe, K.L.; Wallace, K. Toward a trustworthy voice: Increasing the effectiveness of automated outreach calls to promote colorectal cancer screening among African Americans. Perm. J. 2014, 18, 33–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brackett, C.; Kearing, S.; Cochran, N.; Tosteson, A.N.; Blair Brooks, W. Strategies for distributing cancer screening decision aids in primary care. Patient Educ. Couns. 2010, 78, 166–168. [Google Scholar] [CrossRef]
- Benito, L.; Farre, A.; Binefa, G.; Vidal, C.; Cardona, A.; Pla, M.; Garcia, M. Factors related to longitudinal adherence in colorectal cancer screening: Qualitative research findings. Cancer Causes Control. 2018, 29, 103–114. [Google Scholar] [CrossRef] [Green Version]
- Messina, C.; Lane, D.; Grimson, R. Colorectal Cancer Screening Attitudes and Practices Preferences for Decision Making. Am. J. Prev. Med. 2005, 28, 439–446. [Google Scholar] [CrossRef]
- Martens, C.E.; Crutchfield, T.M.; Laping, J.L.; Perreras, L.; Reuland, D.S.; Cubillos, L.; Pignone, M.P.; Wheeler, S.B. Why Wait Until Our Community Gets Cancer?: Exploring CRC Screening Barriers and Facilitators in the Spanish-Speaking Community in North Carolina. J. Cancer Educ. 2016, 31, 652–659. [Google Scholar] [CrossRef]
- Pignone, M.P.; Crutchfield, T.M.; Brown, P.M.; Hawley, S.T.; Laping, J.L.; Lewis, C.L.; Lich, K.H.; Richardson, L.C.; Tangka, F.K.; Wheeler, S.B. Using a discrete choice experiment to inform the design of programs to promote colon cancer screening for vulnerable populations in North Carolina. BMC Health Serv. Res. 2014, 14, 611. [Google Scholar] [CrossRef] [Green Version]
- Baassiri, A.; El-Harakeh, M.; Itani, A.; Nassar, F.J.; Safi, R.; Dassouki, Z.; Romani, M.; Zgheib, N.; Nasr, R. Giant Inflatable Colon Model Enhances Lebanese Community Knowledge and Intention for Colorectal Cancer Screening. JCO Glob. Oncol. 2020, 6, 167–173. [Google Scholar] [CrossRef]
- A Healthier Michigan. Inflatable Colon [Photograph]. 2021. Available online: https://www.flickr.com/photos/healthiermi/13266807653 (accessed on 1 September 2021).
- Banks, J.; Hollinghurst, S.; Bigwood, L.; Peters, T.J.; Walter, F.M.; Hamilton, W. Preferences for cancer investigation: A vignette-based study of primary-care attendees. Lancet Oncol. 2014, 15, 232–240. [Google Scholar] [CrossRef] [Green Version]
- Brewer, K.C.; Peacock, N.R.; Ferrans, C.E.; Campbell, R.T.; Polite, B.; Carnahan, L.; Jones, L.A.; Rauscher, G.H. Gender- and Race-Based Differences in Barriers and Facilitators to Early Detection of Colon Cancer. J. Women’s Health 2020, 29, 1192–1202. [Google Scholar] [CrossRef]
- Nayaradou, M.; Berchi, C.; Dejardin, O.; Launoy, G. Eliciting population preferences for mass colorectal cancer screening organization. Med. Decis. Mak. 2010, 30, 224–233. [Google Scholar] [CrossRef] [PubMed]
- Ho, W.; Broughton, D.E.; Donelan, K.; Gazelle, G.S.; Hur, C. Analysis of barriers to and patients’ preferences for CT colonography for colorectal cancer screening in a nonadherent urban population. Am. J. Roentgenol. 2010, 195, 393–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hollinghurst, S.; Banks, J.; Bigwood, L.; Walter, F.M.; Hamilton, W.; Peters, T.J. Using willingness-to-pay to establish patient preferences for cancer testing in primary care. BMC Med. Inform. Decis. Mak. 2016, 16, 105. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Hultcrantz, R. Aspects of colorectal cancer screening, methods, age and gender. J. Intern. Med. 2021, 289, 493–507. [Google Scholar] [CrossRef]
- Sammarco, G.; Gallo, G.; Vescio, G.; Picciariello, A.; De Paola, G.; Trompetto, M.; Curro, G.; Ammendola, M. Mast Cells, microRNAs and Others: The Role of Translational Research on Colorectal Cancer in the Forthcoming Era of Precision Medicine. J. Clin. Med. 2020, 9, 2852. [Google Scholar] [CrossRef]
- Moazzendizaji, S.; Sevbitov, A.; Ezzatifar, F.; Jalili, H.R.; Aalii, M.; Hemmatzadeh, M.; Aslani, S.; Navashenaq, J.G.; Safari, R.; Hosseinzadeh, R.; et al. microRNAs: Small molecules with a large impact on colorectal cancer. Biotechnol. Appl. Biochem. 2021. [Google Scholar] [CrossRef] [PubMed]
- Canadian Task Force on Preventive Health, C. Recommendations on screening for colorectal cancer in primary care. CMAJ 2016, 188, 340–348. [Google Scholar] [CrossRef] [Green Version]
- Wilkins, T.; McMechan, D.; Talukder, A. Colorectal Cancer Screening and Prevention. Am. Fam. Phys. 2018, 97, 658–665. [Google Scholar]
- Peterse, E.F.P.; Meester, R.G.S.; Siegel, R.L.; Chen, J.C.; Dwyer, A.; Ahnen, D.J.; Smith, R.A.; Zauber, A.G.; Lansdorp-Vogelaar, I. The impact of the rising colorectal cancer incidence in young adults on the optimal age to start screening: Microsimulation analysis I to inform the American Cancer Society colorectal cancer screening guideline. Cancer 2018, 124, 2964–2973. [Google Scholar] [CrossRef]
- Meester, R.G.S.; Peterse, E.F.P.; Knudsen, A.B.; de Weerdt, A.C.; Chen, J.C.; Lietz, A.P.; Dwyer, A.; Ahnen, D.J.; Siegel, R.L.; Smith, R.A.; et al. Optimizing colorectal cancer screening by race and sex: Microsimulation analysis II to inform the American Cancer Society colorectal cancer screening guideline. Cancer 2018, 124, 2974–2985. [Google Scholar] [CrossRef] [PubMed]
- Montminy, E.M.; Zhou, M.; Maniscalco, L.; Abualkhair, W.; Kim, M.K.; Siegel, R.L.; Wu, X.C.; Itzkowitz, S.H.; Karlitz, J.J. Contributions of Adenocarcinoma and Carcinoid Tumors to Early-Onset Colorectal Cancer Incidence Rates in the United States. Ann. Intern. Med. 2021, 174, 157–166. [Google Scholar] [CrossRef]
- Vuik, F.E.; Nieuwenburg, S.A.; Bardou, M.; Lansdorp-Vogelaar, I.; Dinis-Ribeiro, M.; Bento, M.J.; Zadnik, V.; Pellise, M.; Esteban, L.; Kaminski, M.F.; et al. Increasing incidence of colorectal cancer in young adults in Europe over the last 25 years. Gut 2019, 68, 1820–1826. [Google Scholar] [CrossRef] [PubMed]
- US Preventive Services Task Force; Davidson, K.W.; Barry, M.J.; Mangione, C.M.; Cabana, M.; Caughey, A.B.; Davis, E.M.; Donahue, K.E.; Doubeni, C.A.; Krist, A.H.; et al. Screening for Colorectal Cancer: US Preventive Services Task Force Recommendation Statement. JAMA 2021, 325, 1965–1977. [Google Scholar] [CrossRef] [PubMed]
- Foppa, C.; Francesca Bertuzzi, A.; Cianchi, F.; Carvello, M.; Maroli, A.; Wolthuis, A.M.; Rimassa, L.; Laghi, L.; Montorsi, M.; D’Hoore, A.J.L.; et al. Rectal Cancer in Adolescent and Young Adult Patients: Pattern of Clinical Presentation and Case-Matched Comparison of Outcomes. Dis. Colon Rectum 2021, 64, 1064–1073. [Google Scholar] [CrossRef]
- Mehta, S.J.; Morris, A.M.; Kupfer, S.S. Colorectal Cancer Screening Starting at Age 45 Years-Ensuring Benefits Are Realized by All. JAMA Netw. Open 2021, 4, e2112593. [Google Scholar] [CrossRef] [PubMed]
- Joanna Briggs Institute. Joanna Briggs Institute Reviewers’ Manual, 2014 ed.; University of Adelaide: Adelaide, Australia, 2014; Available online: https://nursing.lsuhsc.edu/JBI/docs/ReviewersManuals/ReviewersManual.pdf (accessed on 6 October 2021).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Setting | Methods | Sample Size | Most Preferred Test | % Respondents Choosing the Preferred Test | Tests Compared |
|---|---|---|---|---|---|---|
| Moreno et al., 2019 [41] | USA; 2016 | Survey | 215 | colonoscopy | 80.6% | Colonoscopy vs. stool-based tests vs. CTC |
| Cho et al., 2017 [42] | South Korea, 2016 | Questionnaire | 396 | colonoscopy | 68.7% | Colonoscopy vs. FIT |
| Jung et al., 2009 [43] | South Korea; 2006 | Questionnaire (followed by telephone questionnaire) | 51 | colonoscopy | 64.7% | Colonoscopy vs. CTC |
| Imaeda et al., 2010 [44] | USA | Survey | 92 | colonoscopy | 62% | Colonoscopy vs. FOBT vs. sigmoidoscopy vs. colon capsule vs. CTC |
| Omran et al., 2015 [45] | Jordan; 2014 | Survey | 713 | colonoscopy | 60.4% | Colonoscopy vs. sigmoidoscopy vs. FOBT |
| Calderwood et al., 2011 [46] | USA; 2008–2010 | Survey | 100 | colonoscopy | 59% | Colonoscopy vs. FOBT vs. sDNA vs. CTC |
| Redwood et al., 2019 [31] | USA; 2017 | Survey | 1616 | colonoscopy | 58% | Colonoscopy vs. sDNA |
| Palmer et al., 2010 [47] | USA; 2007 | In-depth personal interview | 60 | colonoscopy | 57% | Colonoscopy vs. FOBT vs. barium enema vs. sigmoidoscopy |
| Chatrath and Rex, 2014 [29] | USA | Survey | 502 | colonoscopy | 57% | Colonoscopy vs. FOBT vs. colon capsule |
| Sandoval et al., 2021 [48] | Switzerland; 2016 | Survey | 1260 | colonoscopy | 54.9% | Colonoscopy vs. FOBT |
| Schroy et al., 2007 [49] | USA; 2002–2003 | Survey | 263 | colonoscopy | 51.6% | Colonoscopy vs. FOBT vs. sigmoidoscopy vs. sigmoidoscopy plus FOBT vs. barium enema vs. sDNA |
| Ruffin et al., 2009 [50] | USA | Focus group interview and survey | 93 | colonoscopy | 49% | Colonoscopy vs. FOBT vs. sigmoidoscopy vs. barium enema |
| Hawley et al., 2012 [51] | USA; 2004–2006 | Telephone survey | 1224 | colonoscopy | 41.1% | Colonoscopy vs. FOBT vs sigmoidoscopys barium enema |
| Lachter et al., 2008 [52] | Israel | Questionnaire and follow-up telephone call | 100 | FOBT | 84% | Colonoscopy vs. FOBT vs. sigmoidoscopy vs. barium enema |
| Qumseya et al., 2014 [53] | Palestine | Self-administered questionnaire | 1352 | FOBT | 79% | Colonoscopy vs. FOBT |
| Zhu et al., 2021 [54] | USA; 2019 | Pannel survey | 1595 | sDNA | >65% | Colonoscopy vs. sDNA vs. FOBT |
| Bonello et al., 2016 [55] | UK | Questionnaire | 491 | FOBT | 60.8% | Colonoscopy vs. FIT |
| Brenner et al., 2014 [56] | USA and Australia; 2011 | Online survey | 920 | FOBT | 55.9% | Colonoscopy vs. FOBT vs. sigmoidoscopy ys radiological test |
| Wolf et al., 2016 [26] | USA; 2011–2013 | Questionnaire | 528 | stool-based | 54.5% | Colonoscopy vs. stool-based test |
| DeBourcy et al., 2008 [28] | USA; 2007 | Survey | 323 | FOBT | 53% | Colonoscopy vs. FOBT |
| Schroy et al., 2005 [57] | USA; 2001–2003 | Survey | 4042 | sDNA | 45% | Colonosocpy vs. FOBT vs. sDNA test |
| Phisalprapa et al., 2021 [58] | Thailand; 2017–2018 | Discrete choice experiment questionnaire | 400 | FOBT | 38.2% | Colonoscopy vs. FIT vs. barium enema vs. CTC vs. sigmoidoscopy |
| Author/Year | Setting | Sample Size | “Payable” Amount (Mean Values) | Test Type and/or Features |
|---|---|---|---|---|
| Ho et al., 2010 [153] | USA | 68 | $244 | CTC |
| Hollinghurst et al., 2016 [154] | UK; 2011–2012 | 35% = between £1 and £100 21% = between £101 and £300 10% = between £301 and £700 16% = over £700 17% = would not pay | Colonoscopy | |
| Mansfield et al., 2018 [109] | USA; 2014–2015 | 2067 | 64% = would choose it if it was free 17% = would pay the cost of $200 | Colonoscopy (over FIT) |
| Up to $1416 | A test that found “most cancer” (compared to “some cancer”) | |||
| Up to $989 | A test that removed polyps | |||
| Up to $690 | Avoiding discomfort (eg. using a sedative) | |||
| Marshall et al., 2009 [20] | Canada and USA; 2005 | 501 | $232 | CTC |
| $222 | sDNA | |||
| Omran et al., 2015 [45] | Jordan; 2014 | 713 | 65.5% = up to $706 25.5% = would wait up to 6 months to get free service 9% = would refuse colonoscopy | Prompt colonoscopy if recommended by physician |
| Osborne et al., 2018 [88] | Australia | 1282 | $13, $8, $21 respectively. | Blood, saliva and stool based-test, respectively |
| $87 and $1, respectively. | 90% and 80% cancer detection rate, respectively | |||
| Phisalprapa et al., 2021 [58] | Thailand; 2017–2018 | 400 | $189, $142, $183, $154, and $251 | Colonoscopy, flexible sigmoidoscopy, double-contrast barium enema, CTC and FIT, respectively. |
| $3 | For every 1% increase in mortaliy risk reduction | |||
| $46 | 5-year interval | |||
| $45 | Less complications | |||
| $38 | No bowel preparation | |||
| Van Bebber et al., 2007 [104] | USA; 2005 | 1087 | $150 (mean), in particular: 37% = $150 23% = $20 17% = would not pay | Genetic tests |
| Zhou et al., 2018 [113] | China | 1240 | 29.2% = less than ¥100 20.7% = ¥100–¥199 14.8% = ¥200–¥299 13.0% = ¥300–¥399 22.4% = more than ¥400 | CRC screening |
| Search History | Results (n) | |
|---|---|---|
| 1 | exp Colorectal Neoplasms/ | 236,253 |
| 2 | exp Early Detection of Cancer/ | 29,324 |
| 3 | exp Patient Preference/ | 9598 |
| 4 | exp “patient acceptance of health care”/or patient compliance/or patient participation/ | 169,803 |
| 5 | 3 or 4 | 177,822 |
| 6 | 1 and 2 and 5 | 829 |
| 7 | exp “surveys and questionnaires”/or health care surveys/or health surveys/or patient health questionnaire/or self-report/ | 1,108,317 |
| 8 | 6 and 7 | 427 |
| 9 | screening.ab,kf,ti. | 970,991 |
| 10 | (Colorectal Cancer or Bowel Cancer or Colon Cancer).ab,kf,ti. | 225,573 |
| 11 | (“prefer*” or willingness*” or “accept*”).ab,kf,ti. | 1,641,532 |
| 12 | (“questionnaire*” or “survey*”).ab,kf,ti. | 2,133,496 |
| 13 | 9 and 10 and 11 and 12 | 692 |
| 14 | 13 or 8 | 1070 |
| 15 | limit 14 to english language | 1027 |
| 16 | limit 15 to yr = “2005-Current” | 943 |
| 17 | remove duplicates from 16 | 742 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tran, T.N.; Ferrari, A.; Hoeck, S.; Peeters, M.; Van Hal, G. Colorectal Cancer Screening: Have We Addressed Concerns and Needs of the Target Population? Gastrointest. Disord. 2021, 3, 173-203. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord3040018
Tran TN, Ferrari A, Hoeck S, Peeters M, Van Hal G. Colorectal Cancer Screening: Have We Addressed Concerns and Needs of the Target Population? Gastrointestinal Disorders. 2021; 3(4):173-203. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord3040018
Chicago/Turabian StyleTran, Thuy Ngan, Allegra Ferrari, Sarah Hoeck, Marc Peeters, and Guido Van Hal. 2021. "Colorectal Cancer Screening: Have We Addressed Concerns and Needs of the Target Population?" Gastrointestinal Disorders 3, no. 4: 173-203. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord3040018