
Influence of Menstrual Cycle or Hormonal Contraceptive Phase on Energy Intake and Metabolic Hormones—A Pilot Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Body Composition
2.4. Nutrition, Energy Intake, and Energy Availability
2.5. Venous Blood Samples
2.6. Statistical Analyses
3. Results
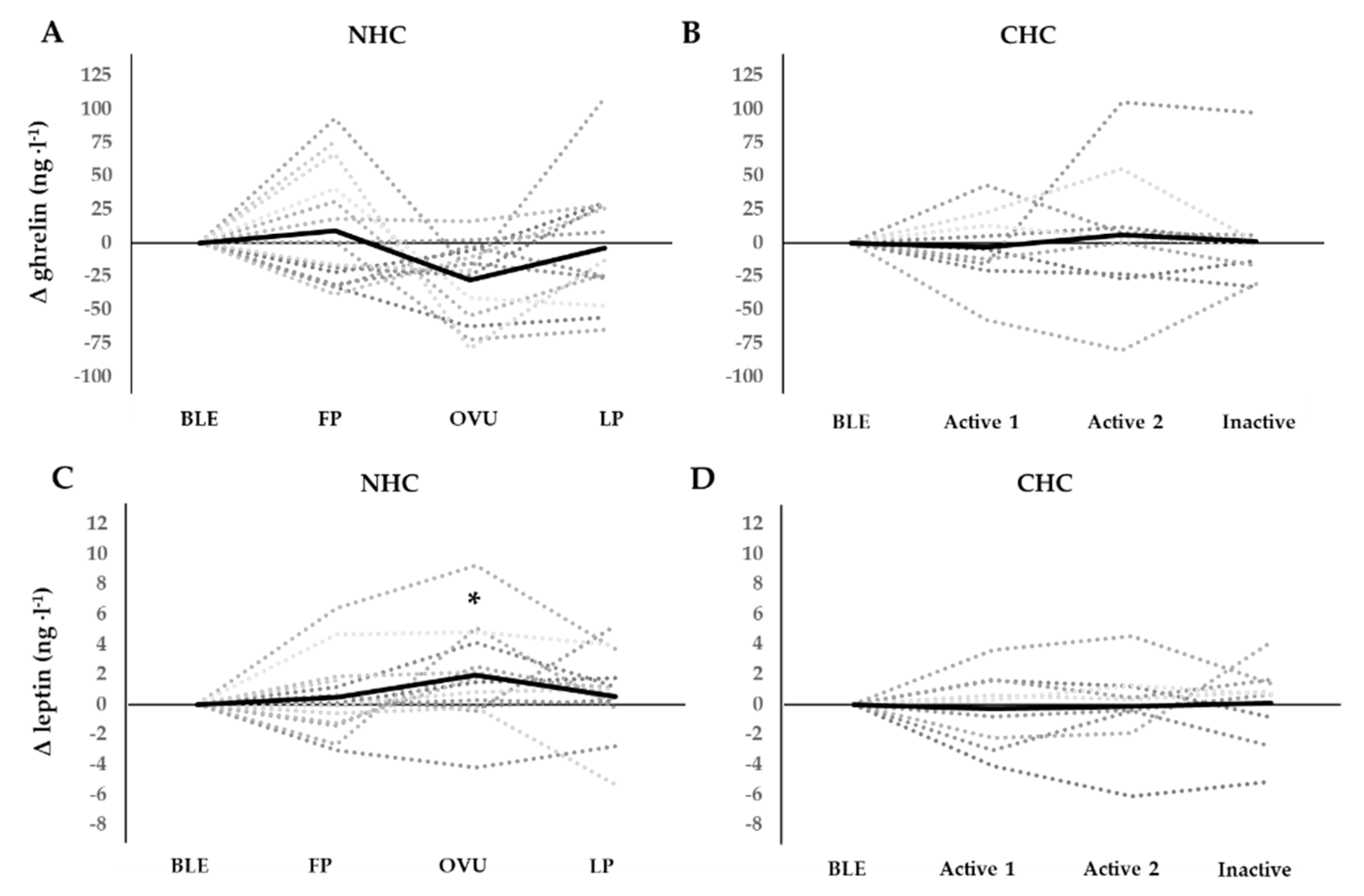
3.1. Hormonal Fluctuations
3.2. Nutritional Intake and Energy Avalability
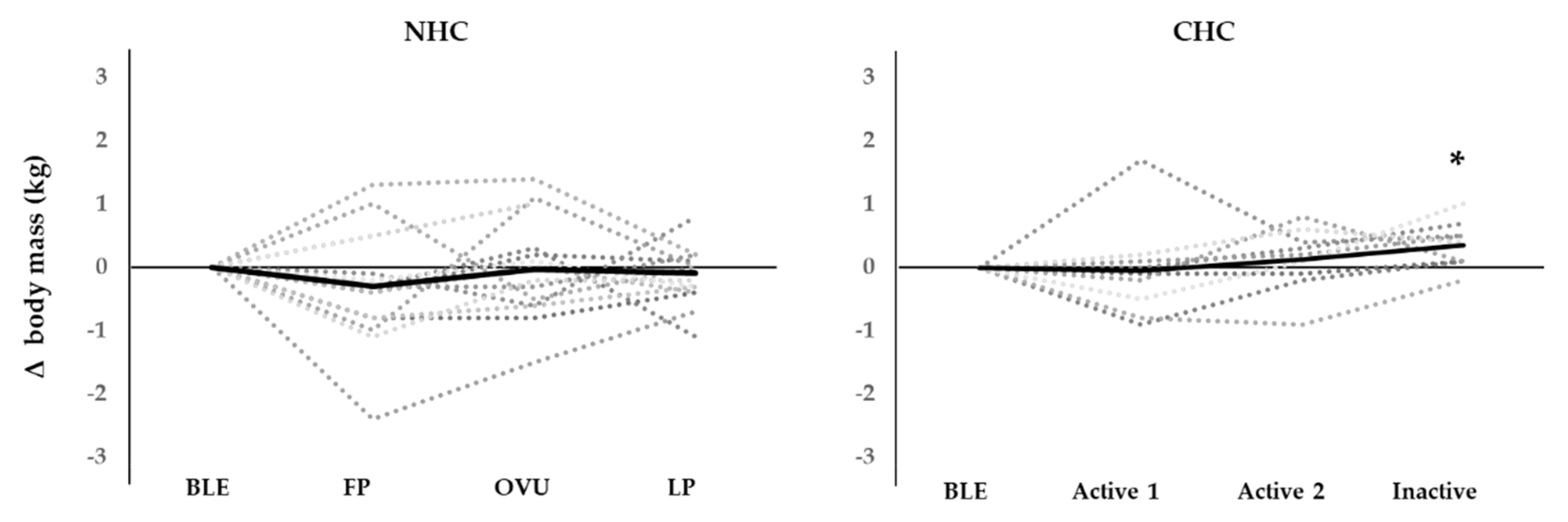
3.3. Body Mass and Cravings
3.4. Associations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fehring, R.J.; Schneider, M.; Raviele, K. Variability in the phases of the menstrual cycle. JOGNN-J. Obstet. Gynecol. Neonatal Nurs. 2006, 35, 376–384. [Google Scholar] [CrossRef] [Green Version]
- Hirschberg, A.L. Sex hormones, appetite and eating behaviour in women. Maturitas 2012, 71, 248–256. [Google Scholar] [CrossRef] [PubMed]
- Elliott-Sale, K.J.; Hicks, K.M. Hormonal-based contraception and the exercising female. In The Exercising Female; Routledge: London, UK, 2018; pp. 30–43. Available online: https://www.taylorfrancis.com/chapters/hormonal-based-contraception-exercising-female-kirsty-elliott-sale-kirsty-marie-hicks/e/10.4324/9781351200271-4 (accessed on 12 March 2021).
- Eck, L.H.; Bennett, A.G.; Egan, B.M.; Ray, J.W.; Mitchell, C.O.; Smith, M.A.; Klesges, R.C. Differences in macronutrient selections in users and nonusers of an oral contraceptive. Am. J. Clin. Nutr. 1997, 65, 419–424. Available online: https://0-academic-oup-com.brum.beds.ac.uk/ajcn/article/65/2/419-424/4655349 (accessed on 12 March 2021). [CrossRef] [PubMed]
- Wallace, R.B.; Heiss, G.; Burrows, B.; Graves, K. Contrasting diet and body mass among users and nonusers of oral contraceptives and exogenous estrogens: The lipid research clinics program prevalence study. Am. J. Epidemiol. 1987, 125, 854–859. Available online: https://0-academic-oup-com.brum.beds.ac.uk/aje/article/124178/CONTRASTING (accessed on 12 March 2021). [CrossRef] [PubMed]
- Procter-Gray, E.; Cobb, K.L.; Crawford, S.L.; Bachrach, L.K.; Chirra, A.; Sowers, M.; Greendale, G.A.; Nieves, J.W.; Kent, K.; Kelsey, J.L. Effect of Oral Contraceptives on Weight and Body Composition in Young Female Runners. Med. Sci. Sports Exerc. 2008, 40, 1205–1212. Available online: https://journals.lww.com/00005768-200807000-00002 (accessed on 12 March 2021). [CrossRef]
- Landersoe, S.K.; Forman, J.L.; Petersen, K.B.; Larsen, E.C.; Nøhr, B.; Hvidman, H.W.; Nielsen, H.S.; Andersen, A.N. Ovarian reserve markers in women using various hormonal contraceptives. Eur. J. Contracept. Reprod. Heal. Care 2020, 25, 65–71. [Google Scholar] [CrossRef]
- Cummings, D.E.; Purnell, J.Q.; Frayo, R.S.; Schmidova, K.; Wisse, B.E.; Weigle, D.S. A Preprandial Rise in Plasma Ghrelin Levels Suggests a Role in Meal Initiation in Humans. Diabetes 2001, 50, 1714–1719. Available online: www.diabetes.org/diabetes (accessed on 12 March 2021). [CrossRef] [Green Version]
- Klok, M.D.; Jakobsdottir, S.; Drent, M.L. The role of leptin and ghrelin in the regulation of food intake and body weight in humans: A review. Obes. Rev. 2007, 8, 21–34. [Google Scholar] [CrossRef]
- Ahrens, K.; Mumford, S.L.; Schliep, K.C.; Kissell, K.A.; Perkins, N.J.; Wactawski-Wende, J.; Schisterman, E.F. Serum leptin levels and reproductive function during the menstrual cycle. In American Journal of Obstetrics and Gynecology; Mosby Inc.: St. Louis, MO, USA, 2014; Volume 210, pp. 248.e1–248.e9. [Google Scholar]
- Rafique, N.; Salem, A.M.; Latif, R.; ALSheikh, M.H. Serum leptin level across different phases of menstrual cycle in normal weight and overweight/obese females. Gynecol. Endocrinol. 2018, 34, 601–604. [Google Scholar] [CrossRef]
- Krishnan, S.; Tryon, R.R.; Horn, W.F.; Welch, L.; Keim, N.L. Estradiol, SHBG and leptin interplay with food craving and intake across the menstrual cycle. Physiol. Behav. 2016, 165, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Riad-Gabriel, M.G.; Jinagouda, S.D.; Sharma, A.; Boyadjian, R.; Saad, M.F. Changes in plasma leptin during the menstrual cycle. Eur. J. Endocrinol. 1998, 139, 528–531. Available online: https://pubmed.ncbi.nlm.nih.gov/9849818/ (accessed on 12 March 2021). [CrossRef] [PubMed] [Green Version]
- Matson, C.A.; Wiater, M.F.; Kuijper, J.L.; Weigle, D.S. Synergy between leptin and cholecystokinin (CCK) to control daily caloric intake. Peptides 1997, 18, 1275–1278. [Google Scholar] [CrossRef]
- Dafopoulos, K.; Sourlas, D.; Kallitsaris, A.; Pournaras, S.; Messinis, I.E. Blood ghrelin, resistin, and adiponectin concentrations during the normal menstrual cycle. Fertil. Steril. 2009, 92, 1389–1394. Available online: https://pubmed.ncbi.nlm.nih.gov/18829017/ (accessed on 12 March 2021). [CrossRef] [PubMed]
- St-Pierre, D.H.; Karelis, A.D.; Cianflone, K.; Conus, F.; Mignault, D.; Rabasa-Lhoret, R.; St-Onge, M.; Tremblay-Lebeau, A.; Poehlman, E.T. Relationship between Ghrelin and Energy Expenditure in Healthy Young Women. J. Clin. Endocrinol. Metab. 2004, 89, 5993–5997. Available online: https://0-academic-oup-com.brum.beds.ac.uk/jcem/article/89/12/5993/2844263 (accessed on 12 March 2021). [CrossRef] [PubMed] [Green Version]
- Loucks, A.B.; Kiens, B.; Wright, H.H. Energy availability in athletes. J. Sports Sci. 2011, 29 (Suppl. S1), S7–S15. [Google Scholar] [CrossRef] [PubMed]
- Logue, D.; Madigan, S.M.; Delahunt, E.; Heinen, M.; Mc Donnell, S.J.; Corish, C.A. Low Energy Availability in Athletes: A Review of Prevalence, Dietary Patterns, Physiological Health, and Sports Performance. Sports Med. 2018, 48, 73–96. [Google Scholar] [CrossRef]
- Koehler, K.; Williams, N.I.; Mallinson, R.J.; Southmayd, E.A.; Allaway, H.C.M.; De Souza, M.J. Low resting metabolic rate in exercise-associated amenorrhea is not due to a reduced proportion of highly active metabolic tissue compartments. Am. J. Physiol. Metab. 2016, 311, E480–E487. [Google Scholar] [CrossRef]
- Melin, A.; Tornberg, Å.B.; Skouby, S.; Faber, J.; Ritz, C.; Sjödin, A.; Sundgot-Borgen, J. The LEAF questionnaire: A screening tool for the identification of female athletes at risk for the female athlete triad. Br. J. Sports Med. 2014, 48, 540–545. Available online: http://0-bjsm-bmj-com.brum.beds.ac.uk/ (accessed on 12 March 2021). [CrossRef]
- Elliott-Sale, K.J.; Ross, E.; Burden, R.; Hicks, K. The BASES Expert Statement on Conducting and Implementing Female Athlete-Based Research. Sport Exerc. Sci. 2020, 65, 6–7. [Google Scholar]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 compendium of physical activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. Available online: https://pubmed.ncbi.nlm.nih.gov/21681120/ (accessed on 12 March 2021). [CrossRef] [Green Version]
- Hardie, L.; Trayhurn, P.; Abramovich, D.; Fowler, P. Circulating leptin in women: A longitudinal study in the menstrual cycle and during pregnancy. Clin. Endocrinol. 1997, 47, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Ajala, O.M.; Ogunro, P.S.; Elusanmi, G.F.; Ogunyemi, O.E.; Bolarinde, A.A. Changes in serum leptin during phases of menstrual cycle of fertile women: Relationship to age groups and fertility. Int. J. Endocrinol. Metab. 2013, 11, 27–33. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC3693651/ (accessed on 12 March 2021). [CrossRef] [PubMed] [Green Version]
- Wunder, D.M.; Yared, M.; Bersinger, N.A.; Widmer, D.; Kretschmer, R.; Birkhäuser, M.H. Serum leptin and C-reactive protein levels in the physiological spontaneous menstrual cycle in reproductive age women. Eur. J. Endocrinol. 2006, 155, 137–142. Available online: www.eje-online.org (accessed on 12 March 2021). [CrossRef] [PubMed]
- Teirmaa, T.; Luukkaa, V.; Rouru, J.; Koulu, M.; Huupponen, R. Correlation between circulating leptin and luteinizing hormone during the menstrual cycle in normal-weight women. Eur. J. Endocrinol. 1998, 139, 190–194. [Google Scholar] [CrossRef] [Green Version]
- Lin, K.C. Changes of circulating leptin levels during normal menstrual cycle: Relationship to estradiol and progesterone. Kaohsiung J. Med. Sci. 1999, 15, 597–602. Available online: https://europepmc.org/article/med/10603707 (accessed on 12 March 2021).
- Stock, S.M.; Sande, E.M.; Bremme, K.A. Leptin levels vary significantly during the menstrual cycle, pregnancy, and in vitro fertilization treatment: Possible relation to estradiol. Fertil. Steril. 1999, 72, 657–662. [Google Scholar] [CrossRef]
- Hausman, G.J.; Barb, C.R.; Lents, C.A. Leptin and reproductive function. Biochimie 2012, 94, 2075–2081. [Google Scholar] [CrossRef]
- Šrámková, M.; Dušková, M.; Vítků, J.; Vçelák, J.; Matucha, P.; Bradnová, O.; De Cordeiro, J.; Stárka, L. Levels of adipokines and some steroids during the menstrual cycle. Physiol. Res. 2015, 64, S147–S154. Available online: https://pubmed.ncbi.nlm.nih.gov/26680475/ (accessed on 12 March 2021). [CrossRef]
- Saǧsöz, N.; Orbak, Z.; Noyan, V.; Yücel, A.; Uçar, B.; Yildiz, L. The effects of oral contraceptives including low-dose estrogen and drospirenone on the concentration of leptin and ghrelin in polycystic ovary syndrome. Fertil. Steril. 2009, 92, 660–666. Available online: https://pubmed.ncbi.nlm.nih.gov/18973889/ (accessed on 12 March 2021). [CrossRef]
- Kellokoski, E.; Pöykkö, S.M.; Karjalainen, A.H.; Ukkola, O.; Heikkinen, J.; Kesäniemi, Y.A.; Hörkkö, S. Estrogen Replacement Therapy Increases Plasma Ghrelin Levels. J. Clin. Endocrinol. Metab. 2005, 90, 2954–2963. Available online: https://0-academic-oup-com.brum.beds.ac.uk/jcem/article/90/5/2954/2836983 (accessed on 12 March 2021). [CrossRef]
- Dafopoulos, K.; Chalvatzas, N.; Kosmas, G.; Kallitsaris, A.; Pournaras, S.; Messinis, I.E. The effect of estrogens on plasma ghrelin concentrations in women. J. Endocrinol. Invest. 2010, 33, 109–112. Available online: https://pubmed.ncbi.nlm.nih.gov/20348837/ (accessed on 12 March 2021). [CrossRef]
- Gortan Cappellari, G.; Barazzoni, R. Ghrelin forms in the modulation of energy balance and metabolism. Eat. Weight Disord. 2019, 24, 997–1013. Available online: https://0-doi-org.brum.beds.ac.uk/10.1007/s40519-018-0599-6 (accessed on 12 March 2021). [CrossRef] [PubMed]
- Hackney, A.C.; Cyren, H.C.; Brammeier, M.; Sharp, R.L. Effects of the menstrual cycle on insulin-glucose at rest and in response to exercise. Biol. Sport 1993, 10, 73–81. [Google Scholar]
- Yeung, E.H.; Zhang, C.; Mumford, S.L.; Ye, A.; Trevisan, M.; Chen, L.; Browne, R.W.; Wactawski-Wende, J.; Schisterman, E.F. Longitudinal Study of Insulin Resistance and Sex Hormones over the Menstrual Cycle: The BioCycle Study. J. Clin. Endocrinol. Metab. 2010, 95, 5435–5442. Available online: https://academic.oup.com/jcem/article-lookup/doi/10.1210/jc.2010-0702 (accessed on 12 March 2021). [CrossRef] [PubMed] [Green Version]
- Loucks, A.B.; Heath, E.M. Induction of low-T3 syndrome in exercising women occurs at a threshold of energy availability. Am. J. Physiol. Regul. Integr. Comp. Physiol. 1994, 266, R817–R823. Available online: https://0-journals-physiology-org.brum.beds.ac.uk/doi/abs/10.1152/ajpregu.1994.266.3.R817 (accessed on 12 March 2021). [CrossRef] [PubMed]
- Wiegratz, I.; Kutschera, E.; Lee, J.H.; Moore, C.; Mellinger, U.; Winkler, U.H.; Kuhl, H. Effect of four different oral contraceptives on various sex hormones and serum-binding globulins. Contraception 2003, 67, 25–32. Available online: http://0-www-sciencedirect-com.brum.beds.ac.uk/science/article/pii/S0010782402004365 (accessed on 12 March 2021). [CrossRef]
- Dipla, K.; Kraemer, R.R.; Constantini, N.W.; Hackney, A.C. Relative energy deficiency in sports (RED-S): Elucidation of endocrine changes affecting the health of males and females. Hormones 2020, 20, 35–47. Available online: https://0-doi-org.brum.beds.ac.uk/10.1007/s42000-020-00214-w (accessed on 12 March 2021). [CrossRef]
- Elliott-Sale, K.J.; Tenforde, A.S.; Parziale, A.L.; Holtzman, B.; Ackerman, K.E. Endocrine Effects of Relative Energy Deficiency in Sport. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 335–349. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/30008240 (accessed on 12 March 2021). [CrossRef]
- Vaiksaar, S.; Jurimae, J.; Maestu, J.; Purge, P.; Kalytka, S.; Shakhlina, L.; Jurimae, T. No effect of menstrual cycle phase on fuel oxidation during exercise in rowers. Eur. J. Appl. Physiol. 2011, 111, 1027–1034. [Google Scholar] [CrossRef]
- Rael, B.; Romero-Parra, N.; Alfaro-Magallanes, V.M.; Barba-Moreno, L.; Cupeiro, R.; Janse de Jonge, X.; Peinado, A.B. Body Composition Over the Menstrual and Oral Contraceptive Cycle in Trained Females. Int. J. Sports Physiol. Perform. 2020, 16, 1–7. Available online: http://0-journals-humankinetics-com.brum.beds.ac.uk/view/journals/ijspp/16/3/article-p375.xml (accessed on 12 March 2021).
- Lebrun, C.M. Effect of the Different Phases of the Menstrual Cycle and Oral Contraceptives on Athletic Performance. Sport. Med. Eval. Res. Exerc. Sci. Sport. Med. 1993, 16, 400–430. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/8303141 (accessed on 12 March 2021). [CrossRef]
- Tsampoukos, A.; Peckham, E.A.; James, R.; Nevill, M.E. Effect of menstrual cycle phase on sprinting performance. Eur. J. Appl. Physiol. 2010, 109, 659–667. Available online: https://0-link-springer-com.brum.beds.ac.uk/article/10.1007/s00421-010-1384-z (accessed on 12 March 2021). [CrossRef] [PubMed]
- Reilly, T. The menstrual cycle and human performance: An overview. Biol. Rhythm Res. 2000, 31, 29–40. [Google Scholar] [CrossRef]
- Pliner, P.; Fleming, A.S. Food intake, body weight, and sweetness preferences over the menstrual cycle in humans. Physiol. Behav. 1983, 30, 663–666. [Google Scholar] [CrossRef]
- Carmichael, M.A.; Thomson, R.L.; Moran, L.J.; Wycherley, T.P. The Impact of Menstrual Cycle Phase on Athletes’ Performance: A Narrative Review. Int. J. Environ. Res. Public Health 2021, 18, 1667. Available online: https://www.mdpi.com/1660-4601/18/4/1667 (accessed on 12 March 2021). [CrossRef]
- Davidsen, L.; Vistisen, B.; Astrup, A. Impact of the menstrual cycle on determinants of energy balance: A putative role in weight loss attempts. Int. J. Obes. 2007, 31, 1777–1785. Available online: www.gw.cs.nsw.gov.au/csls/RPAH/ (accessed on 12 March 2021). [CrossRef] [Green Version]
- Tucci, S.A.; Murphy, L.E.; Boyland, E.J.; Dye, L.; Halford, J.C.G. Oral contraceptive effects on food choice during the follicular and luteal phases of the menstrual cycle. A laboratory based study. Appetite 2010, 55, 388–392. [Google Scholar] [CrossRef]
- Kipnis, V.; Midthune, D.; Freedman, L.; Bingham, S.; Day, N.E.; Riboli, E.; Ferrari, P.; Carroll, R.J. Bias in dietary-report instruments and its implications for nutritional epidemiology. Public Health Nutr. 2002, 5, 915–923. Available online: https://0-www-cambridge-org.brum.beds.ac.uk/core (accessed on 12 March 2021). [CrossRef] [Green Version]
- Asbeck, I.; Mast, M.; Bierwag, A.; Westenhöfer, J.; Acheson, K.; Müller, M. Severe underreporting of energy intake in normal weight subjects: Use of an appropriate standard and relation to restrained eating. Public Health Nutr. 2002, 5, 683–690. Available online: https://0-www-cambridge-org.brum.beds.ac.uk/core (accessed on 12 March 2021). [CrossRef]



{kind=link}
{kind=link}
| NHC (n = 15) | CHC (n = 9) | |
|---|---|---|
| Age (years) | 26 ± 4 | 23 ± 2 |
| Body mass (kg) | 67.6 ± 6.5 | 61.0 ± 4.3 |
| Height (m) | 1.67 ± 0.06 | 1.70 ± 0.06 |
| Body fat (%) | 22.1 ± 6.7 | 19.5 ± 2.8 |
| LEAF-Q (score) | 4.5 ± 2.1 | 5.7 ± 1.8 |
| Group | BLE | FP/Active1 | OVU/Active2 | LP/Inactive | Phase | |
|---|---|---|---|---|---|---|
| E2 (pmol·L−1) | NHC | 290 ± 140 | 560 ± 390 ** | 690 ± 500 ** | 650 ± 240 ** | p < 0.001 |
| CHC | 300 ± 270 | 190 ± 140 aa | 220 ± 230 aa | 190 ± 110 aaa | p = 0.435 | |
| P4 (nmol·L−1) | NHC | 2.0 ± 1.7 | 1.0 ± 0.5 | 4.1 ± 2.7 *,++ | 15.0 ± 8.9 **,++,## | p = 0.001 |
| CHC | 1.1 ± 0.5 | 1.0 ± 0.5 | 1.1 ± 1.0 a | 1.2 ± 1.0 aa | p = 0.239 | |
| Leptin (ng·L−1) | NHC | 6.8 ± 4.0 | 7.2 ± 5.4 | 8.5 ± 6.2 *,+ | 7.8 ± 5.2 | p = 0.014 |
| CHC | 8.3 ± 7.4 | 8.0 ± 7.8 | 8.2 ± 7.6 | 8.4 ± 6.5 | p = 0.706 | |
| Ghrelin (ng·L−1) | NHC | 238 ± 72 | 247 ± 68 | 210 ± 75 | 228 ± 74 | p = 0.089 |
| CHC | 211 ± 106 | 208 ± 101 | 217 ± 138 | 212 ± 136 | p = 0.352 | |
| Insulin (mIU·L−1) | NHC | 2.8 ± 1.7 | 2.5 ± 1.7 | 3.8 ± 3.6 | 3.0 ± 2.6 | p = 0.183 |
| CHC | 2.9 ± 2.9 | 3.4 ± 2.8 | 4.2 ± 3.0 | 2.9 ± 2.4 | p = 0.376 | |
| T3 (pmol·L−1) | NHC | 4.9 ± 0.4 | 4.6 ± 0.7 | 4.9 ± 0.6 | 5.0 ± 0.7 | p = 0.119 |
| CHC | 5.6 ± 0.7 aa | 5.4 ± 0.9 | 5.6 ± 0.9 a | 6.2 ± 1.0 aa | p = 0.062 | |
| Glucose (nmol∙L−1) | NHC | 5.0 ± 0.3 | 5.1 ± 0.4 | 4.9 ± 0.5 | 4.9 ± 0.4 | p = 0.384 |
| CHC | 4.8 ± 0.4 | 4.8 ± 0.5 | 4.9 ± 0.5 | 4.9 ± 0.3 | p = 0.519 |
| Group | BLE | FP/ Active1 | OVU/ Active2 | LP/ Inactive | Phase | |
|---|---|---|---|---|---|---|
| EI (kcal·day−1) | NHC | 2340 ± 660 | 2340 ± 540 | 2280 ± 510 | 2270 ± 370 | p = 0.825 |
| CHC | 2770 ± 500 | 2470 ± 510 | 2660 ± 710 | 2510 ± 380 | p = 0.081 | |
| EEE (kcal·day−1) | NHC | 325 ± 157 | 342 ± 109 | 372 ± 170 | 361 ± 199 | p = 0.099 |
| CHC | 248 ± 117 | 326 ± 94.8 | 251 ± 90 | 251 ± 90 | p = 0.591 | |
| EA (kcal·kgFFM−1·day−1) | NHC | 40.0 ± 11.1 | 39.9 ± 11.1 | 35.9 ± 9.0 | 37.6 ± 7.2 | p = 0.465 |
| CHC | 42.9 ± 9.6 | 51.7 ± 11.4 | 49.4 ± 17.4 | 45.5 ± 5.4 a | p = 0.054 | |
| CHO (g·day−1) | NHC | 255 ± 80 | 260 ± 77 | 247 ± 67 | 250 ± 55 | p = 0.896 |
| CHC | 310 ± 60 | 273 ± 61 | 300 ± 91 | 293 ± 44 | p = 0.506 | |
| PROT (g·day−1) | NHC | 112 ± 40 | 107 ± 30 | 110 ± 27 | 105 ± 31 | p = 0.873 |
| CHC | 118 ± 39 | 109 ± 27 | 109 ± 30 | 110 ± 36 | p = 0.072 | |
| FAT (g·day−1) | NHC | 86 ± 27 | 86 ± 33 | 85 ± 21 | 83 ± 19 | p = 0.992 |
| CHC | 105 ± 30 | 91 ± 29 | 100 ± 34 | 84 ± 18 | p = 0.102 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ihalainen, J.K.; Löfberg, I.; Kotkajuuri, A.; Kyröläinen, H.; Hackney, A.C.; Taipale-Mikkonen, R.S. Influence of Menstrual Cycle or Hormonal Contraceptive Phase on Energy Intake and Metabolic Hormones—A Pilot Study. Endocrines 2021, 2, 79-90. https://0-doi-org.brum.beds.ac.uk/10.3390/endocrines2020008
Ihalainen JK, Löfberg I, Kotkajuuri A, Kyröläinen H, Hackney AC, Taipale-Mikkonen RS. Influence of Menstrual Cycle or Hormonal Contraceptive Phase on Energy Intake and Metabolic Hormones—A Pilot Study. Endocrines. 2021; 2(2):79-90. https://0-doi-org.brum.beds.ac.uk/10.3390/endocrines2020008
Chicago/Turabian StyleIhalainen, Johanna K., Ida Löfberg, Anna Kotkajuuri, Heikki Kyröläinen, Anthony C. Hackney, and Ritva S. Taipale-Mikkonen. 2021. "Influence of Menstrual Cycle or Hormonal Contraceptive Phase on Energy Intake and Metabolic Hormones—A Pilot Study" Endocrines 2, no. 2: 79-90. https://0-doi-org.brum.beds.ac.uk/10.3390/endocrines2020008