Comparison of Canine-Guided Occlusion with Other Occlusal Schemes in Removable Complete Dentures: A Systematic Review

 ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Question
2.2. Search Strategy and Eligibility Criteria
2.3. Quality Assessment of the Included Articles
3. Results
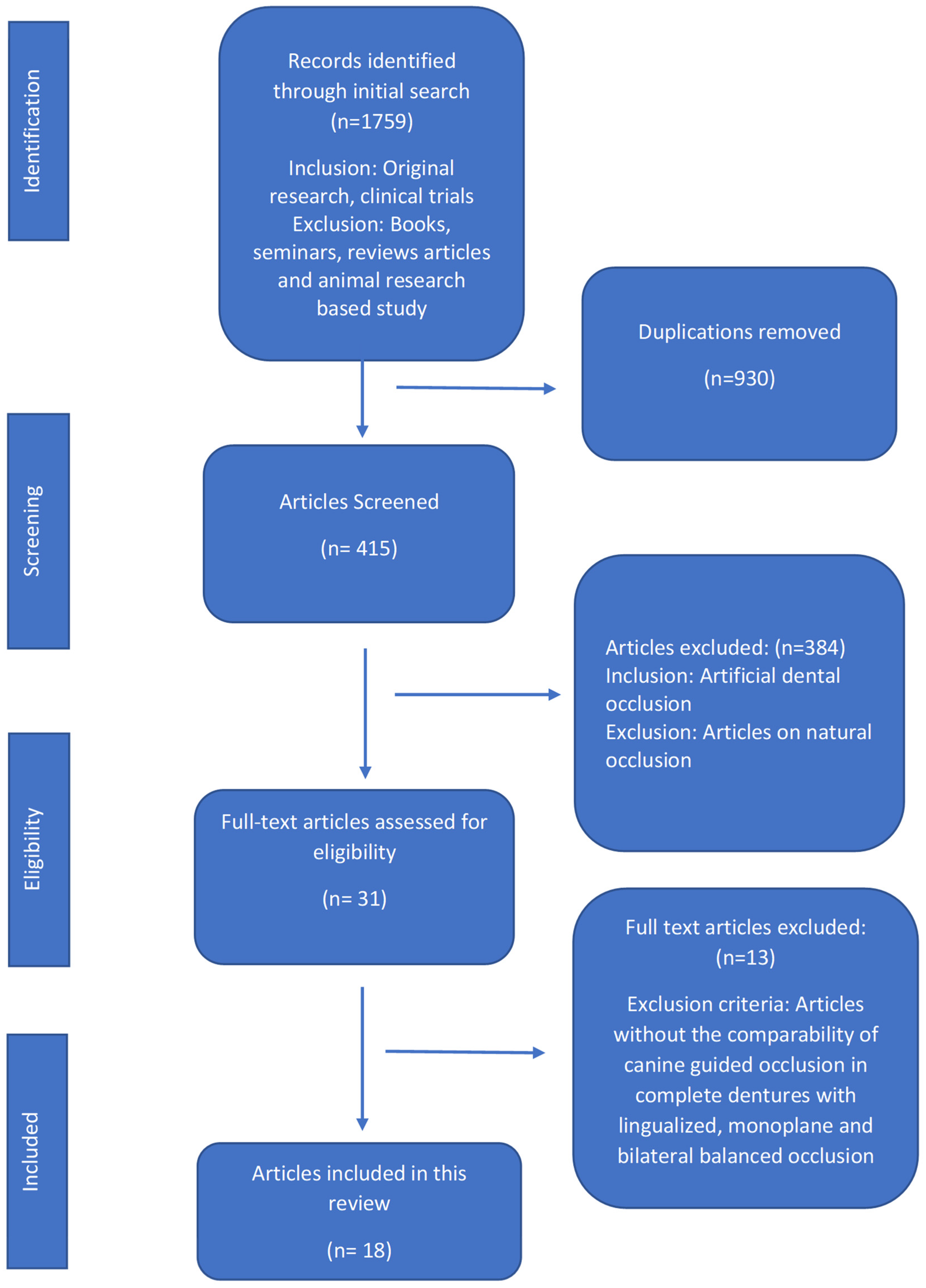
3.1. Search Results
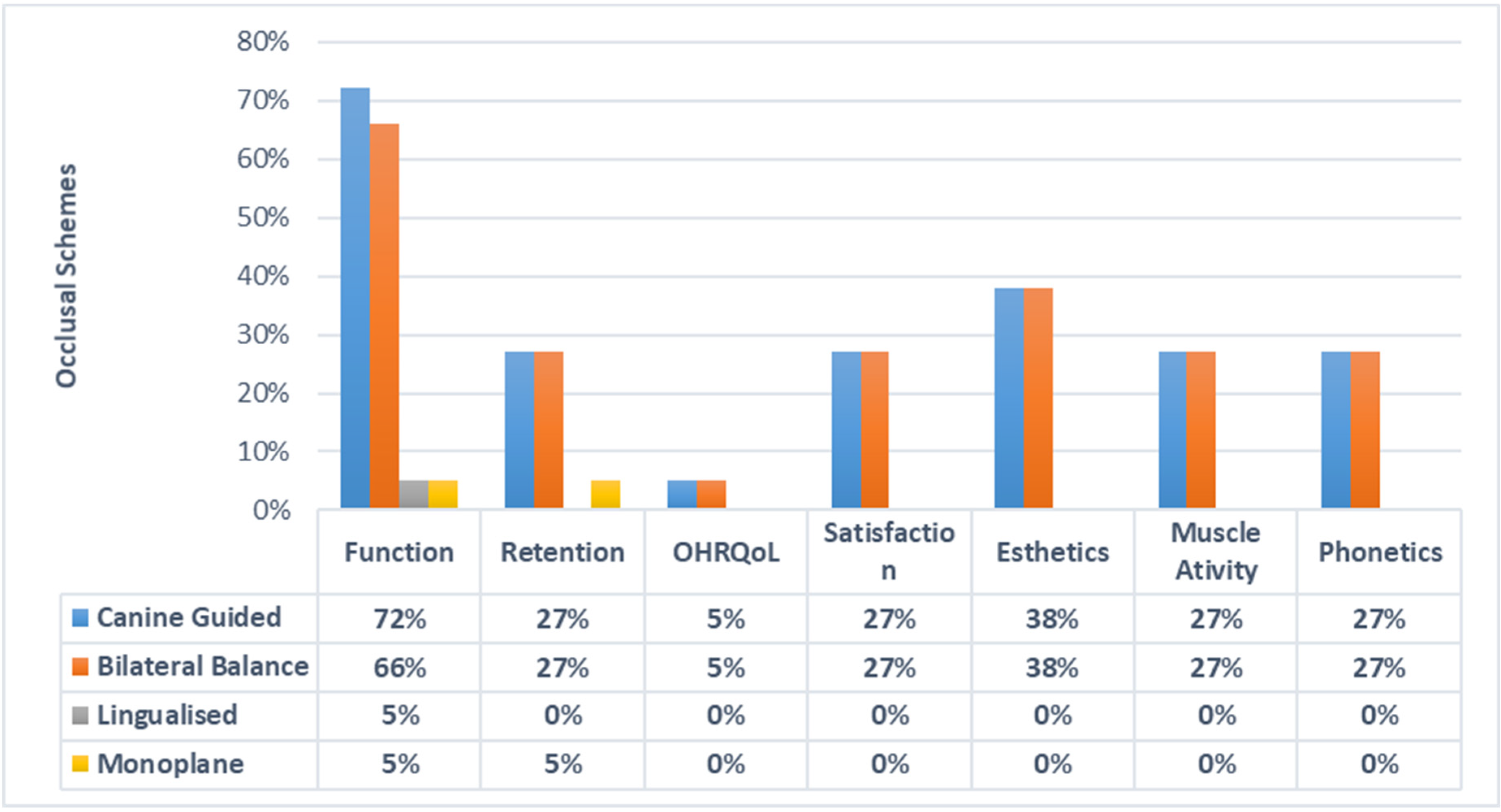
3.2. Assessment of Various Occlusal Schemes from the Included Articles
3.3. Results of Quality Assessment
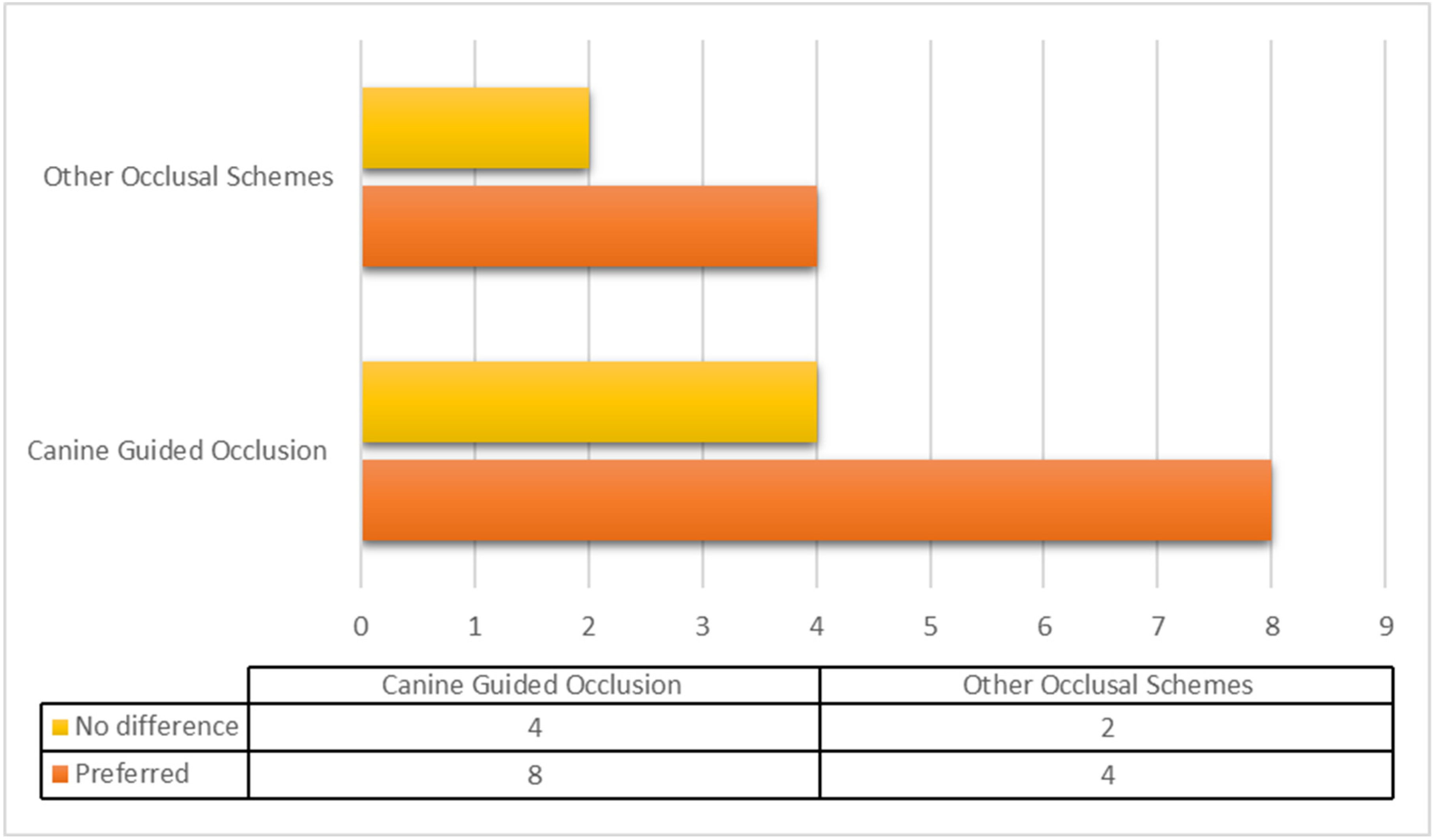
3.4. General Outcomes of Included Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schierz, O.; Reissmann, D. Influence of guidance concept in complete dentures on oral health related quality of life–Canine guidance vs. bilateral balanced occlusion. J. Prosthodont. Res. 2016, 60, 315–320. [Google Scholar] [CrossRef]
- Bilhan, H.; Geckili, O.; Ergin, S.; Erdogan, O.; Ates, G. Evaluation of satisfaction and complications in patients with existing complete dentures. J. Oral Sci. 2013, 55, 29–37. [Google Scholar] [CrossRef] [Green Version]
- Shamsolketabi, S.; Nili, M. The effect of denture adhesive on the efficiency of complete denture in patients with different alveolar ridges. Dent. Res. J. 2018, 15, 271–275. [Google Scholar]
- Zhao, K.; Mai, Q.; Wang, X.; Yang, W.; Zhao, L. Occlusal designs on masticatory ability and patient satisfaction with complete denture: A systematic review. J. Dent. 2013, 41, 1036–1042. [Google Scholar] [CrossRef]
- Maddula, R.T.; Ariga, P.; Jain, A.R. Systematic review of masticatory efficiency with different occlusal scheme in conventional complete dentures. Drug Invent. Today 2018, 10, 1626–1631. [Google Scholar]
- El-Shoukouki, A.H.; Fuad, M.M. Maxillary Acrylic Denture Base Deformation as Related To Different Occlusal Concepts for Complete Denture. Egypt. Dent. J. 2007, 53, 1. [Google Scholar]
- Heydecke, G.; Akkad, A.S.; Wolkewitz, M.; Vogeler, M.; Türp, J.C.; Strub, J.R. Patient ratings of chewing ability from a randomised crossover trial: Lingualised vs. first premolar/canine-guided occlusion for complete dentures. Gerodontology 2007, 24, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, G.; Omar, R. The future of complete dentures in oral rehabilitation. A critical review. J. Oral Rehabil. 2010, 37, 143–156. [Google Scholar] [CrossRef] [PubMed]
- Pero, A.C.; Scavassin, P.M.; Policastro, V.B.; de Oliveira Júnior, N.M.; Marin, D.O.M.; da Silva, M.D.D.; Cassiano, A.F.B.; de Sousa Santana, T.; Compagnoni, M.A. Masticatory function in complete denture wearers varying degree of mandibular bone resorption and occlusion concept: Canine-guided occlusion versus bilateral balanced occlusion in a cross-over trial. J. Prosthodont. Res. 2019, 63, 421–427. [Google Scholar] [CrossRef]
- Brandt, S.; Danielczak, R.; Kunzmann, A.; Lauer, H.; Molzberger, M. Prospective clinical study of bilateral balanced occlusion (BBO) versus canine-guided occlusion (CGO) in complete denture wearers. Clin. Oral Investig. 2019, 23, 4181–4188. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Wells, G.A.; Shea, B.; O’Connell, D. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2011. [Google Scholar]
- Peroz, I.; Leuenberg, A.; Haustein, I.; Lange, K. Comparison between balanced occlusion and canine guidance in complete denture wearers—A clinical, randomized trial. Quintessence Int. 2003, 34, 607–612. [Google Scholar] [PubMed]
- Farias Neto, A.; Mestriner Junior, W.; da Fonte Porto Carreiro, A. Masticatory efficiency in denture wearers with bilateral balanced occlusion and canine guidance. Braz. Dent. J. 2010, 21, 165–169. [Google Scholar] [CrossRef]
- Abdelhamid, A.M.; Hanno, K.I.; Imam, M.H. A prospective cross-over study to evaluate the effect of two different occlusal concepts on the masseter muscle activity in implant-retained mandibular overdentures. Int. J. Implant Dent. 2015, 1, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Afzal, M.; Majeed, M.I.; Mirza, B.A.Q. Assessment of patient satisfaction and Masticatory efficiency with balanced occlusion compared to canine Guided occlusion in complete denture wearers. Pak. Oral Dent. J. 2017, 37, 504–509. [Google Scholar]
- Bolla, V.L.; Bondugula, V.; Munnangi, S.R.; Tandu, A. Comparison of patient satisfaction in complete denture patients with different occlusal schemes. Int. J. Appl. Dent. Sci. 2017, 3, 51–52. [Google Scholar]
- Faten, S.A.; Nazik, A.E.; Esraa, M.A. Colorimetric comparative analysis of masticatory efficiency in complete denture wearers with two different occlusal concepts. Alex. Dent. J. 2016, 41, 117–121. [Google Scholar] [CrossRef] [Green Version]
- Maxwell, D.; Odang, R.; Koesmaningati, H. Correlation of Masticatory Muscle Activity with Masticatory Ability in Complete Denture Patients with Canine Guidance and Balanced Occlusion. J. Phys. Conf. Ser. 2017, 884, 1–7. [Google Scholar] [CrossRef]
- Abdelhamid, A.M.; Hanno, K.I.H.; Imam, M.H. The effect of two different occlusal concepts on the masseter muscle activity in implant retained mandibular overdentures. J. Dent. Implants 2017, 7, 20. [Google Scholar]
- Hofmann, M.; Knauer, G. Studies on canine guidance in complete dentures. Dtsch. Zahnarztl. Z. 1990, 45, 566–570. [Google Scholar] [PubMed]
- Compagnoni, M.A.; Leles, C.R.; Barbosa, D.B.; Valverde, G.B. Oclusão em dentaduras completas: Estudo comparativo entre oclusão balanceada bilateral e desoclusão pelo canino. Rev. CROMG 2002, 8, 92–97. [Google Scholar]
- Miralles, R.; Bull, R.; Manns, A.; Roman, E. Influence of balanced occlusion and canine guidance on electromyographic activity of elevator muscles in complete denture wearers. J. Prosthet. Dent. 1989, 61, 494–498. [Google Scholar] [CrossRef]
- Paleari, A.; Marra, J.; Rodriguez, L.; De Souza, R.; Pero, A.C.; De Assis Mollo Júnior, F., Jr.; Compagnoni, M.A. A cross-over randomised clinical trial of eccentric occlusion in complete dentures. J. Oral Rehabil. 2012, 39, 615–622. [Google Scholar] [CrossRef] [PubMed]
- Rehmann, P.; Balkenhol, M.; Ferger, P.; Wöstmann, B. Influence of the occlusal concept of complete dentures on patient satisfaction in the initial phase after fitting: Bilateral balanced occlusion vs canine guidance. Int. J. Prosthodont. 2008, 21, 1. [Google Scholar]
- Motwani, B.; Sidhaye, A. The need of eccentric balance during mastication. J. Prosthet. Dent. 1990, 64, 689–690. [Google Scholar] [CrossRef]
- Trapozzano, V.R. Tests of balanced and nonbalanced occlusions. J. Prosthet. Dent. 1960, 10, 476–487. [Google Scholar] [CrossRef]
- Jaafar Abduo, B.; DclinDent, M. Occlusal schemes for complete dentures: A systematic review. Int. J. Prosthodont. 2013, 26, 26–33. [Google Scholar] [CrossRef]
- Akören, A.; Karaačaçliočlu, L. Comparison of the electromyographic activity of individuals with canine guidance and group function occlusion. J. Oral Rehabil. 1995, 22, 73–77. [Google Scholar] [CrossRef]
- Ximinis, E.; Tortopidis, D. Electromyographic activity changes of jaw-closing muscles in patients with different occlusion schemes after fixed prosthetic restoration. Balk. J. Dent. Med. 2018, 22, 157–162. [Google Scholar] [CrossRef] [Green Version]
- Michielin, M.; Daniani, M.G.; Orthlieb, J.D.; Simon, J. Statistical analysis of functional interrelations between anterior guidance and posterior determinants. Cah. Prothese 1990, 70, 52–65. [Google Scholar]
- Abduo, J.; Tennant, M.; Mcgeachie, J. Lateral occlusion schemes in natural and minimally restored permanent dentition: A systematic review. J. Oral Rehabil. 2013, 40, 788–802. [Google Scholar] [CrossRef]
- Jemt, T.; Lundquist, S.; Hedegard, B. Group function or canine protection. J. Prosthet. Dent. 2004, 91, 403–408. [Google Scholar] [CrossRef]
- Thalji, G.; McGraw, K.; Cooper, L.F. Maxillary Complete Denture Outcomes: A Systematic Review of Patient-Based Outcomes. Int. J. Oral Maxillofac. Implants 2016, 31, 169–181. [Google Scholar] [CrossRef]
- Sabir, S.; Regragui, A.; Merzouk, N. Maintaining occlusal stability by selecting the most appropriate occlusal scheme in complete removable prosthesis. Jpn. Dent. Sci. Rev. 2019, 55, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Marchini, L. Patients’ satisfaction with complete dentures: An update. Braz. Dent. Sci. 2014, 17, 5–16. [Google Scholar] [CrossRef]
- Aarts, J.M.; Payne, A.G.; Thomson, W.M. Patients’ evaluation of two occlusal schemes for implant overdentures. Clin. Implant Dent. Relat. Res. 2008, 10, 140–156. [Google Scholar] [CrossRef] [PubMed]
- Palla, S. Occlusal considerations in complete dentures. In Science and Practice of Occlusion; Quintessence: Batavia, IL, USA, 1997. [Google Scholar]
- Rangarajan, V.; Yogesh, P.B.; Gajapathi, B.; Ibrahim, M.M.; Kumar, R.G.; Karthik, M. Concepts of occlusion in prosthodontics: A literature review, part II. J. Indian Prosthodont. Soc. 2016, 16, 8–14. [Google Scholar]
- Imran, T.; Ahmed, N.; Nazeer, B. Pattern of occlusal contacts in intercuspal position of natural teeth. Int. J. Dent. Res. 2016, 4, 19–21. [Google Scholar] [CrossRef] [Green Version]
- Jain, P.; Rathee, M. Stability in Mandibular Denture; StatPearls Publishing LLC: Treasure Island, FL, USA, 2020. [Google Scholar]
- Lemos, C.; Verri, F.; Gomes, J.; Santiago Júnior, J.; Moraes, S.; Pellizzer, E. Bilateral balanced occlusion compared to other occlusal schemes in complete dentures: A systematic review. J. Oral Rehabil. 2018, 45, 344–354. [Google Scholar] [CrossRef] [PubMed]
- Abduo, J.; Bennamoun, M.; Tennant, M.; McGeachie, J. Effect of prosthodontic planning on lateral occlusion scheme: A comparison between conventional and digital planning. J. Appl. Oral Sci. 2015, 23, 196–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iegami, C.M.; de Melo Lopes, D.; Nakamae, A.E.M.; Uehara, P.N.; Tamaki, R. Different occlusal schemes in a persistent protruding complete denture wearer. Case Rep. Dent. 2016, 2016, 7418686. [Google Scholar] [CrossRef] [Green Version]
- Bhambhani, R.; Joshi, S.; Roy, S.S.; Shinghvi, A. Choosing the denture occlusion-A Systematic review. J. Indian Prosthodont. Soc. 2020, 20, 269. [Google Scholar] [PubMed]
- Berg, E. Acceptance of full dentures. Int. Dent. J. 1993, 43, 299–306. [Google Scholar] [PubMed]
- Čelebić, A.; Knezović-Zlatarić, D.; Papić, M.; Carek, V.; Baučić, I.; Stipetić, J. Factors related to patient satisfaction with complete denture therapy. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2003, 58, M948–M953. [Google Scholar] [CrossRef] [Green Version]
- Habib, S.R.; Azad, A.A. Comparison of patient’s satisfaction with replacement complete dentures fabricated by copy denture technique versus conventional technique. J. Pak. Dent. Assoc. 2009, 18, 9–13. [Google Scholar]
- Tarazi, E.; Ticotsky-Zadok, N. Occlusal schemes of complete dentures—A review of the literature. Refuat Hapeh Vehashinayim 2007, 24, 56–64. [Google Scholar]
- Brewer, A.A.; Reibel, P.R.; Nassif, N.J. Comparison of zero degree teeth and anatomic teeth on complete dentures. J. Prosthet. Dent. 1967, 17, 28–35. [Google Scholar] [CrossRef]
- Clough, H.E.; Knodle, J.M.; Leeper, S.H.; Pudwill, M.L.; Taylor, D.T. A comparison of lingualized occlusion and monoplane occlusion in complete dentures. J. Prosthet. Dent. 1983, 50, 176–179. [Google Scholar] [CrossRef]
- Kawai, Y.; Ikeguchi, N.; Suzuki, A.; Kuwashima, A.; Sakamoto, R.; Matsumaru, Y.; Kimoto, S.; Iijima, M.; Feine, J.S. A double blind randomized clinical trial comparing lingualized and fully bilateral balanced posterior occlusion for conventional complete dentures. J. Prosthodont. Res. 2017, 61, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Madalli, P.; Murali, C.; Subhas, S.; Garg, S.; Shahi, P.; Parasher, P. Effect of occlusal scheme on the pressure distribution of complete denture supporting tissues: An in vitro study. J. Int. Oral Health JIOH 2015, 7, 68. [Google Scholar] [PubMed]
- Sutton, A.; McCord, J. A randomized clinical trial comparing anatomic, lingualized, and zero-degree posterior occlusal forms for complete dentures. J. Prosthet. Dent. 2007, 97, 292–298. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Study | Study Design and Participants | Prosthesis | Occlusion | Assessment Method | Follow-Up Period | Conclusions |
|---|---|---|---|---|---|---|
| Pero et al. [9] | Crossover, 30 | Complete dentures | CGO BBO | Occlusal force Mastication | 4 weeks | CGO is a viable alternative to BBO in complete dentures |
| Brandt et al. [10] | Crossover, 40 | Complete dentures | CGO BBO | Esthetics, retention Phonetics, mastication | 12 weeks | CGO can be a comfortable alternative to BBO in complete dentures |
| Schierz et al. [1] | Randomized single-blind crossover trial, 19 | Complete dentures | CGO BBO | OHRQoL | 12 weeks | CGO and BBO are similar in terms of OHRQoL |
| Peroz et al. [14] | Randomized control trial, 22 | Complete dentures | CGO BBO | Esthetics, retention Mastication, phonetic | 12 weeks | CGO can be used successfully in complete denture treatment. CGO showed better esthetics, chewing and lower denture retention, while BBO had a limited role in the studied parameters but showed better retention in the upper denture |
| Farias et al. [15] | Double-blinded controlled crossover clinical trial, 24 | Complete denture | CGO BBO | Mastication, phonetics, esthetics Retention, patient satisfaction, comfort | 12 weeks and 24 weeks | CGO is preferred, easier and faster. BBO does not improve masticatory efficiency in complete denture wearers |
| Abdelhamid et al. [16] | Crossover, 12 | Implant-retained lower overdenture and an upper conventional complete denture | CGO BBO | Electromyography of the masseter muscles Mastication | 4 weeks | Both CGO and BBO can be used successfully in implant-retained mandibular denture as analyzed by electromyography |
| Heydecke et al. [7] | Randomized crossover, 20 | Complete denture | CGO LO | Mastication | 12 weeks | LO is not superior to CGO in chewing ability |
| Afzal et al. [17] | Randomized clinical trial, 60 | Complete denture | CGO BBO | Esthetics Retention Mastication Phonetics | 8 weeks | Occlusal schemes alone have a limited role in overall denture adaptation and satisfaction |
| Bolla et al. [18] | Clinical trial, 20 | Complete dentures | CGO BBO | Patient satisfaction Mastication Esthetics Adaptability Retention Phonetics | 12–16 weeks and yearly | BBO showed better initial adaptation in denture wearers. CGO can be used with success. Occlusion adaptation is not a crucial factor for patient adaptation |
| Faten et al. [19] | Crossover clinical trial, 20 | Complete dentures | CGO BBO | Patient satisfaction and comfort Mastication | 4 weeks | Both CGO and BBO improved the masticatory efficiency in complete denture wearers |
| Maxwell et al. [20] | Crossover clinical trial, 10 | Complete dentures | BBO CGO | Electromyography of masseter and anterior temporal muscles Mastication | 4 weeks | Masticatory ability is better when using canine-guided dentures |
| Elshoukouki et al. [6] | Crossover, 10 | Complete dentures | CGO MO BBO | Maxillary acrylic denture base deformation was measured by the strain gauge method Mastication | 8 weeks | MO is recommended for debilitated alveolar ridges |
| Abdelhamid et al. [21] | Crossover design, 12 | Implant-retained lower overdenture and an upper conventional complete denture | CGO BBO | Electromyography | 4 weeks | CGO is similar to BBO in terms of masticatory muscle activity |
| Hofmann et al. [22] | Single maxillary complete denture | CGO BBO | Occlusal analysis mastication | NM | It appeared that canine-guided dentures led to considerable dislocations during tooth-guided lateral movements, BBO generated less disocclusion and denture movement | |
| Compagnoni et al. [23] | Randomized control trials, 15 | Complete denture | CGO BBO | Mastication | NM | CGO-prescribed dentures report lateral disocclusion but no functional impairment in patients |
| Miralles et al. [24] | Clinical trial, 9 | Complete dentures | CGO BBO | Electromyography | 12 weeks | CGO showed low muscle activity in function, and it is helpful in preventing parafunctional activity in edentulous patients |
| Paleari et al. [25] | Randomized clinical trial, 44 | Complete dentures | CGO BBO | Denture satisfaction questionnaire and kinesiograph instrument | 4 weeks | Occlusal scheme alone has no effect on denture satisfaction and kinesiographic analysis, except for the lower vertical intrusion of the maxillary denture with CGO |
| Rehmann et al. [26] | Clinical single-blind trial, 38 | Complete dentures | CGO BBO | Patient satisfaction and comfort | 2 weeks and 4 weeks | Patients preferred BBO in complete dentures when compared with CGO |
| Study | Patient Randomization | Blinding | Withdrawal/Dropout mentioned | Statistics Applied | Sample Size | Inclusion/Exclusion Criteria Clear | Occlusal Performance Measurement | Method of Error Assessment | Quality of Study | |
|---|---|---|---|---|---|---|---|---|---|---|
| Participants’ | Assessor | |||||||||
| Pero et al. [9] | Yes | UC | No | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Brandt et al. [10] | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Schierz et al. [1] | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Peroz et al. [14] | Yes | No | UC | UC | UC | Yes | No | UC | Yes | M |
| Farias et al. [15] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Abdelhamid et al. [16] | No | No | No | No | Yes | Yes | Yes | Yes | Yes | M |
| Heydecke et al. [7] | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | Low |
| Afzal et al. [17] | Yes | No | No | No | Yes | Yes | Yes | Yes | Yes | Low |
| Bolla et al. [18] | No | UC | No | No | Yes | Yes | Yes | Yes | UC | M |
| Faten et al. [19] | Yes | UC | No | No | Yes | Yes | Yes | Yes | Yes | Low |
| Maxwell et al. [20] | Yes | UC | No | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Elshoukouki et al. [6] | No | No | No | No | Yes | Yes | Yes | Yes | Yes | M |
| Abdelhamid et al. [21] | No | No | No | No | Yes | Yes | Yes | Yes | Yes | M |
| Hofmann et al. [22] | No | No | No | No | Yes | Yes | Yes | Yes | Yes | M |
| Compagnoni et al. [23] | No | No | No | No | Yes | Yes | Yes | Yes | Yes | M |
| Miralles et al. [24] | No | No | No | No | No | Yes | Yes | No | Yes | High |
| Paleari et al. [25] | Yes | UC | No | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Rehmann et al. [26] | Yes | Yes | No | UC | UC | Yes | No | UC | Yes | M |
| Author ID | Selection | Comparability | Exposure | Newcastle–Ottawa Quality (Total) |
|---|---|---|---|---|
| Pero et al. [9] | **** | * | ** | Seven |
| Brandt et al. [10] | **** | * | *** | Eight |
| Schierz et al. [1] | *** | * | ** | Six |
| Peroz et al. [14] | *** | * | ** | Six |
| Farias et al. [15] | **** | * | *** | Eight |
| Abdelhamid et al. [16] | *** | * | ** | Six |
| Heydecke et al. [7] | **** | * | *** | Eight |
| Afzal et al. [17] | *** | * | *** | Seven |
| Bolla et al. [18] | *** | * | ** | Six |
| Faten et al. [19] | *** | * | ** | Six |
| Maxwell et al. [20] | *** | * | *** | Seven |
| Elshoukouki et al. [6] | *** | * | ** | Six |
| Abdelhamid et al. [21] | *** | * | ** | Six |
| Hofmann et al. [22] | *** | * | ** | Six |
| Compagnoni et al. [23] | *** | * | ** | Six |
| Miralles et al. [24] | *** | * | ** | Six |
| Paleari et al. [25] | *** | * | *** | Seven |
| Rehmann et al. [26] | *** | * | *** | Seven |
| Occlusal Schemes | Follow-Up Period | Conventional Denture | Implant-Retained Denture |
|---|---|---|---|
| Canine-guided occlusion | 88.88% | 88.88% | 11.11% |
| Bilateral balanced occlusion | 83.33% | 83.33% | 11.11% |
| Lingualized occlusion | 5.55% | 5.55% | 0% |
| Monoplane occlusion | 5.55% | 5.55% | 0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmed, N.; Humayun, M.A.; Abbasi, M.S.; Jamayet, N.B.; Habib, S.R.; Zafar, M.S. Comparison of Canine-Guided Occlusion with Other Occlusal Schemes in Removable Complete Dentures: A Systematic Review. Prosthesis 2021, 3, 85-98. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis3010009
Ahmed N, Humayun MA, Abbasi MS, Jamayet NB, Habib SR, Zafar MS. Comparison of Canine-Guided Occlusion with Other Occlusal Schemes in Removable Complete Dentures: A Systematic Review. Prosthesis. 2021; 3(1):85-98. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis3010009
Chicago/Turabian StyleAhmed, Naseer, Muhammad Anas Humayun, Maria Shakoor Abbasi, Nafij Bin Jamayet, Syed Rashid Habib, and Muhammad Sohail Zafar. 2021. "Comparison of Canine-Guided Occlusion with Other Occlusal Schemes in Removable Complete Dentures: A Systematic Review" Prosthesis 3, no. 1: 85-98. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis3010009