
The Environment of Birthplace and Self-Reported Mental Health Conditions: Findings from the American Panel of Life


{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Sample
2.2. Measures
2.2.1. Environment of Birthplace (Independent)
2.2.2. Psychiatric and Substance Use Disorders (Dependent)
2.2.3. Sociodemographic Characteristics (Covariates)
2.3. Analysis
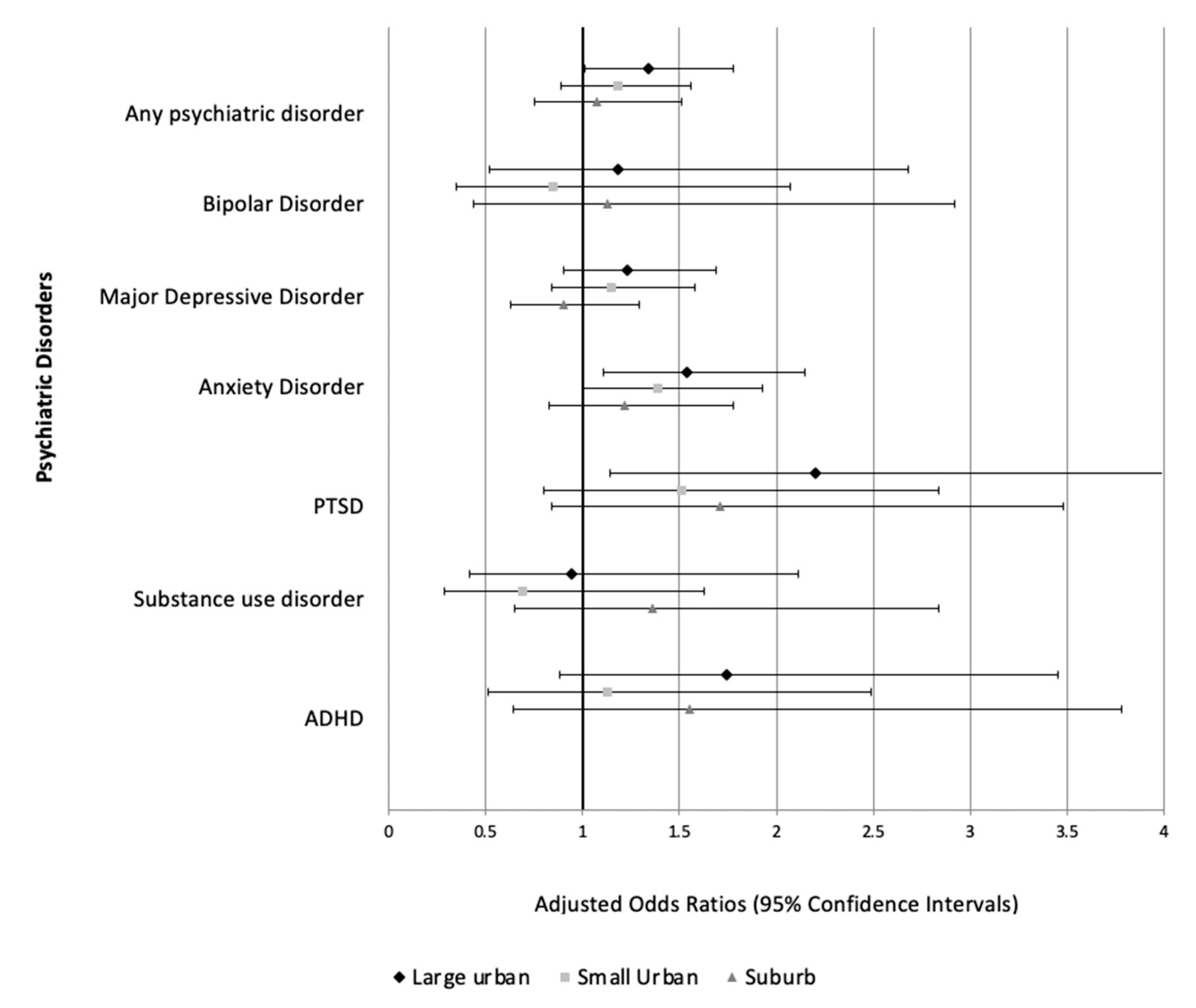
3. Results
4. Discussion
4.1. Main Findings
4.2. Limitations and Future Directions
4.3. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Galea, S.; Vlahov, D. URBAN HEALTH: Evidence, Challenges, and Directions. Annu. Rev. Public Health 2005, 26, 341–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wirth, L. Urbanism as a Way of Life. Am. J. Sociol. 1938, 44, 1–24. [Google Scholar] [CrossRef]
- Ventriglio, A.; Torales, J.; Castaldelli-Maia, J.M.; De Berardis, D.; Bhugra, D. Urbanization and emerging mental health issues. CNS Spectr. 2021, 26, 43–50. [Google Scholar] [CrossRef] [PubMed]
- McCall-Hosenfeld, J.S.; Mukherjee, S.; Lehman, E.B. The Prevalence and Correlates of Lifetime Psychiatric Disorders and Trauma Exposures in Urban and Rural Settings: Results from the National Comorbidity Survey Replication (NCS-R). PLoS ONE 2014, 9, e112416. [Google Scholar] [CrossRef] [PubMed]
- Bakolis, I.; Hammoud, R.; Stewart, R.; Beevers, S.; Dajnak, D.; MacCrimmon, S.; Broadbent, M.; Pritchard, M.; Shiode, N.; Fecht, D.; et al. Mental health consequences of urban air pollution: Prospective population-based longitudinal survey. Soc. Psychiatry Psychiatr. Epidemiol. 2020, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Kristine, E.; Jens-Christian, S.; Lars, A.; Jørgen, B.; Christian, E.; Camilla, G.; Ole, H.; Bo, M.P.; Oleguer, P.; Constantinos, T. Associations between growing up in natural environments and subsequent psychiatric disorders in Denmark. Environ. Res. 2020, 188, 109788. [Google Scholar]
- Peen, J.; Schoevers, R.A.; Beekman, A.; Dekker, J. The current status of urban-rural differences in psychiatric disorders. Acta Psychiatr. Scand. 2010, 121, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Oh, H.; Nicholson, H.L., Jr.; Koyanagi, A.; Jacob, L.; Glass, J. Urban upbringing and psychiatric disorders in the United States: A racial comparison. Int. J. Soc. Psychiatry 2020, 67, 0020764020950781. [Google Scholar] [CrossRef] [PubMed]
- Breslau, J.; Marshall, G.N.; Pincus, H.A.; Brown, R.A. Are mental disorders more common in urban than rural areas of the United States? J. Psychiatr. Res. 2014, 56, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Pollard, M.; Baird, M.D. The RAND American Life Panel: Technical Description; RAND: Santa Monica, CA, USA, 2017. [Google Scholar]
- Braithwaite, I.; Zhang, S.; Kirkbride, J.B.; Osborn, D.P.; Hayes, J.F. Air pollution (particulate matter) exposure and associations with depression, anxiety, bipolar, psychosis and suicide risk: A systematic review and meta-analysis. Environ. Health Perspect. 2019, 127, 126002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, S.-J.; Heinrich, J.; Bloom, M.; Zhao, T.; Shi, T.-X.; Feng, W.-R.; Sun, Y.; Shen, J.-C.; Yang, Z.-C.; Yang, B.-Y.; et al. Ambient air pollution and depression: A systematic review with meta-analysis up to 2019. Sci. Total Environ. 2020, 701, 134721. [Google Scholar] [CrossRef] [PubMed]
- Lan, Y.; Roberts, H.; Kwan, M.-P.; Helbich, M. Transportation noise exposure and anxiety: A systematic review and meta-analysis. Environ. Res. 2020, 191, 110118. [Google Scholar] [CrossRef] [PubMed]
- Krabbendam, L.; Van Vugt, M.; Conus, P.; Söderström, O.; Abrahamyan Empson, L.; van Os, J.; Fett, A.K. Understanding urbanicity: How interdisciplinary methods help to unravel the effects of the city on mental health. Psychol. Med. 2020, 51, 1099–1110. [Google Scholar] [CrossRef] [PubMed]
- Fox, J.C.; Blank, M.; Rovnyak, V.G.; Barnett, R.Y. Barriers to help seeking for mental disorders in a rural impoverished population. Community Ment. Health J. 2001, 37, 421–436. [Google Scholar] [CrossRef] [PubMed]
- National Alliance on Mental Illness. Mental Health by the Numbers. Available online: https://www.nami.org/mhstats (accessed on 7 July 2021).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, H.; Goehring, J.; Jacob, L.; Smith, L. The Environment of Birthplace and Self-Reported Mental Health Conditions: Findings from the American Panel of Life. Epidemiologia 2021, 2, 256-261. https://0-doi-org.brum.beds.ac.uk/10.3390/epidemiologia2030019
Oh H, Goehring J, Jacob L, Smith L. The Environment of Birthplace and Self-Reported Mental Health Conditions: Findings from the American Panel of Life. Epidemiologia. 2021; 2(3):256-261. https://0-doi-org.brum.beds.ac.uk/10.3390/epidemiologia2030019
Chicago/Turabian StyleOh, Hans, Jessica Goehring, Louis Jacob, and Lee Smith. 2021. "The Environment of Birthplace and Self-Reported Mental Health Conditions: Findings from the American Panel of Life" Epidemiologia 2, no. 3: 256-261. https://0-doi-org.brum.beds.ac.uk/10.3390/epidemiologia2030019