Implant-Supported Prosthesis for Edentulous Patient Rehabilitation. From Temporary Prosthesis to Definitive with a New Protocol: A Single Case Report

 , and
, and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
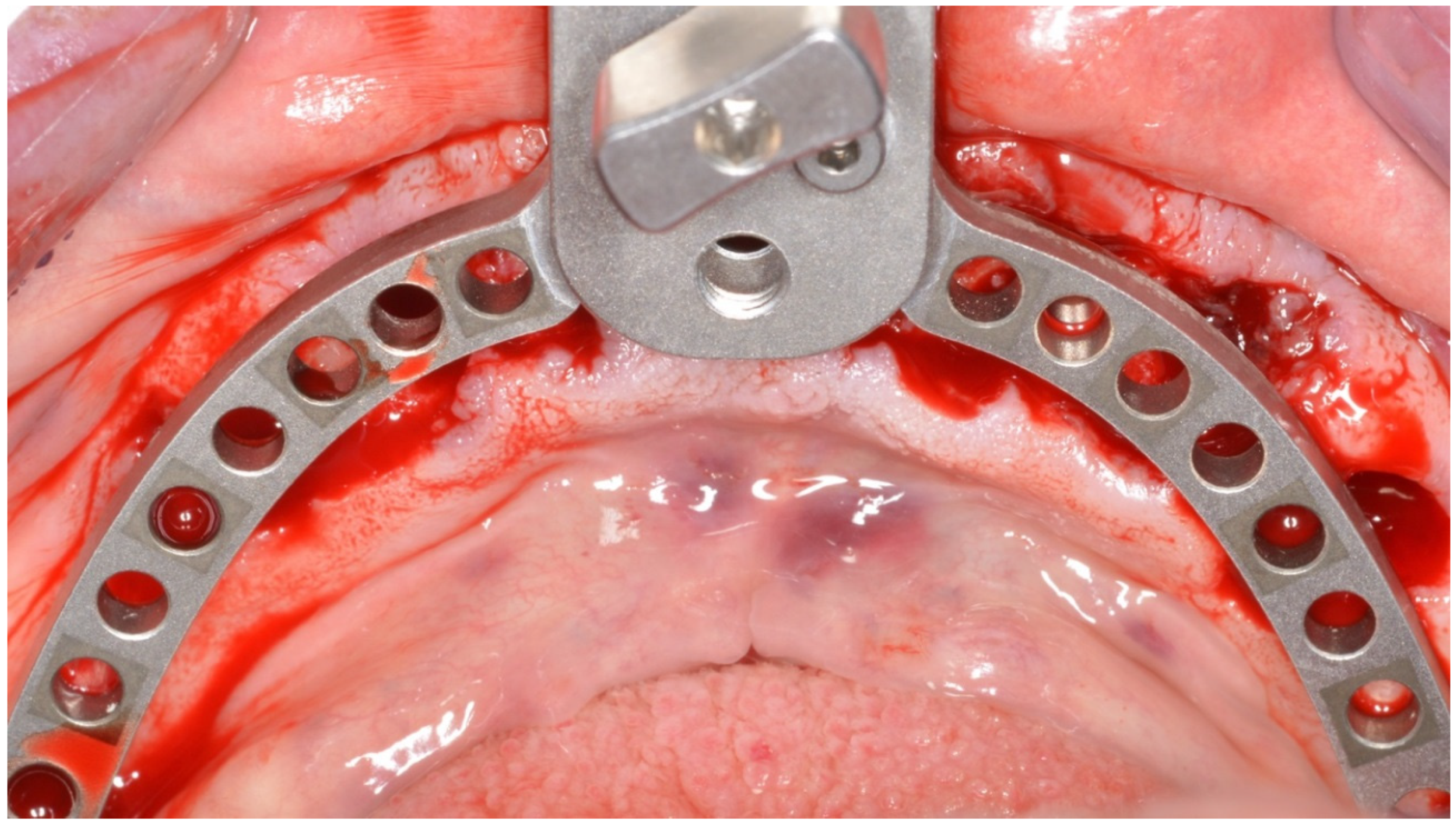
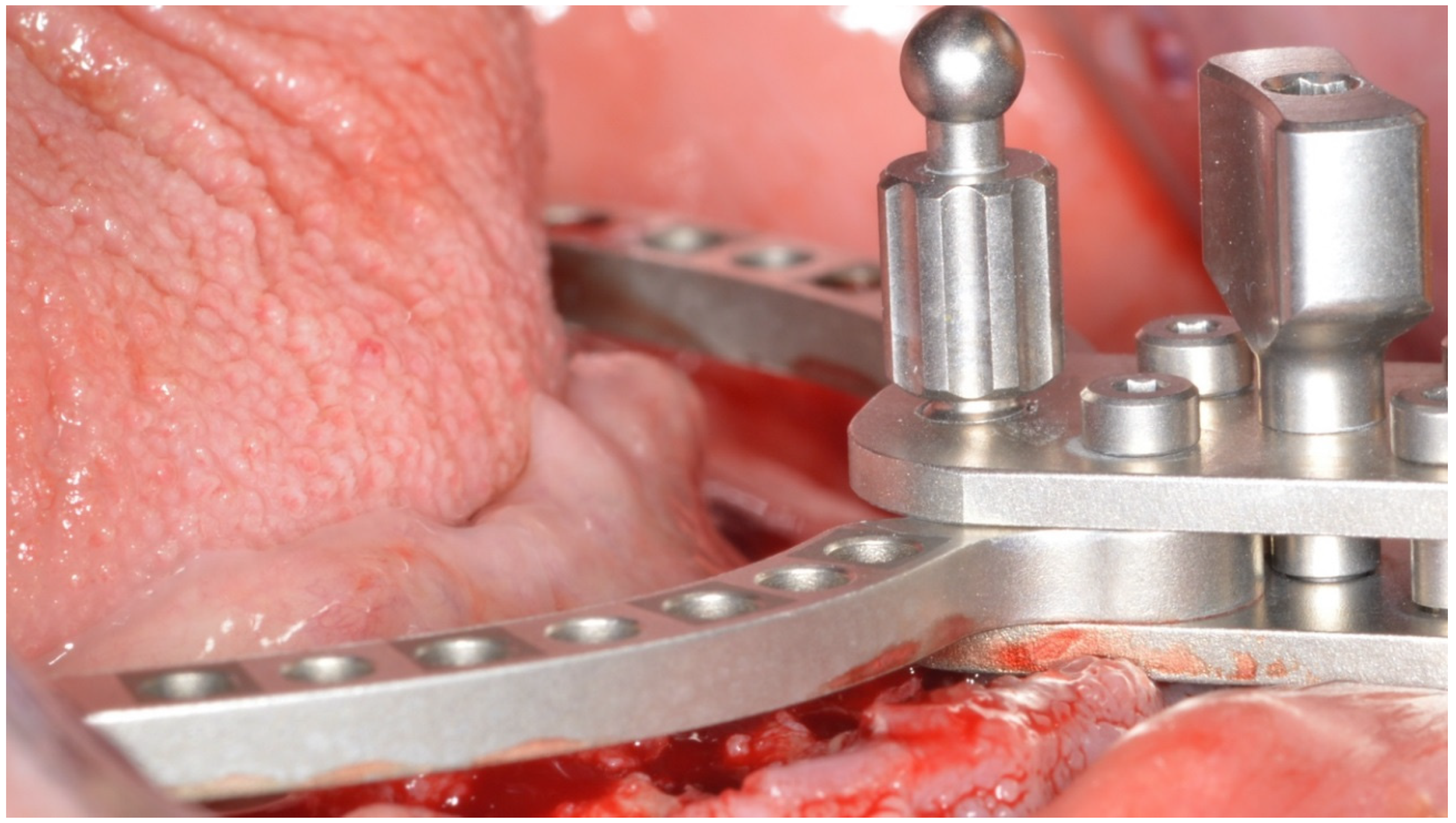
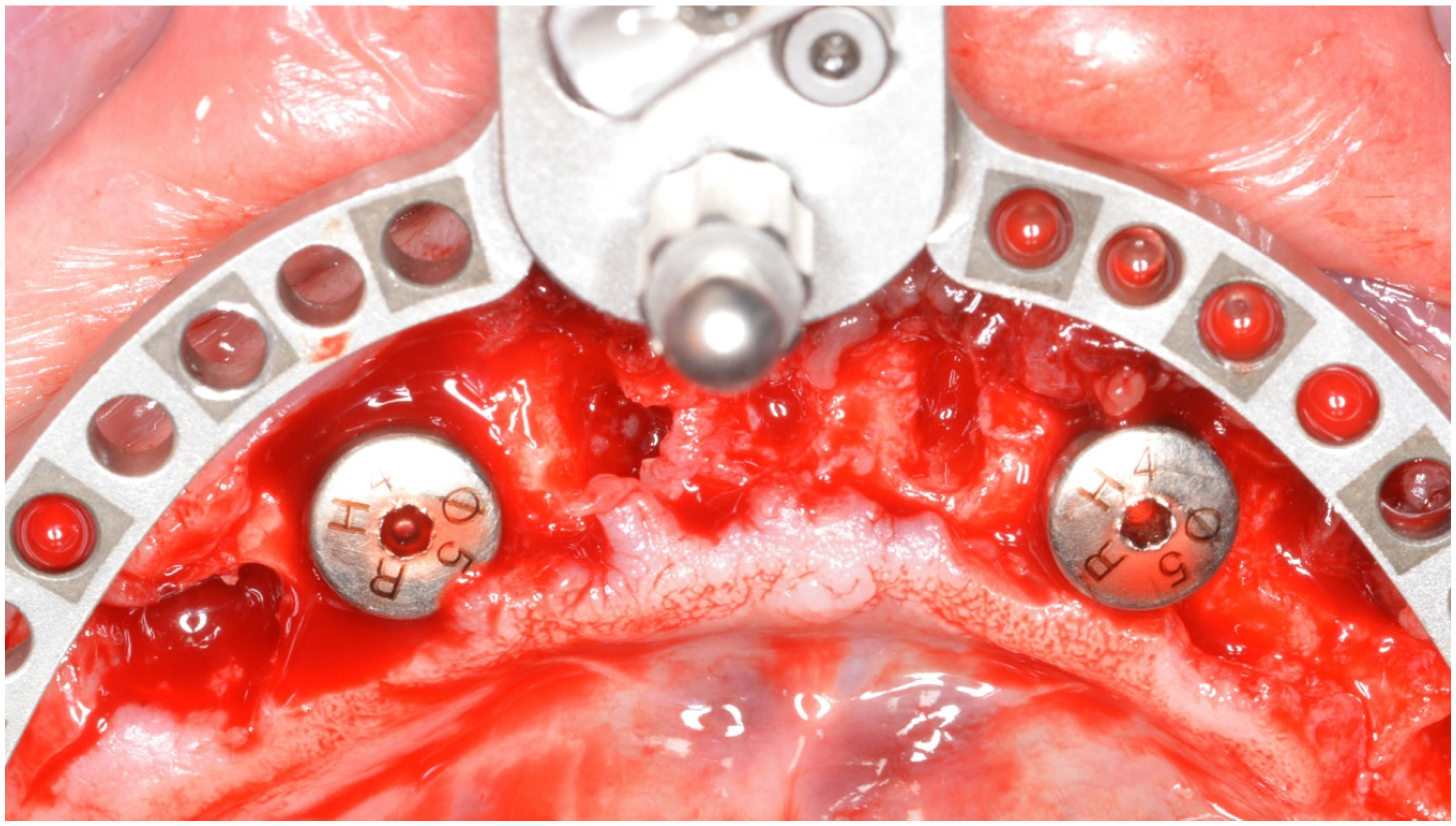
2. Materials and Methods
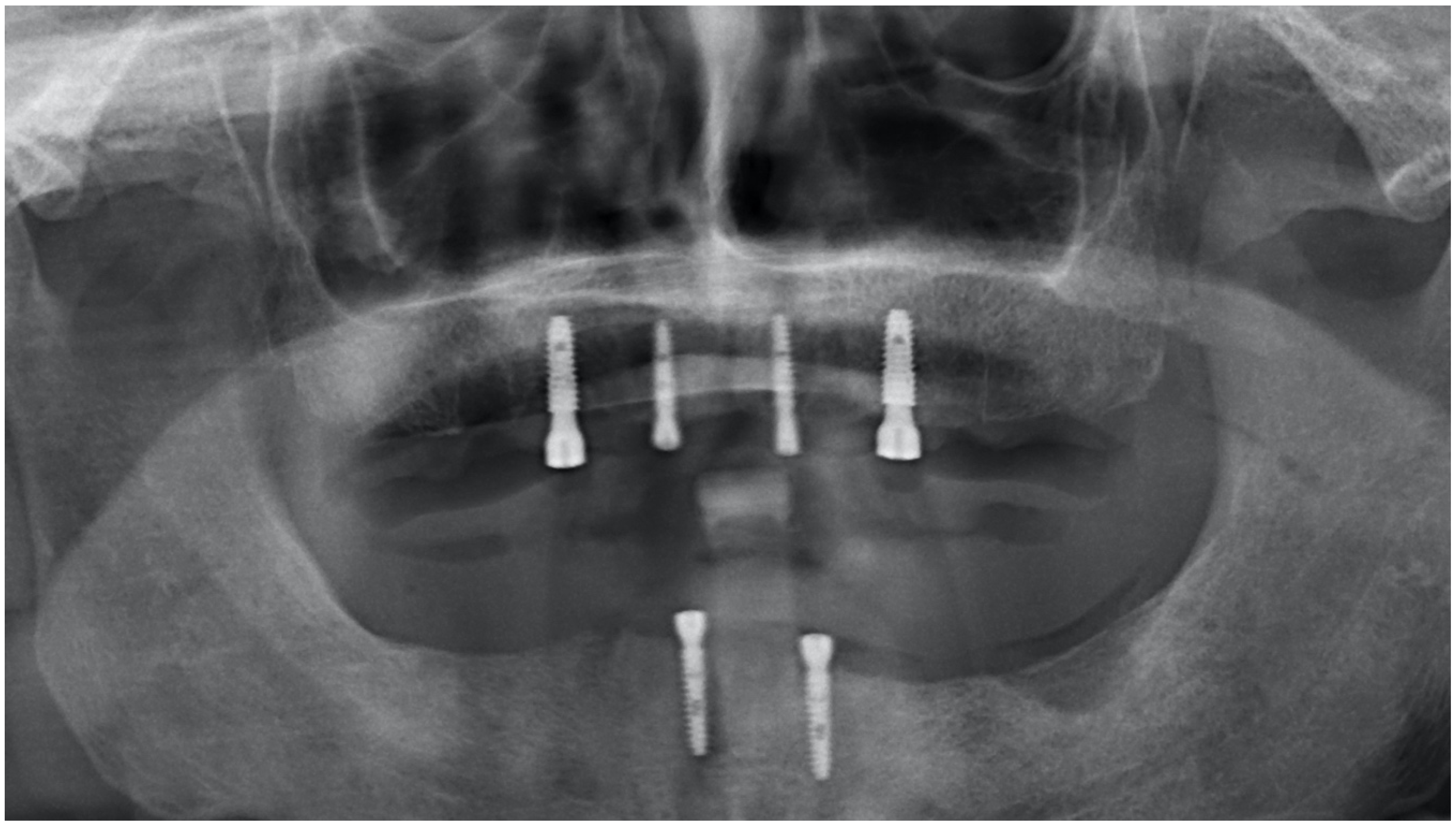
- First panoramic footprints;
- DV detection;
- Facial arch;
- Articulator assembly;
- Mounting of the teeth, a key step especially in the realization of a temporary prosthesis.
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A





















References
- Zitzmann, N.U.; Marinello, C.P.; Sendi, P. A cost-effectiveness analysis of implant overdentures. J. Dent. Res. 2006, 85, 717–721. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Blomberg, S.; Branemark, A.; Carlsson, G.E. Edentulousness–an oral handicap. Patient reactions to treatment with jawbone-anchored prostheses. J. Oral Rehabil. 1987, 14, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Ellis, J.S.; Burawi, G.; Walls, A.; Thomason, J.M. Patient satisfaction with two designs of implant supported removable overdentures; ball attachment and magnets. Clin. Oral Implants Res. 2009, 20, 1293–1298. [Google Scholar] [CrossRef] [PubMed]
- Harris, D.; Höfer, S.; O’Boyle, C.A.; Sheridan, S.; Marley, J.; Benington, I.C.; Clifford, T.; Houston, F.; O’Connell, B. A comparison of implant-retained mandibular overdentures and conventional dentures on quality of life in edentulous patients: A randomized, prospective, within-subject controlled clinical trial. Clin. Oral Implants Res. 2011, 24, 96–103. [Google Scholar] [CrossRef]
- Bramanti, E.; Matacena, G.; Cecchetti, F.; Arcuri, C.; Cicciù, M. Oral health-related quality of life in partially edentulous patients before and after implant therapy: A 2-year longitudinal study. ORAL Implantol. 2013, 6, 37–42. [Google Scholar] [CrossRef]
- Germano, F.; Bramanti, E.; Arcuri, C.; Cecchetti, F.; Cicciù, M. Atomic force microscopy of bacteria from periodontal subgingival biofilm: Preliminary study results. Eur. J. Dent. 2013, 7, 152–158. [Google Scholar] [CrossRef] [Green Version]
- Maiorana, C.; Beretta, M.; Grossi, G.B.; Santoro, F.; Herford, A.S.; Nagursky, H.; Cicciù, M. Histomorphometric evaluation of anorganic bovine bone coverage to reduce autogenous grafts resorption: Preliminary results. Open Dent. J. 2011, 5, 71–78. [Google Scholar] [CrossRef] [Green Version]
- Thomason, J.M.; Kelly, S.A.M.; Bendkowski, A.; Ellis, J.S. Two implant retained overdentures—A review of the literature supporting the McGill and York consensus statements. J. Dent. 2012, 40, 22–34. [Google Scholar] [CrossRef]
- Tallarico, M.; Vaccarella, A.; Marzi, G.C. Clinical and radiological outcomes of 1- versus 2-stage implant placement: 1-year results of a randomised clinical trial. Eur J. Oral Implant. 2011, 4, 13–20. [Google Scholar]
- Babbush, C.A.; Tallarico, M. Twelve-year clinical and radiological results of maxillary and mandibular implant-retained bar overdentures carried out on oxidized (TiUnite) replace select implants: A clinical case. J. Oral Implantol. 2013, 39, 737–742. [Google Scholar] [CrossRef]
- Scrascia, R.; Venezia, P. Healthcare meets Aesthetics: New approaches to the complex oral rehabilitations with implant-supported dental prostheses. Australas. Med J. 2017, 10, 537–541. [Google Scholar] [CrossRef]
- Portelli, M.; Militi, A.; Logiudice, A.; Nucera, R. An Integrated Approach, Orthodontic and Prosthetic, in a Case of Maxillary Lateral Incisors Agenesis. Prosthesis 2019, 1, 3–10. [Google Scholar] [CrossRef] [Green Version]
- Ortensi, L.; Vitali, T.; Bonfiglioli, R.; Grande, F. New Tricks in the Preparation Design for Prosthetic Ceramic Laminate Veeners. Prosthesis 2019, 1, 29–40. [Google Scholar] [CrossRef] [Green Version]
- McGrory, A.C.; McGrory, B.J.; Rana, A.; Babikian, G. Incidence of Heterotopic Ossification in Anterior Based Muscle Sparing Total Hip Arthroplasty: A Retrospective Radiographic Review. Prosthesis 2019, 1, 11–15. [Google Scholar] [CrossRef] [Green Version]
- Frossard, L.; Jones, M.W.M.; Stewart, I.; Leggat, P.A.; Schuetz, M.; Langton, C. Kinetics of Lower Limb Prosthesis: Automated Detection of Vertical Loading Rate. Prosthesis 2019, 1, 16–28. [Google Scholar] [CrossRef] [Green Version]
- Cicciù, M. Prosthesis: New Technological Opportunities and Innovative Biomedical Devices. Prosthesis 2019, 1, 1–2. [Google Scholar] [CrossRef] [Green Version]
- Cicciù, M.; Cervino, G.; Milone, D.; Risitano, G. FEM Investigation of the Stress Distribution over Mandibular Bone Due to Screwed Overdenture Positioned on Dental Implants. Materials 2018, 11, 1512. [Google Scholar] [CrossRef] [Green Version]
- Xhanari, E.; Scrascia, R.; Kadiu, B.; Tallarico, M. Two implants supporting a mandibular overdenture to rehabilitate Cawood and Howell Class V and VI patients: A proof-of-concept study. J. Oral Sci. Rehabilit. 2017, 3, 52–59. [Google Scholar]
- Scrascia, R.; Martinolli, M.; Venezia, P.; Casucci, A.; Ortensi, L.; Tallarico, M. Feasibility of Low Profile Attachments to Improve Quality of Life on Patients with Implant-Retained Mandibular Overdenture: 1-Year Preliminary Results of a Multicenter Prospective Case Series Study. J. Oral Health Dental Manag. 2018, 17, 5. [Google Scholar]
- De Stefano, R. Psychological Factors in Dental Patient Care: Odontophobia. Medicina 2019, 55, 678. [Google Scholar] [CrossRef] [Green Version]
- Bryant, S.R.; Walton, J.N.; MacEntee, M.I. A 5-year randomized trial to compare 1 or 2 implants for implant overdentures. J. Dent. Res. 2015, 94, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Fiorillo, L. Chlorhexidine Gel Use in the Oral District: A Systematic Review. Gels 2019, 5, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Troiano, G.; Laino, L.; Cicciu, M.; Cervino, G.; Fiorillo, L.; D’Amico, C.; Zhurakivska, K.; Lo Muzio, L. Comparison of Two Routes of Administration of Dexamethasone to Reduce the Postoperative Sequelae After Third Molar Surgery: A Systematic Review and Meta-Analysis. Open Dent. J. 2018, 12, 181–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scrascia, R.; Fiorillo, L.; Gaita, V.; Secondo, L.; Nicita, F.; Cervino, G. Implant-Supported Prosthesis for Edentulous Patient Rehabilitation. From Temporary Prosthesis to Definitive with a New Protocol: A Single Case Report. Prosthesis 2020, 2, 10-24. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis2010002
Scrascia R, Fiorillo L, Gaita V, Secondo L, Nicita F, Cervino G. Implant-Supported Prosthesis for Edentulous Patient Rehabilitation. From Temporary Prosthesis to Definitive with a New Protocol: A Single Case Report. Prosthesis. 2020; 2(1):10-24. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis2010002
Chicago/Turabian StyleScrascia, Roberto, Luca Fiorillo, Valeria Gaita, Luigi Secondo, Fabiana Nicita, and Gabriele Cervino. 2020. "Implant-Supported Prosthesis for Edentulous Patient Rehabilitation. From Temporary Prosthesis to Definitive with a New Protocol: A Single Case Report" Prosthesis 2, no. 1: 10-24. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis2010002