
Presentation of SARS-CoV-2 in a Pediatric Heart Transplant Recipient with Multiple Underlying Comorbidities


Department of Pediatric Cardiology, University of Mississippi Medical Center, Mississippi Children’s Hospital, 2500 North State Street, Jackson, MS 39211, USA
Transplantology 2021, 2(1), 87-91; https://0-doi-org.brum.beds.ac.uk/10.3390/transplantology2010009
Submission received: 15 February 2021
/
Revised: 24 February 2021
/
Accepted: 4 March 2021
/
Published: 22 March 2021
(This article belongs to the Special Issue Solid Organ Transplantation in the Era of COVID-19)
{kind=link}
{kind=link}
{kind=link}
Abstract
:A six-year-old heart transplant recipient with additional significant co-morbidities, including severe hypoxic-ischemic injury, gastrostomy, tracheostomy, and mechanical ventilation dependency, encountered SARS-CoV-2 infection. The patient received tacrolimus and mycophenolate to prevent graft rejection, presented initially with SARS-CoV-2 positive and presumed pseudomonas aeruginosa pneumonia. Twenty-three days later, the patient presented with fever recurrence with evidence for systemic inflammation, which resolved rapidly with high-dose methylprednisolone. Interestingly, while IgM to SARS-CoV-2 was present, IgG was not detected even three months after his first positive test for SARS-CoV-2. The author discusses potential immune mechanisms that might have affected the course of multi-system inflammatory syndrome children (MIS-C) in this patient.
1. Introduction
There is little data on clinical characteristics and outcomes with SARS-CoV-2 infection in children and adults with an immunocompromised status after heart transplantation [1,2,3,4,5]. Higher mortality was associated with COVID-19 in adult transplant recipients with right ventricular dysfunction, arrhythmias, thromboembolic events, and markedly elevated cardiac biomarkers [5]. It is not easy to extrapolate adult outcomes to pediatric heart transplant recipients because of higher comorbidities such as hypertension, obesity, and diabetes in adult patients. A six-year-old heart transplant recipient with additional significant co-morbidities, including severe hypoxic-ischemic injury, gastrostomy, tracheostomy, and mechanical ventilation dependency, presented with multi-system inflammatory syndrome children (MIS-C) with evidence for systemic inflammation and masquerade as acute cardiac allograft rejection that resolved rapidly with high-dose steroid tretament.
2. Case Report
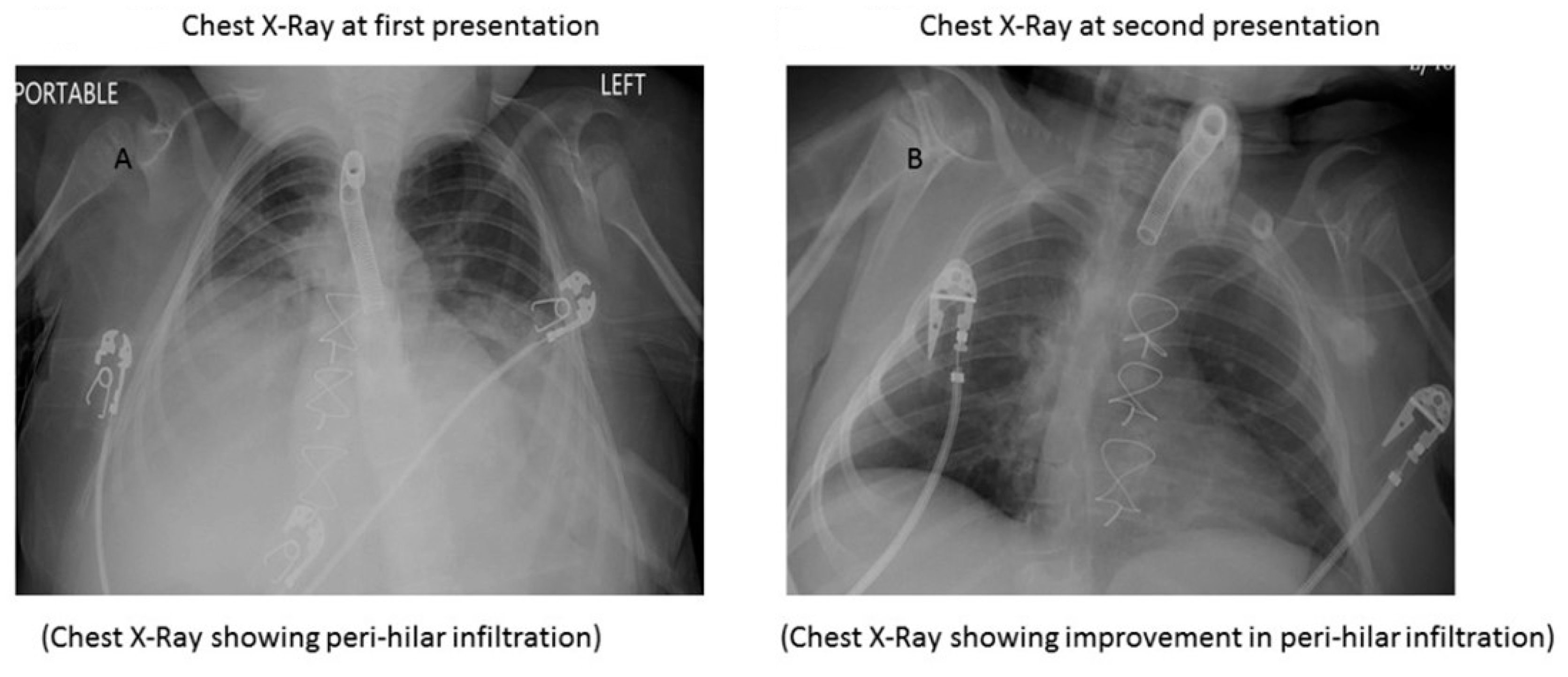
A six-year-old boy was diagnosed with left ventricular noncompaction cardiomyopathy with severe heart failure and underwent heart transplantation at nine months. His postoperative course was complicated by severe hypoxic-ischemic injury, gastrostomy, and tracheostomy, and he remained on mechanical ventilation. He had no clinical rejection evidence with maintenance immunosuppression (tacrolimus and mycophenolate sodium) and was doing well. He encountered SARS-CoV-2 infection and presented with fever and cyanosis. His chest-X ray (CXR) showed bilateral perihilar infiltrations (Figure 1A). Pseudomonas aeruginosa was isolated from tracheal aspirate and was sensitive to Imipenem, Amikacin, and Ofloxacin. The polymerase chain reaction for the viral respiratory panel was negative for other viral pathogens. His tracheal aspirate for aspergillus filament and pneumocystis carinii were negative. He was admitted to the hospital for supportive care and treated with intravenous Imipenem, and discharged home to complete a ten-day course with oral Ofloxacin. His father was also positive for SARS-CoV-2. Both were quarantined at home as per the center for disease control (CDC) guidelines. His father tested negative for SARS-CoV-2 after initial positive test subsequently, but the patient continued to be positive at three weeks.
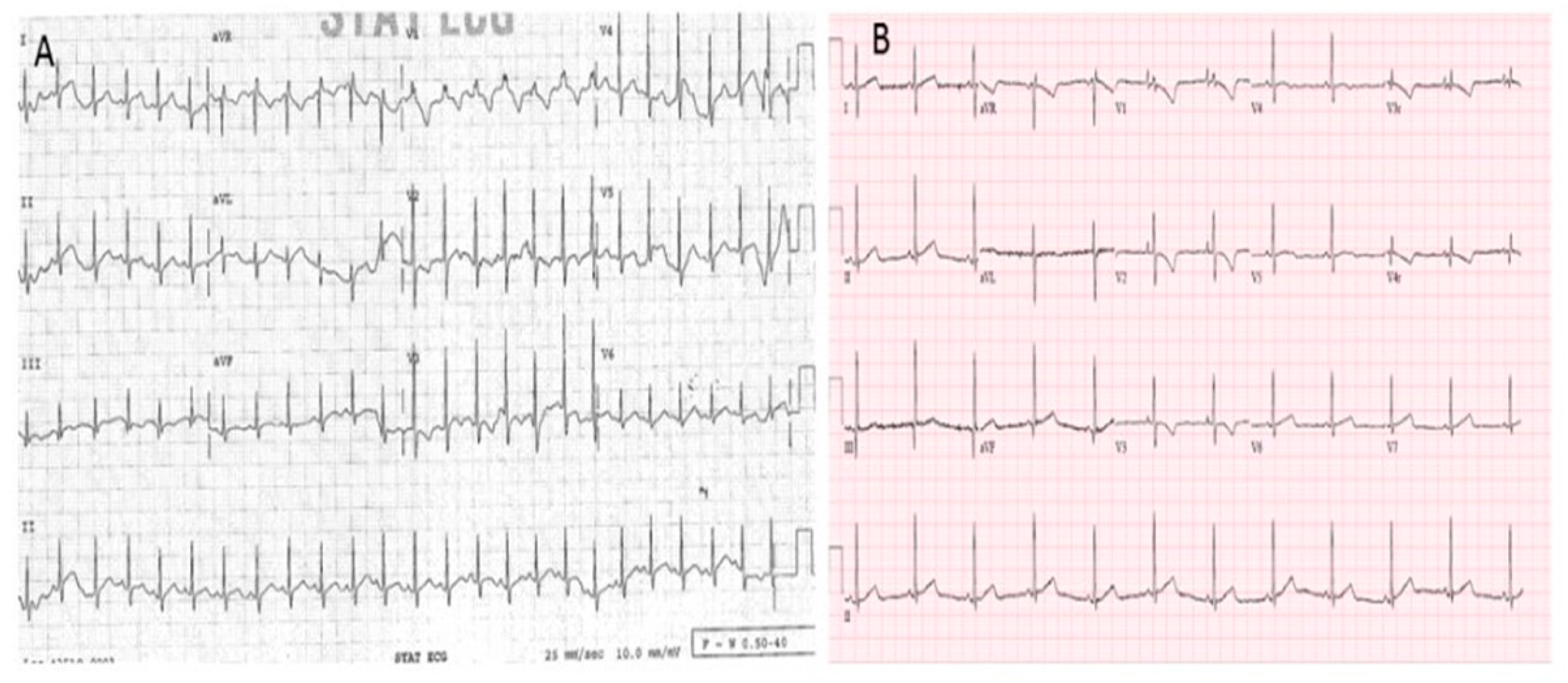
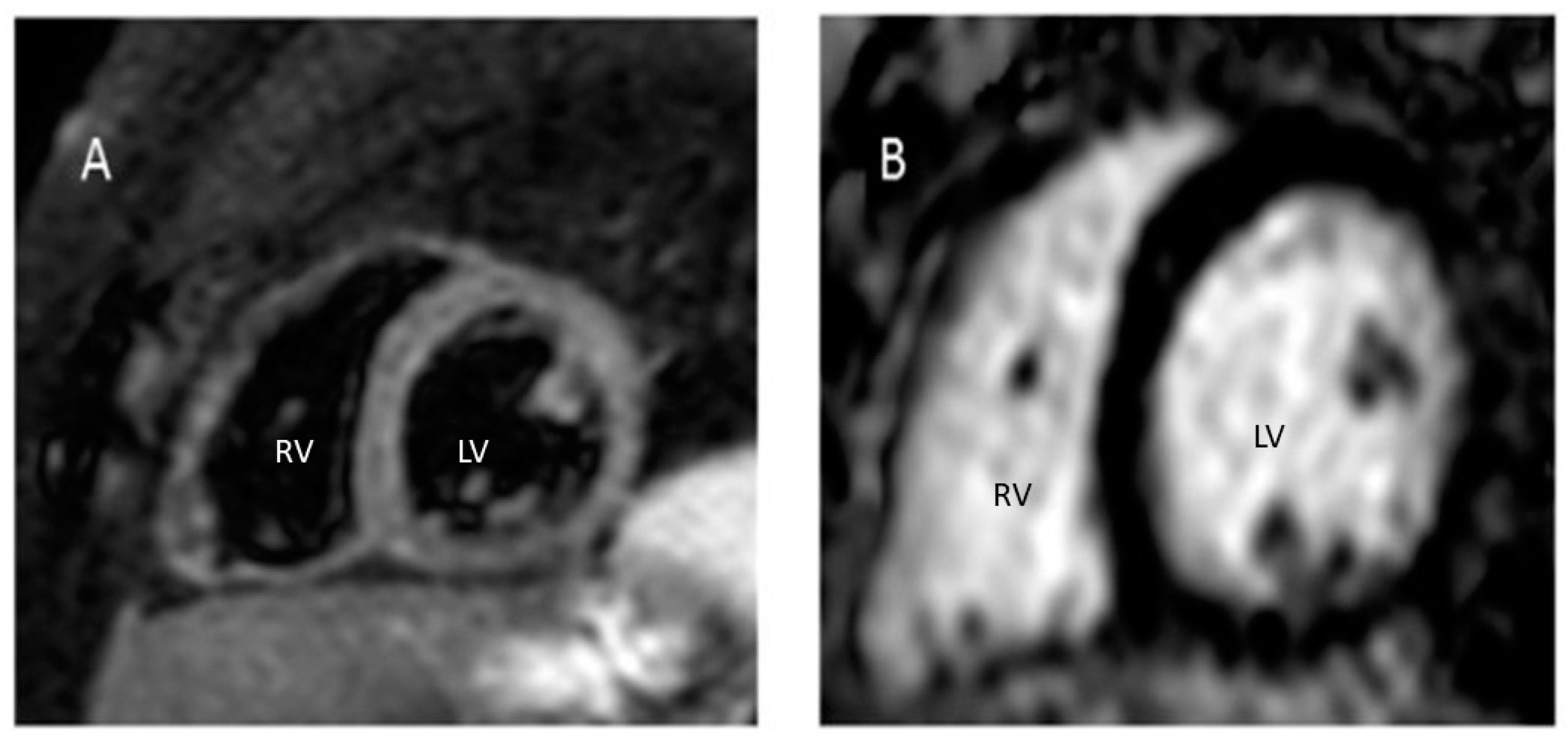
The patient had a fever (38.3 °C) recurrence 23 days after initial positive SARS-CoV-2 and presumed pseudomonas pneumonia. He was hemodynamically stable but noted to have tachycardia (180 beats/min), frequent premature ventricular contractions, cyanosis (oxygen saturation was in the 80 s) for which he was admitted to the cardiac intensive care unit. A repeat CXR (Figure 1B) showed improved lung infiltrations compared to the previous one (Figure 1A). His electrocardiogram showed sinus tachycardia, and non-specific ST changes (Figure 2A) compared to his baseline (Figure 2B). His laboratory tests revealed a white blood cell count of 2.8 × 109/L, hemoglobin 10.5 g/L, platelets 161 × 109/L, and 23% of lymphocytes on the differential count. A complete metabolic panel showed no end-organ damage with normal creatinine and liver enzymes. His C-reactive protein was 88.45 mg/L (<10.01 mg/L), erythrocyte sedimentation rate 88 mm/h (2–34 mm/h), pro-calcitonin 1.5 ng/L (<0.05 ng/L), sedimentation rate 88 mm/h (2–34 mm/h), ferritin 35 ng/mL (22–322 ng/mL), brain natriuretic peptide 4218 pg/mL (0–124 pg/Ml), and troponin 1.2 ng/mL (<0.1 ng/mL). His echocardiogram showed normal biventricular systolic function and normal coronaries. His repeat blood, endotracheal aspirate, and urine cultures were negative. His repeat tracheal swab was negative for adenovirus, metapneumovirus, enterovirus, influenza A and B virus, parainfluenza type1-4 virus, bordetella pertussis, parapertusis, chlamydia, and mycoplasma. The differential diagnoses were presumed SARS-CoV-2 myocarditis or acute cardiac allograft rejection. He was treated with intravenous methylprednisolone 10 mg/kg/dose twice daily for three days. After starting the steroid, within 48 h, his heart rate returned to its baseline (60 s–70 s/min), and his inflammatory markers decreased significantly (erythrocyte sedimentation rate 32 mm/h, C-reactive protein 19 mg/L, and procalcitonin 0.07 ng/mL). His daily troponin trended downward, and at the end of the third day of the steroid pulse, troponin was 0.05 ng/mL, and brain natriuretic peptide was 52 pg/mL. His repeat echocardiogram showed no change in function. No changes to his immunosuppression regimen were made. His tacrolimus trough level was 4.8 ng/mL. He was discharged home four days after hospitalization on his home immunosuppression regimens and oral prednisone, which was tapered over two weeks and stopped. On follow-up after two weeks, he was doing well without recurrence of fever or tachycardia, and inflammatory markers and troponin were normal. His repeat tests for SARS-CoV-2 were positive at six weeks and then three months from his initial positivity. His CD4, CD8, CD3, CD19 cell counts, CD4:CD8 ratio, and immunoglobulin levels were within the normal limit. His serology returned positive for SARS-CoV-2 IgM, but IgG was negative three months from his first positive test for SARS-CoV-2. He became finally SARS-CoV-2 negative four months after his initial positive test and underwent cardiac magnetic resonance (CMR) imaging as a part of surveillance that showed no myocardial edema, myocardial perfusion defects, or regional wall motion abnormalities at rest (Figure 3A). There was no evidence of delayed enhancement to suggest myocardial fibrosis or scarring (Figure 3B).
3. Discussion
The patient described in this report satisfies multi-system inflammatory syndrome children (MIS-C) diagnosis criteria as defined by the CDC [6] with a history of SARS-CoV-2 infection recently, fever for more than 24 h, cardiac arrhythmia, and hypoxemia. This case is interesting because of the dilemma of whether this is a presentation of MIS-C or acute cardiac allograft rejection. Myocarditis appears less likely given the cardiac function is normal by echocardiogram. The intriguing part is that the full clinical manifestation of MIS-C can be masked while on immunosuppression [7] due to its presumed pathomechanism of hyperimmune response. This case probably proves the hypothesis that MIS-C represents a continuum of phenotypic severity from mild organ involvement to severe life-threatening complications such as cardiogenic shock. He responded dramatically to high-dose steroids despite the severe neurological injury, tracheostomy, and mechanical ventilation dependency. The diagnosis is unlikely to be myocarditis as the response to steroids is usually not as dramatic in the case of myocarditis as in this case. In addition, the dramatic improvement in inflammatory biomarkers following intravenous steroid reinforces the diagnosis of MIS-C.
The clinical presentation after SARS-CoV-2 depends upon the immune response of the host. Whether immunosuppression alters the predisposition to acquiring infection with SARS-CoV-2 or if the disease implications are modified for better or worse remains uncertain. The SARS-CoV-2 virus hijacks the host cell machinery and can translate its proteins facilitating viral replication—the viral proteins and RNA released to lead to an interferon-dependent viral response. The unbalanced and excessive pro-inflammatory response can lead to MIS-C. On the other hand, an effective immune response to the Spike protein of SARS-CoV-2 helps contain the viral illness. Due to immunosuppressive treatment, transplant recipients are expected to be particularly susceptible to infection and a severe clinical COVID-19. Treatment of other viral infections in transplant patients often includes a reduction in immunosuppression. However, no current guidelines recommend the optimal approach to managing the treatment of SARS-CoV-2 infection. The case reports and small case series [1,2,3,4,5,7,8] published that have shown that the maintenance immunosuppression regimen is continued in these patients if COVID-19 is mild or asymptomatic. However, in renal transplantation patients, a steroid-sparing immunosuppression regimen is favored [9]. The immunosuppression medications may contribute to possible prolonged infectivity [8]. In this patient, his serological response to SARS-CoV-2 returned with no IgG response but IgM positive, and he remained positive for SARS-CoV-2 for three months. A normal serologic response (IgG positive) in adult solid organ transplant recipients with COVID-19 has been reported previously [10]. Given a lack of clear evidence on the immunological response to SARS-CoV-2 in the immunocompromised patient, the serological finding, as in this case, has implications for vaccine usefulness. It is unclear if immunocompromised patients will generate the intended immune response and need further study.
The case emphasizes the need to collect information further and study the impact of SARS-CoV-2 in different populations. It also demonstrates the potential clinical similarities between MIS-C and acute cardiac allograft rejection in a pediatric heart transplant recipient.
Funding
This research received no external funding. The author has no financial relationship with any commercial entity to disclose.
Institutional Review Board Statement
Not applicable. Our IRB allow a single case report.
Informed Consent Statement
Informed consent is obtained from patient’s father.
Data Availability Statement
Data sharing is not applicable.
Conflicts of Interest
The author has no conflict of interest to disclose.
References
- Latif, F.; Farr, M.A.; Clerkin, K.J.; Habal, M.V.; Takeda, K.; Naka, Y.; Restaino, S.; Sayer, G.; Uriel, N. Characteristics and Outcomes of Recipients of Heart Transplant With Coronavirus Disease 2019. JAMA Cardiol. 2020, 5, 1165–1169. [Google Scholar] [CrossRef] [PubMed]
- Lima, B.; Gibson, G.T.; Vullaganti, S.; Malhame, K.; Maybaum, S.; Hussain, S.T.; Shah, S.; Majure, D.T.; Wallach, F.; Jang, K.; et al. COVID-19 in recent heart transplant recipients: Clinicopathologic features and early outcomes. Transpl. Infect. Dis. 2020, 22, e13382. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Mantell, B.S.; Richmond, M.E.; Law, S.P.; Zuckerman, W.A.; Addonizio, L.J.; Lee, T.M.; Lytrivi, I.D. Varying presentations of COVID-19 in young heart transplant recipients: A case series. Pediatr. Transplant. 2020, 24, e13780. [Google Scholar] [CrossRef] [PubMed]
- Ketcham, S.W.; Adie, S.K.; Malliett, A.; Abdul-Aziz, A.A.; Bitar, A.; Grafton, G.; Konerman, M.C. Coronavirus disease-2019 in heart transplant recipients in Southeastern Michigan: A case series: COVID-19 in patients with heart transplant. J. Card. Fail. 2020, 26, 457–461. [Google Scholar] [CrossRef] [PubMed]
- Rivinius, R.; Kaya, Z.; Schramm, R.; Boeken, U.; Provaznik, Z.; Heim, C.; Knosalla, C.; Schoenrath, F.; Rieth, A.; Berchtold-Herz, M.; et al. COVID-19 among heart transplant recipients in Germany: A multicenter survey. Clin. Res. Cardiol. 2020, 109, 1531–1539. [Google Scholar] [CrossRef] [PubMed]
- CDC. Multi-System Inflammatory Syndrome in Children (MIS-C) Associated with Coronavirus Disease 2019 (COVID-19). Available online: https://emergency.cdc.gov/han/2020/han00432.asp (accessed on 24 February 2021).
- Bösch, F.; Börner, N.; Kemmner, S.; Lampert, C.; Jacob, S.; Koliogiannis, D.; Stangl, M.; Michel, S.; Kneidinger, N.; Schneider, C.; et al. Attenuated early inflammatory response in solid organ recipients with COVID-19. Clin. Transplant. 2020, 34, e14027. [Google Scholar] [CrossRef] [PubMed]
- Decker, A.; Welzel, M.; Laubner, K.; Grundmann, S.; Kochs, G.; Panning, M.; Thimme, R.; Bode, C.; Wagner, D.; Lother, A. Prolonged SARS-COV-2 shedding and mild course of COVID-19 in a patient after recent heart transplantation. Am. J. Transpl. 2020, 20, 3239–3245. [Google Scholar] [CrossRef] [PubMed]
- Johnson, K.M.; Belfer, J.J.; Peterson, G.R.; Boelkins, M.R.; Dumkow, L.E. Managing COVID-19 in Renal Transplant Recipients: A Review of Recent Literature and Case Supporting Corticosteroid-sparing Immunosuppression. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2020, 40, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Fung, M.; Chiu, C.Y.; DeVoe, C.; Doernberg, S.B.; Schwartz, B.S.; Langelier, C.; Henrich, T.J.; Yokoe, D.; Davis, J.; Hays, S.R.; et al. Clinical outcomes and serologic response in solid organ transplant recipients with COVID-19: A case series from the United States. Arab. Archaeol. Epigr. 2020, 20, 3225–3233. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
(A): Chest X-Ray (CXR): (Initial presentation) Perihilar infiltrates (Expiratory film) vs. (B): Second CXR with improvement in infiltrations.
Figure 1.
(A): Chest X-Ray (CXR): (Initial presentation) Perihilar infiltrates (Expiratory film) vs. (B): Second CXR with improvement in infiltrations.

Figure 2.
(A): A 12-lead ECG showing sinus tachycardia (150 bpm) and non-specific ST changes vs. baseline ECG (B): sinus rhythm with heart rate 70 bpm.
Figure 2.
(A): A 12-lead ECG showing sinus tachycardia (150 bpm) and non-specific ST changes vs. baseline ECG (B): sinus rhythm with heart rate 70 bpm.

Figure 3.
Short-axis T2-weighted image through the left ventricle base showing no early (A) or late-gadolinium enhancement (B).
Figure 3.
Short-axis T2-weighted image through the left ventricle base showing no early (A) or late-gadolinium enhancement (B).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Das, B.B. Presentation of SARS-CoV-2 in a Pediatric Heart Transplant Recipient with Multiple Underlying Comorbidities. Transplantology 2021, 2, 87-91. https://0-doi-org.brum.beds.ac.uk/10.3390/transplantology2010009
AMA Style
Das BB. Presentation of SARS-CoV-2 in a Pediatric Heart Transplant Recipient with Multiple Underlying Comorbidities. Transplantology. 2021; 2(1):87-91. https://0-doi-org.brum.beds.ac.uk/10.3390/transplantology2010009
Chicago/Turabian StyleDas, Bibhuti B. 2021. "Presentation of SARS-CoV-2 in a Pediatric Heart Transplant Recipient with Multiple Underlying Comorbidities" Transplantology 2, no. 1: 87-91. https://0-doi-org.brum.beds.ac.uk/10.3390/transplantology2010009