
Comprehensive Management of Severe Dental Fluorosis with Adhesively Bonded All-Ceramic Restorations


Abstract
:1. Introduction
2. Clinical Report
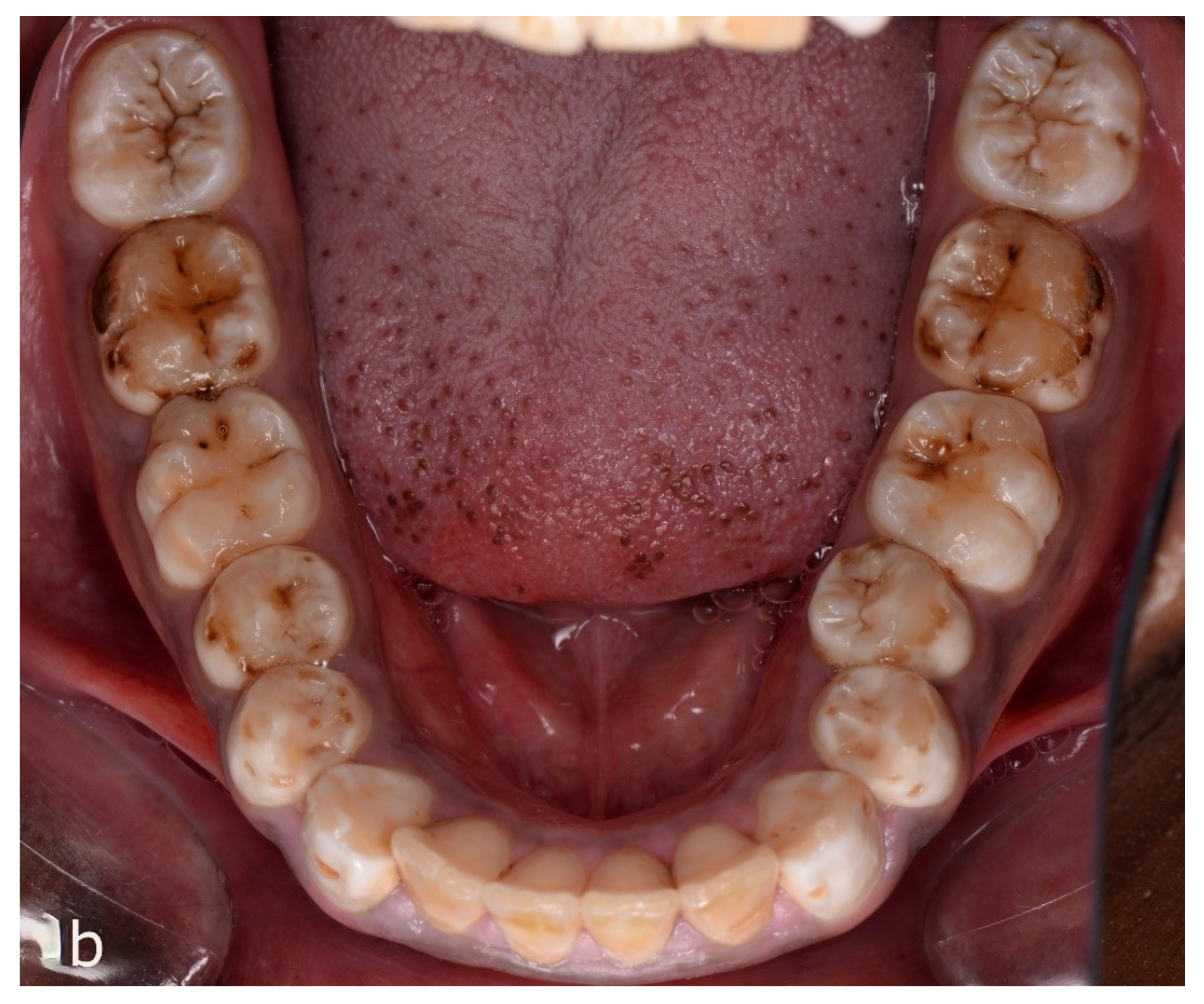
2.1. Intraoral Examination
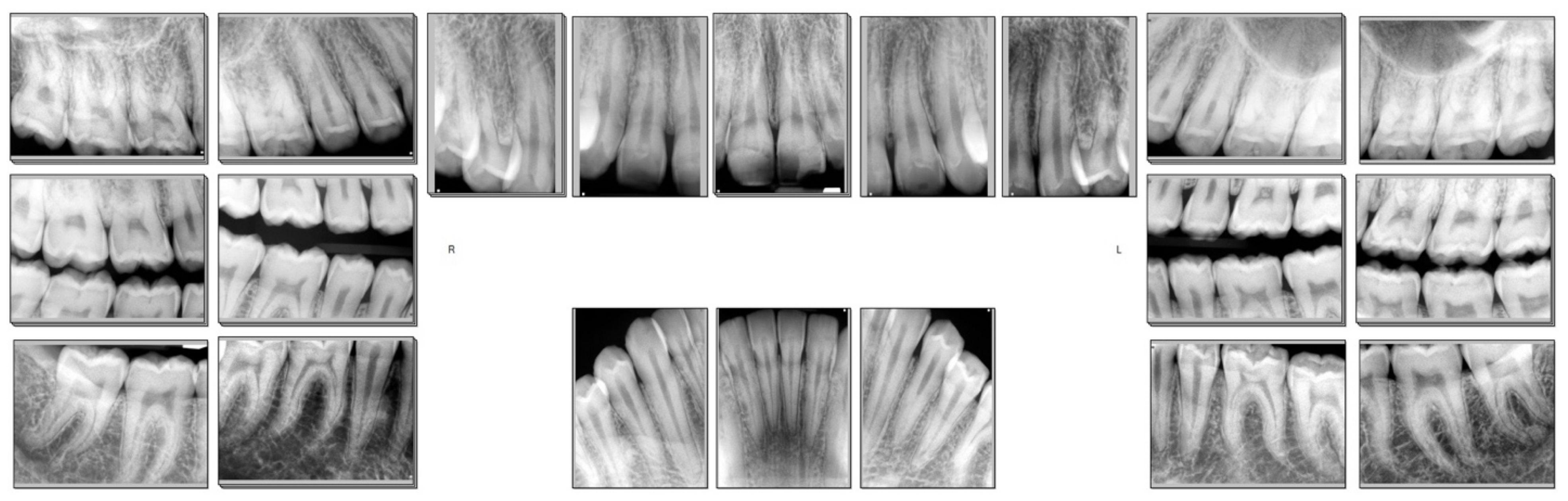
2.2. Diagnostic Work Up
2.3. Treatment Rendered
2.4. Follow Up
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Den Besten, P.K. Dental fluorosis: Its use as a biomarker. Adv. Dent. Res. 1994, 8, 105–110. [Google Scholar] [CrossRef]
- Den Besten, P.K.; Thariani, H. Biological mechanisms of fluorosis and level and timing of systemic exposure to fluoride with respect to fluorosis. J. Dent. Res. 1992, 71, 1238–1243. [Google Scholar] [CrossRef]
- Thylstrup, A.; Fejerskov, O. clinical appearance of dental fluorosis in permanent teeth in relation to histologic changes. Community Dent. Oral. Epidemiol. 1978, 6, 315–328. [Google Scholar] [CrossRef] [PubMed]
- Cunha-Cruz, J.; Nadanovsky, P. Dental fluorosis increases caries risk. J. Evid. Based. Dent. Pract. 2005, 5, 170–171. [Google Scholar] [CrossRef]
- Ibrahim, Y.E.; Bjorvatn, K.; Birkeland, J.M. Caries and dental fluorosis in a 0.25 and a 2.5 ppm fluoride area in the Sudan. Int. J. Paediatr. Dent. 1997, 7, 161–166. [Google Scholar] [CrossRef]
- Ramesh, M.; Narasimhan, M.; Krishnan, R.; Aruna, R.M.; Kuruvilla, S. The effect of fluorosis on human teeth under light microscopy: A cross-sectional study. J. Oral. Maxillofac. Pathol. 2017, 21, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Vieira, A.; Hancock, R.; Dumitriu, M.; Schwartz, M.; Limeback, H.; Grynpas, M. How does fluoride affect dentin microhardness and mineralization? J. Dent. Res. 2005, 84, 951–957. [Google Scholar] [CrossRef]
- Rozier, R.G. Epidemiologic indices for measuring the clinical manifestations of dental fluorosis: Overview and critique. Adv. Dent. Res. 1994, 8, 39–55. [Google Scholar] [CrossRef]
- Chankanka, O.; Levy, S.M.; Warren, J.J.; Chalmers, J.M. A literature review of aesthetic perceptions of dental fluorosis and relationships with psychosocial aspects/oral health-related quality of life. Community Dent. Oral. Epidemiol. 2010, 38, 97–109. [Google Scholar] [CrossRef]
- Whelton, H.; Crowley, E.; O’Mullane, D.; Donaldson, M.; Kelleher, V.; Cronin, M. Dental caries and enamel fluorosis among the fluoridated and non-fluoridated populations in the Republic of Ireland in 2002. Community Dent. Health 2004, 21, 37–44. [Google Scholar]
- Dean, H.T.; McKay, F.S. Production of Mottled Enamel Halted by a Change in Common Water Supply. Am. J. Public Health Nations Health 1939, 29, 590–596. [Google Scholar] [CrossRef]
- Clark, D.C. Trends in prevalence of dental fluorosis in North America. Community Dent. Oral. Epidemiol. 1994, 22, 148–152. [Google Scholar] [CrossRef]
- McDonagh, M.S.; Whiting, P.F.; Wilson, P.M.; Sutton, A.J.; Chestnutt, I.; Cooper, J.; Misso, K.; Bradley, M.; Treasure, E.; Kleijnen, J. Systematic review of water fluoridation. BMJ 2000, 321, 855–859. [Google Scholar] [CrossRef] [Green Version]
- Curtis, A.M.; Levy, S.M.; Cavanaugh, J.E.; Warren, J.J.; Kolker, J.L.; Weber-Gasparoni, K. Decline in Dental Fluorosis Severity during Adolescence: A Cohort Study. J. Dent. Res. 2020, 99, 388–394. [Google Scholar] [CrossRef]
- Srivastava, S.; Flora, S.J.S. Fluoride in Drinking Water and Skeletal Fluorosis: A Review of the Global Impact. Curr. Environ. Health Rep. 2020, 7, 140–146. [Google Scholar] [CrossRef]
- Malago, J.; Makoba, E.; Muzaka, A.N.N. Fluoride levels in surface and groundwater in Africa: A review. Am. J. Water Sci. Eng. 2017, 3, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Keshavarz, S.; Ebrahimi, A.; Nikaeen, M. Fluoride exposure and its health risk assessment in drinking water and staple food in the population of Dayyer, Iran, in 2013. J. Educ. Health Promot. 2015, 4, 72. [Google Scholar]
- Demelash, H.; Beyene, A.; Abebe, Z.; Melese, A. Fluoride concentration in ground water and prevalence of dental fluorosis in Ethiopian Rift Valley: Systematic review and meta-analysis. BMC Public Health 2019, 19, 1298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hawley, G.M.; Ellwood, R.P.; Davies, R.M. Dental caries, fluorosis and the cosmetic implications of different TF scores in 14–year–old adolescents. Community Dent. Health 1996, 13, 189–192. [Google Scholar] [PubMed]
- Nair, R.; Chuang, J.C.; Lee, P.S.; Leo, S.J.; Yang, N.Q.; Yee, R.; Tong, H.J. Adult perceptions of dental fluorosis and select dental conditions-an Asian perspective. Community Dent. Oral Epidemiol. 2016, 44, 135–144. [Google Scholar] [CrossRef]
- Lalumandier, J.A.; Rozier, R.G. Parents’ satisfaction with children’s tooth color: Fluorosis as a contributing factor. J. Am. Dent. Assoc. 1998, 129, 1000–1006. [Google Scholar] [CrossRef]
- Bouschor, C.F. Bleaching fluorosis stained teeth. N. M. Dent. J. 1965, 16, 33–34. [Google Scholar]
- Pontes, D.G.; Correa, K.M.; Cohen-Carneiro, F. Re-establishing esthetics of fluorosis-stained teeth using enamel microabrasion and dental bleaching techniques. Eur. J. Esthet. Dent. 2012, 7, 130–137. [Google Scholar] [PubMed]
- Di Giovanni, T.; Eliades, T.; Papageorgiou, S.N. Interventions for dental fluorosis: A systematic review. J. Esthet. Restor. Dent. 2018, 30, 502–508. [Google Scholar] [CrossRef] [Green Version]
- Akpata, E.S. Occurrence and management of dental fluorosis. Int. Dent. J. 2001, 51, 325–333. [Google Scholar] [CrossRef]
- Weerasinghe, D.S.; Nikaido, T.; Wettasinghe, K.A.; Abayakoon, J.B.; Tagami, J. Micro-shear bond strength and morphological analysis of a self-etching primer adhesive system to fluorosed enamel. J. Dent. 2005, 33, 419–426. [Google Scholar] [CrossRef]
- Ermis, R.B.; De Munck, J.; Cardoso, M.V.; Coutinho, E.; Van Landuyt, K.L.; Poitevin, A.; Lambrechts, P.; Van Meerbeek, B. Bonding to ground versus unground enamel in fluorosed teeth. Dent. Mater. 2007, 23, 1250–1255. [Google Scholar] [CrossRef] [PubMed]
- Ermis, R.B.; Gokay, N. Effect of fluorosis on dentine shear bond strength of a self-etching bonding system. J. Oral Rehabil. 2003, 30, 1090–1094. [Google Scholar] [CrossRef]
- Farid, H.; Khan, F.R. Clinical management of severe fluorosis in an adult. BMJ Case Rep. 2012, 2012, bcr2012007138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morimoto, S.; Rebello de Sampaio, F.B.; Braga, M.M.; Sesma, N.; Ozcan, M. Survival Rate of Resin and Ceramic Inlays, Onlays, and Overlays: A Systematic Review and Meta-Analysis. J. Dent. Res. 2016, 95, 985–994. [Google Scholar] [CrossRef] [PubMed]
- Sailer, I.; Makarov, N.A.; Thoma, D.S.; Zwahlen, M.; Pjetursson, B.E. All-ceramic or metal-ceramic tooth-supported fixed dental prostheses (FDPs)? A systematic review of the survival and complication rates. Part I: Single crowns (SCs). Dent. Mater. 2015, 31, 603–623. [Google Scholar] [CrossRef] [Green Version]
- Luciano, M.; Francesca, Z.; Michela, S.; Tommaso, M.; Massimo, A. Lithium disilicate posterior overlays: Clinical and biomechanical features. Clin. Oral Investig. 2020, 24, 841–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malament, K.A.; Natto, Z.S.; Thompson, V.; Rekow, D.; Eckert, S.; Weber, H.P. Ten-year survival of pressed, acid-etched e.max lithium disilicate monolithic and bilayered complete-coverage restorations: Performance and outcomes as a function of tooth position and age. J. Prosthet. Dentistry 2019, 121, 782–790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pieger, S.; Salman, A.; Bidra, A.S. Clinical outcomes of lithium disilicate single crowns and partial fixed dental prostheses: A systematic review. J. Prosthet. Dent. 2014, 112, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Rojpaibool, T.; Leevailoj, C. Fracture Resistance of Lithium Disilicate Ceramics Bonded to Enamel or Dentin Using Different Resin Cement Types and Film Thicknesses. J. Prosthodont. 2017, 26, 141–149. [Google Scholar] [CrossRef]
- Sasse, M.; Krummel, A.; Klosa, K.; Kern, M. Influence of restoration thickness and dental bonding surface on the fracture resistance of full-coverage occlusal veneers made from lithium disilicate ceramic. Dent. Mater. 2015, 31, 907–915. [Google Scholar] [CrossRef] [PubMed]
- Baldissara, P.; Monaco, C.; Onofri, E.; Fonseca, R.G.; Ciocca, L. Fatigue resistance of monolithic lithium disilicate occlusal veneers: A pilot study. Odontology 2019, 107, 482–490. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TFI | Criteria |
|---|---|
| 0 | Normal translucency of enamel remains after prolonged air-drying. |
| 1 | Narrow white lines located corresponding to perikymata. |
| 2 | Smooth surface: Pronounced lines of opacity that follow perikymata. Occasional confluence of adjacent lines. Occlusal surface: scattered areas of opacity <2 mm in diameter and pronounced opacity of cuspal ridges. |
| 3 | Smooth surface: Merging and irregular cloudy areas of opacity. Accentuated drawing of perikymata often visible between opacities. Occlusal surface: Confluent areas of marked opacity. Worn areas appear almost normal but usually circumscribed by a rim of opaque enamel. |
| 4 | Smooth surface: Entire surface exhibits marked opacity or appears chalky white. Parts of surface exposed to attrition appear less affected. Occlusal surface: Entire surface exhibits marked opacity. Attrition is often pronounced shortly after eruption. |
| 5 | Entire surface displays marked opacity with focal loss of outermost enamel (pits) <2 mm in diameter. |
| 6 | Smooth surface: pits are regularly arranged in horizontal bands <2 mm in vertical extension. Occlusal surface: Confluent areas <3 mm in diameter exhibit loss of enamel. Marked attrition. |
| 7 | Smooth surface: loss of outermost enamel in irregular areas involving <1/2 of entire surface. Occlusal surface: changes in the morphology caused by merging pits and marked attrition. |
| 8 | Loss of outermost enamel involving >1/2 of surface. |
| 9 | Loss of main part of enamel with change in anatomic appearance of surface. Cervical rim of almost unafffected enamel is often noted. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.D.; Inoue, N.; Lee, C.; Park, S.; Lee, S.J. Comprehensive Management of Severe Dental Fluorosis with Adhesively Bonded All-Ceramic Restorations. Prosthesis 2021, 3, 194-208. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis3030020
Lee JD, Inoue N, Lee C, Park S, Lee SJ. Comprehensive Management of Severe Dental Fluorosis with Adhesively Bonded All-Ceramic Restorations. Prosthesis. 2021; 3(3):194-208. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis3030020
Chicago/Turabian StyleLee, Jason D., Natalie Inoue, Christine Lee, Sohyun Park, and Sang J. Lee. 2021. "Comprehensive Management of Severe Dental Fluorosis with Adhesively Bonded All-Ceramic Restorations" Prosthesis 3, no. 3: 194-208. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis3030020