
Real-Time Operative Coding for Endoscopic Sinonasal Procedures: Quality Improvement in Practice


Nottingham University Hospitals NHS Trust, Nottingham NG7 2FT, UK
*
Author to whom correspondence should be addressed.
Sinusitis 2021, 5(1), 32-44; https://0-doi-org.brum.beds.ac.uk/10.3390/sinusitis5010004
Submission received: 9 December 2020
/
Revised: 19 January 2021
/
Accepted: 1 February 2021
/
Published: 4 February 2021
Abstract
:Simple Summary
Clinical coding is important not only for reimbursement but also to guarantee high quality care. Coding accuracy is highly dependent on coder experience and quality of operative notes. The aim of this project is to establish whether integration of the intraoperative coding sticker (ICS) in operation notes significantly improves the legibility and accuracy of coding of sinonasal procedures. The sticker represents a low-cost option in institutions lacking electronic patient records. It can also extrapolate to a range of other complex operative procedures.
Abstract
Objective: investigate the impact of an intraoperative coding sticker (ICS) on the accuracy of coding in endoscopic sinonasal procedures. Methods: this was a two-cycle audit evaluating the accuracy (and financial impact) of intraoperative coding of sinonasal procedures at a single tertiary centre. An ICS was introduced following consultation with the coding department. The accuracy of coding was measured before (cycle 1) and after (cycle 2) the ICS was introduced to a pilot firm and compared to a control firm. The ICS was used in 35% of the pilot firm cases. Results: the accuracy of clinical coding for endoscopic sinus surgery was 60% in the first cycle. Switching to the ICS has improved the accuracy in that firm from 50% in first cycle to 70% in the second cycle (p = 0.936; Chi-squared test). The median reimbursement for endoscopic sinus surgery was equal in both cycles of £1493.00 per patient. However, inaccurate coding resulted in £109.92 excess tariff payment in first cycle and £130.96 deficiency in the second cycle. Users of ICS reported it to be easy to use for clinicians, staff and clinical coders, whilst minimizing human error. Conclusions: The integration of the ICS improves the coding in sinonasal procedures and offers low-fidelity option alternative to live coding on the computer. The accuracy was not statistically significant in the study possibly due to the low number of observations. This can allow a precise coding standard with reliable service remuneration.
1. Introduction
Clinical coding is the process of translating medical terminology into an international syntax that can be a familial process for use by non-medical staff. It covers different aspects for the disease such as diagnosis, morbidity, procedures and complications [1]. Clinical coding is important not only for reimbursement but also to guarantee high quality care. The Hospital Episode Statistics (HES) database comprises activity data, including individual patient records for all inpatient admissions, outpatient appointments and A&E attendances [2]. These codes incorporate HES database, which is subsequently used in decisions regarding local service plans and monitoring month-on-month clinical activity [1,3].
HES data is generated in the National Health Service (NHS) in England using two standardized coding systems: the international classification of diseases (ICD) and the office of population censuses and surveys (OPCS) classification [4]. The 10th version (ICD-10) has been used in the UK since 1995 to classify the diseases and health conditions of patients [5]. In the current version of OPCS-4.8, each intervention and surgical procedure has an allocated code [6]. The Health Resource Group (HRG) is the method of summarizing the ICD and OPCS codes into isoresource units that can be exchanged into a predetermined currency called “tariffs” [3]. This is the English equivalent of the Diagnosis Related Groups (DRG) in Europe. It has evolved in use from benchmarking to reimbursement. In 2002, a further prospective fixed national payment scheme per patient according to the HRG was allocated [2]. This way, the health care provider can generate income for their activity [3].
This whole process is performed by trained medical coders without clinician involvement. The accuracy of coding depends on a myriad of actors including coding experience and access to the relevant information to generate HRG. Although most cases are relatively easy to code, occasionally coders will encounter a non-familiar operative note to code or complex procedures requiring in-depth research and prolonged communication with clinicians to achieve the correct code [7]. A recent publication explored the problems of coded data that identified the following actors including variability in the used documents for coding, illegibility of handwriting, increased errors when transcribed from paper, difficulties in the diagnoses’ coding, coding delay and insufficient resources and tools to help coders [8].
Within the otolaryngology specialty, extensive work conducted by Nouraei et al. demonstrated where difficulties in this complicated translation of clinical care in the financial reward could occur. HRG had a reported accuracy of 80% in capturing primary diagnosis and procedures [1,9,10]. More specifically in rhinology, the coding in septoplasty and septorhinoplasty was demonstrated to be mistranslated in just under 15% of procedures [7].
We decided to perform this audit on sinonasal procedures due to the frequent required clarification of the operative notes by the clinical coders. With functional endoscopic sinus surgery (FESS), the tariffs vary depending on whether a basic, intermediate, or complex FESS is undertaken. Therefore, the subtle differences in subprocedures in FESS could feasibly be misinterpreted during this translation. The audit aimed to introduce a new live low-cost intraoperative coding to minimize errors of clinical coding. To our knowledge, there has been no study or audit that specifically examines the extent and impact of coding inaccuracy in FESS. No ethical committee consideration has been required during for that quality improvement audit.
2. Materials and Methods
A quality improvement project was conducted through a two-cycle audit in a single otorhinolaryngology tertiary centre.
The clinical codes (OPCS) used in sinonasal surgery, in addition to their HRG and current tariff, were collected from the divisional clinical coding department after discussion with senior rhinology (Table 1). The list included all sinonasal surgical steps with the associated OPCS and tariff.
Patients were identified from the electronic operation (Bluespier theatre management system) records for the two specialist rhinologists in the trust. All patients who had an endoscopic sinonasal procedure for elective or emergency condition were identified using ICD codes (J31.0, J32.9, J34.1, G96.0, R04.0 and H05.0). Patients who underwent septoplasty (except for access), septorhinoplasty or turbinate surgery as a primary procedure were excluded from the study.
The first cycle of the audit was a retrospective analysis of the accuracy of the coding by clinical coding department along with the processed tariffs. All patients consecutively operated between May and August 2017 were analysed. Two independent otolaryngologists recoded the same operations using the coding list without discrepancies and generated corresponding HRG coding (OPCS-S and HRG-S), which was used as a standard measure. The original reports for both OPCS and HRG were obtained from clinical coding department for comparison of their accuracy (OPCS-O and HRG-O respectively). The associated tariffs for the two arms were calculated.
Analysis of any discrepancy between the two reports was undertaken to describe the errors in coding, which were classified into upcoding or undercoding (original tariff was higher or lower than standard respectively, e.g., missing additional procedures). A third description of wrong coding was used where incorrect recording of primary operation notes into their corresponding OPCS (whether the tariff was equal between the original and standard HRG or not). Subjective analysis of the challenges encountered was recorded for the inaccurate coding. The ICD-10 coding for the patient was not recorded in the clinician standard report, as the primary aim of the study was to assess the accuracy of operative recording and translation to OPCS codes. The recommendation from the first cycle was discussed in the information governance otolaryngology meeting for implementing the intraoperative coding sticker (ICS) into operation notes.
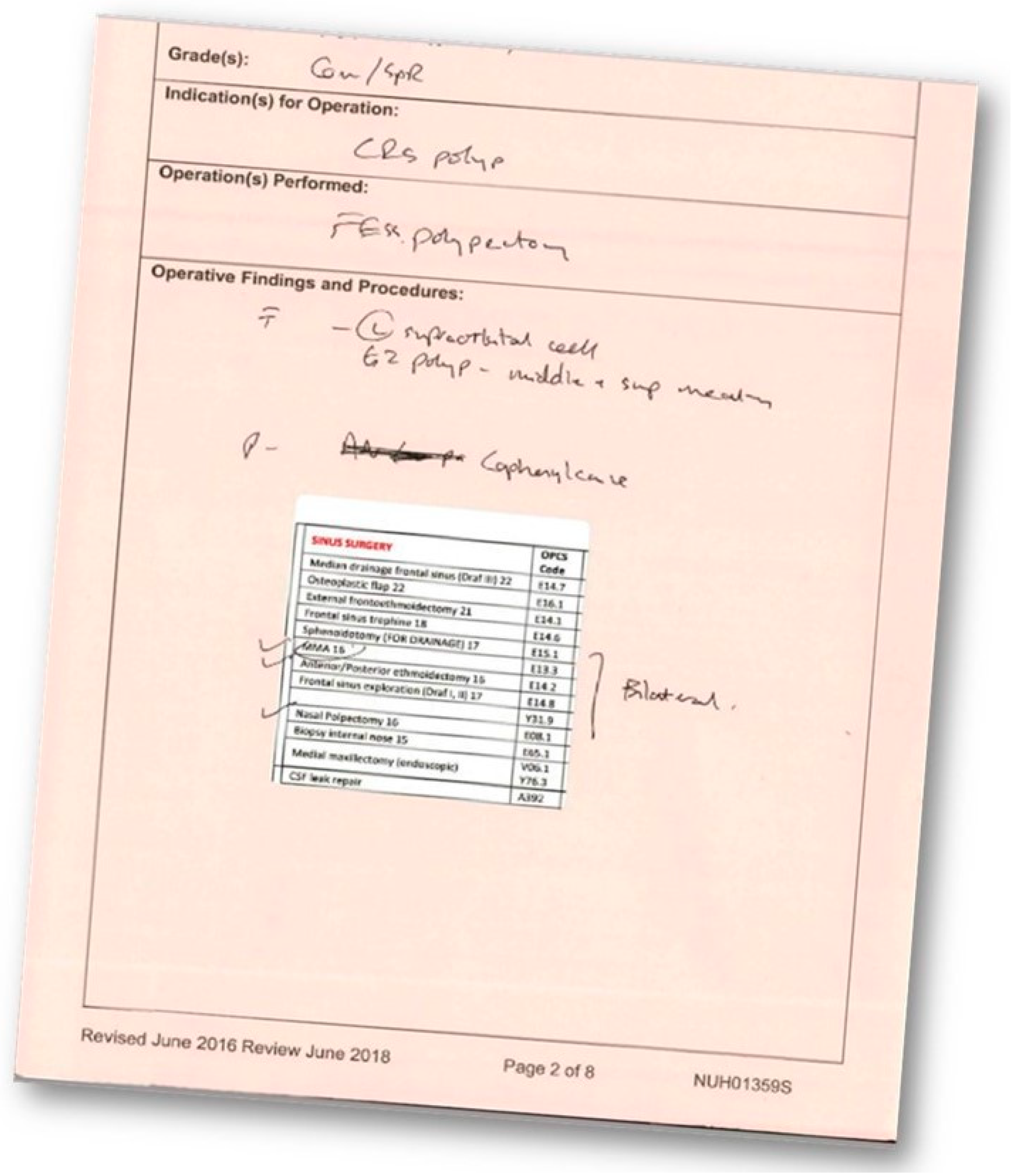
The second prospective cycle was conducted between September and December 2017. In this cycle, ICS was introduced into the operation note after refinement with clinical coding department for usage (Figure 1) to act as real-time coding of the event. A non-randomized controlled approach was used where one rhinology firm piloted the ICS (intervention firm) and the other firm continued with a standard handwriting operation note (non-intervention firm).
Microsoft Excel was used in data collection and analysis. In both cycles, demographic data was collected. Statistical Package for Social Science (SPSS) version 22 (Chicago, IL, USA) was used through Chi-square tests for statistical analysis. A one-way ANOVA analysis was used for statistical comparison between the errors of coding in both cycles.
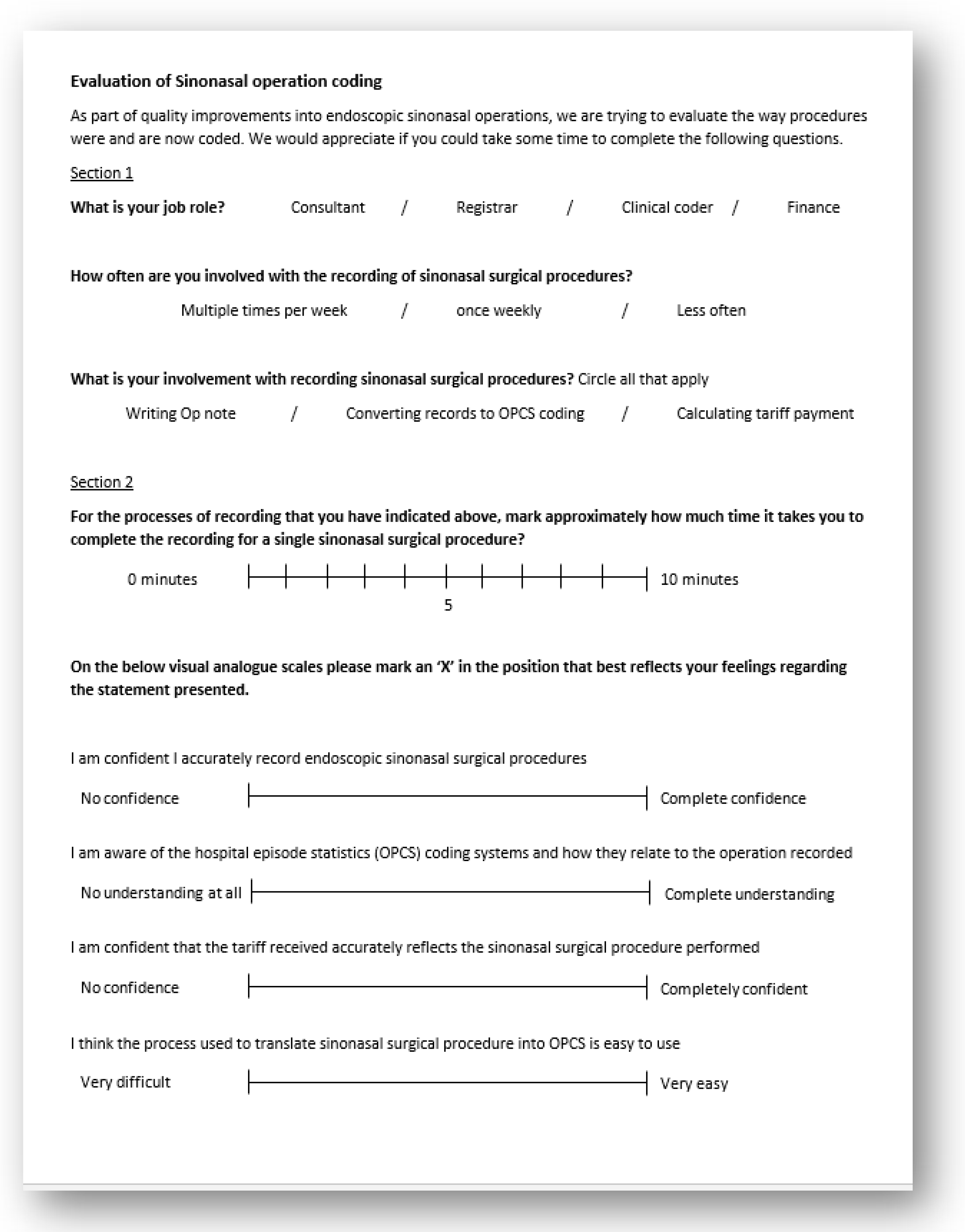
A feedback questionnaire (Figure 2) from involved clinicians and clinical coding team was conducted at the end to gauge usability, understandability and feasibility of the intervention.
3. Results
3.1. First Cycle (May 2017–August 2017)
There were 45 patients with a median age of 53.5 years (IQR 34.8–66.2).
The revised coding by clinicians (OPCS-S) found that the original clinical coding report (OPCS-O) was 60% accurate across both rhinology firms. The inaccuracy of coding is further broken down to 18% upcoding, 9% undercoding and 13% wrongful coding. Detailed summary of coding errors and financial reimbursement are summarized in Table 2.
The median projected tariff for the original OPCS-O and the revised OPCS-S was equal at £1493.0 per patient (IQR 1317.0–1493.0). The income based on revised coding by clinicians generated £61,690. The original coding (without uplifts for ICD codes) brought in a cumulative income of £66,634. The overall difference in tariff per patient was £109.90 in excess.
3.2. Second Cycle (September and December 2017)
There were 49 patients with a median age of 54.7 years (IQR 45.5–68.5).
The revised coding by clinicians (OPCS-S) found that the original clinical coding report (OPCS-O) was overall 59% accurate across the two rhinology firms. The inaccuracy of clinical coding was further broken down to 4% upcoding, 20% undercoding and 16% wrongful coding. The intervention firm used the ICS sticker in 35% of the endoscopic sinus surgery they performed (10 out of 28). Seven of 10 where the ICS was used were correctly coded. This gave the intervention firm an overall 61% accuracy, compared to 57% accuracy in a non-intervention firm (without stickers). Inside the intervention firm, 55% (10 out of 18) who did not have the ICS used were accurate. When comparing ICS versus total patients who did not have ICS used for both rhinology firms, accuracy was 61% and 56% respectively. Of the three inaccurate OPCS-O codes when using the ICS, two were undercoded due to omission of some operative details (sphenoidotomy and Draf III) and one was wrongly coded, most likely due to the rarity of the operation and unfamiliar clinical coding of it (biopsy pterygopalatine fossa was coded as biopsy maxillary antrum).
The income based on revised coding by clinicians would have generated £75,324. The original coding (without uplifts for ICD codes) brought in a cumulative income of £69,169. There was a £130.96 deficiency in income per patient. The median tariffs generated from OPCS-S and OPCS-O were equal at £1493.0 (IQR 1317.0–1493.0).
3.3. Both Cycles
The accuracy of clinical coding for each firm across the two cycles are summarized in Table 3.
The error of upcoding was observed often during the summation process of different captured codes from operation notes. The wrong coding or undercoding were commonly encountered during coding of non-standard unfamiliar surgical steps. The ANOVA test for the three variables of up, under and wrong coding in both cycles showed a p-value of 0.82 and F-value was 0.21 (no significant difference in cause of miscoding between firms).
There was no significant difference in accuracy between the first and second cycles in the rhinology firm that used the ICS (p = 0.801; chi-squared). The accuracy of coding in each rhinology firm is presented in Table 3 to illustrate the difference when intraoperative coding sticker (ICS) was applied.
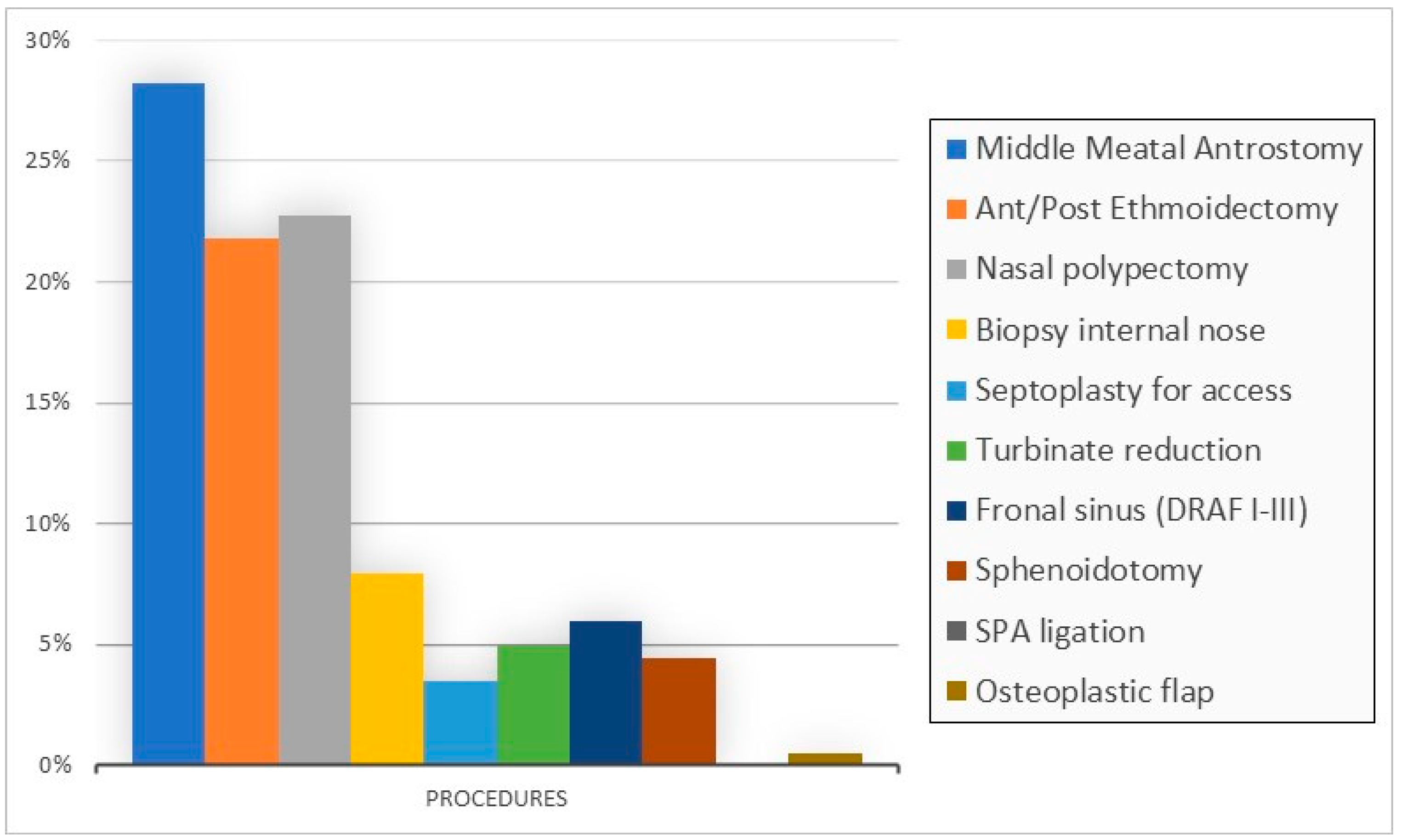
The £1493.0 tariff was assigned automatically when advanced surgical steps such as sphenoidotomy or frontal trephine surgery were undertaken. Surgery also assigned this tariff when there was a combination of other standard steps creating a combination score greater than 4. For example, nasal polypectomy, middle meatal antrostomy and ethmoidectomy generated a combination score of 6. Each of these three steps was used in more than 20% of the patients and middle meatal antrostomy was the commonest surgical step (Figure 3).
There was no statistically significant difference between accuracy of registrars and consultants in their recorded operations in the two cycles (p = 0.270; chi-squared).
The feedback was completed by five doctors in the department including the two independent clinicians auditing the project. This found that the process of coding of operative notes was difficult and it took 10 min in a single sinonasal procedure for coding. Four out of five rated the ICS as easy to interpret, shorter time to code and less chance for errors.
4. Discussion
In the United Kingdom (UK), clinical coding is done after the patient’s discharge by trained non-medical coders. The sources of information for this process varied between different trusts. Some hospitals rely on discharge summaries; others revisit patients’ notes or depend on the diagnosis and procedures recorded on the electronic system of patient care [10].
HRG4 represents a major development from HRG3.5, which was designed to evolve year on year [2]. It covers patient visits including critical care admission, emergency and outpatient episodes. It refines the classification of complications and comorbidities [2]. Nouraei et al. showed a significant reduction in the number of changed HRG from 16% (HRG3.5) to 9% (HRG4) in auditing otolaryngology procedures [1].
In the OPCS codes, the letter “E” codes for procedures in the mouth, head, neck and ears [6]. In otolaryngology, there is a wide range of procedures performed in close anatomical regions with similar codes. Therefore, coding is intrinsically susceptible to inaccuracy during interpretation of an operation note or written communication. Nouraei et al. recognizes this problem became more evident with the expansion of HRG version 4 [1].
There is a single OPCS for every surgical step in endoscopic sinonasal surgery. Steps of similar complexity in sinus surgery are reflected in being assigned a common HRG code. In addition, OPCS codes offer a combination score, which are used to calculate the complexity of the overall FESS procedure and assign the appropriate HRG code [6]. For instance, ethmoidectomy and middle meatal antrostomy each has a different OPCS (E13.3, 14.2) but the same HRG of CA29. When added together in operative notes, the combination upgrade to HRG CA28Z. This combination HRG attracted a higher tariff than the individual HRG would, therefore it is important that all parts of the sinus surgery are accurately converted into OPCS.
4.1. Understand Inaccuracy in Coding
The accuracy of clinical coding in otolaryngology in previous research was found to be approximately 75% [10]. Coding errors can arise from multiple sources. Clinicians’ factors include a lack of awareness of coding issues and highly variable recording of operative details between surgeons [11]. Some may use unrecognized abbreviations that are extremely difficult to interpret [11]. Studies have shown that physicians provide information, without assuming the diagnosis. A coder cannot infer the diagnosis if not explicitly written in the health record [8]. Legibility is another issue. Some may use word processing systems or dictate letters, while others rely on hand-written notes. Clearly, the clinician must be as specific and clear as possible for capturing reimbursement for rendered procedures [8,11].
Coder factors include recruitment, experience, specialization and time-pressure. It can be challenging for non-medical staff to understand unfamiliar medical terms to produce an accurate report [8,11]. Nouraei highlighted the importance of accurate and legible documentation of medical information by a clinician who is aware of clinical codes. In addition, they proposed the “double-reading with arbitration” to increase detection rate. This involved using two independent clinicians and coders to capture and record coding avoiding transcription errors from the source. They believed this resulted in considerable financial gains with little impact on clinicians [8]. However, their proposed structure is more time and resource consuming as clinical-coders will cost 5% more than coder-coders [10].
Four years later, the same authors changed their practice and recommend “coding in theatre”. Indeed, they stressed on investment in training and reskilling of surgeons in clinical coding [1]. The author found that coding by surgeons alone was just over 30% accurate and depth of coding was significantly lower when compared either with coding by clinical coders or the joined-assured clinician–auditor [1]. Interestingly, in countries such as Portugal, the coders are the physicians, where it might be easier to interpret health records however the problem of incorrect, under and upcoding are still reported [1,8]. Education of both clinicians and coders has shown significant reduction in coding inaccuracy through the reaudit work of Cheema and Khwaja [11]. The idea of coding in theatre (real-time coding) or coding at the source was introduced to the NHS following its use in private practice, however both have fundamentally different uses of OPCS [1,7].
There is a shift to computerized theatre management system such as “Operating Room Management Information System” (ORMIS) in many centres. The procedural coding is normally carried out by theatre nurses at the point-of-care. In theory, incorporating clinical coding into the daily workflow pattern (real-time coding) should reap major benefits as the clinical teams are ideally placed to produce accurate timely data [12]. Colville compared the coding of plastic surgery operations by theatre nursing staff and concluded that clinical coding in theatre was so poor it should be discontinued [13]. Unfortunately, the accuracy of ORMIS cannot mimic the standard of trained medical coders. There are several reasons for this discrepancy, including a lack of training of nurses and feedback quality control systems, and poor computerized search facility that can lead to increased error rates [12]. In addition, ORMIS captures the summary of the operation without surgical details, which can upgrade the corresponding HRG in otolaryngology as illustrated before.
A coder focus group suggested improvements in health records and misreading information. A single episode coding is time consuming taking almost a day [8]. They encouraged reducing variability between hospitals, and unifying e-coding and software programs used for coding to allow working anywhere [8].
This influenced the basis for creating the preprinted intraoperative coding sticker (ICS) in our study by mutual collaboration between clinicians and clinical-coders. To improve the granularity further, free text can be added into the operative note where the preprinted ICS is incorporated.
The concept of an ICS is becoming popular in many other specialties such as breast surgery, urology, trauma, oral surgery and neurosurgery [1,7,11,14]. Coding will assist clinicians and managers in many aspects; benchmarking, apportionment of payment from clinical commissioning groups and revalidation of surgeons [14]. The accuracy of ICS systems has been reported as 54% in oral surgery and 81% in neurosurgery [14,15]. The low accuracy rate of coding in oral surgery is related to three factors: the rapid turnover of cases (as majority are the day case), the large number of abbreviations used in recording and paucity of documentation of oral surgeons due to a lack of insight in clinical coding [14]. This all has relevance in sinonasal surgery, which in the UK are predominantly the day case and commonly use an abbreviation and short-terms to describe steps. For example, middle meatal antrostomy is shortened to MMA (OPCS = E13.3), which can be easily misread by coders not specifically looking for it. Nouraei noted 13% change in clinical coding of translated general otolaryngology procedures [1], other authors have shown 14.5% wrong primary procedure coding [16].
Different terms were used in the literature to describe generated errors of coding. In one study, they are termed “correct”, “incomplete” and “incorrect” where incomplete reflect missing translated data [11]. Others refer to this as undercoding. Others used only the terms “correct” and “incorrect” [10,14]. The term “under” or “low” coding was used from studies on septorhinoplasty [7] and medical admission to hospital [9]. Studies have shown that inpatient episodes are more complex than outpatient episodes; therefore, more prone to errors of coding [8]. The practice of upcoding involves shifting the DRG or HRG of a patient to another yielding a higher payment from the third-party to health providers to increase their profits through reimbursement without an increase in the quality of care [15]. A theory on quality was introduced in 2013 to explain the rational that high prices naturally generate higher manipulative efforts and output, hence more auditing effort is required reduce upcoding [17]. The term “incorrect” or “wrong” coding is recognized from a study on hepatopancreatobiliary surgeries in the same health centre as this in our study. The author separated the term “incorrect” from “missing” coding [16].
Upcoding was recognized in the United States chiefly in the profit hospital however it has also been recognized in the National Health Service system in European countries such as Portugal. Peer Review Organizations (PROs) has been introduced in USA to carry out annual monitoring of upcoding however it proved to be inefficient and a worse method than previous hospitals auditing due to a lack of financial incentives to hire coding specialists [18]. Several studies in the United Kingdom could not identify upcoding in their system [14,16]. A systemic review showed that the precise documentation of comorbidities and complications related to procedures could lead to upcoding, which reported to be 1% of hospital episodes in Germany [18]. The author showed improvements in the system over 4-5 years [18]. The current financial burden is small with an estimated average increase of 0.04% in cost [15].
The use of proforma or multidisciplinary coding standard document had improved the coding of primary procedures in different specialties. For example, 5.7% in the septoplasty and septorhinoplasty, 35% in oral surgery and 7.5% in hepatopancreatobiliary [7,14,16]. Furthermore, additional secondary procedures were captured in 17.5%, 41% and 37.6% of these specialties respectively [7,14,16]. Nouraei reported improved coding precision with the multidisciplinary document and benchmarking despite the non-significant drift in HRG [7]. Our study demonstrated that the use of the ICS for sinonasal procedures could increase accuracy of coding to 70%. Although this was not significant, we believe this was likely the effect of a small sample size and further ongoing quality improvement work will be needed to confirm this. The clear myriad of inaccuracy in the first cycle was missing recorded steps, false upgrading minor to major operation, misunderstanding written notes and demonstrating confusion between biopsy of polyp or lesion versus complete excision of it.
4.2. Financial Implication
Inaccurate coding can falsely simplify cases that consume resources, leading to under-recovery of reimbursement, or convey the wrong picture of workload in the department. Previous studies showed an average income loss between £109.46 and £114 per patient or episode, which is consistent with the same finding in our study [1,11]. Interesting, the first cycle showed the exact waste per patient (£109) as Nouraei [1]. Reference to both studies would benchmark any future rhinological remuneration as each cover different spectrum of sinonasal surgery.
The cumulative HRG score in FESS can vary between CA28Z (£1493) and CA26Z (£2301) as the complexity increases. The excess tariff per patient in the first cycle reflects the over expression of the complexity of the procedures when combining different OPCS and upgrading into corresponding HRG. The under-payment in the second cycle reflects two problems. The first is missing OPCS codes especially for sphenoidotomy. The second is the over-reduction of data that does not match a finite list of common operative steps. The firm conducting more complex sinus/skull base surgery had less accurate coding than the other firm in the first cycle. There was obvious improvement to accuracy when that firm applied ICS. The presence of the not otherwise classified “NOC” code in OPCS and HRG could be a compromised solution for both a clinical coder and clinicians when the non-recognized surgical step is recorded. Alternatively, as discussed earlier the need for free text space that is clearly part of the ICS can be used to state where a rare or particularly complex step of the procedure has been undertaken. Although “NOC” would attract uniform HRG, more importantly, this will prompt the clinical-coder to recognize and upgrade undefined OPCS for surgical steps.
4.3. Strength and Limitation in Our Study
This audit shows a simple, robust system that can be applied in the theatre. The net result was that procedural coding is no longer duplicated in time, location and administration. The proforma reflects increased communication and engagement with clinical coding for real estimation of the department workload.
The observed difference was not statistically significant in this paper however we believed that this might be an issue with study power. We unfortunately encountered several logistical difficulties in implementing the ICS stickers even in the intervention firm, which resulted in only around a third of eligible procedures being recorded in the new way. This is an important learning point from this work. Despite these issues, it is worth noting the importance of ICS stickers in both the accuracy and reliability of coding. In the intervention firm, despite using the ICS in approximately a third of cases for the 2nd cycle, 60% of cases using the ICS sticker were accurate. In the first cycle (without ICS), only 50% were accurate. In the non-intervention firm (without ICS), there was a great degree of variation of the clinical coding between the 1st (74%) and 2nd cycle (57%). This therefore demonstrated a need to collect data over a longer period in larger samples to account for variability in individual operations and operating lists.
The literature recognizes a persistent increase in the number of secondary diagnoses as a proxy for age, severity of cases and associated comorbidities [17]. There is a role for the regression model to account for the number of secondary diagnoses and age as an important driving factor for upcoding [17]. In our trust, clinical coding only upgrades the HRG with related ICD in sinus surgery if the patient has had an overnight stay or added other procedures in the preparation for the surgery due to high surgical or anaesthetic risk. Therefore, when sinus surgery is deployed as a day case, there is no addition of ICD for the comorbidity to the final HRG code. This therefore means that our presentation of the financial implications is not hypothetical, and the figures reported are a relatively accurate representation of the “real-life” day case sinus surgery cost.
4.4. Feedback on Intraoperative Coding
The clinicians described the new ICS document as easy to interpret. As previous recognized difficulty in interpretation can lead to miscoding and the ICS is thought to minimize the error of human factors. Continuous evolution with ICS will reflect the complexity of sinus surgery especially with the addition of anterior skull base refining jobs such as CSF leak repair or endoscopic ablation procedure as medial maxillectomy. It can be easily upgraded in the future into electronic recoding of operation notes by scanning a barcode that can be fixed next to each checklist.
5. Conclusions
The integration of the ICS improves the ease of coding in sinonasal procedures and offers a low-cost supplement to complex clinical coding prone to error. This can also be extrapolated to other subspecialties in otorhinolaryngology, allowing improvement coding standards with reliable service remuneration across the health service. The non-significant improvements in accuracy are possibly related to the small number of ICS used in the intervention firm in the second cycle.
Author Contributions
Clinical coding is a challenging process to ensure proper remuneration in each hospital. The introduction of real time coding in theatre by doctors was always a challenge for training and time restrain in theatre. There is no previous study that introduced clinical coding document in sinus surgery with assessment of service improvement. The authors designed the document that can be used to benchmark service improvement in very popular ENT procedures i.e., endoscopic sinus surgery. B.M. (ENT Specialty Registrar) is the main and corresponding author who audited the improvement in the service, wrote first draft of the paper. Y.R. designed the operative sticker checklist from hospital episode statistic with collaborative work with clinical coding department. J.D.W. assisted in data collection, analysis and draft preparation. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was registered as an audit for service improvement in clinical practice hence ethical review and approval were not required.
Informed Consent Statement
Formal consent was waived after discussion with audit department as only anonymous data were used in data collection.
Data Availability Statement
The data are not publicly available without and through the permission of Nottingham University Hospitals.
Acknowledgments
Joanne Riggs; Clinical coding, Nottingham University Hospitals NHS trust, UK. Kathryn Alvey; Finance and procurement, Nottingham University Hospitals NHS trust, UK. Katherine Midwinter; ENT Consultant, QMC, Nottingham University Hospitals NHS trust, UK.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- Nouraei, S.A.R.; Hudovsky, A.; Virk, J.; Chatrath, P.; Sandhu, G.S. An audit of the nature and impact of clinical coding subjectivity variability and error in otolaryngology. Clin. Otolaryngol. 2013, 38, 512–524. [Google Scholar] [CrossRef] [PubMed]
- Mason, A.; Ward, P.; Street, A. England: The Healthcare Resource Group system. In Diagnosis-Related Groups in Europe, Ch 12, 12; Busse, R., Ed.; Open University Press: Berkshire, UK, 2011; pp. 197–220. [Google Scholar]
- NHS Digital. Hospital Episode Statistics. Available online: http://content.digital.nhs.uk/hes (accessed on 24 November 2017).
- World Health Organization. International Classification of Diseases. Available online: http://www.who.int/classifications/icd/en/ (accessed on 24 November 2017).
- NHS Digital. Clinical Classifications. Available online: https://digital.nhs.uk/article/1117/Clinical-Classifications (accessed on 24 November 2017).
- NHS Digital. SCCI0084—OPCS Classification of Interventions and Procedures. Available online: http://content.digital.nhs.uk/isce/publication/scci0084 (accessed on 24 November 2017).
- Nouraei, S.A.R.; Hudovsky, A.; Virk, J.S.; Saleh, H.A. Impact of developing a multidisciplinary coded dataset standard on administrative data accuracy for septoplasty, septorhinoplasty and nasal trauma surgery. J. Laryngol. Otol. 2017, 131, 341–346. [Google Scholar] [CrossRef]
- Alonso, V.; Santos, J.V.; Pinto, M.; Ferreira, J.; Lema, I.; Lopes, F.; Freitas, A. Problems and Barriers during the Process of Clinical Coding: A Focus Group Study of Coders’ Perceptions. J. Med. Syst. 2020, 44, 44–62. [Google Scholar] [CrossRef]
- Nouraei, S.A.R.; Virk, J.S.; Hudovsky, A.; Wathen, C.; Darzi, A.; Parsons, D. Accuracy of clinician-clinical coder information handover following acute medical admissions: Implication for using administrative datasets in clinical outcomes management. J. Public Health (Bangkok) 2015, 38, 352–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nouraei, S.A.R.; O’Hanlon, S.; Butler, C.R.; Hadovsky, A.; Donald, E.; Benjamin, E.; Sandhu, G.S. A multidisciplinary audit of clinical coding accuracy in otolaryngology: Financial, managerial and clinical governance considerations under payment-by-results. Clin. Otolaryngol. 2009, 34, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Juniat, V.; Athwal, S.; Khandwala, M. Clinical coding and data quality in oculoplastic procedures. Eye J. 2019, 33, 1733–1740. [Google Scholar] [CrossRef] [PubMed]
- Maclean, D.; Younes, H.B.; Forrest, M.; Towers, H.K. The accuracy of real-time procedure coding by theatre nurses: A comparison with the central national system. Health Inform. J. 2012, 18, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Colville, R.J.; Laing, J.H.; Murison, M.S. Coding plastic surgery operations: An audit of performance using OPCS-4. Br. J. Plast. Surg. 2000, 53, 420–422. [Google Scholar] [CrossRef] [PubMed]
- Naran, S.; Hudovsky, A.; Antscherl, J.; Howells, S.; Nouraei, S.A.R. Audit of accuracy of clinical coding in oral surgery. Br. J. Oral Maxillofac. Surg. 2014, 52, 735–739. [Google Scholar] [CrossRef] [PubMed]
- Barros, P.; Braun, G. Upcoding in a National Health Service: The evidence from Portugal. Health Econ. 2017, 26, 600–618. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.; May, C.; Di Carlo, S.; Beckingham, I.; Cameron, I.C.; Gomez, D. Coding in surgery: Impact of a specialized coding proforma in hepato-pancreato-biliary surgery. ANZ J. Surg. 2018, 88, 621–625. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, M.; Siciliani, L. Manipulation and auditing of public sector contracts. Eur. J. Political Econ. 2013, 32, 251–267. [Google Scholar] [CrossRef]
- Lüngen, M.; Lauterbach, K.W. Upcoding—Eine Gefahr für den Einsatz von Diagnosis-Related Groups (DRG)? [Upcoding—A risk for the use of diagnosis-related groups]. Dtsch. Med. Wochenschr. 2000, 125, 852–856. (In German) [Google Scholar] [CrossRef] [PubMed]
- Haliasos, N.; Rezajooi, K.; O’Neill, K.S.; Van Dellen, J.; Hudovsky, A.; Nouraei, S. Financial and clinical governance implications of clinical coding accuracy in neurosurgery: A multidisciplinary audit. Br. J. Neurosurg. 2010, 24, 191–195. [Google Scholar] [CrossRef]
Figure 1.
An example of an operation note using the first edition of the intraoperative coding sticker (ICS).
Figure 1.
An example of an operation note using the first edition of the intraoperative coding sticker (ICS).

Figure 2.
Feedback questionnaire.

Figure 3.
Sinonasal procedure performed by OPCS-S coding.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Multidisciplinary coding standard (MCS) used to record SINUS SURGERY during the study (NB. Further add-ons and additional procedures with and without uplifts in code not included here for simplicity).
Table 1.
Multidisciplinary coding standard (MCS) used to record SINUS SURGERY during the study (NB. Further add-ons and additional procedures with and without uplifts in code not included here for simplicity).
| Elements of Sinus Surgery as Recorded in Operation Notes | OPCS Code | HRG Translations | HRG | Tariff (£) | Combination Scores * |
|---|---|---|---|---|---|
| Median drainage frontal sinus (Draf III) | E14.7 | Median drainage of frontal sinus | CA26 | 2301 | |
| Osteoplastic flap | E16.1 | Frontal sinus osteoplasty | CA26 | 2301 | |
| External frontoethmoidectomy | E14.1 | External frontoethmoidectomy | CA26 | 2301 | |
| Frontal sinus trephine | E14.6 | Trephine of frontal sinus | CA28 | 1493 | 4 |
| Sphenoidotomy (FOR DRAINAGE) | E15.1 | Drainage of sphenoid sinus | CA28 | 1493 | 3 |
| MMA | E13.3 | Intranasal antrostomy | CA29 | 1317 | 2 |
| Anterior/Posterior ethmoidectomy | E14.2 | Intranasal ethmoidectomy | CA29 | 1317 | 2 |
| Frontal sinus exploration (Draf I, II) | E14.8 | Other specified operations on frontal sinus | CA28 | 1493 | 3 |
| Unspecified exploration of organ NOC | Y31.9 | Unspecified exploration of organ NOC | |||
| Nasal Polpectomy | E08.1 | Polypectomy of internal nose | CA14 | 1259 | 2 |
| Biopsy internal nose | E65.1 | Diagnostic endoscopic examination of nasal cavity and biopsy of lesion of nasal cavity | CA24 | 768 | 1 |
| * Combination codes—If procedures include a combination score use the cumulative score to generate a replacement upgrade code. | |||||
| 12 and above | CA26Z | 2301 | |||
| 8 and above | CA27Z | 1626 | |||
| 4 and above | CA28Z | 1493 | |||
Table 2.
Summary of patients from cycle one with inaccurate Health Resource Group (HRG) coding and tariff payments with associated reasons for inaccuracy.
Table 2.
Summary of patients from cycle one with inaccurate Health Resource Group (HRG) coding and tariff payments with associated reasons for inaccuracy.
| OPCS-S | HRG-S | OPCS-O | HRG-O | Inaccuracy | Explanation | Tarif |
|---|---|---|---|---|---|---|
| E651 | CA24 | E271 | CA83 | Wrong | Convert minor to major | 933 |
| E81, E133, E142, E151 | CA27 | E81, E133, E142 | CA28 | Under | Did not add a step of adenoidectomy | −133 |
| E148, E142, E81, E133 | CA27 | E81, E133, E142, E147 | CA26 | Up | Cumulative score 9 = CA27z not CA26z, E147 Draf III did not happen | 675 |
| E142, E151, E042 | CA28 | E142, E043, | CA29 | Under | Missing step of sphenoidotomy, navigation use was not counted | −176 |
| C81, E36 | CA14 | E81, Y762, E36 | CA22 | Up | Convert simple polypectomy to major nasal excision | 129 |
| E148, E042, E133 | CA28 | E147, E162, E133 | CA29 | Up | Cumulative HRG is over, putting osteoplastic flap instead turbinate reduction | 808 |
| E651 | CA24 | E033, E045 | CA15 | Wrong | Wrong coding | −28 |
| E081, E133, E142, E151 | CA27 | E081, E133, E142 | CA28 | Under | Did not add sphenoidotomy | −133 |
| E148, E142 | CA28 | E147, E142, E042 | CA26 | Up | Cumulative score is over | 808 |
| E081, E133, E036, E142 | CA28 | E083, E133, E036, E142 | CA21 | Up | Escalate to major surgery after adding septoplasty | 194 |
| E081, E133, E142 | CA28 | E641, E133, E142, E069 | CA21 | Up | Add codes to steps not done | 194 |
| E651 | CA24 | E271 | CA83 | Wrong | Convert biopsy postnasal to major mouth operation | 689 |
| E081, E133, E142 | CA28 | E081 | CA14 | Under | Cumulative score is underestimate | −234 |
| E082, E133, E142 | CA28 | E081, E133, E142, E162 | CA21 | Up | Frontal recess clearance recorded as osteoplastic flap | 194 |
| E042 | CA24 | E043 | CA15 | Wrong | The operation was partial turbinectomy (histology) not biopsy | −28 |
| E036, E133, E142, E081 | CA28 | E036, E133, E142, E064, E063 | CA21 | Up | Cumulative is overestimate | 194 |
| E651, E042 | CA24 | E081 | CA14 | Up | Biopsy of papillomatosis not polypectomy | 496 |
| Total | £4944.0 (£109.9 excess per patient in sample) | |||||
Office of population censuses and surveys (OPCS)-S, HRG-S: OPCS, HRG standard use in recording by clinician; OPCS-O, HRG-O: OPCS, HRG original use by clinical coder.
Table 3.
Comparison between accuracy of clinical coding for each firm during 2 cycles.
| % of Accurate Coding | 1st Cycle (no ICS Sticker) n = 45 | 2nd Cycle n = 49 | p-Value * |
|---|---|---|---|
| Intervention firm (using ICS in 35% cases in 2nd cycle) | 50% | 61% ^ | 0.429 |
| Control firm (not using ICS at any point) | 74% | 57% | 0.357 |
| p-value * | 0.140 | 0.801 | |
| Overall | 60% | 59% | 0.936 |
* Chi-squared test ^ 35% of this intervention firm used stickers in the second cycle.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Mettias, B.; Whittaker, J.D.; Ramakrishnan, Y. Real-Time Operative Coding for Endoscopic Sinonasal Procedures: Quality Improvement in Practice. Sinusitis 2021, 5, 32-44. https://0-doi-org.brum.beds.ac.uk/10.3390/sinusitis5010004
AMA Style
Mettias B, Whittaker JD, Ramakrishnan Y. Real-Time Operative Coding for Endoscopic Sinonasal Procedures: Quality Improvement in Practice. Sinusitis. 2021; 5(1):32-44. https://0-doi-org.brum.beds.ac.uk/10.3390/sinusitis5010004
Chicago/Turabian StyleMettias, Bassem, Joshua D. Whittaker, and Yujay Ramakrishnan. 2021. "Real-Time Operative Coding for Endoscopic Sinonasal Procedures: Quality Improvement in Practice" Sinusitis 5, no. 1: 32-44. https://0-doi-org.brum.beds.ac.uk/10.3390/sinusitis5010004