
Influence of Gender on Occurrence of Aseptic Loosening and Recurrent PJI after Revision Total Knee Arthroplasty

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
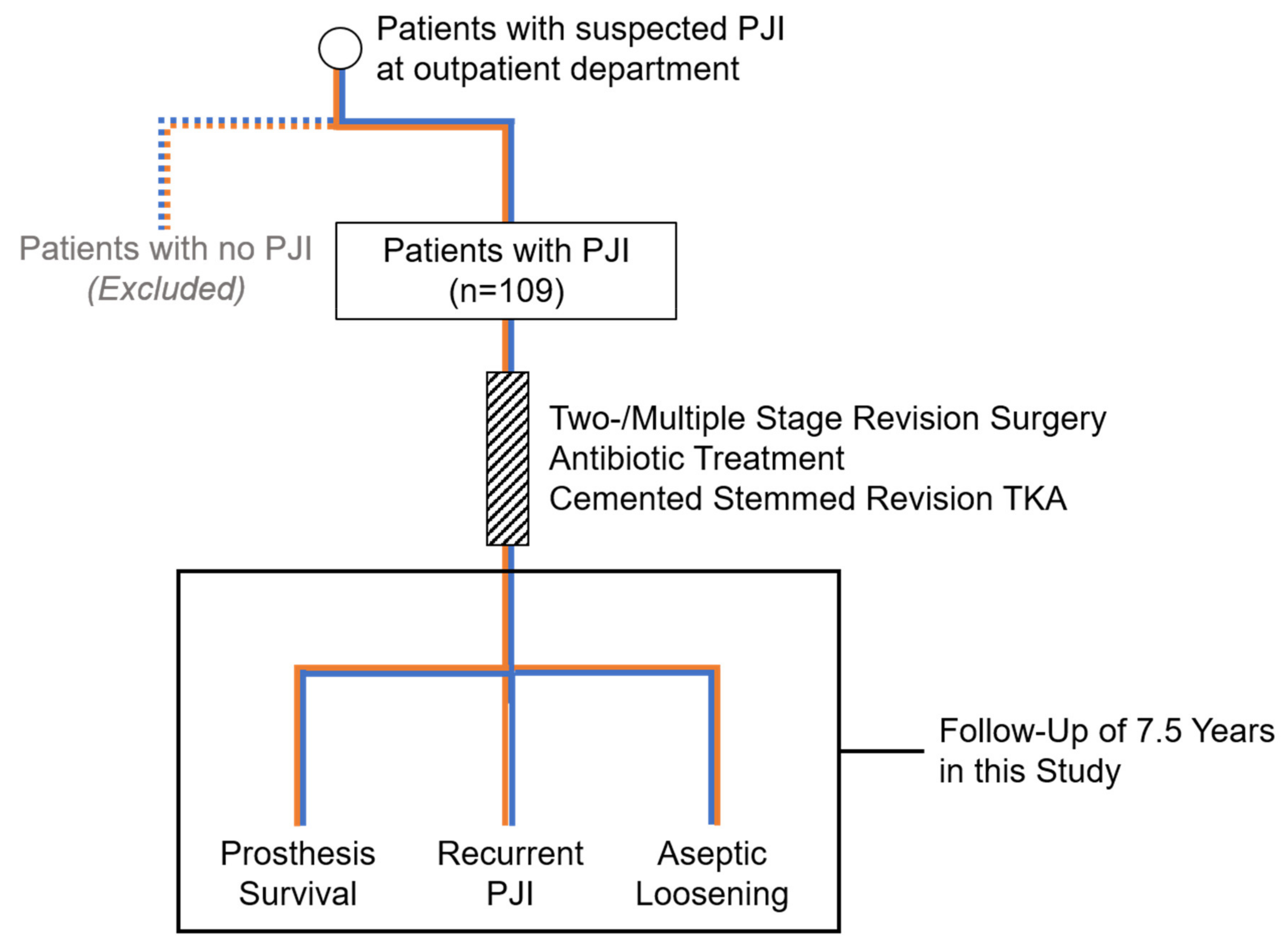
2.1. Patients
2.2. Treatment
2.3. Microbiology
2.4. Follow-Up
2.5. X-ray Analysis
2.6. Statistics
3. Results
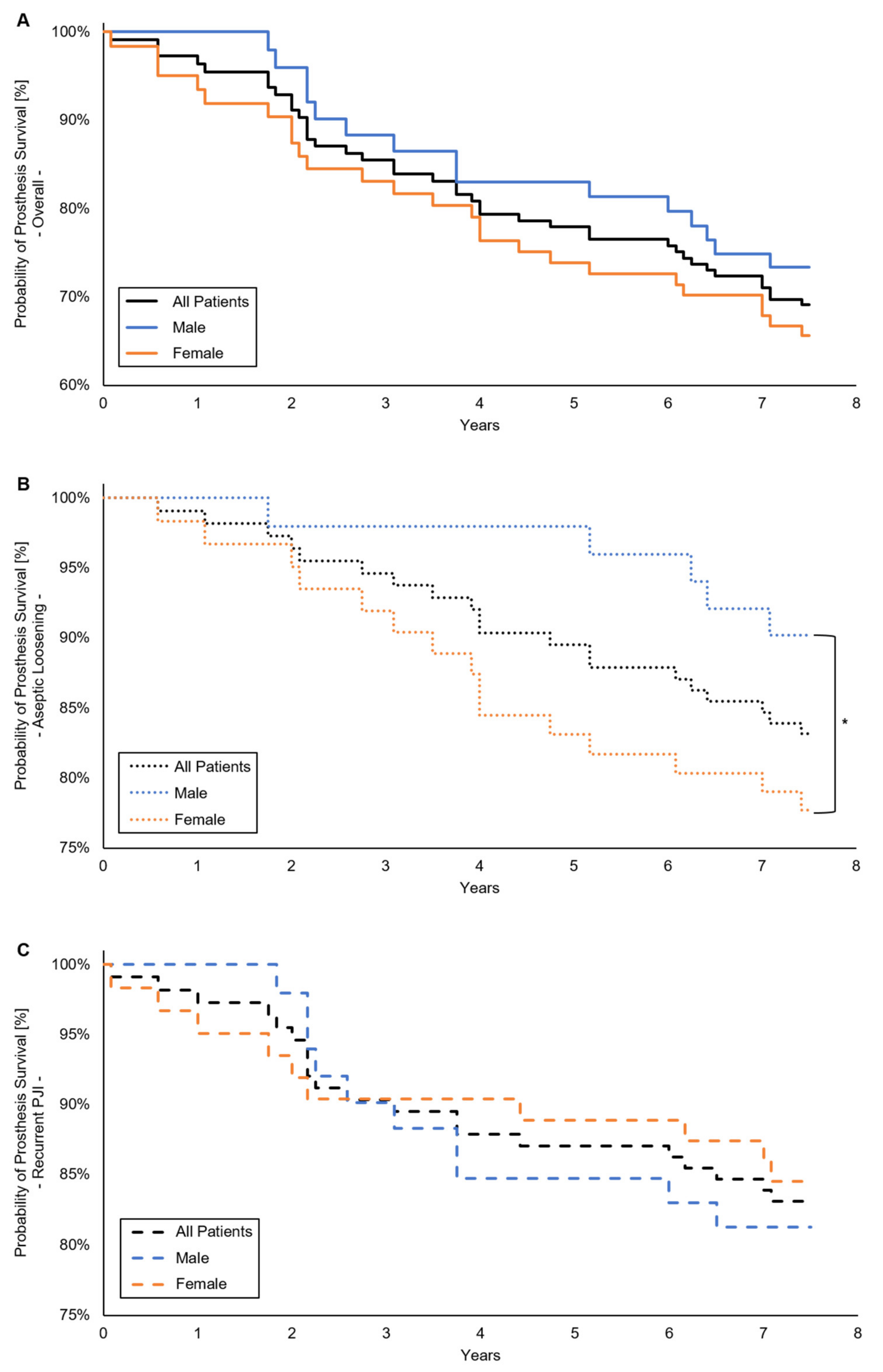
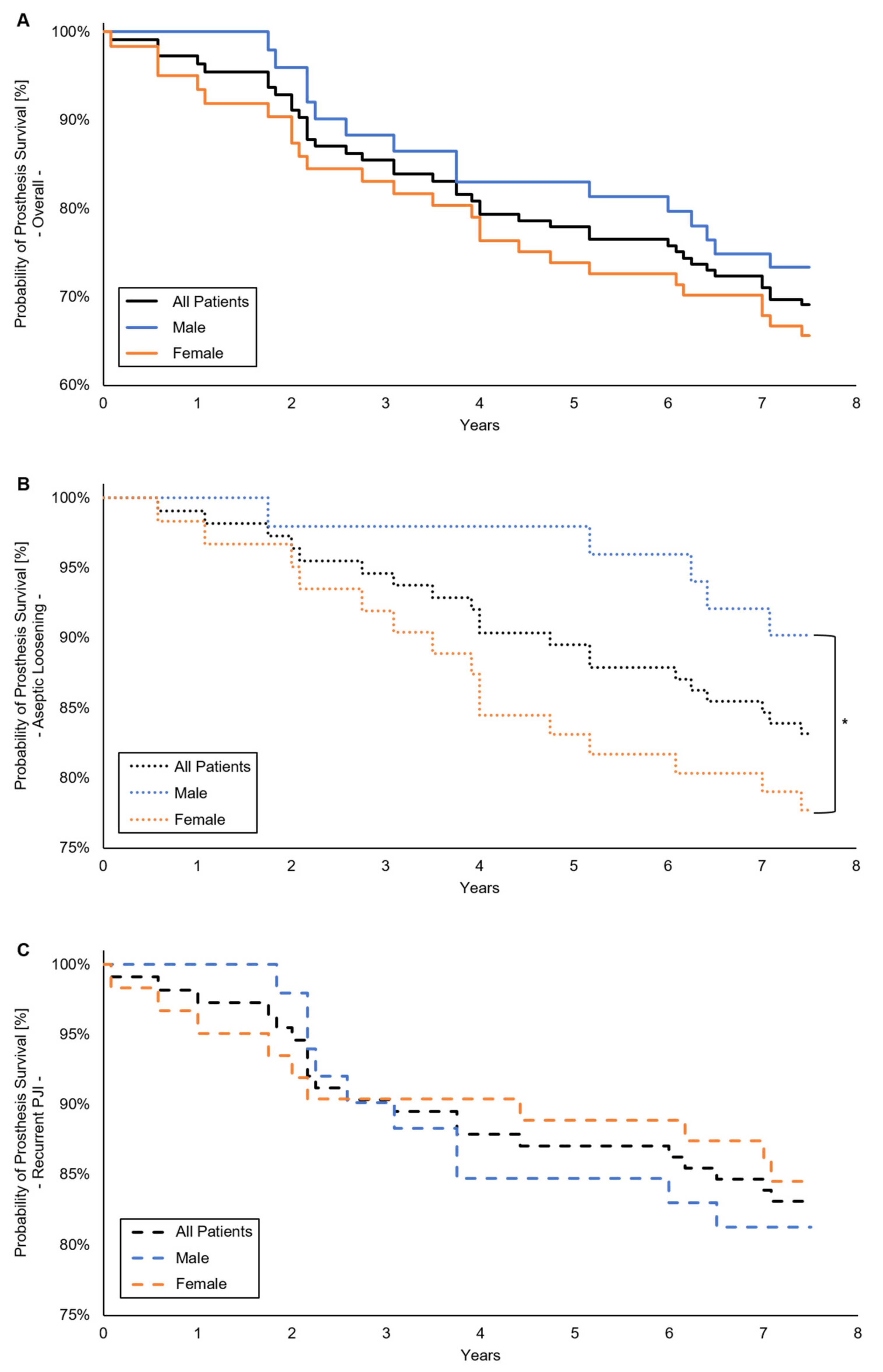
3.1. Prosthesis Survival
3.2. Patient Characteristics
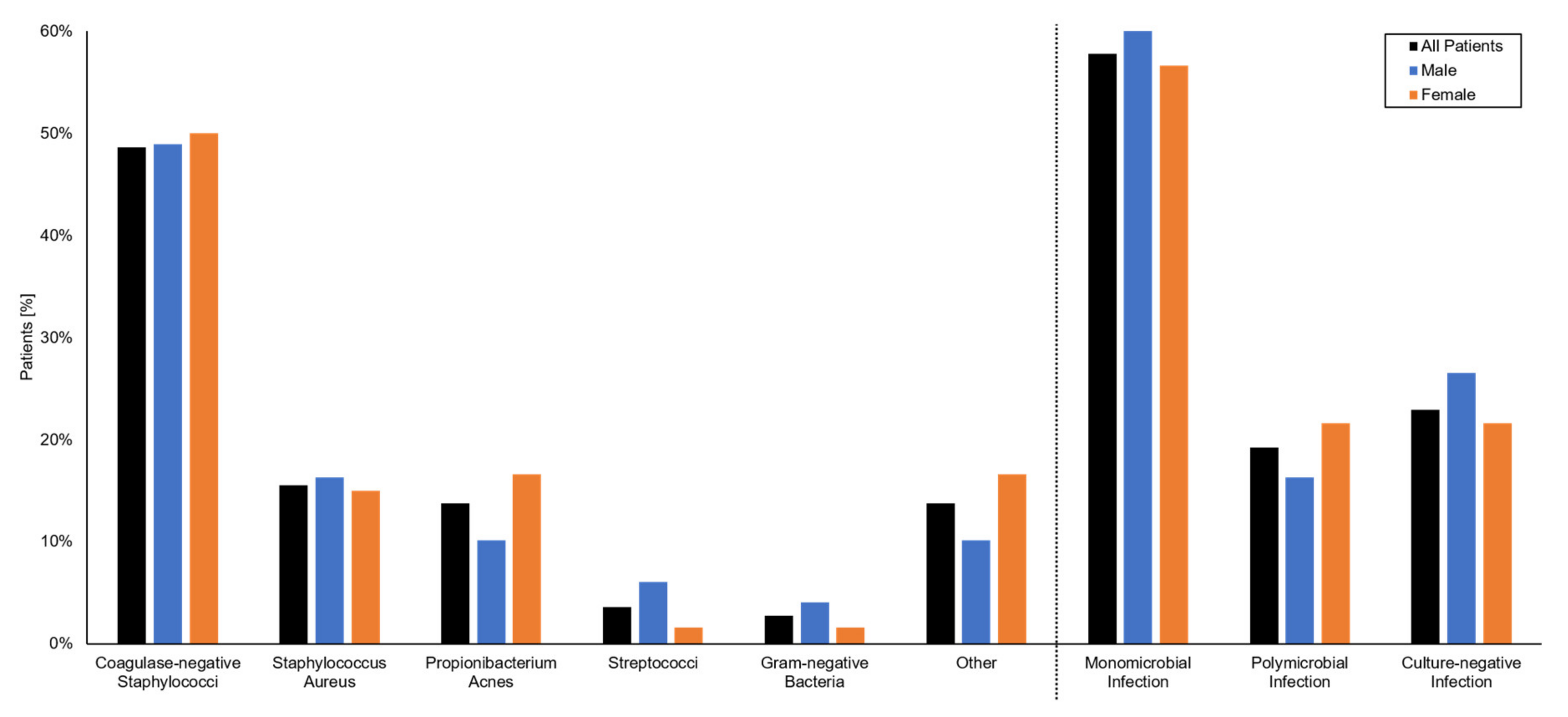
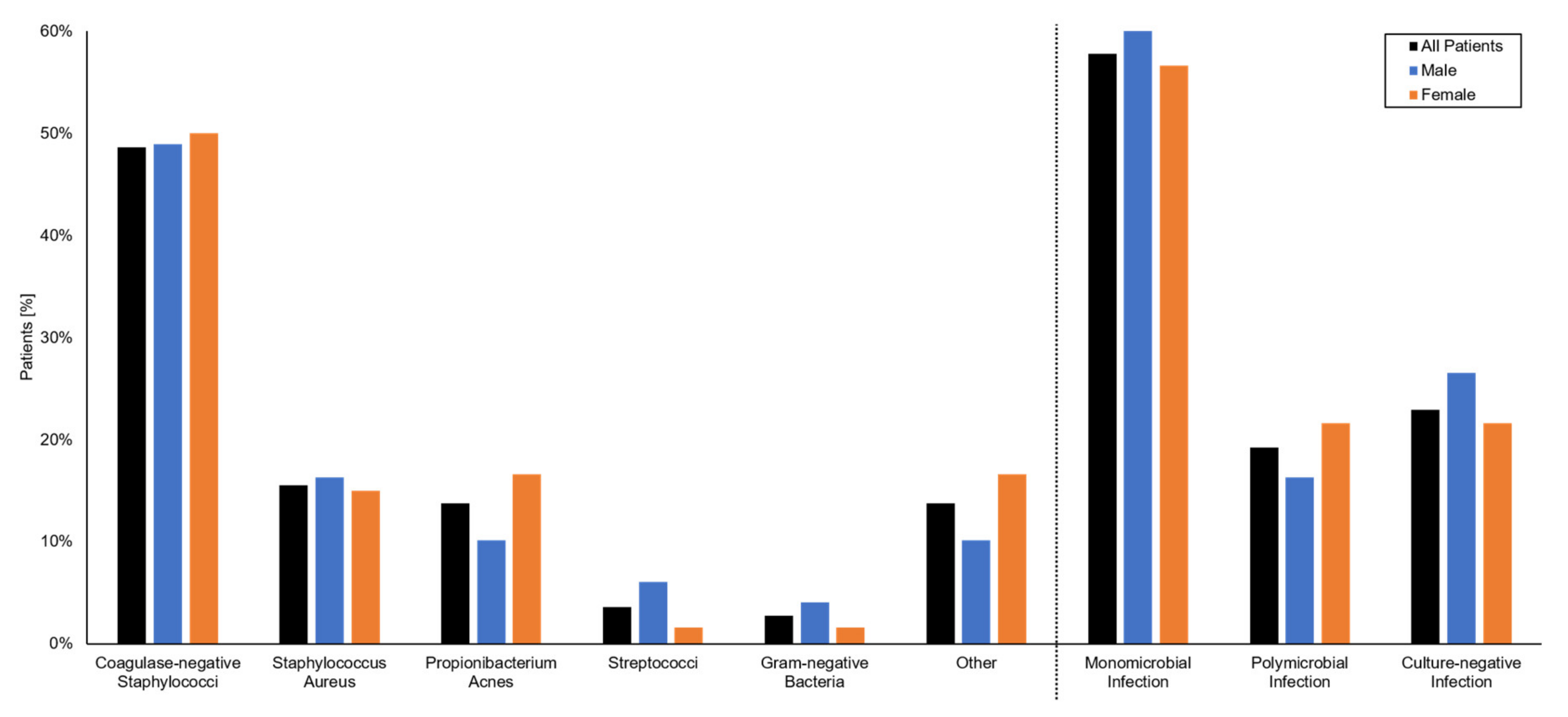
3.3. Microbiology
3.4. Laboratory and Pathology
3.5. Treatment
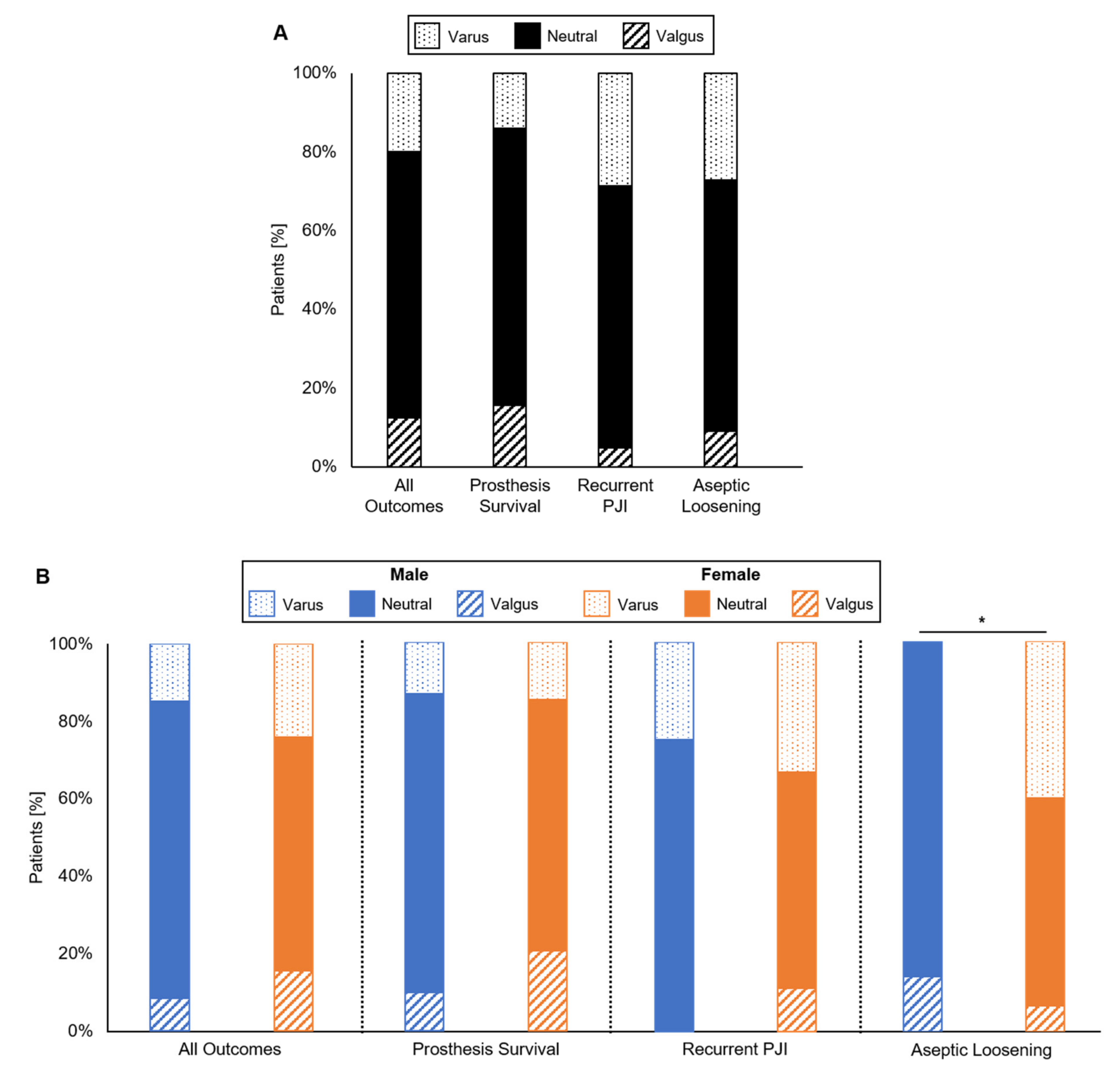
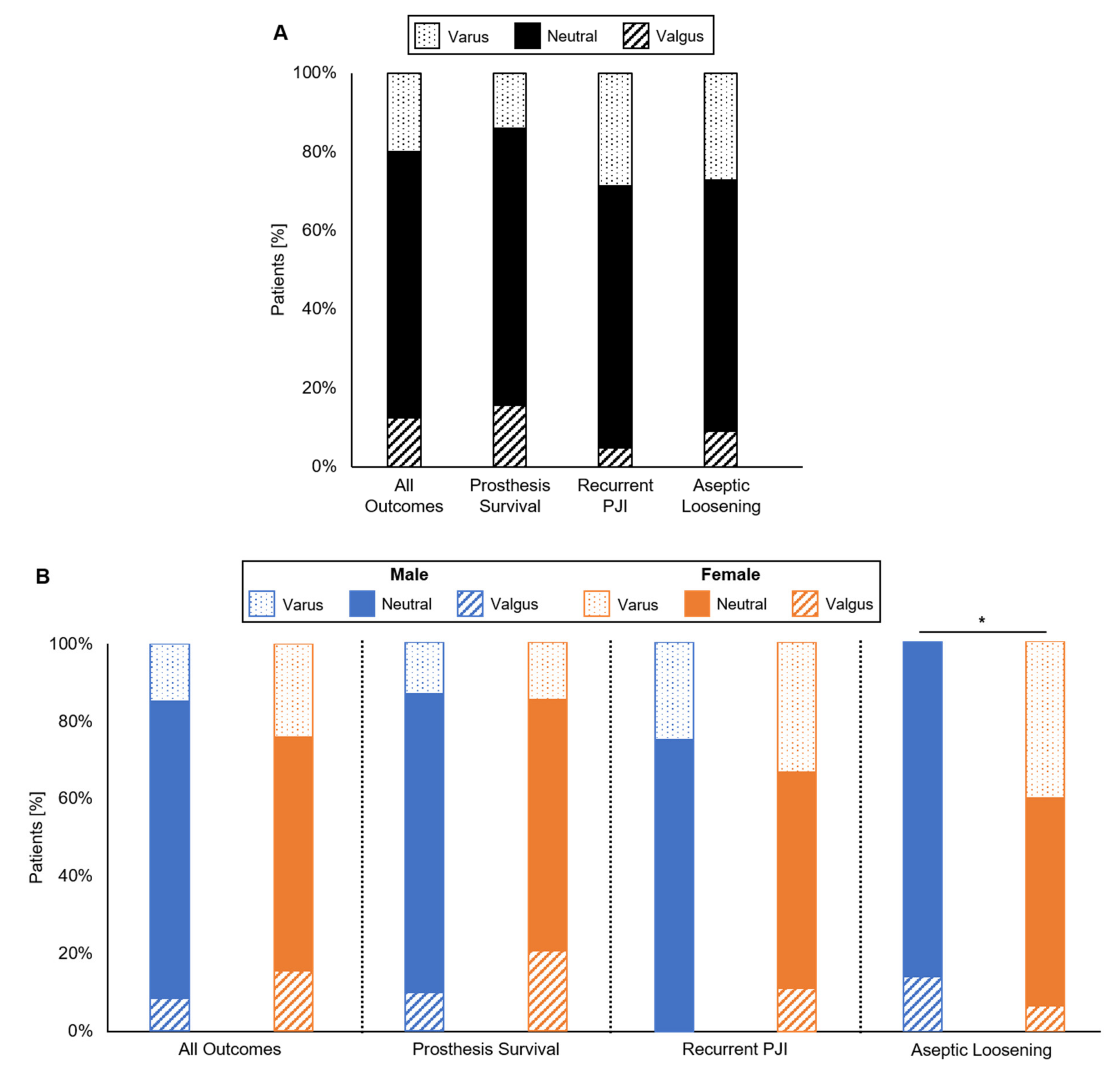
3.6. Coronal Alignment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kurtz, S.; Ong, K.; Schmier, J.; Mowat, F.; Saleh, K.; Dybvik, E.; Kärrholm, J.; Garellick, G.; Havelin, L.I.; Furnes, O.; et al. Future clinical and economic impact of revision total hip and knee arthroplasty. J. Bone Jt. Surg. 2007, 89, 144–151. [Google Scholar]
- Delanois, R.E.; Mistry, J.B.; Gwam, C.U.; Mohamed, N.S.; Choksi, U.S.; Mont, M.A. Current Epidemiology of Revision Total Knee Arthroplasty in the United States. J. Arthroplast. 2017, 32, 2663–2668. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.M.; Lau, E.; Schmier, J.; Ong, K.L.; Zhao, K.; Parvizi, J. Infection Burden for Hip and Knee Arthroplasty in the United States. J. Arthroplast. 2008, 23, 984–991. [Google Scholar] [CrossRef]
- Insall, J.N.; Thompson, F.M.; Brause, B.D. Two-stage reimplantation for the salvage of infected total knee arthroplasty. J. Bone Jt. Surg. Am. Vol. 1983, 65, 1087–1098. [Google Scholar] [CrossRef] [Green Version]
- Poss, R.; Thornhill, T.S.; Ewald, F.C.; Thomas, W.H.; Batte, N.J.; Sledge, C.B. Factors influencing the incidence and outcome of infection following total joint arthroplasty. Clin. Orthop. Relat. Res. 1984, 1984, 117–126. [Google Scholar] [CrossRef]
- Karczewski, D.; Winkler, T.; Renz, N.; Trampuz, A.; Lieb, E.; Perka, C.; Müller, M. A standardized interdisciplinary algorithm for the treatment of prosthetic joint infections. Bone Jt. J. 2019, 101, 132–139. [Google Scholar] [CrossRef]
- Blom, A.W.; Brown, J.; Taylor, A.H.; Pattison, G.; Whitehouse, S.L.; Bannister, G.C. Infection after total knee arthroplasty. J. Bone Jt. Surg. Br. Vol. 2004, 86, 688–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thiele, K.; Perka, C.; Matziolis, G.; Mayr, H.O.; Sostheim, M.; Hube, R. Current Failure Mechanisms After Knee Arthroplasty Have Changed: Polyethylene Wear Is Less Common in Revision Surgery. J. Bone Jt. Surg. Am. Vol. 2015, 97, 715–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urquhart, D.M.; Hanna, F.S.; Brennan, S.L.; Wluka, A.E.; Leder, K.; Cameron, P.A.; Graves, S.E.; Cicuttini, F.M. Incidence and Risk Factors for Deep Surgical Site Infection After Primary Total Hip Arthroplasty: A Systematic Review. J. Arthroplast. 2010, 25, 1216–1222. [Google Scholar] [CrossRef] [PubMed]
- Suarez, J.; Griffin, W.; Springer, B.; Fehring, T.; Mason, J.B.; Odum, S. Why Do Revision Knee Arthroplasties Fail? J. Arthroplast. 2008, 23, 99–103. [Google Scholar] [CrossRef]
- Kienzle, A.; Walter, S.; Von Roth, P.; Fuchs, M.; Winkler, T.; Müller, M. High Rates of Aseptic Loosening after Revision Total Knee Arthroplasty for Periprosthetic Joint Infection. JB JS open Access 2020, 5, e20.00026. [Google Scholar] [CrossRef]
- Johanson, N.A.; Bullough, P.G.; Wilson, P.D.; Salvati, E.A.; Ranawat, C.S. The microscopic anatomy of the bone-cement interface in failed total hip arthroplasties. Clin. Orthop. Relat. Res. 1987, 1987, 123–135. [Google Scholar] [CrossRef]
- Calton, T.F.; Fehring, T.K.; Griffin, W.L. Bone Loss Associated with the Use of Spacer Blocks in Infected Total Knee Arthroplasty. Clin. Orthop. Relat. Res. 1997, 345, 148–154. [Google Scholar] [CrossRef]
- Haleem, A.A.; Berry, D.J.; Hanssen, A.D. The Chitranjan Ranawat Award: Mid-Term to Long-Term Followup of Two-stage Reimplantation for Infected Total Knee Arthroplasty. Clin. Orthop. Relat. Res. 2004, 428, 35–39. [Google Scholar] [CrossRef]
- Russell, K.A.; Palmieri, R.M.; Zinder, S.M.; Ingersoll, C.D. Sex differences in valgus knee angle during a single-leg drop jump. J. Athl. Train. 2006, 41, 166–171. [Google Scholar] [PubMed]
- Nguyen, A.-D.; Shultz, S.J. Sex Differences in Clinical Measures of Lower Extremity Alignment. J. Orthop. Sports Phys. Ther. 2007, 37, 389–398. [Google Scholar] [CrossRef]
- Thomsen, M.G.; Husted, H.; Bencke, J.; Curtis, D.; Holm, G.; Troelsen, A. Do we need a gender-specific total knee replacement? A randomised controlled trial comparing a high-flex and a gender-specific posterior design. J. Bone Jt. Surg. Br. 2012, 94, 787–792. [Google Scholar] [CrossRef] [PubMed]
- Xie, X.; Lin, L.; Zhu, B.; Lu, Y.; Lin, Z.; Li, Q. Will gender-specific total knee arthroplasty be a better choice for women? A systematic review and meta-analysis. Eur. J. Orthop. Surg. Traumatol. 2013, 24, 1341–1349. [Google Scholar] [CrossRef]
- Ochsner, P.E.; Borens, O.; Bodler, P.-M. Infections of the Musculoskeletal System: Basic Principles, Prevention, Diagnosis and Treatment; Swiss Orthopaedics in-House-Publisher: Grandvaux, Switzerland, 2014. [Google Scholar]
- Diaz-Ledezma, C.; Higuera, C.A.; Parvizi, J. Success after Treatment of Periprosthetic Joint Infection: A Delphi-based International Multidisciplinary Consensus. Clin. Orthop. Relat. Res. 2013, 471, 2374–2382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmerli, W.; Trampuz, A.; Ochsner, P.E. Prosthetic-Joint Infections. N. Engl. J. Med. 2004, 351, 1645–1654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmerli, W.; Moser, C. Pathogenesis and treatment concepts of orthopaedic biofilm infections. FEMS Immunol. Med. Microbiol. 2012, 65, 158–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ewald, F.C. The Knee Society total knee arthroplasty roentgenographic evaluation and scoring system. Clin. Orthop. Relat. Res. 1989, 1989, 9–12. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, M.H.; Mekhail, A.O. The Failed Total Knee Arthroplasty: Evaluation and Etiology. J. Am. Acad. Orthop. Surg. 2004, 12, 436–446. [Google Scholar] [CrossRef]
- Hsu, R.W.; Himeno, S.; Coventry, M.B.; Chao, E.Y. Normal axial alignment of the lower extremity and load-bearing distribution at the knee. Clin. Orthop. Relat. Res. 1990, 1990, 215–227. [Google Scholar] [CrossRef]
- Manninen, P.; Riihimäki, H.; Heliövaara, M.; Mäkelä, P. Overweight, gender and knee osteoarthritis. Int. J. Obes. Relat. Metab. Disord. J. Int. Assoc. Study Obes. 1996, 20, 595–597. [Google Scholar]
- Chin, K.R.; Dalury, D.F.; Zurakowski, D.; Scott, R.D. Intraoperative measurements of male and female distal femurs during primary total knee arthroplasty. J. Knee Surg. 2002, 15, 213–217. [Google Scholar] [PubMed]
- Dargel, J.; Michael, J.W.; Feiser, J.; Ivo, R.; Koebke, J. Human Knee Joint Anatomy Revisited: Morphometry in the Light of Sex-Specific Total Knee Arthroplasty. J. Arthroplast. 2011, 26, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Rönn, K.; Reischl, N.; Gautier, E.; Jacobi, M. Current Surgical Treatment of Knee Osteoarthritis. Arthritis 2011, 2011, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Kastner, N.; Aigner, B.A.; Meikl, T.; Friesenbichler, J.; Wolf, M.; Glehr, M.; Gruber, G.; Leithner, A.; Sadoghi, P. Gender-specific outcome after implantation of low-contact-stress mobile-bearing total knee arthroplasty with a minimum follow-up of ten years. Int. Orthop. 2014, 38, 2489–2493. [Google Scholar] [CrossRef] [PubMed]
- Ritter, M.A.; Wing, J.T.; Berend, M.E.; Davis, K.E.; Meding, J.B. The Clinical Effect of Gender on Outcome of Total Knee Arthroplasty. J. Arthroplast. 2008, 23, 331–336. [Google Scholar] [CrossRef]
- Schiffner, E.; Latz, D.; Thelen, S.; Grassmann, J.P.; Karbowski, A.; Windolf, J.; Jungbluth, P.; Schneppendahl, J. Aseptic Loosening after THA and TKA- Do gender, tobacco use and BMI have an impact on implant survival time? J. Orthop. 2019, 16, 269–272. [Google Scholar] [CrossRef] [PubMed]
- Pun, S.Y.; Ries, M.D. Effect of Gender and Preoperative Diagnosis on Results of Revision Total Knee Arthroplasty. Clin. Orthop. Relat. Res. 2008, 466, 2701–2705. [Google Scholar] [CrossRef] [Green Version]
- Abele, J.T.; Swami, V.G.; Russell, G.; Masson, E.C.; Flemming, J.P. The Accuracy of Single Photon Emission Computed Tomography/Computed Tomography Arthrography in Evaluating Aseptic Loosening of Hip and Knee Prostheses. J. Arthroplast. 2015, 30, 1647–1651. [Google Scholar] [CrossRef]
- Nelson, C.L.; McLaren, A.C.; McLaren, S.G.; Johnson, J.W.; Smeltzer, M.S. Is aseptic loosening truly aseptic? Clin. Orthop. Relat. Res. 2005, 437, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Kempthorne, J.T.; Ailabouni, R.; Raniga, S.; Hammer, D.; Hooper, G. Occult Infection in Aseptic Joint Loosening and the Diagnostic Role of Implant Sonication. BioMed Res. Int. 2015, 2015, 946215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sundfeldt, M.; Carlsson, L.V.; Johansson, C.B.; Thomsen, P.; Gretzer, C. Aseptic loosening, not only a question of wear: A review of different theories. Acta Orthop. 2006, 77, 177–197. [Google Scholar] [CrossRef] [PubMed]
- Gallo, J.; Goodman, S.; Konttinen, Y.; Wimmer, M.; Holinka, M. Osteolysis around total knee arthroplasty: A review of pathogenetic mechanisms. Acta Biomater. 2013, 9, 8046–8058. [Google Scholar] [CrossRef] [Green Version]
- Schmalzried, T.P.; Kwong, L.M.; Jasty, M.; Sedlacek, R.C.; Haire, T.C.; O’Connor, D.O.; Bragdon, C.R.; Kabo, J.M.; Malcolm, A.J.; Harris, W.H. The mechanism of loosening of cemented acetabular components in total hip arthroplasty. Analysis of specimens retrieved at autopsy. Clin. Orthop. Relat. Res. 1992, 1992, 60–78. [Google Scholar]
- Howie, D.W.; Vernon-Roberts, B.; Oakeshott, R.; Manthey, B. A rat model of resorption of bone at the cement-bone interface in the presence of polyethylene wear particles. J. Bone Jt. Surg. Am. Vol. 1988, 70, 257–263. [Google Scholar] [CrossRef]
- Mirra, J.M.; Marder, R.A.; Amstutz, H.C. The pathology of failed total joint arthroplasty. Clin. Orthop. Relat. Res. 1982, 1982, 175–183. [Google Scholar] [CrossRef]
- Reinke, S.; Geissler, S.; Taylor, W.R.; Schmidt-Bleek, K.; Juelke, K.; Schwachmeyer, V.; Dahne, M.; Hartwig, T.; Akyüz, L.; Meisel, C.; et al. Terminally Differentiated CD8+ T Cells Negatively Affect Bone Regeneration in Humans. Sci. Transl. Med. 2013, 5, 177ra36. [Google Scholar] [CrossRef] [PubMed]
- Kienzle, A.; Servais, A.B.; Ysasi, A.B.; Gibney, B.C.; Valenzuela, C.D.; Wagner, W.L.; Ackermann, M.; Mentzer, S.J. Free-Floating Mesothelial Cells in Pleural Fluid After Lung Surgery. Front. Med. 2018, 5, 89. [Google Scholar] [CrossRef] [Green Version]
- Henry, Y.M.; Eastell, R. Ethnic and Gender Differences in Bone Mineral Density and Bone Turnover in Young Adults: Effect of Bone Size. Osteoporos. Int. 2000, 11, 512–517. [Google Scholar] [CrossRef]
- Jabbar, S.; Drury, J.; Fordham, J.N.; Datta, H.K.; Francis, R.M.; Tuck, S.P. Osteoprotegerin, RANKL and bone turnover in postmenopausal osteoporosis. J. Clin. Pathol. 2011, 64, 354–357. [Google Scholar] [CrossRef]
- Nevitt, M.C.; Felson, D.T. Sex hormones and the risk of osteoarthritis in women: Epidemiological evidence. Ann. Rheum. Dis. 1996, 55, 673–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papastavrou, A.; Schmidt, I.; Deng, K.; Steinmann, P. On age-dependent bone remodeling. J. Biomech. 2020, 103, 109701. [Google Scholar] [CrossRef]
- Jeffery, R.S.; Morris, R.W.; Denham, R.A. Coronal alignment after total knee replacement. J. Bone Jt. Surg. Br. Vol. 1991, 73, 709–714. [Google Scholar] [CrossRef] [PubMed]
- Fang, D.M.; Ritter, M.A.; Davis, K.E. Coronal alignment in total knee arthroplasty: Just how important is it? J. Arthroplast. 2009, 24, 39–43. [Google Scholar] [CrossRef]
- Slevin, O.; Hirschmann, A.; Schiapparelli, F.F.; Amsler, F.; Huegli, R.W.; Hirschmann, M.T. Neutral alignment leads to higher knee society scores after total knee arthroplasty in preoperatively non-varus patients: A prospective clinical study using 3D-CT. Knee Surg. Sports Traumatol. Arthrosc. 2017, 26, 1602–1609. [Google Scholar] [CrossRef] [PubMed]
- Morgan, S.S.; Bonshahi, A.; Pradhan, N.; Gregory, A.; Gambhir, A.; Porter, M.L. The influence of postoperative coronal alignment on revision surgery in total knee arthroplasty. Int. Orthop. 2007, 32, 639–642. [Google Scholar] [CrossRef] [Green Version]
- Salim, X.; Lopez, D.; Jeys, L.; Smith, R.C. Cones and sleeves in knee arthroplasty: A narrative review. Curr. Orthop. Pr. 2019, 30, 520–525. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Descriptive | All Outcomes | Prosthesis Survival | Aseptic Loosening | Recurrent PJI | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All Patients | Male | Female | p Value | Male | Female | p Value | Male | Female | p Value | Male | Female | p Value | |
| Count [number] | 109 | 49 | 60 | - | 32 | 35 | - | 7 | 15 | - | 12 | 10 | - |
| Age [years] | 69.1 ± 10.3 | 68.2 ± 10.0 | 69.9 ± 10.5 | 0.401 | 69.0 ± 11.1 | 69.1 ± 11.3 | 0.969 | 66.8 ± 6.7 | 68.7 ± 10.0 | 0.872 | 67.1 ± 7.2 | 74.2 ± 5.7 | 0.025 |
| Follow-Up Time [months] | 39.3 ± 24.5 | 37.3 ± 24.4 | 41.0 ± 24.5 | 0.362 | 32.0 ± 23.8 | 40.9 ± 23.5 | 0.135 | 56.7 ± 23.3 | 45.7 ± 23.1 | 0.266 | 40.6 ± 17.9 | 38.4 ± 30.4 | 0.844 |
| >1 Comorbidity | 96.3% (105) | 93.9% (46) | 98.3% (59) | - | 93.8% (30) | 97.1% (34) | - | 100.0% (7) | 100.0% (15) | - | 91.7% (11) | 100.0% (10) | - |
| Number of Prior Surgeries on Affected Knee [Count] | 3.5 ± 3.0 | 3.5 ± 3.5 | 3.5 ± 3.5 | 0.935 | 3.1 ± 2.0 | 3.5 ± 4.3 | 0.692 | 4.7 ± 2.0 | 4.3 ± 3.7 | 0.655 | 4.3 ± 2.1 | 2.6 ± 1.9 | 0.082 |
| Clinical Scores | |||||||||||||
| BMI | 31.3 ± 6.9 | 30.2 ± 5.7 | 32.2 ± 7.7 | 0.141 | 29.7 ± 5.6 | 32.8 ± 8.2 | 0.080 | 30.5 ± 4.4 | 30.8 ± 7.5 | 0.115 | 32.3 ± 6.6 | 31.9 ± 5.0 | 0.903 |
| CCI | 4.3 ± 2.5 | 4.4 ± 2.6 | 4.3 ± 2.3 | 0.943 | 4.5 ± 2.9 | 4.1 ± 2.3 | 0.550 | 3.7 ± 2.2 | 4.5 ± 2.4 | 0.807 | 4.6 ± 1.8 | 5.0 ± 2.4 | 0.660 |
| ASA1 [%] (No. of Patients) | 8.3% (9) | 12.2% (6) | 5.0% (3) | 0.190 | 12.5% (4) | 5.7% (2) | 0.285 | 0.0% (0) | 0.0% (0) | - | 16.7% (2) | 10.0% (1) | 0.450 |
| ASA2 [%] (No. of Patients) | 43.1% (47) | 42.9% (21) | 43.3% (26) | 0.970 | 46.9% (15) | 60.0% (21) | 0.692 | 28.6% (2) | 26.7% (4) | 0.567 | 33.3% (4) | 10.0% (1) | 0.115 |
| ASA3 [%] (No. of Patients) | 48.6% (53) | 44.9% (22) | 51.7% (31) | 0.614 | 40.6% (13) | 34.3% (12) | 0.479 | 71.4% (5) | 73.3% (11) | 0.270 | 50.0% (6) | 80.0% (8) | 0.875 |
| Descriptive | All Outcomes | Prosthesis Survival | Aseptic Loosening | Recurrent PJI | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All Patients | Male | Female | p Value | Male | Female | p Value | Male | Female | p Value | Male | Female | p Value | |
| Length [Days] | |||||||||||||
| Stay for Prosthesis Removal | 19.4 ± 13.5 | 20.7 ± 16.7 | 18.3 ± 10.0 | 0.365 | 21.8 ± 19.6 | 19.0 ± 12.3 | 0.502 | 19.8 ± 18.4 | 16.7 ± 10.8 | 0.338 | 17.1 ± 4.1 | 18.0 ± 3.3 | 0.655 |
| Interval between Surgeries | 70.9 ± 51.5 | 73.2 ± 63.1 | 69.0 ± 39.6 | 0.678 | 71.2 ± 70.0 | 66.7 ± 38.5 | 0.745 | 87.1 ± 68.1 | 57.5 ± 34.4 | 0.368 | 67.5 ± 34.9 | 94.7 ± 51.9 | 0.178 |
| Stay for Prosthesis Reimplantation | 18.0 ± 17.3 | 17.1 ± 11.5 | 18.8 ± 21.0 | 0.553 | 16.7 ± 11.9 | 17.3 ± 13.1 | 0.840 | 19.0 ± 11.1 | 14.6 ± 11.4 | 0.806 | 18.5 ± 12.4 | 31.4 ± 44.5 | 0.321 |
| Stay total | 33.8 ± 15.9 | 35.7 ± 19.3 | 32.3 ± 12.1 | 0.841 | 35.0 ± 20.9 | 34.3 ± 13.6 | 0.880 | 38.7 ± 20.3 | 29.1 ± 12.6 | 0.419 | 36.4 ± 13.9 | 29.6 ± 8.2 | 0.568 |
| Number of Revision Surgeries on Affected Knee [Count] | 0.8 ± 1.1 | 0.9 ± 0.9 | 0.7 ± 0.7 | 0.580 | 0.2 ± 0.5 | 0.3 ± 0.6 | 0.644 | 1.7 ± 0.9 | 1.1 ± 0.7 | 0.846 | 2.3 ± 1.4 | 1.8 ± 1.6 | 0.441 |
| Surgical Strategy [%] (No. of Patients) | |||||||||||||
| Two-stage Exchange | 84.4% (92) | 81.6% (40) | 86.7% (52) | 0.776 | 78.1% (25) | 85.7% (30) | 0.732 | 85.7% (6) | 93.3% (14) | 0.860 | 91.7% (11) | 80.0% (8) | 0.769 |
| Multiple-stage Exchange | 15.6% (17) | 18.4% (9) | 13.3% (8) | 0.508 | 21.9% (7) | 14.3% (5) | 0.463 | 14.3% (1) | 6.7% (1) | 0.580 | 8.3% (1) | 20.0% (2) | 0.461 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kienzle, A.; Walter, S.; Palmowski, Y.; Kirschbaum, S.; Biedermann, L.; von Roth, P.; Perka, C.; Müller, M. Influence of Gender on Occurrence of Aseptic Loosening and Recurrent PJI after Revision Total Knee Arthroplasty. Osteology 2021, 1, 92-104. https://0-doi-org.brum.beds.ac.uk/10.3390/osteology1020010
Kienzle A, Walter S, Palmowski Y, Kirschbaum S, Biedermann L, von Roth P, Perka C, Müller M. Influence of Gender on Occurrence of Aseptic Loosening and Recurrent PJI after Revision Total Knee Arthroplasty. Osteology. 2021; 1(2):92-104. https://0-doi-org.brum.beds.ac.uk/10.3390/osteology1020010
Chicago/Turabian StyleKienzle, Arne, Sandy Walter, Yannick Palmowski, Stephanie Kirschbaum, Lara Biedermann, Philipp von Roth, Carsten Perka, and Michael Müller. 2021. "Influence of Gender on Occurrence of Aseptic Loosening and Recurrent PJI after Revision Total Knee Arthroplasty" Osteology 1, no. 2: 92-104. https://0-doi-org.brum.beds.ac.uk/10.3390/osteology1020010