1. Introduction
In the 1960s, hip replacement revolutionized management of patients affected by hip osteoarthritis, and nowadays total hip arthroplasty (THA) is widely considered one of the most successful procedures producing excellent outcomes, being named the operation of the century in orthopaedical and traumatological fields. Instability and dislocation after THA are a common reason for revision surgery and therefore they are perceived as a serious complication by both surgeons and patients [
1].
Instability following THA is a multi-factorial event, with different etiologies, and eventually several categories of risk factors are recognized, related to the patients and/or to the surgeons’ choice: primary diagnosis such as femoral neck fracture and post-traumatic arthritis, secondary diagnosis at the neighbor joints such as spino-pelvic imbalance, neurological and psychiatric disorders such as Parkinson’s disease, epilepsy, and schizophrenia, implant orientation and design, and laxity of the surrounding soft tissues [
2,
3,
4].
The concept of dual mobility (DM) was thought up in the 1970s and combined two articulations: one large and one smaller by a recruitment phenomenon increasing the jumps distance and so decreasing dislocation forces, with advantages of large head without adverse effects. Use of first-generation DM was limited worldwide due to concern regarding the fact that the cup, to avoid the flowing of polyethylene (PE) debris and among the plugs of the metallic shell, did not have holes for implementation of fixation with additional screws whether required; such a design also did not allow to check for the proper seating of the cup into the reamed acetabulum. Furthermore, wear of the PE could lead to macrophagic reaction and consequent periprosthetic osteolysis and mechanical failure [
5,
6].
The scope of this prospective single-center study is to report on the preliminary outcomes achieved with the use of a novel dual mobility cup—with holes and macrostructures on the back of the cup, in order to have better mechanical support, with a modular metallic inlay and using crosslinked PE-implanted in subjects at risk for luxation of the THA. To our knowledge, there is no paper in English that describes the system proposed.
2. Material and Methods
We prospectively evaluated the records of 32 consecutive cases of patients who underwent primary THR using a novel DM acetabular system; exclusion criteria included patients with less than two-year minimum follow-up and patients with active or previous hip joint infection. Study protocol was in accordance with the Declaration of Helsinki for human research. For each patient, the complete medical history was collected. The cohort of patients were composed by 17 women and 14 men. One female patient underwent bilateral THA consecutively, not simultaneously. The mean age was 60.8 years (range 23–84) and the mean follow-up was 39.6 months (24–50). The right hip was operated in 19 cases, the left in 13.
Preoperatively clinical assessment was done using the Harris hip score (HHS): the preoperative HHS was 54.7 on average (range, 47–64); for radiological evaluation an anteroposterior pelvic radiograph was obtained to estimate the predicted cup size. Templating was performed by two fellowship-trained orthopedic surgeons. The main diagnosis that had led to the operations was: 14 primary hip osteoarthritis, 11 intracapsular fracture of the femoral neck, 6 post-traumatic osteoarthritis after internal fixation of acetabular fracture and 1 conversion to THA of a failed osteosynthesis with an intramedullary nail due to intertrochanteric fracture.
Informed consent was obtained from all patients. Concomitant diseases, considered as risk factors for THA instability, were registered as follows: Parkinson disease in 6 cases, schizophrenia in 2 case, epilepsy in 4 cases, hip-spine syndrome in 10 cases.
All patients were intravenously administered an antibiotic prophylaxis using 2 g of Cefazolin during the operation and 1 g every 6 h for a total of 3 postoperative doses. In general anesthesia or combined spinal-epidural anesthetic all the THAs were implanted using the direct lateral approach (with patient laying in lateral decubitus position on the contralateral unaffected side) in a conventional turbulent flow theatre. Operations were done by 3 senior orthopedic surgeons; none was performed by a trainee as first surgeon, even under supervision
The acetabular component (G7 Dual Mobility Acetabular system
®, Zimmer-Biomet, Warsaw, Indiana, USA) is a 3D porous titanium alloy acetabular cup with a mean pore size of 475 microns, 70% porosity, and a coefficient of friction of 1.25. A multi-hole design for the acetabular cup was used in all cases (
Figure 1): it was press-fit after progressive reaming of the acetabular cavity, with an intended inclination angle at 40°–50° and an intended anteversion at 10°–20°. The diameter of the acetabular component ranged from 48 mm to 58 mm as follows: size 50 in 10 cases, size 52 in 8 cases, size 54 in 5 case, size 56 in 4 cases, size 48 in 3 cases, and size 58 in 2 cases. Two or more additional acetabular screws were used in 14 cases to implement fixation whether the press-fit stability was in question, or where the bone quality was not optimal, and according to the preference of the surgeon; in these cases protrusion of the screw head must obviously be avoided to allow for the proper seating of the metallic modular liner.
The chrome-cobalt definitive liner implant was manually introduced, after ensuring that the interior of the shell and all tapers were dry. A polar pilot hole allows the taper interface to properly be aligned for seating of the definitive metal liner, that should be impacted with several moderate mallet strikes. Thereafter it is compulsory to visually verify whether the ring is fully seated against the face of the liner: when properly seated, the liner will sit flush with the face of the shell.
Two different types of crosslinked PE were used: ArCom XL® used in 9 cases, and antioxidant vitamin-E infused E1® in 23 cases.
On the femoral side in all cases we implanted cementless stems: 19 Taperloc, 9 CLS, 3 Conus and 1 Arcos (all manufactured by Zimmer-Biomet, Warsaw, Indiana, USA). Progressive broaches were manually used to prepare the femoral medullary canal until resistance against the inner cortex was felt; the chosen stem was then inserted by guiding it with its appropriate device, aiming to obtain approximately 10–20° of anteversion.
Before closure in layers, the stability of the hip implant was assessed examining the primary arc range of motion. Perioperative care was the same for all patients: thromboembolic prophylaxis with low molecular weight heparin was administered for five weeks; during the same period of time patients used compression stockings. Passive motion exercises with the assistance of a therapist started immediately after the operation; patients were free to walk with two supports after 3 days for about 6 weeks and thereafter full weight-bearing was usually allowed.
3. Results
All statistical analyses were performed using MedCalc Version 18.2.1. Quantitative variables were analyzed using a Student’s t-test. A p value of less than 0.05 was considered statistically significant. A clinical and radiographic evaluation was performed at 1, 3, 6, 12 months postoperatively and annually thereafter. All patients completed the HHS pre-operatively and at a minimum of two-years post-operatively. At the last follow-up the Harris Hip Score (HHS) was submitted to the patients. All patients declared that they were satisfied with the results of surgery, showed clinical improvement, and walked normally without any help at 3 months after surgery, the mean HHS being raised up to a mean value of 88.4 (range, 84–93). This improvement was statistically significant (p < 0.0001). No clear relationship between HHS, gender, age, diagnosis, and prosthetic components dimension were seen in this study. Radiologically, any sign of tilting/loosening/migration of the acetabular component was documented. All eventual local complications, as intraoperative periprosthetic fracture, periprosthetic infection, dislocation, breakages of the polyethylene and/or of the head, dissociation within the prosthesis, were recorded. Any eventual clicking and/or squeaking was also recorded. Failure was defined when a subjective feeling of instability was referred and/or whether a revision surgery for any cause was needed, because this is a firm, objective endpoint.
None of the patients enrolled in this study sustained a postoperative dislocation at a mean follow-up of 39.6 months. Furthermore, no patients sustained modular liner dissociation or an intraprosthetic dislocation. As such, survivorship free from dislocation was 100% at both 2 and 5 years.
One patient (3.12%) experienced a complication and he underwent a superficial irrigation and debridement for a superficial wound infection without deep penetration at 1 month postoperatively.
4. Discussion
Dislocation after THA has become a significant problem, surpassing aseptic loosening; DM implants are currently selected particularly often for patients at high risk of postoperative instability.
Fractures of the femoral neck in elderly population are very common in orthopedic practice and THA is considered the best option of treatment. The size of the femoral head is an important factor that influences the outcome of THA: implants with a 28 mm femoral head are more prone to dislocate than implants with a 32 mm head or larger. Large metal-on-metal bearings are no longer used and ceramic-on-ceramic bearings have proven long-term satisfactory outcomes, but some specific complications such as implant breakages and noise have arisen; therefore nowadays PE is still considered the best tribological option for THA in most of the patients worldwide. Obviously, a large head coupled to a polyethylene inlay can lead to more wear, osteolysis, and failure of the implant. Furthermore, patients with THA done for femoral fracture are more prone to dislocation because of the attempt to regain the complete range of motion the patient had before the fall and due to the sarcopenia of the surrounding muscular tissues in the elderly, that causes laxity of the artificial joint. The dual mobility concept is a PE insert, locked on the femoral ball-head, which moves about freely in a press-fit metallic shell, in fact realizing a compromise that conciliates two advantages: low friction (i.e., less wear) and large heads (i.e., less dislocation) [
7,
8]. In our series we do not report any dislocation of the 11 implants done for femoral neck fracture, thus demonstrating that the use of DM cups in the treatment of displaced fractures of the femoral neck appears safer in terms of the criteria of postoperative dislocation when compared to conventional cups. In their systematic review including 59 articles and 17,908 THAs, De Martino et al. [
9] reported the rate of dislocation following the use of DM acetabular components: the mean rate of dislocation was 0.9% in the primary THA group and they concluded that the use of DM acetabular components is effective in minimizing the risk of instability after THA. Eventually this benefit must be balanced against continuing concerns about the additional modularity: our little sample demonstrates no negative effects in a short follow-up period.
Some patients in our series were also affected by altered mental status or neuromuscular diseases; some authors have stated that psychological factors and mental status, such as depression, anxiety, schizophrenia, or dementia can affect outcome in primary total hip (and knee) replacement. These comorbidities determine the prevalence and are firmly associated with increased odds of adverse events, suggesting that psychological support, together with specific implants, should be rigorous steps to follow for gaining subjective and objective satisfactory clinical results [
10,
11,
12]. Dual mobility hip replacement has been also proposed in ambulatory patients with cerebral palsy in the more severe Gross Motor Function Classification System stages. [
13]
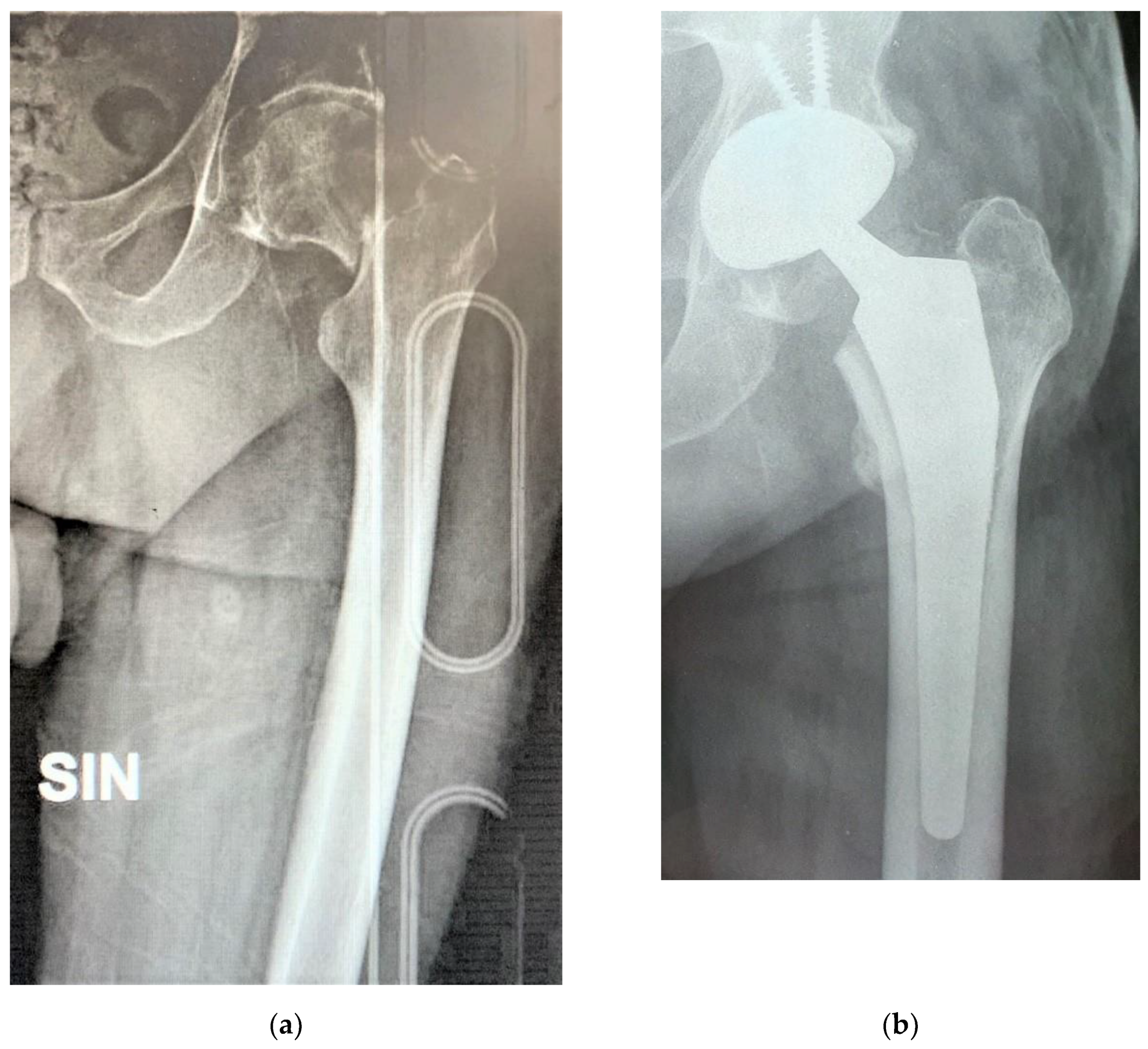
Figure 2 shows the case of a 54 years old male who was admitted to our hospital due to a displaced fracture of his left femoral neck and was in treatment since several years for depression, treated with the G7 modular cementless DM cup with 2 screws and a Taperloc stem on the femoral side.
Intertrochanteric fracture, mainly due to osteoporosis or sometimes severe trauma, is one of the most frequent fractures in orthopedic surgery and is usually treated by internal fixation. Depending on several factors, a small group of patients have complications including nonunion, malunion, avascular necrosis, or failure of the device; thus the incidence of failure of internal fixation should be encountered in a certain percentage and an option currently used is the conversion to THA.
Hip arthroplasty after failure of internal fixation is challenging, and may be complicated by dislocation in a relatively short postoperative period, because these patients were nonambulatory for a while and senile muscular hypotrophy would not be improved except with ambulation; an eventual further damage of the hip stabilizers may also be added when removing from the femur the failed internal fixation devices, sometimes with broken screws [
14,
15,
16,
17]. Archibeck et al. [
18] reported that 12 patients of their 102 who had undergone THA after failed internal fixation of proximal femoral fractures had early surgical complications related to the procedure, dislocations being 5 of them, while in their multi-center study Pui et al. claimed rates of postoperative dislocations of greater than 15% [
19]. Conversion in THA after failed internal fixation of pelvic or femoral fractures is nowadays a clear indication for DM implants; in our 7 cases (6 posttraumatic osteoarthritis and 1 conversion) we do not report any dislocation of the prosthesis.
Concurrent hip and spine pathologies can alter the biomechanics of spinopelvic mobility in primary THA, and a too high THA dislocation rate has been demonstrated among THA patients with concurrent spinopelvic malalignment. The risk of dislocation increases especially within the first six months in patients who had previously undergone a lumbar fusion involving the sacrum and in patients affected by a sagittal imbalance due to concomitant degenerative pathology of the hip and lumbosacral spine (“hip-spine syndrome”) and therefore surgeons should take care with component positioning and must consider modular implants to adapt the prosthesis to the morphometric differences of patients, to allow better accuracy in restoring the anatomy and biomechanics of hip joint. In fact, in the above-mentioned scenarios, the degree of lumbar spine lordosis cannot change to allow the pelvis to tilt so that the range of movement demanded from the replaced hip is greater than that required in a normal THA and higher stability implants, such as DM components, must be considered in this high-risk cohort [
20,
21,
22,
23,
24,
25,
26].
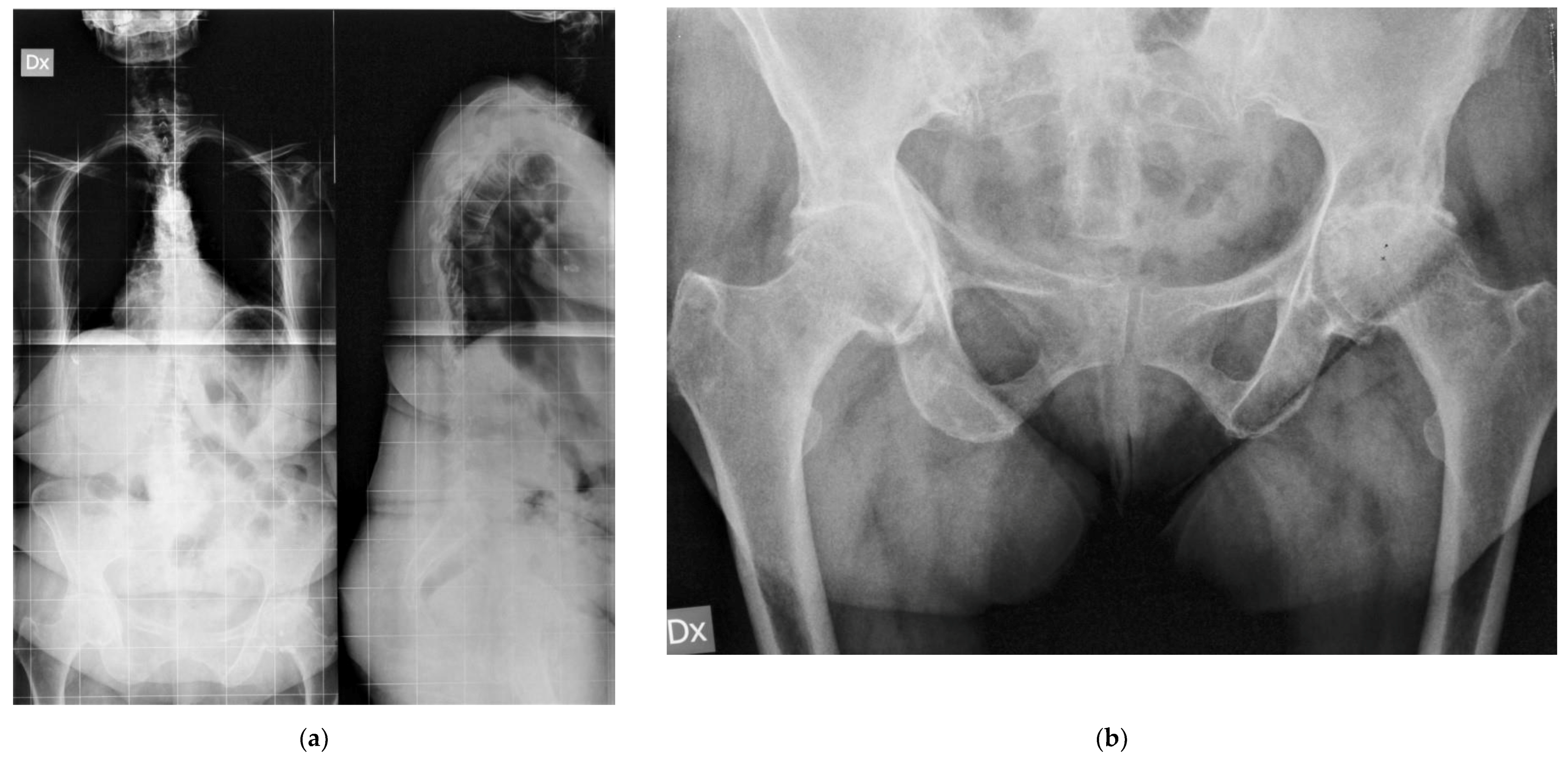
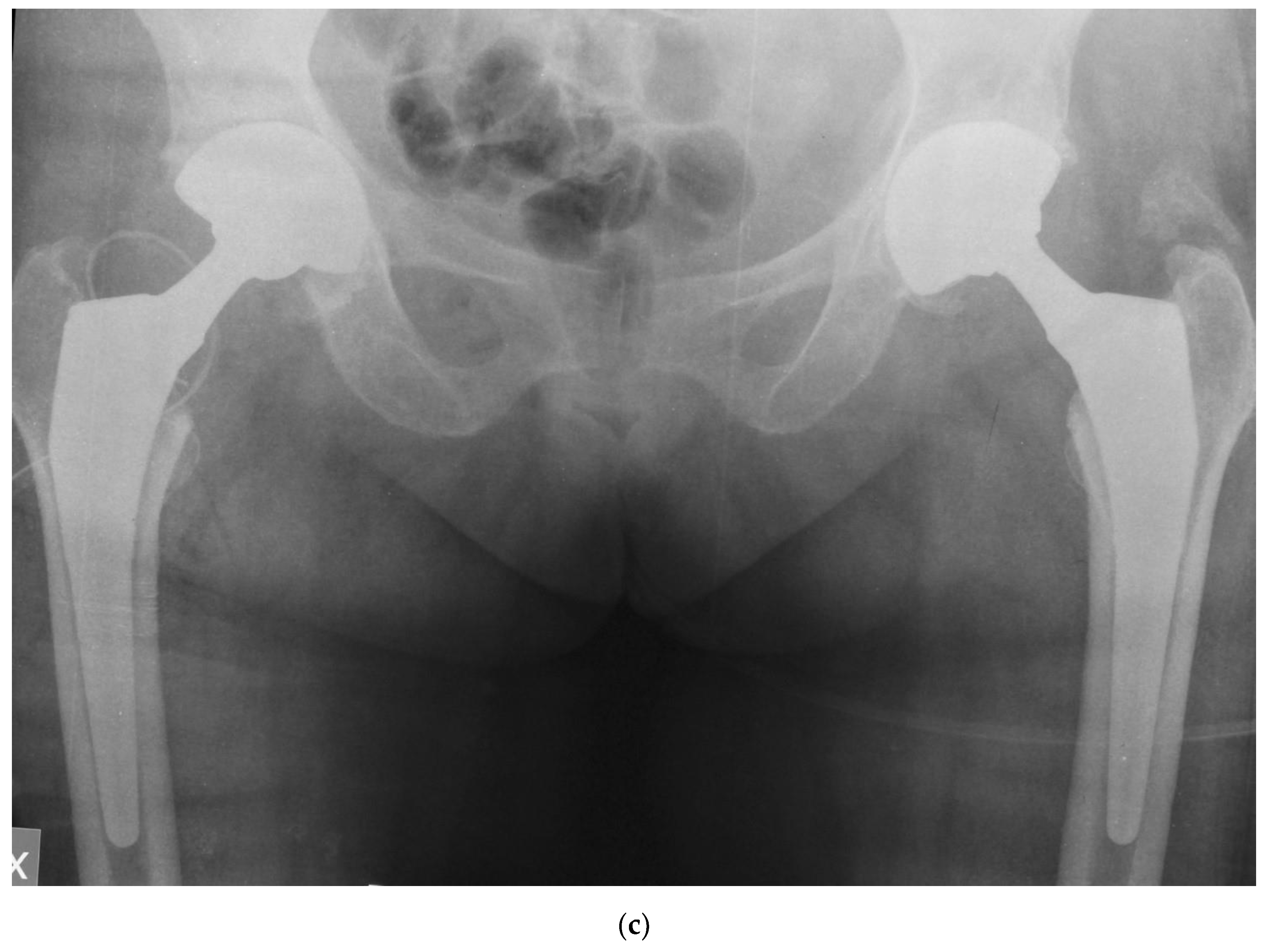
Figure 3 shows the case of a 68 years old female, who was referred to our unit due to persistent low back pain for vertebral steno-instability and consequent sagittal imbalance to undergo spinal lumbo-sacral fusion; clinical and radiological examinations revealed a concomitant severe osteoarthritis in both her hips that was treated with bilateral THA with the G7 modular cementless DM cup. After surgical treatment in the hips, low back pain improved dramatically, and the patient did not need any surgery in her spine.
In conclusion, despite decades of investigating improvements in implant design and surgical technique, dislocation following primary THA remains a concern. Our study confirms, using a novel modular acetabular component, that DM implants can avoid this complication, even in patients considered at risk.
Our study has some limitations: first, it is a preliminary report of a small sample size, in the absence of a control group, and with a short follow-up. However, this has ensured that all the patients were eligible at the final follow-up. Second, we have not measured biomechanical parameters in the coronal plane such as vertical and horizontal femoral offset, and abduction of the cup. Finally, despite the liner is in CoCr alloy and the shell is in titanium alloy, we have not monitored metal ion levels.
In conclusion, despite the above-mentioned limitations, our prospective single center study shows that the modular DM socket provides dual articulation, larger jump distance, and greater range of motion before impingement, which significantly reduce the rate of dislocation. Further studies with large cohorts are needed to demonstrate the superiority of this implant compared to conventional ones even at longer follow-up.


 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}



