
Neuroendocrine Changes during Menopausal Transition


Department of Experimental and Clinical Medicine, Division of Obstetrics and Gynecology, University of Pisa, 56126 Pisa, Italy
*
Author to whom correspondence should be addressed.
Endocrines 2021, 2(4), 405-416; https://0-doi-org.brum.beds.ac.uk/10.3390/endocrines2040036
Submission received: 13 July 2021
/
Revised: 28 September 2021
/
Accepted: 8 October 2021
/
Published: 14 October 2021
(This article belongs to the Special Issue Neuroendocrine, Endocrine and Metabolic Triggers of Impaired Female Reproduction)
{kind=link}
Abstract
:Menopause is the permanent cessation of menstrual cycles following the loss of ovarian follicular activity. Quality of life of postmenopausal woman is the result of a series of psychobiological transformations, that see in the reduction of sex hormones and steroids the etiopathogenetic determinant moment. Symptoms of menopause range from somatic side such as metabolic changes, increased cardiovascular disease, irregular vaginal bleeding, urogenital symptoms, vaginal dryness, osteoporosis and risk of bones fractures to changes of central nervous system as vasomotor symptoms, sleep disruption, mood changes, migraine, sexual dysfunctions. It is fundamental to know the mechanisms underlying changes in the central nervous system during menopause, related to hypoestrogenism, to be able to create appropriate target therapy for patients, improving their quality of life. In fact, the central nervous system is now one of the major targets of sex steroids that cannot be achieved disregard when dealing with the problem of choice of a particular type of MHT.
1. Introduction
Quality of life of postmenopausal woman is the result of a series of psychobiological transformations, that see in the reduction of sex hormones and steroids the etiopathogenetic determinant moment. During climacteric period 80% of women complain about subjective bothersome symptomatology that often negatively impact the quality of life (QoL) in personal, social and working activities. Symptoms of menopause range from somatic side (such as metabolic changes, increased cardiovascular disease, irregular vaginal bleeding, urogenital symptoms, vaginal dryness, osteoporosis and risk of bones fractures) to central nervous system (CNS) changes (vasomotor symptoms, sleep disruption, mood changes, migraine, sexual dysfunctions). Changes in neuroendocrine and neurotransmitter systems, related to decreased estrogen seem to negatively affect psycho-physical wellbeing of women and could explain, at least in part, the increased incidence of mental disorders and neurological in the postmenopausal era, respect to women in fertility age.
This group of manifestations includes alterations of psychological balance represented above all from irritability, emotional instability with crisis of sudden crying, insomnia, fatigue, apathy. In particularly predisposed patients, such imbalances can hesitate in real psychiatric illnesses, or anxiety disorders and depressive syndrome [1,2]. Other alterations due to postmenopausal estrogen deficiency lead to alterations in hypothalamic thermoregulatory homeostasis, contributing to the onset of heat flashes and sweats. Several studies instead show a correlation between menopause and the onset of conditions such as Alzheimer’s disease or Parkinson’s disease, thus suggesting a plausible link between neurodegenerative disease and climacteric period.
However, independently from these two pathologies there is a decline of cognitive faculties of the woman (memory changes or cognitive impairment), related to hypoestrogenism. Two other elements to take into consideration when talking about alterations of the central nervous system are migraines, which increase in menopausal women, and to disorders of the sexual sphere (sexual arousal and satisfaction). It is fundamental to know the mechanisms underlying the CNS modifications during menopause, related to hypoestrogenism, so as to be able to create appropriate target therapy for the patients, improving their quality of life. In fact, the central nervous system is now one of the major targets of sex steroids that cannot be disregarded when dealing with the problem of choosing a particular type of menopausal hormonal therapy (MHT). Due to the constant increase of the ageing population and of the number of women experiencing climacteric periods, it is mandatory to understand the relevance of menopausal transition and the postmenopausal period that has relevance for every women worldwide. In fact, nowadays women spent more than one third of their lifespan in the transition and in the postmenopausal period, with potential negative impact in their general quality of life, family, relationships and working activities. The care of women during the climacteric transition involves several healthcare providers who have to monitor and promote healthy activities, prevention strategies, and to prescribe medical or alternative compounds according to the women’s need and personal risk factors. The concept that women are differently vulnerable to menopausal changes strength the concepts of developing a personalized approach and a gender-specific medicine. This article presents an overview on the solid and novel knowledge about the neuroendocrine changes during menopausal transition that is of paramount importance for women’s health and the specialists involved in womens’ healthcare.
2. Neuroendocrine Changes in Menopause
Menopause signs start with the reduction of follicle reserves and the subsequent impairment of ovarian function [3]. From a clinical standpoint, a suitable and reproducible classification of the nomenclature and stages for reproductive ageing was developed during the Stages of Reproductive Aging Workshop (STRAW) in 2001 and implemented in 2012 (STRAW+10). This system aims to classify womens‘ adult life in three different phases: reproductive life, menopausal transition and post-menopausal period. These three phases are than divided into seven stages with final menstrual period (FMP) as the most central event. The STRAW+10 criteria classify bleeding patterns for the early and the late menopausal transition and suggested changes to the criteria for the late reproductive stage (Stage −3) and the early postmenopausal period (Stage +1), provided specified on the length of the late transition (Stage −1) and early postmenopausal period (Stage +1). Moreover, the system suggested applying these rules regardless of the age, body constitution and weight, lifestyle and ethnicity. This progression is characterized by several hormonal modifications that are described as the menopausal transition that take some years to conclude. These changes begin with a significant reduction of the concentrations of inhibin B, thus determining a lack of negative feedback on pituitary FSH secretion [3,4].
The decreased secretion of inhibin B causes an increase in FSH production throughout the menstrual cycle, especially during the follicular phase. Ovulation is anticipated and progesterone secretion slowly decreases. In the premenopausal period the FSH increases, but reduced levels of estrogens, progesterone and LH still exist, but the production of estradiol slowly becomes insufficient and only rarely determines the peak of LH, causing anovulatory cycles. In this case, besides FSH, LH also tends to increase. In menopausal transition, the increase in FSH is 10 times bigger than that of LH; this increase is secondary to the lack of inhibin and to the estrogen feedback, as already mentioned. The levels of estradiol are slowly reduced in favor of an increase in estrone (produced by the aromatization of ovarian and adrenal androstenedione). Estrone has 1/3 the activity compared to estradiol. In addition to inhibin and progesterone, AMH also decreases. In contrast, GnRH increases the frequency and magnitude of the peak secretion (increase in gonadotropins). FSH and LH levels reach their highest levels about 1–3 years after menopause. In women undergoing ovariectomy, the levels of the gonadotropins increase more rapidly. Hypoestrogenism in menopause is associated with a lower sensitivity of the hypothalamus-hypophysis-gonadal axis and its structural and functional modifications. This explains the menopausal symptoms that appear in the transitional period such as hot flashes, insomnia and night sweats. In fact, estrogen and progesterone regulate, in addition to that, the proliferation and maturation of oligodendrocytes, glial cells, increasing number of synapses, promote angiogenic activity of endothelial cells and modulate mitochondrial activity. It is possible to identify two different type of estrogen receptors: ER alpha and beta. We find ER-alpha in the prefrontal cortex, hippocampus, amygdala and hypothalamus (memory and emotional process regions). ER-beta is expressed in the hippocampus, neocortex claustrum, thalamus and in mitochondria (where it exerts a protective action against oxidative diseases like Alzheimer’s disease). The interaction of estradiol with these receptors allow the release and metabolism regulation of neurotransmitters such as dopamine, serotonin, acetylcholine, β-endorphin and some neurosteroids such as allopregnanolone and dehydroepiandrosterone (DHEA) [5].
From a neurobiological standpoint, the monoamine neurotransmitters serotonin, norepinephrine and dopamine seem to modulate both hot flashes and mood disorders. Thus, an impairment of these regulatory pathways can favor the onset of depression when that dysregulation occurs within prefrontal cortex and limbic system that are SNC areas involved in mood control. Moreover, a deregulation of the hypothalamic thermoregulatory centers impacts the onset of vasomotor symptoms. In this view, the treatment of hot flashes with the administration of menopausal hormonal therapy (MHT) can prevent or reduce depressive symptoms in vulnerable women, instead of treating only mood disorders without controlling the vasomotor symptoms. However, in addition to the cessation of estrogenic secretion by the ovaries, a production of sex hormones at the intracranial level remains. Nowadays, gonadal steroid hormones are well recognized to be actively involved in the processes of CNS growth, differentiation, physiology, and ageing. Dehydroepiandrosterone sulphate (DHEAS) levels rise during reproductive age, reaching maximum peripheral concentrations around 30 years of age while around the seventh decade the levels of DHEAS progressively decline to 10–20% of the previous highest concentrations [6]. DHEAS is the principal peripheral product of adrenal glands which is the main source of circulating steroids. Moreover, ovarian thecal cells produce around 20% of peripheral DHEA under the regulation of LH and CNS [7,8]. Consistent evidence from the literature indicates that DHEA acts on CNS through antagonizing GABA-A receptor in a dose-dependent manner thus determining an increase in neuronal excitability and resulting in improvement of memory performances [9,10]. Furthermore, the conditions of low sexual desire and responsiveness in younger women and low responsiveness in older women seem to be significantly associated to low peripheral levels of DHEA relative to age [11]. In extragonadal tissues such as adipose tissue, brain, and bone, DHEA and DHEAS are converted either to androstenedione to testosterone that may be aromatized to estrone (E1) or estradiol (E2) or dihydrotestosterone (DHT). For that reason, DHEAS is considered a therapeutic option for the treatment of the androgen deficiency syndrome in menopause. During menopause, a reduction of another neurotransmitter—allopregnanolone (ALLO)—is also observed ALLO is a 3,5-reduced metabolite of progesterone produced by the complex 5-α-reductase and 3-α-hydroxysteroid oxidoreductase in the CNS, adrenals and ovaries [12,13]. It is the main neurosteroid derived from cholesterol in the neocortex, subcortical and hippocampus [13,14,15]. ALLO has anxiolytic and relaxant properties and it affects mood and behavior. Reduced serum and cerebrospinal fluid concentration of ALLO have been reported in women with depression [16,17,18]. New data confirm a putative effect of ALLO in γ-aminobutyric acid receptor A (GABA-A) receptors. This effect seems to be modulated by ovarian steroids, and estrogens and progesterone control the GABA response through a long-term genomic action [19,20]. In addition, hypoestrogenism causes a reduction secretion of β-endorphin (in β-EP), which is the main biologically relevant and active endogenous opioid peptide with neuroendocrinologic, analgesic and thermoregulatory properties. The postmenopausal reduction was shown to be associated with vasomotor symptoms and mood disorders [4,21]. DHEA supplementation results in the increase of plasmatic, hippocampal and hypothalamic β-EP concentrations and this effect seem to be dose-related thus improving menopause symptoms. MHT is able to positively influence on climacteric symptomatology of the CNS, by restoring an adequate adrenergic tone, serotoninergic and opioid, rebalancing the whole complex of induced neuroendocrine modifications from menopause [2].
2.1. Vasomotor Symptoms and Sleep Disruption
Vasomotor symptoms, in particular hot flushing, are the most frequent symptoms in menopause. Vasomotor symptoms occur in 75–80% of women during the late premenopause and early postmenopause period. In 5% of persons who experience these changes, hot flushes can remain decades after menopause [22,23,24]. A hot flush is an unexpected event of vasodilatation in the face and neck, with abundant sweating with subsequent shivering and feeling of coldness or redness. The duration can range from a few seconds to even 60 min and can be moderate or severe according to the number and the strength of the events. Black race, smoking and overweight are risk factors for vasomotor symptoms [25,26]. The number of daily hot flushes and their intensity can impair general QoL, modify lifestyle and determine stress and anxiety [27]. This bothersome symptom is caused by a deregulation of the hypothalamic thermoregulatory anterior nuclei and the preoptic region. The variation of the corporeal temperature from the baseline stimulates endocrine mediators to start regulatory actions to increase or reduce the production and the dispersion of energy as required to return to baseline temperature. A compression of the thermoregulatory area of the hypothalamus intermittently releases heat in response to a slight increase of the temperature [24]. Impairment of thermoregulation can be associated with deregulation of the serotoninergic and noradrenergic pathway that occur during the fluctuations of estrogens concentrations. Indeed, vasomotor symptoms decrease with passing years, demonstrating that they are triggered by hormone fluctuations and not only hypoestrogenism. The brain undergoes a readjustment to the different sex hormone concentrations during menopausal transition. Many studies have shown a correlation between hot flashes and alterations in glucose metabolism. During menopause the glucose levels in the brain are reduced and even at peripheral level there is an altered glucose tolerance. In fact, ketone bodies and the acid metabolism of fats increase. The SWAN study [28] showed a correlation between hot flushes and dysregulation of glucose metabolism, demonstrated by an increase in fasting blood glucose and HOMA scores. In addition, the onset of hot flashes are more frequent during the first 4 h of sleep, thus determining significant disruption of rest and reduction of the sleep quality. Insomnia and sleep disturbance are prevalent symptoms of perimenopause transition. They are maximal during late perimenopause and persist in post-menopause, independently of vasomotor symptoms [29]. The mechanism of sleep disturbance is not known, but the superchiasmatic nucleus may have a role given its estrogen receptor beta expression in relation to circadian rhythm. Furthermore, low levels of inhibin B are a marker of poor sleep quality. Moreover, many prospective studies indicate an association with poor sleep quality and dementia [30], with an accumulation of β-amyloid in the brain (Figure 1).
2.2. Mood Disorders
Postmenopausal changes in neuropeptide levels and neurotransmitters are implicated in the pathogenesis of characteristic mood disorders of this woman’s life phase. Oscillations in the concentrations of steroids, more than their reduction, could cause depression during menopausal transition. Specially, fluctuations of estrogen impact an impaired regulation of CNS serotonin and noradrenaline paths. Beneficial effects of estrogen administration on mood in postmenopausal women depend on the direct action of gonadal steroids on neuronal activity and on the serotonergic system.
Estrogens modify the concentration of serotonin determining an increase of the rate of degradation of monoamine oxidase (MAO), enzyme responsible for the catabolism of serotonin. Effects exerted by estrogens on the mood cannot be excluded and they can also be partly linked to a direct effect on neuronal activity, given that such steroids would be able to modulate the cerebral blood flow, the glucose levels, as well as neuronal growth and synaptic activity. In the postmenopausal period, those women who start MHT across the perimenopausal transition or at the beginning of menopause seem to maintain glucose metabolism in some brain areas which present neurological functions dependent from the estrogen milieu, such as the hippocampus, entorhinal cortex, medial temporal cortex and posterior cingulate. On the contrary, glucose metabolism in women who do not undertake MHT during perimenopause and menopause, deteriorates in estrogen-dependent areas of the CNS, but seem to be improved in the pons, caudate and precuneus [31,32].
Studies that demonstrated this evidence enrolled symptomatic women and compared them to women who were premenopausal or asymptomatic, so the data derived are possibly only relevant to women who experience symptoms. Some symptoms like depression, irritability, anxiety as well as psychological processes may be affected by the fluctuation of neurosteroid synthesis and secretion. As previously mentioned, ALLO modulates stress, mood and the character traits, expressing anxiolytic properties and sedative-hypnotic, acting as an agonist on GABA-A receptors, [33,34]. MHT can modify the levels of neurosteroids increasing ALLO and reducing DHEA. In this view, the raise of ALLO with MHT could be responsible of the reduction of the anxiety and of sedative effects on women in menopause [35]. However, DHEA is synthesized as a neurosteroid, from the CNS and acts as an antagonist on the receptor GABA-A, with a consequent increase in excitability neuronal and anxiety in menopause women. DHEA levels undergo a decrease starting from the third decade of life (at the age of 70 the concentration plasma of that steroid is reduced to 20% of the maximum peak observed between 18 and 25 years) [36]. Therefore, it has been shown that administration of DHEA in these women leads to an improvement in quality of life of these women, in their cognitive faculties, like memory, anxiety and sexual dysfunction (Figure 1).
2.3. Neurological Disorders, Alzheimer’s Disease and Parkinson’s Disease
Female individuals have a higher constitutional risk of developing chronic and degenerative disorders as the reduction of the short-term memory and the increase in incidence of Alzheimer’s disease (AD), compared to men of the same age [37]. There is a close link between estrogens and cognitive and memory functions. Estrogens play a key role in the physiopathology of degenerative CNS diseases, as they act in areas like the prefrontal cortex, hippocampus and striatum that control learning, registering, and retrieving information, judgment, language skills. Sex hormones and their receptors contribute to the processes of synaptogenesis [38], neuronal growth and neuronal transmission. Also, they limit the inflammatory response in the CSN that cause dystrophy and dementia. Among degenerative pathologies we must recall Alzheimer’s disease. Although the etiology of the memory impairment related with AD is multifactorial, it has been described that estrogens have a protective effect and prolong the latency period of the disease [39]. Some epidemiological data support the hypothesis that MHT may reduce the incidence of AD in women [37,40]. In fact, there is dose-dependent association between estrogens supplementation and frequency of AD, as demonstrated by the reduction of the relative risk of AD with the increase of the estrogen dose and duration of therapy (the risk of AD is reduced of about 50% in patients who have used estrogen, if therapy was undertaken at an early age) [37]. Reduction of cognitive performances, observed in patients suffering from AD, recognizes as neurochemical defect the alteration of the system cholinergic neurotransmitter. In fact, estrogens provide trophic support to cholinergic cells, stimulating the release of acetylcholine and choline acetyltransferase (ChAT), both cholinergic functioning markers; they are also involved in the regulation of survival, regeneration and neuronal plasticity and develop antioxidant neuroprotective action and appear inhibit the formation of β-amyloid [39]. In postmenopausal women affected by AD there were studied gonadotrophin levels, founding a relation among increased β-amyloid and high level of FSH and LH [41]. Many other studies show that the expression of apolipoprotein E, which is responsible of transport of lipids in the blood, is stimulated in hippocampus and prefrontal cortex, through the interaction of 17β-estradiol with estrogen receptors. In women the correlation between apolipoprotein E and AD is more evident than in men, demonstrating the main role of female sex hormones in protecting from neurodegenerative diseases. Lastly, the Mayo Clinic Cohort Study of Oophorectomy and Aging-2, a cohort of patients who experienced bilateral salpingo-oophorectomy before age 50 and reaching natural menopause, shows an accelerated accumulation of multimorbidity and a dysregulation of numerous cellular, tissue, organ and system essential ageing process, for example DNA methylation levels [42]. Surgical menopause may lead to medial temporal lobe structural abnormalities, smaller amygdala volumes, thinner para-hippocampal-entorhinal cortices and β-amyloid deposition thus, increasing the risk of cognitive dysfunction or dementia and presence of AD, compared to women control group [43]. In conclusion, MHT significantly improves cognitive capabilities, positively modulating patterns of activity brain during psychometric tests, facilitating the blood flow towards structures that modulate the memory and improving mood. Another possible correlation is between hypoestrogenism and Parkinson’s disease. There are data in the literature which attest a role of estrogens as potentials neuroprotective agents of dopaminergic neurons. Sawada and coll. have shown that estradiol is protective on mesencephalic dopaminergic neurons from oxidative stress and apoptosis induced by bleomycin [44]. Moreover, estrogens inhibit the uptake of neurotoxins that induce degeneration of dopaminergic neurons [45]. Clinical studies show that estrogen replacement therapy produces less severe symptoms in women with PD in the early stage of the disease, especially if hormone therapy is undertaken before starting levodopa therapy [46]. However, the data are conflicting and there are different opinions in the literature regarding the efficacy of MHT in patients suffering from Parkinson’s disease. Therefore further experimental and clinical studies are necessary to define which role sex steroids may have in PD.
2.4. Migraine
Women who had migraine during their fertility age and, specially, in the premenstrual period, are more susceptible of headaches during the menopause transition. However, the prevalence of migraine in menopause ranges from 10% to 29% and decreases in post-menopause [47]. The reason is that migraine is triggered by sudden declines of estrogen levels and their action in hippocampus and prefrontal cortex. Lower estrogen levels cause vasodilatation, release and plasma extravasation of proinflammatory mediators and consequently cause migraine [48]. Over time the brain adapts its systems to lower hormone and steroid levels. In any case, not all women benefit from hormone therapy, and further scientific evidence is needed to explain the phenomenon.
2.5. Sexual Dysfunctions
Sexual dysfunction is frequent in post-menopause and it depends on hypoestrogenism as well as cultural factors. The prevalence is about 8–50% and it is reported to rise with age from the third decade as well as after oophorectomy. Sexual dysfunction in menopause involves vaginal dryness, reduced libido and reduced pleasure during sexual intercourse. Postmenopausal hormonal deficiency negatively influences sexual function since estrogenic support fails. Estrogens maintain the trophism and elasticity of the vaginal walls, vaginal lubrification and trophism of the entire genitourinary tract. The reduced vulvovaginal receptivity in turn determines dyspareunia and consequently reduced libido. However, the mood and cognitive changes of CNS, described above, contribute to determine disorders of the sexual sphere in a woman during menopause. Sexual behavior in women is significantly determined by endogenous sex steroid concentrations. Several reports suggest that testosterone therapy can be beneficial for patients with hypoactive sexual desire disorder [49]. In parallel, many studies have reported a negative correlation between low peripheral DHEA levels and the impairment of sexual function in pre- and postmenopausal women. In the CNS the neurosteroid DHEA is a regulator of neurotransmitter receptors. In fact, androgen deficiency syndrome, a consequence of a reduced androgen synthesis at both adrenal and ovarian levels, is recognized as a distinctive trait of reduced libido, a sense of psychological well-being and motivation, as well as a cause of easy fatigability [31]. In addition, to improve genital and urinary trophism MHT can play an important role in symptom relief, even if it does not seem to have primary effects on libido.
3. New Evidence in Neuroendocrine Ageing and Menopause
Numerous studies have identified kisspeptin (KP) as an important regulator of GnRH neurons and consequently in controlling the development of puberty. Evidence from the literature demonstrates that epigenetic silencing of repressive factors activates the hypothalamic-pituitary-gonadal axis. In the hypothalamus, the expression of kisspeptin activates GnRH-releasing neurons that stimulate the synthesis and release of FSH and LH by the pituitary gland. Then, the gonadotropins stimulate the ovaries and the testes to synthetize and secrete estrogen and testosterone, respectively. In details, this protein, encoded by the Kiss1 gene, acts through the respective KissR or Gpr54 receptor at the hypothalamic level, stimulating the secretion of GnRH. As evidence, inactivating mutations of the Kiss1 gene or Kiss R result in hypogonadotropic hypogonadism, while activating mutations lead to precocious puberty. In association with KP, other mediators also involved in the modulation of GnRh neuron activity have been identified, such as neurokinin B (NKB) and its NK3R receptor that act indirectly through the regulation of kisspeptin and leptin the hormone of energy expenditure. During the ageing of the reproductive system, pituitary responsiveness to GnRH decreases and the pulsatility of LH lack synchronization resulting in an impairment of sex steroid secretion and in the loss of negative feedback to the pituitary gland and hypothalamus. While the genetic profile is generally unmodified, the environment can induce epigenetic modifications during crucial stages in the brain, thus determining changes in the phenotype during life. Novel theories hypothesize that sexual maturation is strongly determined by epigenetic processes which depend on a complicated flow of biological events that initiate during the intrauterine life and continue after birth and throughout the lifespan. In parallel, the transition through puberal development is a dynamic event that is largely conditioned by environment influences. Indeed, environmental factors during puberty can sensitize the brain towards precise neurological outcomes and aging phenotypes later in life by alterations in histone modifications and DNA methylation [50].
3.1. Relevance of Perimenopausal Neuroendocrine Changes in the Quality of Life
Women’s priority symptoms when evaluating their impact on quality of life are mostly vasomotor symptoms, but also sleep, concentration, and fatigue [51]. These are CNS-related disturbances and often come in clusters and can strongly interfere with daily performance, and well-being at the workplace and in the household. MHT represents the most effective treatment to alleviate bothersome symptoms and ameliorate quality of life. This is true for many estrogen-progestogen formulations as well as for TSEC and tibolone [52]. Women who are severely symptomatic are the ones that experience the most significant improvements in quality of life [53].
Well-being begins in the central nervous system. Transition states, like the menopausal one, require restructuring of regulatory networks, in other words adaptation to a new neuroendocrine status that can take years [54]. There are many hormonal targets for estrogens in the female brain. CNS-related menopausal symptoms are influenced by acyclical modification of estrogens peripheral concentration and decline which determine modifications in production and metabolism of neuroendocrine modulators and neurotransmitters such as serotonin, dopamine and acetylcholine, neuropeptides, such as β-endorphin, neurosteroids and DHEA [55]. The more symptomatic women are therefore possibly the ones that adapt less well to the new menopause-induced hormonal status and are the ones who benefit the most from MHT. MHT has been shown to restore neurosteroid levels in different estrogen-sensitive brain areas of ovariectomized rats and, in post-menopausal women, to increase circulating levels of GABA-A agonists [56].
3.2. Rationale and Role of Menopausal Hormonal Treatment on Neuroendocrine Ageing
Statements of international scientific societies in the field of menopausal medicine currently suggest initiation of MHT in healthy women within ten years of their last menstruation in case of moderate or severe VMS, however the debate on when to stop MHT is still open. In the absence of contraindications, the interruption of the therapy can be decided according to the individual needs and characteristics. Some international guidelines recommend that MHT can be used as long as women recognize that the positive effects outweigh the risks. Indeed, for a significant proportion of women, bothersome menopausal symptoms persist well into advanced age and constitute a problem. Peri/postmenopausal vasomotor symptoms have been shown to persist on average 7.4 years and up to 12 years. In women who are started on MHT, early discontinuation and annual discontinuation is not a good practice, particularly in recently menopausal women. In women who discontinue hormone therapy, vasomotor symptoms recur in 50% of cases, regardless of whether MHT is stopped abruptly or tapered off [57]. Moreover, observational studies have reported the emergence of depressive symptoms after the discontinuation of MHT in 5% to 10% of women [58]. The data were verified by a study on patients with depression during menopausal transition. The women evaluated in the experimental study showed a fast increase in depressive symptoms after a sharp reduction if estradiol [59]. Relevantly, the discontinuation of MHT assumption seems to determine a 26% to 66% increase in deaths due to cardiac problems or stroke in a large study population. Interestingly, the authors reported that the risk was higher in women who started or discontinued MHT before 60 years of age and they hypothesized that an abrupt reduction of vasodilatation induced by estrogen may product vasoconstriction of coronary arteries and lethal thrombogenic complications, especially in younger women with preserved cardiovascular sensitivity to estrogens [60]. Women frequently complain about mood changes, sleep disorders, memory impairment and body shape modifications and the occurrence of vasomotor and urogenital symptoms that accompany the menopause. It is well noted that the symptoms occurring during menopause could significantly affect the personal and social quality of life and cause distress; in this view caregivers involved in women’s health should be prepared and skilled to aid women, especially through the menopausal transition. An emerging concept within the area of menopausal medicine is that to experience some menopausal symptoms is predictive of possible health pathologies in the future. Complaints of vasomotor symptoms and poor quality of sleep seem to be related to the increased onset of cardiovascular disease, climacteric depressive disorders and cognitive dysfunctions. Moreover, severe vasomotor symptoms are correlated with increased osteoporosis andA higher number of bone fractures, and short sleep or insomnia have been associated with impairment of sexual function In this view, a growing body of evidence from the literature is consistent in affirming that symptomatic perimenopausal women who are not treated with hormonal compounds could experience significant reduction of the QoL, negative impacts on their workplace activity and general impairment of health conditions [61]. MHT is an effective treatment for bothersome menopausal disturbances. Furthermore, targeting one symptom may influence and benefit other domains of a woman’s health if MHT is started early enough. By properly evaluating cardiovascular risk factors, VTE risk factors, the health hazards can be reduced to a minimum. Moreover, promoting a healthy lifestyle and eliminating any modifiable risk factors, such as obesity, alcohol and tobacco consumption, can reduce the personal risk of developing cancer. Finally, where possible, transdermal routes of MHT administration should be preferred as they have the least impact on coagulation, glucose and lipid metabolism. Within combined treatment options, natural progesterone should be favored as it is devoid of the antiapoptotic properties of other progestogens on breast cells. Upon beginning MHT, low doses should be used and increased gradually until effective control of symptoms is achieved. Unless contraindications develop, patients may elect to continue MHT while the benefits outweigh the risks. Menopause occurs within a natural aging process therefore regular reassessment of the woman’s health status is necessary. Women should be made aware that there is a small increased risk of stroke and breast cancer with long-term estrogen-progestin use. However, early treatment initiators will probably gain more profit than harm by improving bothersome symptoms, while obtaining offset benefits like cardiovascular risk reduction, increase in bone mineral density and reduction in bone fracture risk, decrease in colorectal cancer risk and in overall mortality [62].
Tailoring treatment also means taking into account a women’s needs like her right to have a satisfactory sexual life, or her need to preserve body image, or her athletic performance. These are all important factors to consider when choosing the right treatment option. Androgen replacement in addition to MHT may therefore be considered in selected cases. To this regard, MHT may also help patients maintain the ability to continue coping with their environment. Because of the role that women have assumed in society, the new challenge of healthcare is that of guaranteeing a congruent quality of life. Menopausal medicine is far from recommending MHT to women for anything besides treatment of bothersome menopausal symptoms, but it is very close to improving women’s daily lives.
4. Conclusions
Menopause is the last phase in a long and complex cascade of events occurring both in the CNS and in the ovaries. Several neuroendocrine changes and hypoestrogenism play a key role in these modifications and to cause vasomotor symptoms, migraine, depression or anxiety, cognitive disorders. The knowledge of these process allows to offer new therapeutic perspectives with personalized therapies based on woman’s clinic needs.
Author Contributions
A.G. writing and bibliographic research, revision of the literature, figure; M.C. revision of the scientific literature; A.R.G. supervision and revision of scientific literature; T.S. supervision and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Genazzani, A.R.; Gambacciani, M. Hormone replacement therapy: The prospectives for the 21st century. Maturitas 1999, 32, 11–17. [Google Scholar] [CrossRef]
- Genazzani, A.R.; Spinetti, A.; Gallo, R.; Bernardi, F. Menopause and the central nervous system: Intervention options. Maturitas 1999, 3, 103–110. [Google Scholar] [CrossRef]
- Davis, S.R. Menopause. Nat. Rev. Dis. Primers 2015, 1, 15004. [Google Scholar] [CrossRef] [PubMed]
- Harlow, S.D.; Gass, M.; Hall, J.E.; Lobo, R.; Maki, P.; Rebar, R.W.; Sherman, S.; Sluss, P.M.; de Villiers, T.J. Executive summary of the stages of reproductive aging workshop. Addressing the unfinished agenda of staging reproductive aging. J. Clin. Endocrinol. Metab. 2012, 97, 1159–1168. [Google Scholar] [CrossRef]
- Farrag, A.F.; Khedr, E.M.; Abdel-Aleem, H.; Rageh, T.A. Effects of Surgical Menopause on Cognitive Functions. Dement. Geriatr. Cogn. Disord. 2002, 13, 193–198. [Google Scholar] [CrossRef]
- Orentreich, N.; Brind, J.L.; Vogelman, J.H.; Andres, R.; Baldwin, H. Long-term longitudinal measurements of plasma dehydroepiandrosterone sulfate in normal men. J. Clin. Endocrinol. Metab. 1992, 75, 1002–1004. [Google Scholar] [PubMed]
- Yamaji, T.; Ibayashi, H. Serum deydroepiandrosterone sulphate in normal and pathological canditions. J. Clin. Endocrinol. Metab. 1969, 29, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Corpechot, C.; Robert, P.; Axelson, M.; Sjovall, J.; Baulieu, E.E. Characterization and measurement of deydriepiandrosterone sulfate in the rat brain. Proc. Natl. Acad. Sci. USA 1981, 78, 4704–4707. [Google Scholar] [CrossRef] [Green Version]
- Majewska, M.D.; Demirgoren, S.; Spivak, C.E.; London, E.D. The neurosteroid DHEA is an allosteric antagonist of the GABA A receptor. Brain Res. 1990, 526, 143–146. [Google Scholar] [CrossRef]
- Baulieu, E.E. Dehydroepiandrosterone: A fountain of youth? J. Clin. Endocrinol. Metab. 1996, 81, 3147–3151. [Google Scholar] [CrossRef]
- Davis, S.; Shah, S.M.; McKenzie, D.P.; Kulkarni, J.; Davison, S.; Bel, R.J. Dehydroepiandrosterone Sulfate Levels Are Associated with More Favorable Cognitive Function in Women. J. Clin. Endocrinol. Metab. 2008, 93, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baulieu, E.E. Neurosteroids: A new function in the brain. Biol. Cell 1991, 71, 3–10. [Google Scholar] [CrossRef]
- Robel, P.; Baulieu, E.E. Neurosteroids. Biosynthesis and function. Trends Endocrinol. Metab. 1994, 5, 1–8. [Google Scholar] [CrossRef]
- Stoffel-Wagner, B. Neurosteroid metabolism in the human brain. Eur. J. Endocrinol. 2001, 145, 669–679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoffel-Wagner, B.; Watzka, M.; Steckelbroeck, S.; Ludwig, M.; Clusmann, H.; Bidlingmaier, F.; Casarosa, E.; Luisi, S.; Elger, C.E.; Beyenburg, S. Allopregnanolone serum levels and expression of 5-alpha-reductase and 3-alpha hydroxysteroid dehydrogenase isoforms in hippocampal and temporal cortex of patients with epilepsy. Epilepsy Res. 2003, 54, 11–19. [Google Scholar] [CrossRef]
- Sundstrom, I.; Andersson, A.; Nyberg, S.; Purdy, R.H.; Bäckström, T. Patients with premenstrual syndrome have a different sensitivity to a neuroactive steroid during the menstrual cycle compared to control subjects. Neuroendocrinology 1998, 67, 126–138. [Google Scholar] [CrossRef] [PubMed]
- Khisti, R.T.; Mandhane, S.N.; Chopde, C.T. The neurosteroid 3-alpha-hydroxy-5-alpha-pregnan-20-one induces catalepsy in mice. Neurosci. Lett. 1998, 251, 85–88. [Google Scholar] [CrossRef]
- Johansson, I.M.; Birzniece, V.; Lindblad, C.; Olsson, T.; Bäckström, T. Allopregnanolone inhibits learning in the Morris water maze. Brain Res. 2002, 934, 125–131. [Google Scholar] [CrossRef]
- Genazzani, A.R.; Bernardi, F.; Pluchino, N.; Begliuomini, S.; Lenzi, E.; Casarosa, E.; Luisi, M. Endocrinology of menopausal transition and its brain implications. CNS Spectr. 2005, 10, 449–457. [Google Scholar] [CrossRef]
- Słopien, R.; Junik, R.; Meczekalski, B.; Halerz-Nowakowska, B.; Maciejewska, M.; Warenik-Szymankiewicz, A.; Sowińskib, J. Influence of hormonal replacement therapy on the regional cerebral blood flow in postmenopausal women. Maturitas 2003, 46, 255–262. [Google Scholar] [CrossRef]
- Słopien, R.; Jasniewicz, J.; Meczekalski, B.; Warenik-Szymankiewicza, A.; Lianeri, M.; Jagodzińskib, P.P. Polymorphic variants of genes encoding MTHFR, MTR and MTHFD1 and the risk of depression in postmenopausal women in Poland. Maturitas 2008, 8, 252–255. [Google Scholar] [CrossRef]
- Downs, J.L.; Wise, P.M. The role of the brain in female reproductive aging. Mol. Cell Endocrinol. 2009, 299, 32–38. [Google Scholar] [CrossRef] [Green Version]
- Santoro, N. Symptoms of menopause: Hot flushes. Clin. Obstet. Gynecol. 2008, 51, 539–548. [Google Scholar] [CrossRef]
- Freedman, R.R. Menopausal hot flashes: Mechanisms, endocrinology, treatment. J. Steroid Biochem. Mol. Biol. 2014, 142, 115–120. [Google Scholar] [CrossRef] [Green Version]
- Richard-Davis, G.; Wellons, M. Racial and ethnic differences in the physiology and clinical symptoms of menopause. Semin. Reprod. Med. 2013, 31, 380–386. [Google Scholar]
- Duffy, O.K.; Iversen, L.; Aucott, L.; Hannaford, P.C. Factors associated with resilience or vulnerability to hot flushes and night sweats during the menopausal transition. Menopause 2013, 20, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Thurston, R.C.; Chang, Y.; Mancuso, P.; Matthews, K.A. Adipokines, adiposity, and vasomotor symptoms during the menopause transition: Findings from the Study of Women’s Health across the Nation. Fertil. Steril. 2013, 100, 793–800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thurston, R.C.; Khoudary, S.R.E.; Sutton-Tyrrell, K.; Crandall, C.J.; Sternfeld, B.; Joffe, H.; Gold, E.B.; Selzer, F.; Matthews, K.A. Vasomotor symptoms and insulin resistance in the study of women’s health across the nation. J. Clin. Endocrinol. Metab. 2021, 97, 3487–3494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kravitz, H.M.; Joffe, H. Sleep during the perimenopause: A Swan story. Obstet. Gynecol. Clin. N. Am. 2011, 38, 567–586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yaffe, K.; Falvey, C.M.; Hoang, T. Connections between sleep and cognition in older adults. Lancet Neurol. 2014, 13, 1017–1028. [Google Scholar] [CrossRef]
- Rasgon, N.L.; Silverman, D.; Siddarth, P.; Miller, K.; Ercoli, L.M.; Elman, S.; Lavretsky, H.; Huang, S.-C.; Phelpsc, M.E.; Small, G.W. Estrogen use and brain metabolic change in postmenopausal women. Neurobiol. Aging 2005, 26, 229–235. [Google Scholar] [CrossRef]
- Maki, P.M.; Resnick, S.M. Longitudinal effects of estrogen replacement therapy on PET cerebral blood flow and cognition. Neurobiol. Aging 2000, 21, 373–383. [Google Scholar] [CrossRef]
- Majewska, M.D. Neurosteroids: Endogenous bimodal modulators of the GABA A receptors. Mechanism of action and physiological significance. Prog. Neurobiol. 1992, 38, 379–395. [Google Scholar] [CrossRef]
- Mellon, S.H. Neurosteroids: Action and clinical relevance. J. Clin. Endocrinol. Metab. 1994, 78, 1003–1008. [Google Scholar] [PubMed]
- Bernardi, F.; Pieri, M.; Stomati, M.; Luisi, S.; Palumbo, M.; Pluchino, N.; Ceccarelli, C.; Genazzani, A.R. Effect of different hormonal replacement therapies on circulating allopregnanolone and dehydroepiandrosterone levels in postmenopausal women. Gynecol. Endocrinol. 2003, 17, 65–77. [Google Scholar] [CrossRef] [PubMed]
- Davis, S.R.; Burger, H.G. Androgens and the postmenopausal woman, Clinical Review. J. Clin. Endocrinol. Metab. 1996, 81, 2759–2763. [Google Scholar] [PubMed]
- Paganini-Hill, A.; Henderson, V. Estrogen deficiency and risk of Alzheimer’s Disease in women. Am. J. Epidemiol. 1994, 140, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.; Irwin, R.W.; Zhao, L.; Nilsen, J.; Hamilton, R.T.; Brinton, R.D. Mitochondrial bioenergetic deficit precedes Alzheimer’s pathology in female mouse model of Alzheimer’s disease. Proc. Natl. Acad. Sci. USA 2009, 106, 14670–14675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherwin, B.B. Estrogen effects on cognition in menopausal women. Neurology 1997, 48, S21–S26. [Google Scholar] [CrossRef] [PubMed]
- Zandi, P.P.; Carlson, M.C.; Plassman, B.L.; Welshbohmer, K.A.; Mayer, L.S.; Steffens, D.C.; Breitner, J.C. Hormone replacement therapy and incidence of Alzheimer disease in older women: The Cache County Study. JAMA 2002, 288, 2123–2129. [Google Scholar] [CrossRef] [Green Version]
- Brinton, R.D. Investigative models for determining hormone therapy-induced outcomes in brain: Evidence in support of a healthy cell bias of estrogen action. Ann. N. Y. Acad. Sci. 2005, 1052, 57–74. [Google Scholar] [CrossRef]
- Rocca, W.A.; Rocca, L.G.; Smith, C.Y.; Grossardt, B.R.; Faubion, S.; Shuster, L.T.; Kirkland, J.L.; LeBrasseur, N.K.; Schafer, M.J.; Mielke, M.; et al. Loss of ovarian hormones and accelerated somatic and mental aging. Physiology 2018, 33, 374–383. [Google Scholar] [CrossRef]
- Zeydan, B.; Tosakulwong, N.; Schwarz, C.G.; Senjem, M.L.; Gunter, J.L.; Reid, R.I.; Rocca, G.L.; Lesnick, T.G.; Smith, C.Y.; Bailey, K.R.; et al. Association of bilateral salpingo-oophorectomy before menopause onset with medial temporal lobe neurodegeneration. JAMA Neurol. 2019, 76, 1. [Google Scholar] [CrossRef] [Green Version]
- Sawada, H.; Ibi, M.; Kihara, T.; Urushitani, M.; Akaika, A.; Shimohama, S. Estradiol protects mesencephalic dopaminergic neurons from oxidative stress-induced neuronal death. J. Neurosci. Res. 1998, 54, 707–719. [Google Scholar] [CrossRef]
- Dluzen, D.E.; MCDermott, J.L. Gender differences in neurotoxicity of the nigrostriatal dopaminergic system: Implications for Parkinson’s disease. J. Gend. Specif. Med. 2000, 3, 36–42. [Google Scholar]
- Saunders-Pullman, R.; Gordon-Elliott, J.; Parides, M.; Fahn, S.; Saunders, H.R.; Bressman, S. The effect of estrogen replacement on early Parkinson’s disease. Neurology 1999, 52, 1417–1421. [Google Scholar] [CrossRef]
- Short, R.A.; Bowen, R.L.; O’Brien, P.C.; Graff-Radford, N.R. Elevated gonadotropin levels in patients with Alzheimer disease. Mayo Clin. Proc. 2001, 76, 906–909. [Google Scholar] [CrossRef]
- Hagemann, G.; Ugur, T.; Schleussner, E.; Mentzel, H.J.; Fitzek, C.; Witte, O.W.; Gaser, C. Changes in Brain Size during the Menstrual Cycle. PLoS ONE 2011, 6, e14655. [Google Scholar] [CrossRef] [PubMed]
- Laumann, E.; Paik, A.; Rosen, R.C. Sexual dysfunction in the United States: Prevalence and predictors. JAMA 1999, 281, 537–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bacon, E.R.; Brinton, R.D. Epigenetics of the developing and aging brain: Mechanisms that regulate onset and outcomes of brain reorganization. Neurosci. Biobehav. Rev. 2021, 125, 503–516. [Google Scholar] [CrossRef]
- Rahkola-Soisalo, P.; Savolainen-Peltonen, H.; Gissler, M.; Hoti, F.; Vattulainen, P.; Ylikorkala, O.; Mikkola, T.S. Increased risk for stress urinary incontinence in women with postmenopausal hormone therapy. Int. Urogynecol. J. 2019, 30, 251–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nappi, P.R.; Cucinella, L.; Martella, S.; Rossi, M.; Tiranini, L.; Martini, E. Female sexual dysfunction (FSD): Prevalence and impact on quality of life (QoL). Maturitas 2016, 94, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Gass, M.L.; Cochrane, B.B.; Larson, J.C.; Manson, J.E.; Barnabei, V.M.; Brzyski, R.G.; Lane, D.S.; LaValleur, J.; Ockene, J.K.; Mouton, C.P.; et al. Patterns and predictors of sexual activity among women in the Hormone Therapy trials of the Women’s Health Initiative. Menopause 2011, 18, 1160–1171. [Google Scholar] [CrossRef] [PubMed]
- Scheffers, C.S.; Armstrong, S.; Cantineau, A.E.; Farquhar, C.; Jordan, V. Dehydroepiandrosterone for women in the peri- or postmenopausal phase. Cochrane Database Syst. Rev. 2015, 1, CD011066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peixoto, C.; Carrilho, C.G.; Barros, J.A.; Ribeiro, T.T.; Silva, L.M.; Nardi, A.E.; Cardoso, A.; Veras, A.B. The effects of dehydroepiandrosterone on sexual function: A systematic review. Climacteric 2017, 20, 129–137. [Google Scholar] [CrossRef]
- Dören, M.; Ruebig, A.; Holzgreve, W. Differential effects on the androgen status of postmenopausal women treated with tibolone and continuous combined estradiol and norethindrone acetate replacement therapy. Fertil. Steril. 2001, 75, 554–558. [Google Scholar] [CrossRef]
- Gartoulla, P.; Worsley, R.; Bell, R.J.; Davis, S.R. Moderate to severe vasomotor and sexual symptoms remain problematic for women aged 60 to 65 years. Menopause 2018, 25, 1331–1338. [Google Scholar] [CrossRef]
- Ockene, J.K.; Barad, D.H.; Cochrane, B.B. Symptom experience after discontinuing use of estrogen plus progestin. JAMA 2005, 294, 183–193. [Google Scholar] [CrossRef]
- Schmidt, P.J.; Dor, R.B.; Martinez, P.E.; Guerrieri, G.M.; Harsh, V.L.; Thompson, K.; Koziol, D.E.; Nieman, L.K.; Rubinow, D.R. Effects of Estradiol Withdrawal on Mood in Women With Past Perimenopausal Depression: A Randomized Clinical Trial. JAMA Psychiatry 2015, 72, 714–726. [Google Scholar] [CrossRef] [Green Version]
- Mikkola, T.S.; Tuomikoski, P.; Lyytinen, H.; Korhonen, P.; Hoti, F.; Vattulainen, P.; Gissler, M.; Ylikorkala, O. Increased cardiovascular mortality risk in women discontinuing postmenopausal hormone therapy. J. Clin. Endocrinol. Metab. 2015, 100, 4588–4594. [Google Scholar] [CrossRef] [Green Version]
- Monteleone, P.; Mascagni, G.; Giannini, A.; Genazzani, A.R.; Simoncini, T. Symptoms of menopause—global prevalence, physiology and implications. Nat. Rev. Endocrinol. 2018, 14, 199–215. [Google Scholar] [CrossRef] [PubMed]
- Genazzani, A.R.; Monteleone, P.; Giannini, A.; Simoncini, T. Hormone therapy in the postmenopausal years: Considering benefits and risks in clinical practice. Hum. Reprod. Update 2021. [Google Scholar] [CrossRef]
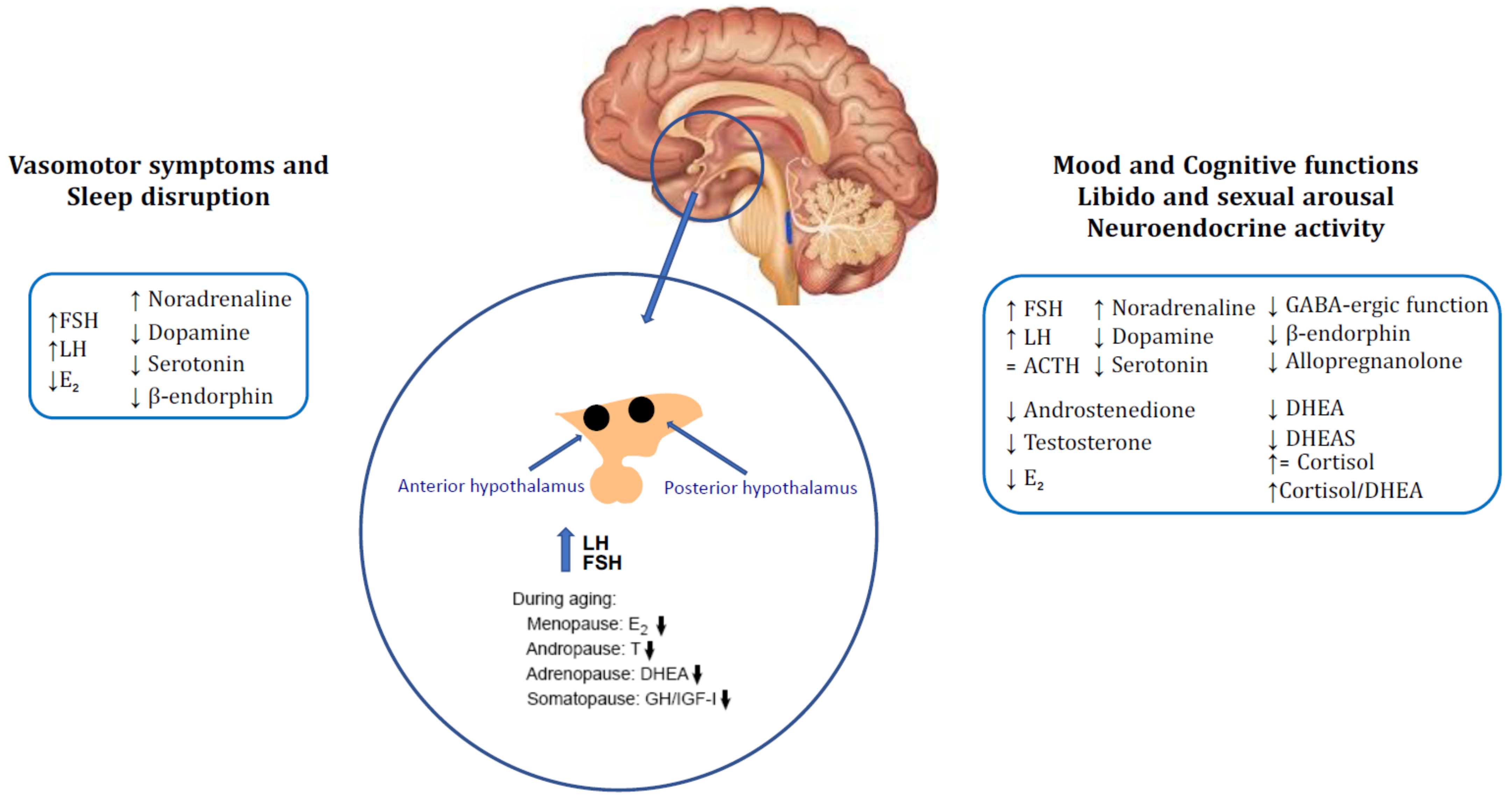
Figure 1.
Brain neuroendocrine changes of menopause and the related symptoms: Modifications of gonadotropins, E2, neuromodulators and opioid tone in the hypothalamus causing onset of vasomotor symptoms and consequent sleep disruption. Mood, cognitive functions, libido, sexual arousal and neuroendocrine activity are close related to the impairment of GABAergic, opioid and neurosteroid milieu in central nervous system (CNS) occurred with ageing. Menopausal condition determines reduction in estrogens and ovarian and adrenal steroids (testosterone, androstenedione, DHEA and DHEA-S) which results in increase cortisol/DHEA ratio leading to sexual, mood and cognitive dysfunctions. ↑: increased, ↓: decreased, =: unchanged.
Figure 1.
Brain neuroendocrine changes of menopause and the related symptoms: Modifications of gonadotropins, E2, neuromodulators and opioid tone in the hypothalamus causing onset of vasomotor symptoms and consequent sleep disruption. Mood, cognitive functions, libido, sexual arousal and neuroendocrine activity are close related to the impairment of GABAergic, opioid and neurosteroid milieu in central nervous system (CNS) occurred with ageing. Menopausal condition determines reduction in estrogens and ovarian and adrenal steroids (testosterone, androstenedione, DHEA and DHEA-S) which results in increase cortisol/DHEA ratio leading to sexual, mood and cognitive dysfunctions. ↑: increased, ↓: decreased, =: unchanged.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Giannini, A.; Caretto, M.; Genazzani, A.R.; Simoncini, T. Neuroendocrine Changes during Menopausal Transition. Endocrines 2021, 2, 405-416. https://0-doi-org.brum.beds.ac.uk/10.3390/endocrines2040036
AMA Style
Giannini A, Caretto M, Genazzani AR, Simoncini T. Neuroendocrine Changes during Menopausal Transition. Endocrines. 2021; 2(4):405-416. https://0-doi-org.brum.beds.ac.uk/10.3390/endocrines2040036
Chicago/Turabian StyleGiannini, Andrea, Marta Caretto, Andrea R. Genazzani, and Tommaso Simoncini. 2021. "Neuroendocrine Changes during Menopausal Transition" Endocrines 2, no. 4: 405-416. https://0-doi-org.brum.beds.ac.uk/10.3390/endocrines2040036