Multimodal Frequency Treatment for Facial Pain Caused by Chronic Rhinosinusitis: A Pilot Study

Abstract
:1. Introduction
2. Materials and Methods
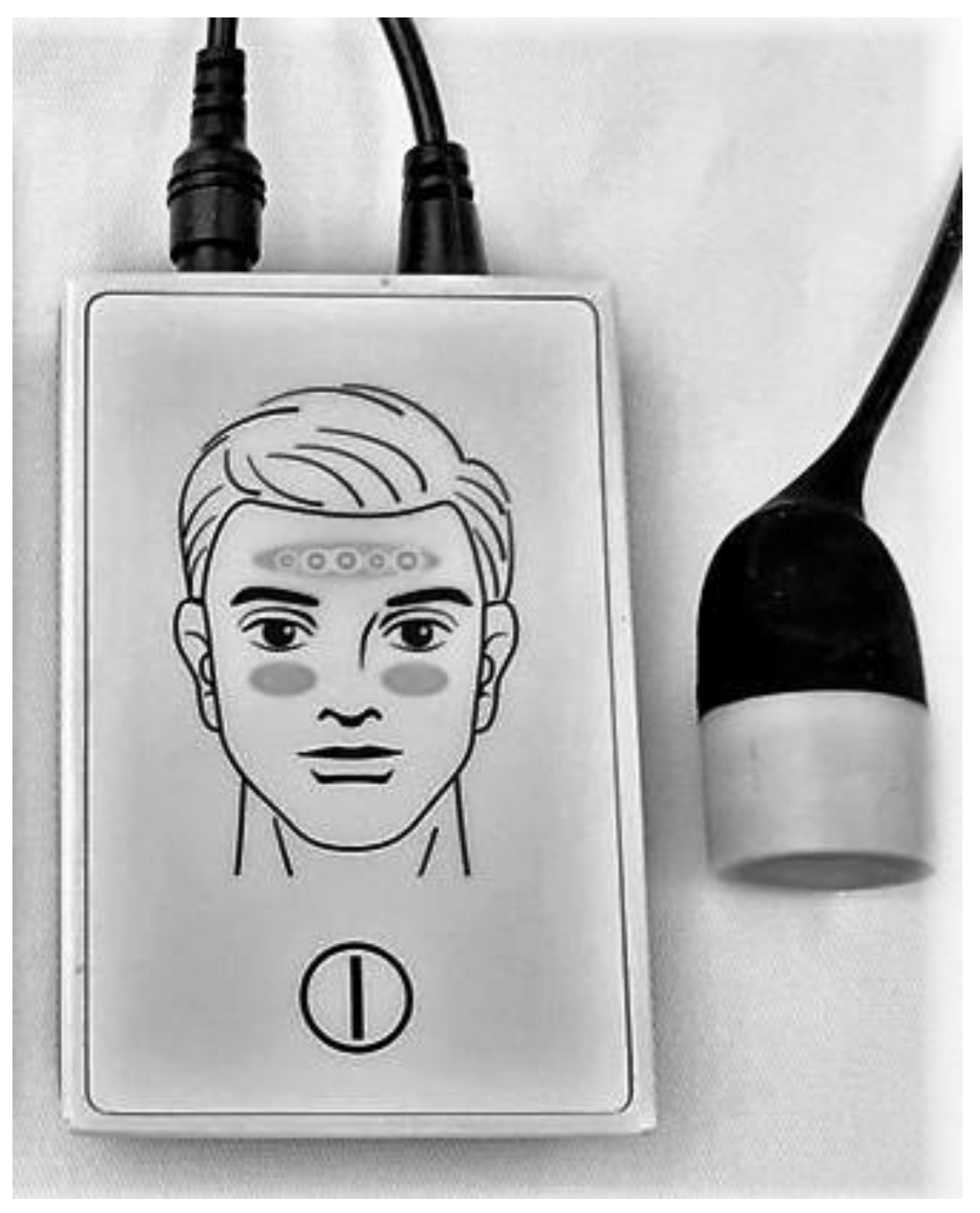
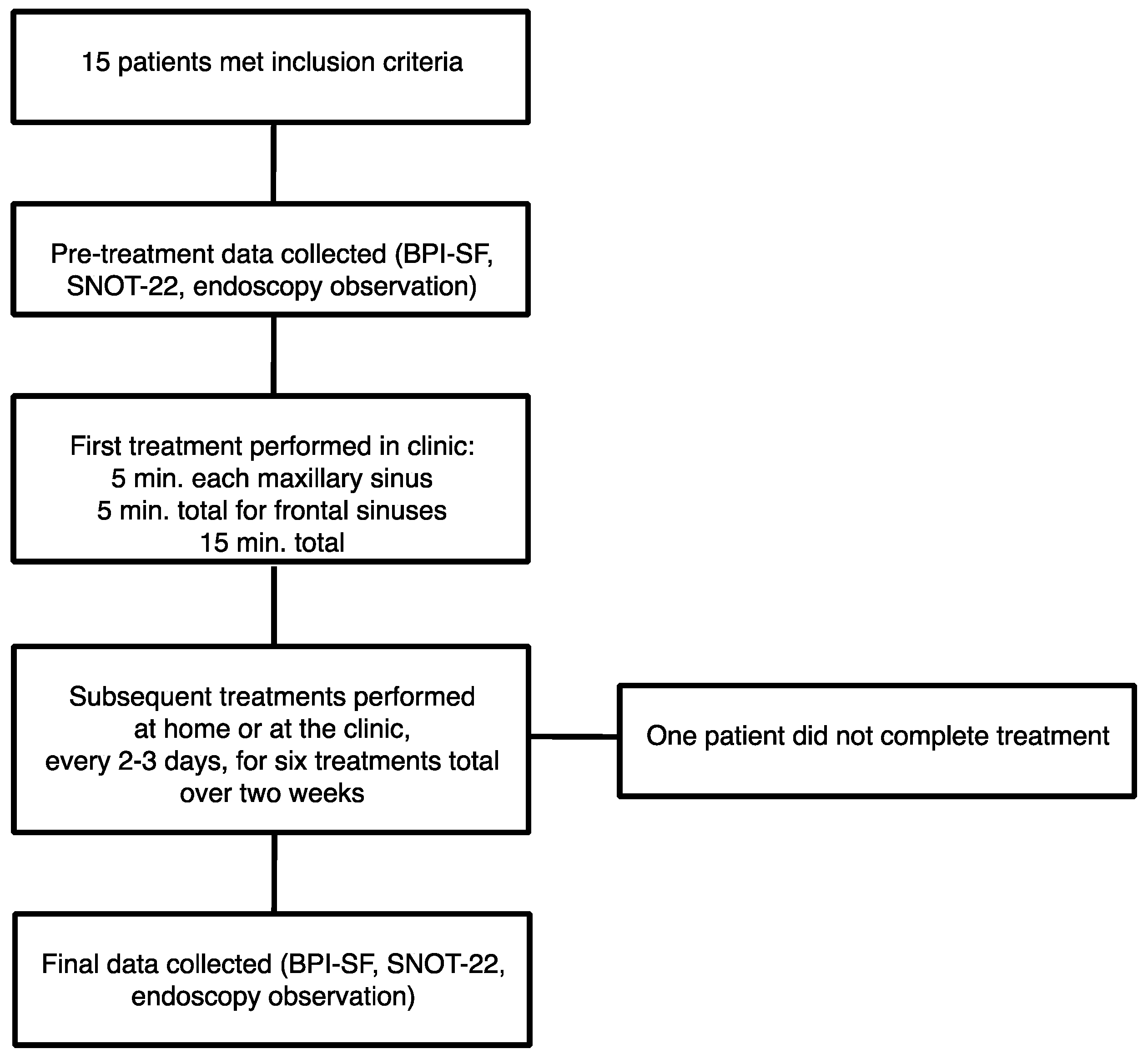
2.1. Prospective Clinical Trial of Multimodal Frequencies for the Treatment of Chronic Rhinosinusitis Patients
2.2. Analysis of Previously-Published Data
2.3 Ethical Standards
3. Results
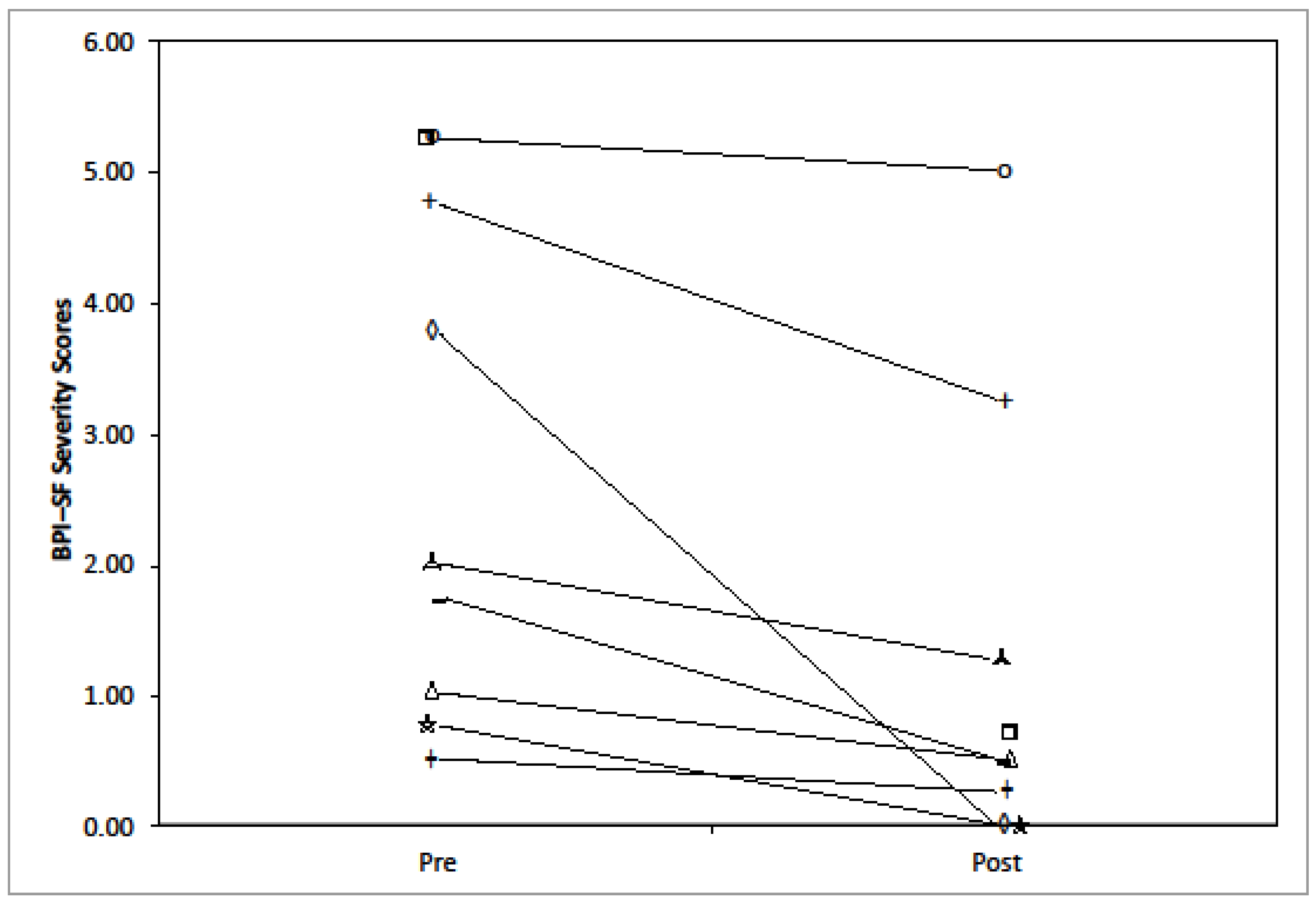
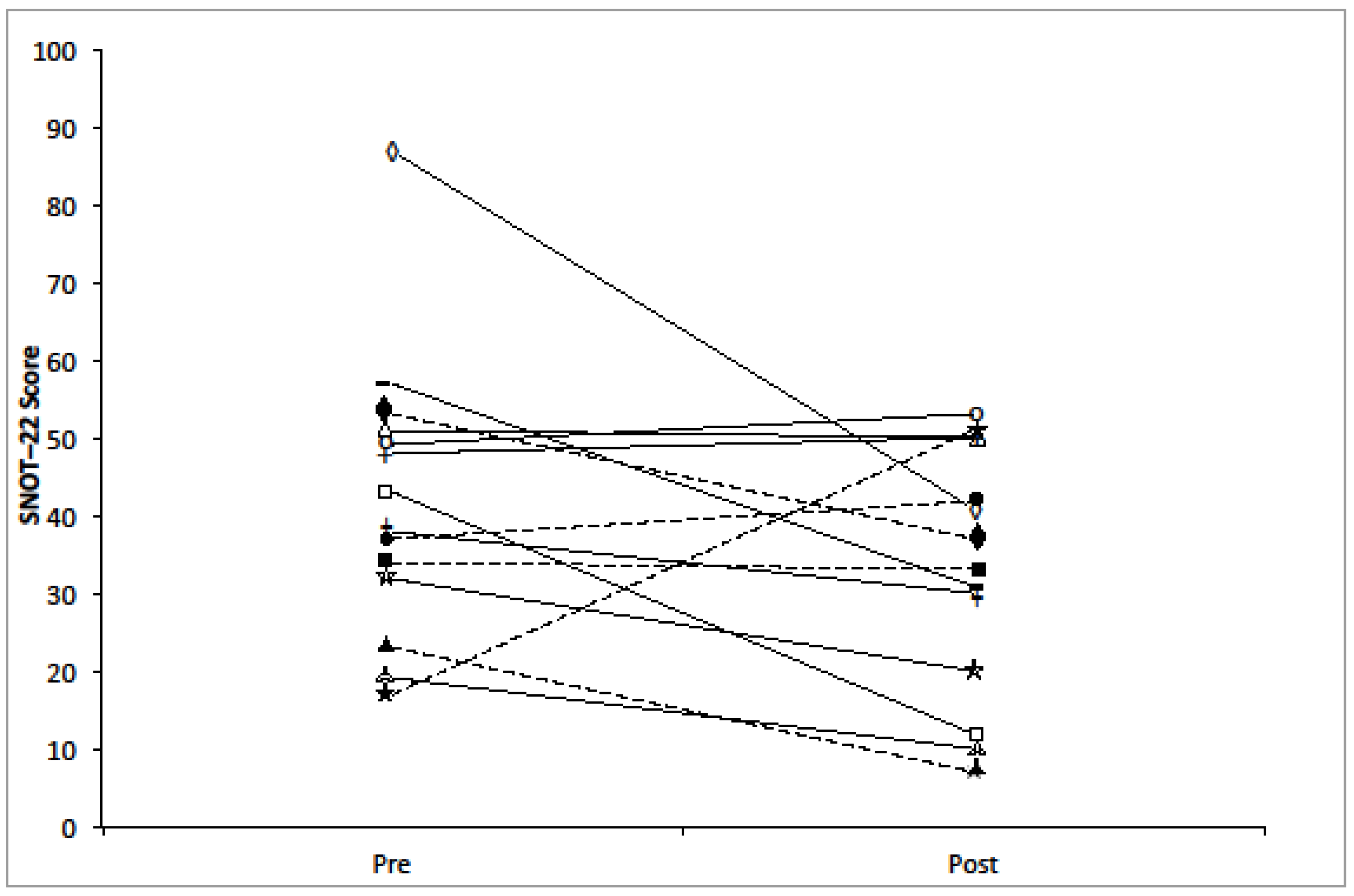
3.1. Clinical Trial Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Blackwell, D.L.; Lucas, J.W. Tables of summary health statistics for U.S. Adults: 2014 national health interview survey. 2015. Available online: http://www.cdc.gov/nchs/nhis/SHS/tables.htm (accessed on 13 July 2017).
- Fokkens, W.J.; Lund, V.J.; Mullol, J.; Bachert, C.; Alobid, I.; Baroody, F.; Cohen, N.; Cervin, A.; Douglas, R.; Gevaert, P.; et al. European position paper on rhinosinusitis and nasal polyps 2012. Rhinology 2012, 50, 1–298. [Google Scholar] [PubMed]
- Cox, D.R.; Asbhy, S.; Mace, J.C.; DelGaudio, J.M.; Smith, T.L.; Orlandi, R.R.; Alt, J.A. The pain-depression dyad and the association with sleep dysfunction in chronic rhinosinusitis. Int. Forum Allergy Rhinol. 2017, 7, 56–63. [Google Scholar] [CrossRef] [PubMed]
- DeConde, A.M.; Made, J.C.; Ashby, S.; Smith, T.L.; Orlandi, R.R.; Alt, J.A. Characterization of facial pain associated wtih chronic rhinosinusitis using validated pain evaluation instruments. Int. Forum Allergy Rhinol. 2015, 5, 682–689. [Google Scholar] [CrossRef] [PubMed]
- Bartley, J.; Ansari, N.N.; Naghdi, S. Therapeutic ultrasound as a treatment modality for chronic rhinosinusitis. Curr. Infect. Dis. Rep. 2014, 16, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, E.O.; Hamilos, D.L. Rhinosinusitis diagnosis and management for the clinician: A synopsis of recent consensus guidelines. Mayo Clin. Proc. 2011, 86, 427–443. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, R.; Piccirillo, J.; Chandrasekhar, S.; Brook, I.; Kumar, K.; Kramper, M.; Orlandi, R.; Palmer, J.; Patel, Z.; Peters, A.; et al. Clinical practice guideline (update): Adult sinusitis. Otolaryngol. Head Neck Surg. 2015, 152, S1–S39. [Google Scholar] [CrossRef] [PubMed]
- Lanza, D.C.; Kennedy, D.W. Adult rhinosinusitis defined. Otolaryngol. Head Neck Surg. 1997, 117, S1–S7. [Google Scholar] [CrossRef]
- Ramakrishnan, V.R.; Hauser, L.J.; Feazel, L.M.; Ir, D.; Robertson, C.E.; Frank, D.N. Sinus microbiota varies among chronic rhinosinusitis phenotypes and predicts surgical outcome. J. Allergy Clin. Immunol. 2015, 136, 334–342. [Google Scholar] [CrossRef] [PubMed]
- Schäcke, H.; Döcke, W.; Asdullah, K. Mechanisms involved in the side effects of glucocorticoids. Pharmacol. Ther. 2002, 96, 23–43. [Google Scholar] [CrossRef]
- Patel, Z.M.; Thamboo, A.; Rudmik, L.; Nayak, J.V.; Smith, T.L.; Hwang, P.H. Surgical therapy vs continued medical therapy for medically refractory chronic rhinosinusitis: A systematic review and meta-analysis. Int. Forum Allergy Rhinol. 2017, 7, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Hinz, B.; Cheremina, O.; Brune, K. Acetaminophen (paracetamol) is a selective cyclooxygenase-2 inhibitor in man. FASEB J. 2008, 22, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Lund, V.J.; MacKay, I.S. Outcome assessment of endoscopic sinus surgery. J. R. Soc. Med. 1994, 87, 70–72. [Google Scholar] [PubMed]
- Ragab, S.M.; Lund, V.J.; Scadding, G. Evaluation of the medical and surgical treatment of chronic rhinosinusitis: A prospective, randomised, controlled trial. Laryngoscope 2004, 114, 923–930. [Google Scholar] [CrossRef] [PubMed]
- Friedman, M.; Schalch, P.; Lin, H.; Mazloom, N.; Neidich, M.; Joseph, N.J. Functional endoscopic dilatation of the sinuses: Patient satisfaction, postoperative pain, and cost. Am. J. Rhinol. 2008, 22, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, J.L. Sino-nasal outcome test (SNOT-22): A predictor of postsurgical improvement in patients with chronic sinusitis. Ann. Allergy Asthma Immunol. 2013, 111, 246–251.e2. [Google Scholar] [CrossRef] [PubMed]
- Chaaban, M.R.; Kejner, A.; Rowe, S.M.; Woodworth, B.A. Cystic fibrosis chronic rhinosinusitis: A comprehensive review. Am. J. Rhinol. Allergy 2013, 27, 387–395. [Google Scholar] [CrossRef] [PubMed]
- Younis, R.T.; Ahmed, J. Predicting revision sinus surgery in allergic fungal and eosinophilic mucin chronic rhinosinusitis. Laryngoscope 2017, 127, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Benninger, M.S.; Ferguson, B.J.; Hadley, J.A.; Hamilos, D.L.; Jacobs, M.; Kennedy, D.W.; Lanza, D.C.; Marple, B.F.; Osguthorpe, J.D.; Stankiewicz, J.A.; et al. Adult chronic rhinosinusitis: Definitions, diagnosis, epidemiology, and pathophysiology. Otolaryngol. Head Neck Surg. 2003, 129, S1–S32. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, N.; Orlandi, R.R.; Grebner, J.; Martinson, M. Cost burden of chronic rhinosinusitis: A claims-based study. Otolaryngol. Head Neck Surg. 2011, 144, 440–445. [Google Scholar] [CrossRef] [PubMed]
- Jones, N.S.; Cooney, T.R. Facial pain and sinonasal surgery. Rhinology 2003, 41, 193–200. [Google Scholar] [PubMed]
- Ryan, W.R.; Ramachandra, T.; Hwang, P.H. Correlations between symptoms, nasal endoscopy, and in-office computed tomography in post-surgical chronic rhinosinusitis patients. Laryngoscope 2011, 121, 674–678. [Google Scholar] [CrossRef] [PubMed]
- Shields, G.; Seikaly, H.; LeBoeuf, M.; Guinto, F.; LeBoeuf, H.; Pincus, T.; Calhoun, K. Correlation between facial pain or headache and computed tomography in rhinosinusitis in Canadian and U.S. subjects. Laryngoscope 2003, 113, 943–945. [Google Scholar] [CrossRef] [PubMed]
- Clerico, D.M. An experimental study of pain upon stimulation of the nasal and sinus cavities. Am. J. Otolaryngol. 2014, 35, 300–304. [Google Scholar] [CrossRef] [PubMed]
- Mehle, M.E.; Schreiber, C.P. Sinus headache, migraine, and the otolaryngologist. Otolaryngol. Head Neck Surg. 2005, 133, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Jones, N.S. Sinus headaches: Avoiding over- and mis-diagnosis. Expert Rev. Neurother. 2009, 9, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Mehle, M.E.; Schreiber, C.P. What do we know about rhinogenic headache? Otolaryngol. Clin. North Am. 2014, 47, 255–268. [Google Scholar] [CrossRef] [PubMed]
- Aaseth, K.; Grande, R.B.; Kværner, K.; Lundqvist, C.; Russell, M.B. Chronic rhinosinusitis gives a ninefold increased risk of chronic headache. Cephalalgia 2010, 30, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Lundeberg, T. The pain suppressive effect of vibratory stimulation and transcutaneous electrical nerve stimulation (TENS) as compared to aspirin. Brain Res. 1984, 294, 201–209. [Google Scholar] [CrossRef]
- Kitay, G.S.; Koren, M.J.; Helfet, D.L.; Parides, M.K.; Markenson, J.A. Efficacy of combined local mechanical vibrations, continuous passive motion and thermotherapy in the management of osteoarthritis of the knee. Osteoarthr. Cartil. 2009, 17, 1269–1274. [Google Scholar] [CrossRef] [PubMed]
- Gay, A.; Aimonetti, J.; Roll, J.; Ribot-Ciscar, E. Kinesthetic illusions attenuate experimental muscle pain, as do muscle and cutaneous stimulation. Brain Res. 2015, 1615, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Trulsson, M.; Essick, G.K. Sensations evoked by microstimulation of single mechanoreceptive afferents innervating the human face and mouth. J. Neurophysiol. 2010, 103, 1741–1747. [Google Scholar] [CrossRef] [PubMed]
- Johansson, R.S.; Trulsson, M.; Olsson, K.Å.; Westbert, K.G. Mechanoreceptor activity from the human face and oral mucosa. Exp. Brain Res. 1988, 72, 204–208. [Google Scholar] [CrossRef] [PubMed]
- Sessle, B.J. Acute and chronic craniofacial pain: Brainstem mechanisms of nociceptive transmission and neuroplasticity, and their clinical correlates. Crit. Rev. Oral Biol. Med. 2000, 11, 57–91. [Google Scholar] [CrossRef] [PubMed]
- Woolf, C.J. Central sensitization: Implications for the diagnosis and treatment of pain. Pain 2011, 152, S2–S15. [Google Scholar] [CrossRef] [PubMed]
- Miller, S.; Sinclair, A.J.; Davies, B.; Matharu, M. Neurostimulation in the treatment of primary headaches. Pract. Neurol. 2015, 16, 362–375. [Google Scholar] [CrossRef] [PubMed]
- Nanitsos, E.; Vartuli, R.; Forte, A.; Dennison, P.J.; Peck, C.C. The effect of vibration on pain during local anaesthesia injections. Aust. Dent. J. 2009, 52, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Ansari, N.N.; Soofia, N.; Farhadi, M.; Jalaie, S. A preliminary study into the effect of low-intensity pulsed ultrasound on chronic maxillary and frontal sinusitis. Physiother. Theory Pract. 2007, 23, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Naghdi, S.; Ansari, N.N.; Farhadi, M. A clinical trial on the treatment of chronic rhinosinusitis with continuous ultrasound. J. Phys. Ther. Sci. 2008, 20, 233–238. [Google Scholar] [CrossRef]
- Young, D.; Morton, R.; Bartley, J. Therapeutic ultrasound as treatment for chronic rhinosinusitis: Preliminary observations. J. Laryngol. Otol. 2010, 124, 495–499. [Google Scholar] [CrossRef] [PubMed]
- Baker, K.G.; Robertson, V.J.; Duck, F.A. A review of therapeutic ultrasound: Biophysical effects. Phys. Ther. 2001, 81, 1351–1358. [Google Scholar] [CrossRef] [PubMed]
- Tyrell, D.; Barrow, I.; Arthur, J. Local hyperthermia benefits natural and experimental common colds. Br. Med. J. 1989, 298, 1280–1283. [Google Scholar] [CrossRef]
- Bartley, J.; Young, D. Ultrasound as a treatment for chronic rhinosinusitis. Med. Hypotheses 2009, 73, 15–17. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.-I.; Barua, S.; Choi, B.H.; Min, B.-H.; Han, H.C.; Baik, E.J. Anti-inflammatory effect of low intensity ultrasound (LIUS) on complete Freund’s adjuvant-induced arthritis synovium. Osteoarthr. Cartil. 2012, 20, 314–322. [Google Scholar] [CrossRef] [PubMed]
- Tan, N.C.; Foreman, A.; Jardeleza, C.; Douglas, R.; Tran, H.; Wormald, P.J. The multiplicity of Staphylococcus aureus in chronic rhinosinusitis: Correlating surface biofilm and intracellular residence. Laryngoscope 2012, 122, 1655–1660. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, R.H.; Turk, D.C.; Wyrwich, K.W.; Beaton, D.; Cleeland, C.S.; Farrar, J.T.; Haythornthwaite, J.A.; Jensen, M.P.; Kerns, R.D.; Ader, D.N.; et al. Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. J. Pain 2007, 9, 105–121. [Google Scholar] [CrossRef] [PubMed]
- Tarasidis, G.S.; DeConde, A.M.; Mace, J.C.; Ashby, S.; Smith, T.L.; Orlandi, R.R.; Alt, J.A. Cognitive dysfunction associated to pain and quality of life in chronic rhinosinusitis. Int. Forum Allergy Rhinol. 2015, 5, 1004–1009. [Google Scholar] [CrossRef] [PubMed]
- Schedlowski, M.; Enck, P.; Rief, W.; Bingel, U. Neuro-bio-behavioral mechanisms of placebo and nocebo responses: Implications for clinical trials and clinical practice. Pharmacol. Rev. 2015, 67, 697–730. [Google Scholar] [CrossRef] [PubMed]
- DeConde, A.S.; Mace, J.C.; Bodner, T.; Hwang, P.H.; Rudmik, L.; Soler, Z.M.; Smith, T.L. SNOT-22 quality of life domains differentially predict treatment modality selection in chronic rhinosinusitis. Int. Forum Allergy Rhinol. 2014, 4, 972–979. [Google Scholar] [CrossRef] [PubMed]
- Sanderson, M.J.; Dirksen, E.R. Mechanosensitivity of cultured ciliated cells from the mammalian respiratory tract: Implications for the regulation of mucociliary transport. Proc. Natl. Acad. Sci. USA 1986, 83, 7302–7306. [Google Scholar] [CrossRef] [PubMed]
- Cleeland, C.S. Brief pain inventory user’s guide. 2009. Available online: https://www.mdanderson.org/documents/Departments-and-Divisions/Symptom-Research/BPI_UserGuide.pdf (accessed on 27 June 2017).
- Ansari, N.N.; Fathali, M.; Naghdi, S.; Hasson, S.; Jalaie, S.; Rastak, M.S. A randomized, double-blind clinical trial comparing the effects of continuous and pulsed ultrasound in patients with chronic rhinosinusitis. Physiother. Theory Pract. 2012, 28, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Ansari, N.N.; Naghdi, S.; Farhadi, M. Physiotherapy for chronic rhinosinusitis: The use of continuous ultrasound. Int. J. Ther. Rehabil. 2007, 14, 306–310. [Google Scholar] [CrossRef]
- Ansari, N.N.; Naghdi, S.; Fathali, M.; Bartley, J.; Rastak, M.S. A randomized clinical trial comparing pulsed ultrasound and erythromycin phonophoresis in the treatment of patients with chronic rhinosinusitis. Physiother. Theory Pract. 2015, 32, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Høsøien, E.; Lund, A.B.; Vasseljen, O. Similar effect of therapeutic ultrasound and antibiotics for acute bacterial rhinosinusitis: a randomized trial. J. Physiother. 2010, 56, 27–32. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Earlbaum Associates: Hillsdale, NH, USA, 1988. [Google Scholar]
- Guieu, R.; Tardy-Gervet, M.; Roll, J. Analgesic effects of vibration and transcutaneous electrical nerve stimulation applied separately and simultaneously to patients with chronic pain. Can. J. Neurol. Sci. 1991, 18, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Ïnal, S.; Kelleci, M. Relief of pain during blood specimen collection in pediatric patients. MCN 2012, 37, 339–345. [Google Scholar] [CrossRef]
- Moadad, N.; Kozman, K.; Shahine, R.; Ohanian, S.; Badr, L.K. Distraction using the BUZZY for children during an IV insertion. J. Pediatr. Nurs. 2016, 31, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Taddio, A.; Shah, V.; McMurtry, C.M.; MacDonald, N.E.; Ipp, M.; Riddell, R.P.; Noel, M.; Chambers, C.T. Procedural and physical interventions for vaccine injections. Clin. J. Pain 2015, 31, S20–S37. [Google Scholar] [CrossRef] [PubMed]
- Hara, E.S.; Witzel, A.L.; De Luca, C.E.P.; Ballester, R.Y.; Kuboki, T.; Bolzan, M.C. A novel vibratory stimulation-based occlusal splint for alleviation of TMD painful symptoms: a pilot study. J. Oral Rehabil. 2013, 40, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Roy, E.A.; Hollins, M.; Maixner, W. Reduction of TMD pain by high-frequency vibration: A spatial and temporal analysis. Pain 2003, 101, 267–274. [Google Scholar] [CrossRef]
- Rocha, W.A.; Rodrigues, K.M.; Pereira, R.R.; Nogueira, B.V.; Gonçalves, W.L. Acute effects of therapeutic 1-MHz ultrasound on nasal unblocking of subjects with chronic rhinosinusitis. Braz. J. Otorhinolaryngol. 2011, 77, 7–12. [Google Scholar] [CrossRef] [PubMed]
- West, S.J.; Bannister, K.; Dickenson, A.H.; Bennett, D.L. Circuitry and plasticity of the dorsal horn—Toward a better understanding of neuropathic pain. Neuroscience 2015, 300, 254–275. [Google Scholar] [CrossRef] [PubMed]
- Craig, T.J.; Ferguson, B.J.; Krouse, J.H. Sleep impairment in allergic rhinitis, rhinosinusitis, and nasal polyposis. Am. J. Otolaryngol. 2008, 29, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, C.; Gillett, S.; Slack, R.; Lund, V.J.; Browne, J.P. Psychometric validity of the 22-item Sinonasal Outcome Test. Clin. Otolaryngol. 2009, 34, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Duan, B.; Cheng, L.; Bourane, S.; Britz, O.; Padilla, C.; Garcia-Campmany, L.; Krashes, M.; Knowlton, W.; Velasquez, T.; Ren, X.; et al. Identification of spinal circuits transmitting and gating mechanical pain. Cell 2014, 159, 1417–1432. [Google Scholar] [CrossRef] [PubMed]
- Melzack, R.; Wall, P.D. Pain mechanisms: A new theory. Science 1965, 150, 971–979. [Google Scholar] [CrossRef] [PubMed]
- Vierck, C.J.; Whitsel, B.L.; Favorov, O.V.; Brown, A.W.; Tommerdahl, M. Role of primary somatosensory cortex in the coding of pain. Pain 2013, 154, 334–344. [Google Scholar] [CrossRef] [PubMed]
- Hollins, M.; McDermott, K.; Harper, D. How does vibration reduce pain? Perception 2014, 43, 70–84. [Google Scholar] [CrossRef] [PubMed]
- Day, M. Sympathetic blocks: The evidence. Pain Practice 2008, 8, 98–109. [Google Scholar] [CrossRef] [PubMed]
- Felisati, G.; Arnone, F.; Lozza, P.; Leone, M.; Curone, M.; Bussone, G. Sphenopalatine endoscopic ganglion block: A revision of a traditional technique for cluster headache. Laryngoscope 2006, 16, 1447–1450. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Schoenen, J.; Ashina, M. Sphenopalatine ganglion neuromodulation in migraine: What is the rationale? Cephalalgia 2014, 34, 382–391. [Google Scholar] [CrossRef] [PubMed]
- Robbins, M.S.; Robertson, C.E.; Kaplan, E.; Ailani, J.; Charleston, L.; Kuruvilla, D.; Blumenfeld, A.; Berliner, R.; Rosen, N.L.; Duarte, R.; et al. The sphenopalatine ganglion: Anatomy, pathophysiology, and therapeutic targeting in headache. Headache 2015, 56, 240–258. [Google Scholar] [CrossRef] [PubMed]
- Talman, W.T.; Corr, J.; Dragon, D.N.; Wang, D. Parasympathetic stimulation elicits cerebral vasodilatation in rat. Auton. Neurosci. 2007, 133, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Uddman, R.; Malm, L.; Fahrenkrug, J.; Sundler, F. Vip increases in nasal blood during stimulation of the Vidian nerve. Acta Otolaryngol. 1981, 91, 135–138. [Google Scholar] [CrossRef]
- Ansarinia, M.; Rezai, A.; Tepper, S.J.; Steiner, C.P.; Stump, J.; Stanton-Hicks, M.; Machado, A.; Narouze, S. Electrical stimulation of sphenopalatine ganglion for acute treatment of cluster headaches. Headache 2010, 50, 1164–1174. [Google Scholar] [CrossRef] [PubMed]
- Bjordal, J.M.; Johnson, M.I.; Lopes-Martins, R.A.; Bogen, B.; Chow, R.; Ljunggren, A.E. Short-term efficacy of physical interventions in osteoarthritic knee pain. A systematic review and meta-analysis of randomised placebo-controlled trials. BMC Musculoskelet. Disord. 2006, 8, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, M.; Martinson, M. Efficacy of electrical nerve stimulation for chronic musculoskeletal pain: A meta-analysis of randomized controlled trials. Pain 2007, 130, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Lobre, W.D.; Callegari, B.J.; Gardner, G.; Marsh, C.M.; Bush, A.C.; Dunn, W.J. Pain control in orthodontics using a micropulse vibration device: A randomized clinical trial. Angle Orthod. 2015, 86, 625–630. [Google Scholar] [CrossRef] [PubMed]
- Mücke, M.; Cuhls, H.; Radbruch, L.; Weigl, T.; Rolke, R. Evidence of heterosynaptic LTD in the human nociceptive system: Superficial skin neuromodulation using a matrix electrode reduces deep pain sensitivity. PLoS ONE 2014, 9, e107718. [Google Scholar] [CrossRef] [PubMed]
- Peirs, C.; Seal, R.P. Neural circuits for pain: Recent advances and current views. Science 2017, 354, 578–584. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.; Sarah Bush Lincoln Health Center, Matoon, IL, USA. Personal Communication, 2016.
- Van Cauwenberge, P.; Watelet, J.B. Epidemiology of chronic rhinosinusitis. Thorax 2000, 55, S20–S21. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Information | Value (SD*) |
|---|---|
| Patients enrolled | 15 |
| Patients completed study | 14 |
| Age (mean) | 60 (12.64) |
| Male | 6 |
| Female | 9 |
| Diabetic (controlled) | 3 |
| Past sinus surgery | 2 |
| Hypertension | 6 |
| Patients reporting facial pain at the beginning of the study | 9 |
| Item | Baseline | Post-Treatment | Change (SD) | Effect Size (Cohen’s d) |
|---|---|---|---|---|
| Facial Pain (from SNOT-20) | 2.20 (1.73) | 1.45 (1.46) | 0.75 (1.48) | 0.51 * |
| Facial Pain Analog Scale | 4 (2.12) | 3 (1.67) | 1 (1.65) | 0.76 |
| SNOT-20 total score | 43.15 (24.75) | 27.40 (21.18) | 15.75 (17.41) | 0.90 *** |
| Domain | Baseline | Post-Treatment | Change (SD) | Effect Size |
|---|---|---|---|---|
| BPI-SF Severity (Facial Pain) | 2.78 (1.97) | 1.28 (1.72) | 1.50 (1.56) | 0.96 ** |
| BPI-SF Interference | 2.65 (2.44) | 1.25 (1.86) | 1.40 (2.26) | 0.62 |
| SNOT-22 total score | 47.11 (18.80) | 33.00 (16.56) | 14.11 (16.85) | 0.84 * |
| Domain | Baseline (SD) | Post-Treatment (SD) | Change (SD) | Effect Size |
|---|---|---|---|---|
| BPI-SF Severity (Facial Pain) | 1.82 (2.00) | 1.02 (1.62) | 0.80 (1.52) | 0.67 ** |
| BPI-SF Interference | 1.91 (2.11) | 0.83 (1.51) | 1.09 (1.78) | 0.60 * |
| SNOT-22 total score | 41.47 (17.56) | 34.27 (15.73) | 7.20 (19.18) | 0.45 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smith, M.; Berenger, P.G.; Bonutti, P.; Ramakrishnan, A.P.; Beyers, J.; Ramakrishnan, V. Multimodal Frequency Treatment for Facial Pain Caused by Chronic Rhinosinusitis: A Pilot Study. Sinusitis 2017, 2, 5. https://0-doi-org.brum.beds.ac.uk/10.3390/sinusitis2030005
Smith M, Berenger PG, Bonutti P, Ramakrishnan AP, Beyers J, Ramakrishnan V. Multimodal Frequency Treatment for Facial Pain Caused by Chronic Rhinosinusitis: A Pilot Study. Sinusitis. 2017; 2(3):5. https://0-doi-org.brum.beds.ac.uk/10.3390/sinusitis2030005
Chicago/Turabian StyleSmith, Michael, Philippe G. Berenger, Peter Bonutti, Alisa P. Ramakrishnan, Justin Beyers, and Vivek Ramakrishnan. 2017. "Multimodal Frequency Treatment for Facial Pain Caused by Chronic Rhinosinusitis: A Pilot Study" Sinusitis 2, no. 3: 5. https://0-doi-org.brum.beds.ac.uk/10.3390/sinusitis2030005