Low-Grade B Cell Lymphoproliferative Disorder Masquerading as Chronic Rhinosinusitis

Scottish Centre for Respiratory Research and Rhinology Mega-Clinic, School of Medicine, University of Dundee, Ninewells Hospital, Dundee DD1 9SY, UK
*
Author to whom correspondence should be addressed.
Sinusitis 2021, 5(1), 1-4; https://0-doi-org.brum.beds.ac.uk/10.3390/sinusitis5010001
Submission received: 16 November 2020
/
Revised: 21 December 2020
/
Accepted: 30 December 2020
/
Published: 11 January 2021
(This article belongs to the Special Issue Allergic Rhinosinusitis and Airway Diseases)
Abstract
:Chronic rhinosinusitis (CRS) is one of the most common persistent disorders of the developed world, requiring input from various specialists including primary care physicians, otolaryngologists, respiratory physicians, and allergologists. B-cell lymphoproliferative disorders (BLPDs) are a heterogenous group of malignant conditions defined by an accumulation of mature B lymphocytes in the bone marrow, blood, and lymphoid tissues. We present a case report of an elderly man with rhinosinusitis-like symptoms and atypical features prompting further investigations that culminated in a diagnosis of BLPD.
1. Introduction
Chronic rhinosinusitis (CRS) is one of the most common persistent disorders of the developed world, requiring input from various specialists including primary care physicians, otolaryngologists, respiratory physicians, and allergologists [1]. Current international guidelines recommend that diagnosis is made by clinicians on the basis of symptoms such as nasal blockage, discharge, facial pressure, and loss of smell for at least 12 weeks [2]. However, the diagnostic work up can be fraught with difficulty, especially when attempting to differentiate between CRS and allergic and nonallergic rhinitis on symptoms alone. Additionally, not all patients with CRS criteria will have evidence of disease on nasal endoscopy and CT imaging [2].
Based on high quality evidence, medical therapy with long term nasal corticosteroids, short courses of oral corticosteroids, and/or nasal irrigation with isotonic saline or Ringer’s lactate are effective in treating CRS [2]. Dupilumab (anti-IL4rα) is the only monoclonal antibody approved for the treatment of CRS with nasal polyps (CRSwNP) at present. Two studies have demonstrated efficacy of intravenous mepolizumab (anti-IL5) 750 mg q4w on reducing the need for nasal polyp surgery and total polyp score [3,4] but at the current subcutaneous licensed dose of 100 mg q4w, our experience has shown a clear disconnect in response between severe eosinophilic asthma and CRSwNP [5]. Surgical management is usually indicated when CRSwNP is refractory to medical therapy [2].
B-cell lymphoproliferative disorders (BLPDs) are a heterogenous group of malignant haematological conditions with a significantly higher incidence in individuals with primary or secondary immunodeficiency [6]. Diagnosis is usually made on the basis of clinical features such as enlarged lymph nodes or splenomegaly and excess fatigue and/or apparent cytopenia and lymphocytosis on a full blood count [7]. Morphological examination demonstrating a lymphocytic increase or abnormality would prompt further immunophenotypic investigations. Multiparameter flow cytometry on peripheral blood or bone marrow is a rapid and efficient tool for the diagnosis of BLPDs [7].
2. Case
A 72-year-old man was referred by his general practitioner for chronic bilateral nasal congestion, worse at night, and purulent nasal secretions predominantly in the morning. In addition to multiple courses of antibiotics, he had previously tried fluticasone furoate, mometasone furoate, and beclomethasone dipropionate nasal sprays to no avail. He retained his sense of smell and denied post-nasal drip, sneezing, breathlessness, or cough. He had no history of excess fatigue, weight loss, or night sweats. His past medical history included essential hypertension for which he was taking perindopril 2 mg once daily (OD) and a previous cerebral infarction treated with clopidogrel 75 mg OD. He is an ex-smoker with no relevant family history.
Nasal endoscopy (30° oblique rigid Hopkins 3.0 mm) performed in our rhinology mega-clinic revealed an oedematous friable bleeding nasal mucosal surface with significant crusting but no polyps per se. Biopsy samples were taken from the middle turbinate and crusting was debrided. Nasal douching with saline/bicarbonate was recommended, and he was treated with concurrent azithromycin 500 mg OD and prednisolone 25 mg OD for 5 and 7 days, respectively, pending further results.
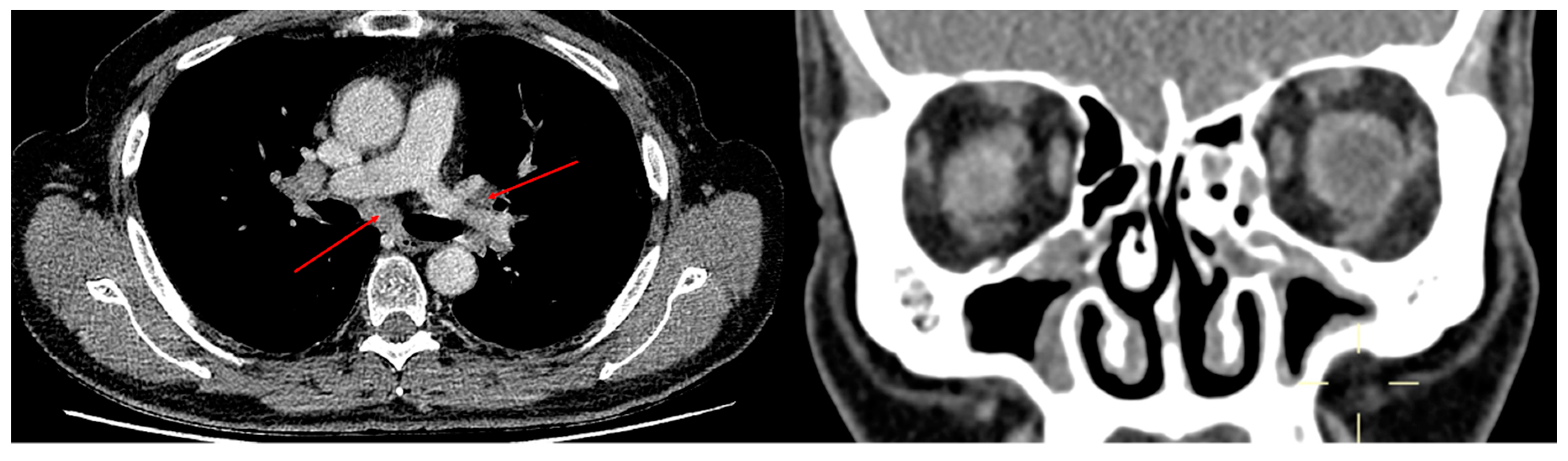
Initial laboratory results and subsequent lymphocyte surface marker analysis are presented in Table 1. Protein electrophoresis identified two monoclonal bands consistent with IgM lambda and kappa bands quantifiable at 10 g/L. CT sinus scan (Figure 1) revealed mucosal disease predominantly affecting the ethmoid bullae and ostiomeatal complex, with a Lund Mackay score of 12. Apart from minor basal atelectasis, chest X-ray was normal. Histopathology subsequently revealed chronic non-specific inflammatory changes with mixed microbial flora abundant in gram-positive cocci.
Our patient was consequently referred to haematology where on physical examination there was no clinical evidence of palpable lymphadenopathy or hepatosplenomegaly. A CT chest-abdomen-pelvis scan (Figure 1) identified significant mediastinal and hilar lymphadenopathy and the combination of serum and radiological findings in turn made the clinical diagnosis of B-cell lymphoproliferative disorder (BLPD).
3. Discussion
In this case report, we present a patient referred from primary care for CRS without nasal polyposis and suspicious atypical features who was subsequently diagnosed with low grade BLPD. To our knowledge, although there have been case series on localised sinonasal lymphoma [8,9], we have not yet encountered a case report of BLPD masquerading as CRS.
While the diagnosis of BLPD was clinical, the value of endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) of mediastinal and hilar lymph nodes in the diagnosis of lymphoma is controversial [10] and hence a negative result would likely still mandate surgical mediastinoscopy confirmation. In the absence of B symptoms or abnormal full blood count, a watch and wait strategy is usually employed for low grade BLPDs and therefore no bone marrow or lymph nodes were sampled in our patient, to avoid unnecessary additional risk.
The abundance of gram-positive cocci is likely to infer chronic staphylococcal infection, which in turn is highly suggestive of immunosuppression. Although the acute abundance of gram-positive cocci commonly infers nasal colonisation with Streptococcus pneumoniae, failure to respond to recurrent courses of antibiotic therapy likely results in a selection pressure towards treatment resistant organisms such as Staphylococcus aureus [11]. Risk factors for S. aureus nasal colonisation depends on host factors but is more frequent in conditions that result in immunosuppression such as in patients infected with human immunodeficiency virus (HIV) or those who are diabetic and undergoing dialysis [12]. The combination of immunosuppression, IgM paraproteinaemia, and extensive mediastinal and hilar lymphadenopathy is probably sufficient to make a clinical diagnosis of BLPD.
The key learning point here is that although nasal crusting is a frequently encountered clinical feature that often requires no specific treatment, it is nevertheless crucial for the clinician to identify the small number of cases that are due to a potentially wide differential diagnosis including systemic inflammatory disorders such as vasculitis, malignancy, and infection, amongst others [13]. Clinicians should have a high index of clinical suspicion and our usual practice should be to check serum protein electrophoresis and immunoglobulins in all patients presenting with CRS-like symptoms and signs of immunosuppression as it may lead to an earlier diagnosis and potentially better outcome for patients.
4. Conclusions
Patients with chronic rhinosinusitis who present with atypical clinical features such as nasal crusting and treatment resistant organisms may have underlying immunosuppression. Identifying this in a timely manner with further focused investigations may lead to earlier diagnoses and better outcomes for patients.
Author Contributions
The manuscript has been read and approved by all the authors and the requirements for authorship have been met. We (authors) certify that we have (collectively) personally written 100 percent of the manuscript. The manuscript has not been published previously in print/electronic format or in another language and the manuscript is not under consideration by another publication or electronic media. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data sharing not applicable. No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
There are no financial conflict of interest to disclose.
References
- Vaidyanathan, S.; Barnes, M.; Williamson, P.; Hopkinson, P.; Donnan, P.T.; Lipworth, B. Treatment of Chronic Rhinosinusitis With Nasal Polyposis With Oral Steroids Followed by Topical Steroids: A Randomized Trial. Ann. Intern. Med. 2011, 154, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology 2020, 58, 1–464. [Google Scholar] [CrossRef] [PubMed]
- Bachert, C.; Sousa, A.R.; Lund, V.J.; Scadding, G.K.; Gevaert, P.; Nasser, S.; Durham, S.R.; Cornet, M.E.; Kariyawasam, H.H.; Gilbert, J.; et al. Reduced need for surgery in severe nasal polyposis with mepolizumab: Randomized trial. J. Allergy Clin. Immunol. 2017, 140, 1024–1031.e1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gevaert, P.; Van Bruaene, N.; Cattaert, T.; Van Steen, K.; Van Zele, T.; Acke, F.; De Ruyck, N.; Blomme, K.; Sousa, A.R.; Marshall, R.P.; et al. Mepolizumab, a humanized anti-IL-5 mAb, as a treatment option for severe nasal polyposis. J. Allergy Clin. Immunol. 2011, 128, 989–995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, R.; Kuo, C.R.; Lipworth, B. Disconnect between effects of mepolizumab on severe eosinophilic asthma and chronic rhinosinusitis with nasal polyps. J. Allergy Clin. Immunol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Knowles, D.M. Immunodeficiency-associated lymphoproliferative disorders. Mod. Pathol. 1999, 12, 200–217. [Google Scholar] [CrossRef] [PubMed]
- Debord, C.; Wuillème, S.; Eveillard, M.; Theisen, O.; Godon, C.; Le Bris, Y.; Béné, M.C. Flow cytometry in the diagnosis of mature B-cell lymphoproliferative disorders. Int. J. Lab. Hematol. 2020, 42, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Steele, T.O.; Buniel, M.C.; Mace, J.C.; El Rassi, E.; Smith, T.L. Lymphoma of the nasal cavity and paranasal sinuses: A case series. Am. J. Rhinol. Allergy 2016, 30, 335–339. [Google Scholar] [CrossRef] [PubMed]
- Peng, K.A.; Kita, A.E.; Suh, J.D.; Bhuta, S.M.; Wang, M.B. Sinonasal lymphoma: Case series and review of the literature. Int. Forum Allergy Rhinol. 2014, 4, 670–674. [Google Scholar] [CrossRef] [PubMed]
- Erol, S.; Erer, O.F.; Anar, C.; Aktogu, S.; Aydogdu, Z. Diagnostic yield of EBUS-TBNA for mediastinal lymphoma. Eur. Respir. J. 2016, 48, PA3853. [Google Scholar] [CrossRef]
- Brook, I. Microbiology of Sinusitis. Proc. Am. Thorac. Soc. 2011, 8, 90–100. [Google Scholar] [CrossRef] [PubMed]
- Sakr, A.; Brégeon, F.; Mège, J.-L.; Rolain, J.-M.; Blin, O. Staphylococcus aureus Nasal Colonization: An Update on Mechanisms, Epidemiology, Risk Factors, and Subsequent Infections. Front. Microbiol. 2018, 9, 2419. [Google Scholar] [CrossRef] [PubMed]
- Yaneza, M.M.; Broomfield, S.J.; Morar, P. 12 minute consultation: A patient with nasal crusting. Clin. Otolaryngol. 2010, 35, 313–320. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Transverse CT chest image with arrows indicating mediastinal and hilar lymphadenopathy. Coronal CT sinus image depicting disease affecting the ethmoid bullae and ostio-meatal complex.
Figure 1.
Transverse CT chest image with arrows indicating mediastinal and hilar lymphadenopathy. Coronal CT sinus image depicting disease affecting the ethmoid bullae and ostio-meatal complex.


{kind=link}
Table 1.
Laboratory results and lymphocyte surface marker analysis.
| White Blood Cells (×109/L) | 9.8 | Corr. Calcium (mmol/L) | 2.44 |
| Haemoglobin (g/L) | 136 | C-reactive protein (mg/L) | <4 |
| Haematocrit (%) | 41.3 | Sodium (mmol/L) | 141 |
| Platelets (×109/L) | 328 | Potassium (mmol/L) | 4.8 |
| Neutrophils (×109/L) | 5.4 | Urea (mmol/L) | 6.4 |
| Lymphocytes (×109/L) | 3.5 | Creatinine (µmol/L) | 86 |
| Eosinophils (×109/L) | 0.14 | PR3/MPO antibodies | negative |
| Plasma viscosity (mPa.s) | 1.99 ↑ | CTD screen | negative |
| Total bilirubin (µmol/L) | 5 | RAST to ABCDH | negative |
| ALT (U/L) | 25 | RAST to grass | weakly positive |
| ALP (U/L) | 110 | Total IgE (kU/L) | 89.5 |
| Albumin (g/L) | 36 | IgG (g/L) | 9.94 (NR 5.5–13) |
| Pneumococcal ab (mg/L) | 52.64 | IgA (g/L) | 1 (NR 0.5–4) |
| IgM (g/L) | 10.2 ↑ (NR 0.5–2.5) | ||
| CD3 (%) | 88.57 ↑ | CD19 (%) | 3.53 |
| CD3 (×106/L) | 2922 ↑ | CD19 (×106/L) | 116 |
| CD4 (%) | 32.94 ↑ | NK cells (%) | 6.88 |
| CD4 (×106/L) | 1087 | NK cells (×106/L) | 227 |
| CD8 (%) | 53.6 ↑ | CD4/CD8 ratio | 0.62 ↓ |
| CD8 (×106/L) | 1769 ↑ |
A = aspergillus fumigatus; ALP = alkaline phosphatase; ALT = alanine aminotransferase; B = silver birch; C = cat dander; CD = cluster of differentiation; CTD = connective tissue disease; D = dog dander; H = house dust mite; MPO = myeloperoxidase; NK = natural killer; NR = normal range; PR3 = proteinase-3; RAST = radioallergosorbent testing for specific IgE. ↑ and ↓ denote values outside NR.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Chan, R.; Kuo, C.R.; Lipworth, B. Low-Grade B Cell Lymphoproliferative Disorder Masquerading as Chronic Rhinosinusitis. Sinusitis 2021, 5, 1-4. https://0-doi-org.brum.beds.ac.uk/10.3390/sinusitis5010001
AMA Style
Chan R, Kuo CR, Lipworth B. Low-Grade B Cell Lymphoproliferative Disorder Masquerading as Chronic Rhinosinusitis. Sinusitis. 2021; 5(1):1-4. https://0-doi-org.brum.beds.ac.uk/10.3390/sinusitis5010001
Chicago/Turabian StyleChan, Rory, Chris RuiWen Kuo, and Brian Lipworth. 2021. "Low-Grade B Cell Lymphoproliferative Disorder Masquerading as Chronic Rhinosinusitis" Sinusitis 5, no. 1: 1-4. https://0-doi-org.brum.beds.ac.uk/10.3390/sinusitis5010001