Proposal for a Clinical Approach to Geriatric Patients with Anchor Need on Implant for Removable Denture: New Technique

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Aim
3. Materials and Methods
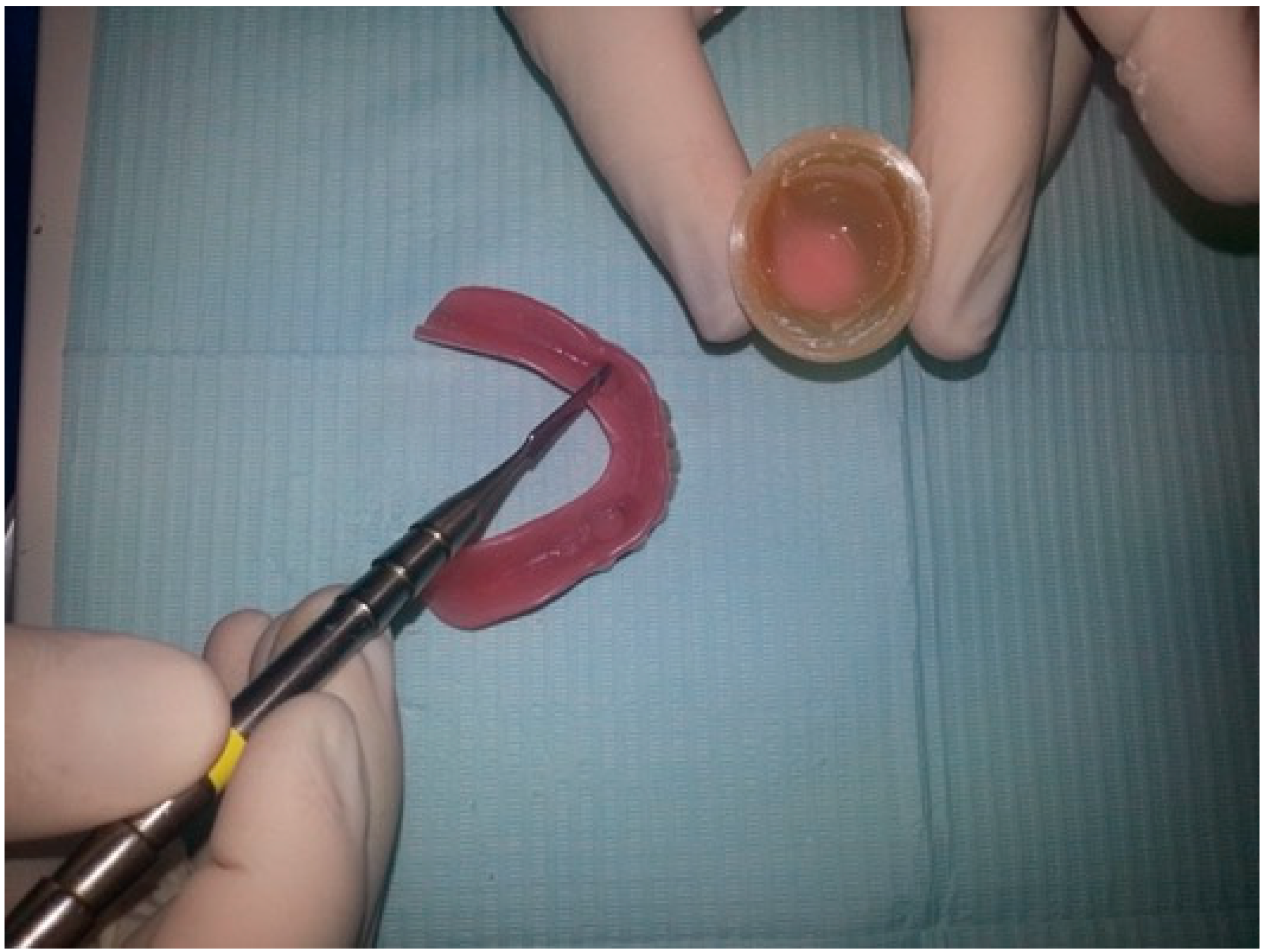
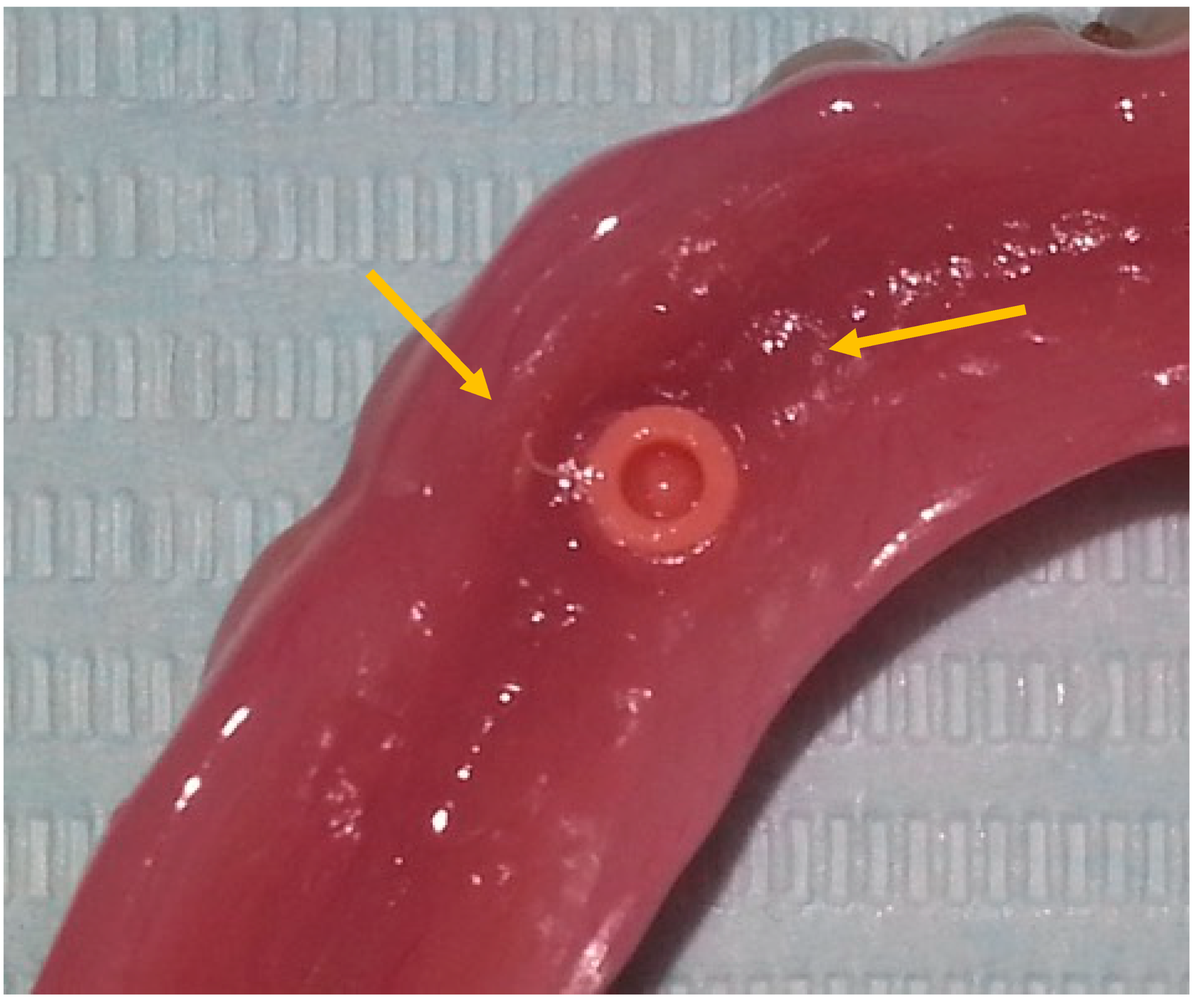
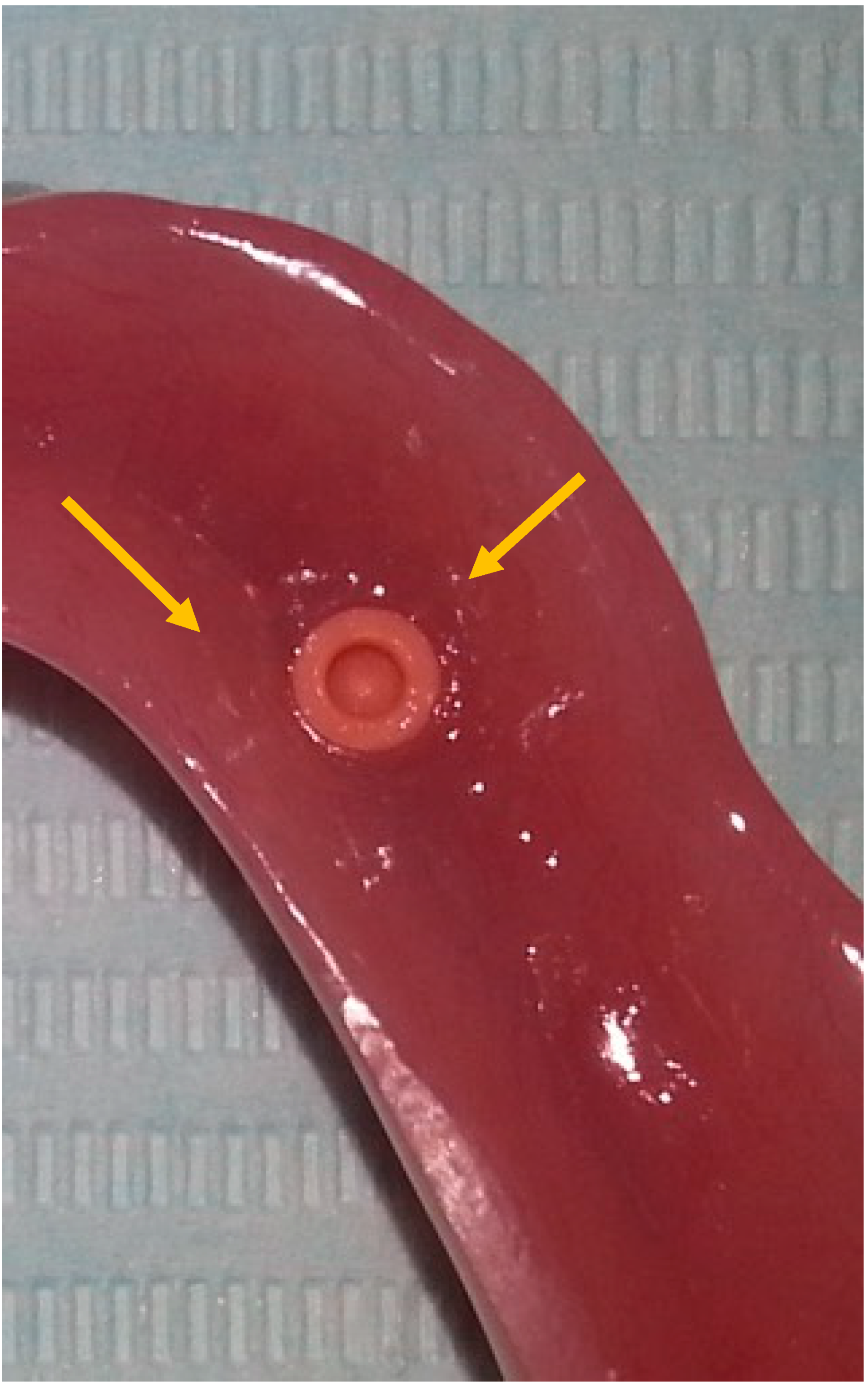
- After 7 days, the Teflon/o-ring is replaced. After preparing the housing for the Teflon on the mobile prosthesis and evaluating the necessary height, insert the small silicone tube cut at the right height in the ball-attachment. Then, the Teflon is inserted. The silicone tube adheres superiorly to the Teflon inferiorly to the gingiva protecting the entire retentive attachment (Figure 4, Figure 5, Figure 6 and Figure 7). After mixing the acrylic resin and inserting it in the right quantity (filling the previously prepared cavity 50%), the prosthesis is fitted into the oral cavity, causing the patient to close in full intercuspidation and waiting for polymerization (Figure 8, Figure 9 and Figure 10). Once the polymerization has taken place, the mobile prosthesis can be removed very easily as the acrylic resin will be present only around the Teflon and will have filled all the walls of the cavity previously prepared leaving them smooth; there may be small smears of resin that will easily be removed in a short time with the aid of rubber pads (Figure 11).
4. Results
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Volkert, D. Nutrition in dementia. Internist 2017, 58, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Parrotta, I.; Maltais, M.; Rolland, Y.; Spampinato, D.A.; Robert, P.; de Souto Barreto, P.; Vellas, B. The association between apathy and frailty in older adults: A new investigation using data from the Mapt study. Aging Ment. Health 2019, 14, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Bell, C.L.; Lopez, R.P.; Mahendra, N.; Tamai, A.; Davis, J.; Amella, E.J.; Masaki, K. Person-centered Feeding Care: A Protocol to Re-introduce OralFeeding for Nursing Home Patients with Tube Feeding. J. Nutr. Health Aging 2016, 20, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, N.; Amano, N.; Nakamura, T.; Yanagi, M. Relationship between tooth loss, low masticatory ability, and nutritional indices in the elderly: A cross-sectional study. BMC Oral Health 2019, 19, 110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caccianiga, G.; Rey, G.; Baldoni, M.; Paiusco, A. Clinical, Radiographic and Microbiological Evaluation of High Level Laser Therapy, a New Photodynamic Therapy Protocol, in Peri-Implantitis Treatment; A Pilot Experience. Biomed. Res. Int. 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caccianiga, G.; Rey, G.; Fumagalli, T.; Cambini, A.; Denotti, G.; Giacomello, M. Photodynamic therapy (association diode laser/hydrogen peroxide): Evaluation of bactericidal effects on periodontopathic bacteria: An in vitro study. Eur. J. Inflamm. 2012, 10 (Suppl. 2), 101–106. [Google Scholar] [CrossRef] [Green Version]
- Caccianiga, G.; Cambini, A.; Rey, G.; Paiusco, A.; Fumagalli, T.; Giacomello, M. The use of laser diodes superpulses in implantology. Eur. J. inflamm. 2012, 10, 97–100. [Google Scholar] [CrossRef] [Green Version]
- Čelebić, A.; Peršić, S.; Kovačić, I.; Buković, D.; Lešić, N.; Rener-Sitar, K. Comparison of Three Prosthodontic Treatment Modalities for Patients with Periodontally Compromised Anterior Mandibular Teeth: A 2-year follow-up study. Acta Stomatol. Croat. 2019, 53, 4–16. [Google Scholar] [CrossRef] [PubMed]
- Karabuda, C.; Yaltirik, M.; Bayraktar, M. A clinical comparison of prosthetic complications of implant-supported overdentures with different attachment systems. Implant Dent. 2008, 17, 74–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abou-Ayash, S.; Enkling, N.; Srinivasan, M.; Haueter, M.; Worni, A.; Schimmel, M. Evolution of in vivo assessed retention forces in one-piece mini dental implant-retained mandibular overdentures: 5-Year follow-up of a prospective clinical trial. Clin. Implant Dent. Relat. Res. 2019, 16. [Google Scholar] [CrossRef] [PubMed]
- Ceraulo, S. Modifica della dimensione vertical. Caso clinic. PROtech 2008, 9, 17–22, ISSN 15910067. [Google Scholar]
- Ortensi, L.; Ortensi, M.; Minghelli, A.; Grande, F. Implant-Supported Prosthetic Therapy of an Edentulous Patient: Clinical and Technical Aspects. Prosthesis 2020, 2, 140–152. [Google Scholar] [CrossRef]
- Tallarico, M.; Cervino, G.; Scrascia, R.; Uccioli, U.; Lumbau, A.; Meloni, S.M. Minimally Invasive Treatment of Edentulous Maxillae with Overdenture Fully Supported by a Cad/Cam Titanium Bar with a Low-Profile Attachment Screwed on Four or Six Implants: A Case Series. Prosthesis 2020, 2, 53–64. [Google Scholar] [CrossRef]













© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ceraulo, S.; Leonida, A.; Lauritano, D.; Baldoni, A.; Longoni, S.; Baldoni, M.; Caccianiga, G. Proposal for a Clinical Approach to Geriatric Patients with Anchor Need on Implant for Removable Denture: New Technique. Prosthesis 2020, 2, 185-195. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis2030016
Ceraulo S, Leonida A, Lauritano D, Baldoni A, Longoni S, Baldoni M, Caccianiga G. Proposal for a Clinical Approach to Geriatric Patients with Anchor Need on Implant for Removable Denture: New Technique. Prosthesis. 2020; 2(3):185-195. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis2030016
Chicago/Turabian StyleCeraulo, Saverio, Alessandro Leonida, Dorina Lauritano, Alessandro Baldoni, Salvatore Longoni, Marco Baldoni, and Gianluigi Caccianiga. 2020. "Proposal for a Clinical Approach to Geriatric Patients with Anchor Need on Implant for Removable Denture: New Technique" Prosthesis 2, no. 3: 185-195. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis2030016