
Prevalence and Patterns of Risk of Osteoporosis in Bangladeshi Adult Population: An Analysis of Calcaneus Quantitative Ultrasound Measurements



Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Anthropometric Data
2.3. Sociodemographic and Reproductive Health Data
2.4. Quantitative Bone Density
2.5. Statistical Analysis
3. Results
3.1. Sociodemographic and Clinical Data
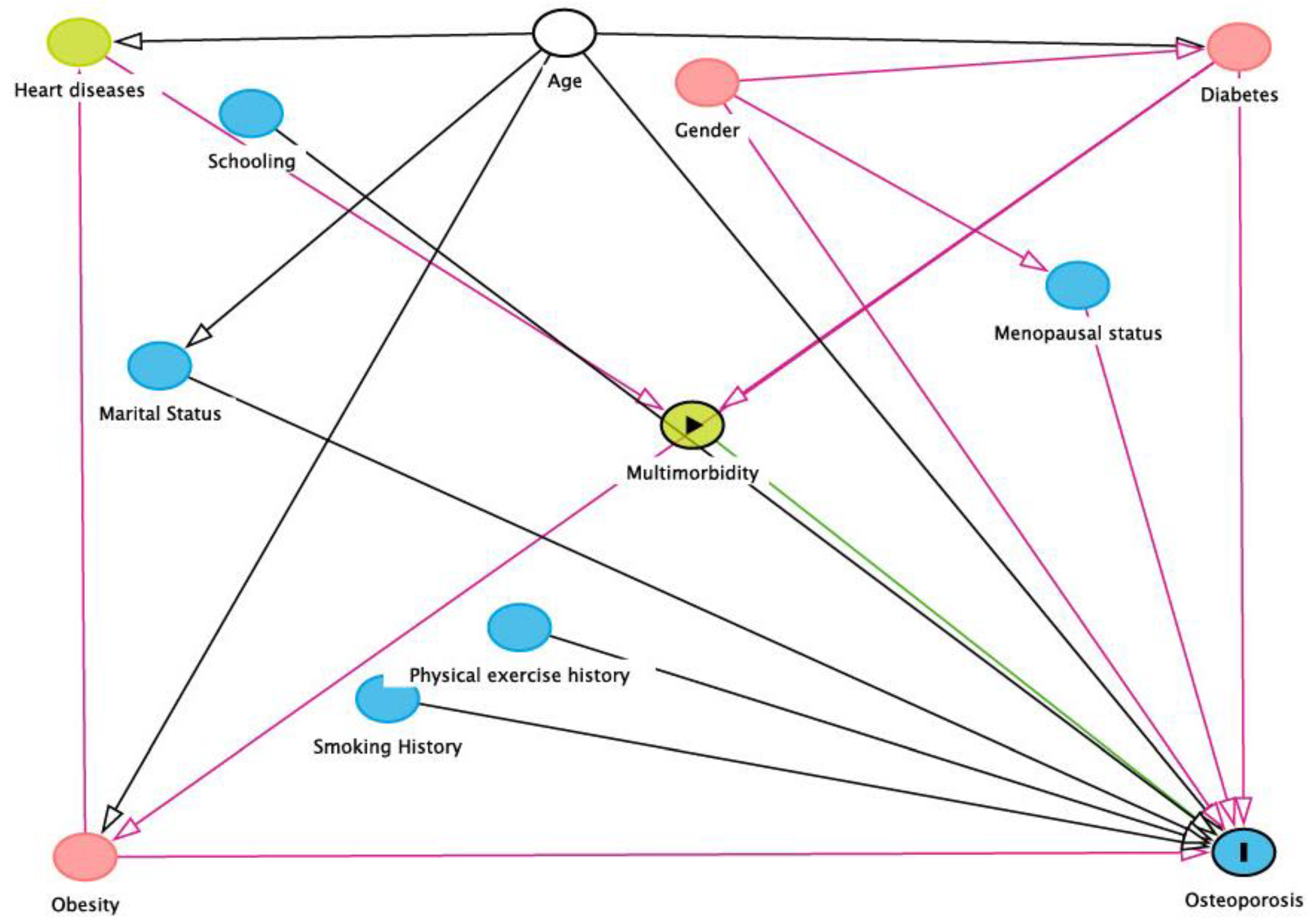
3.2. Variables Associated with the RO
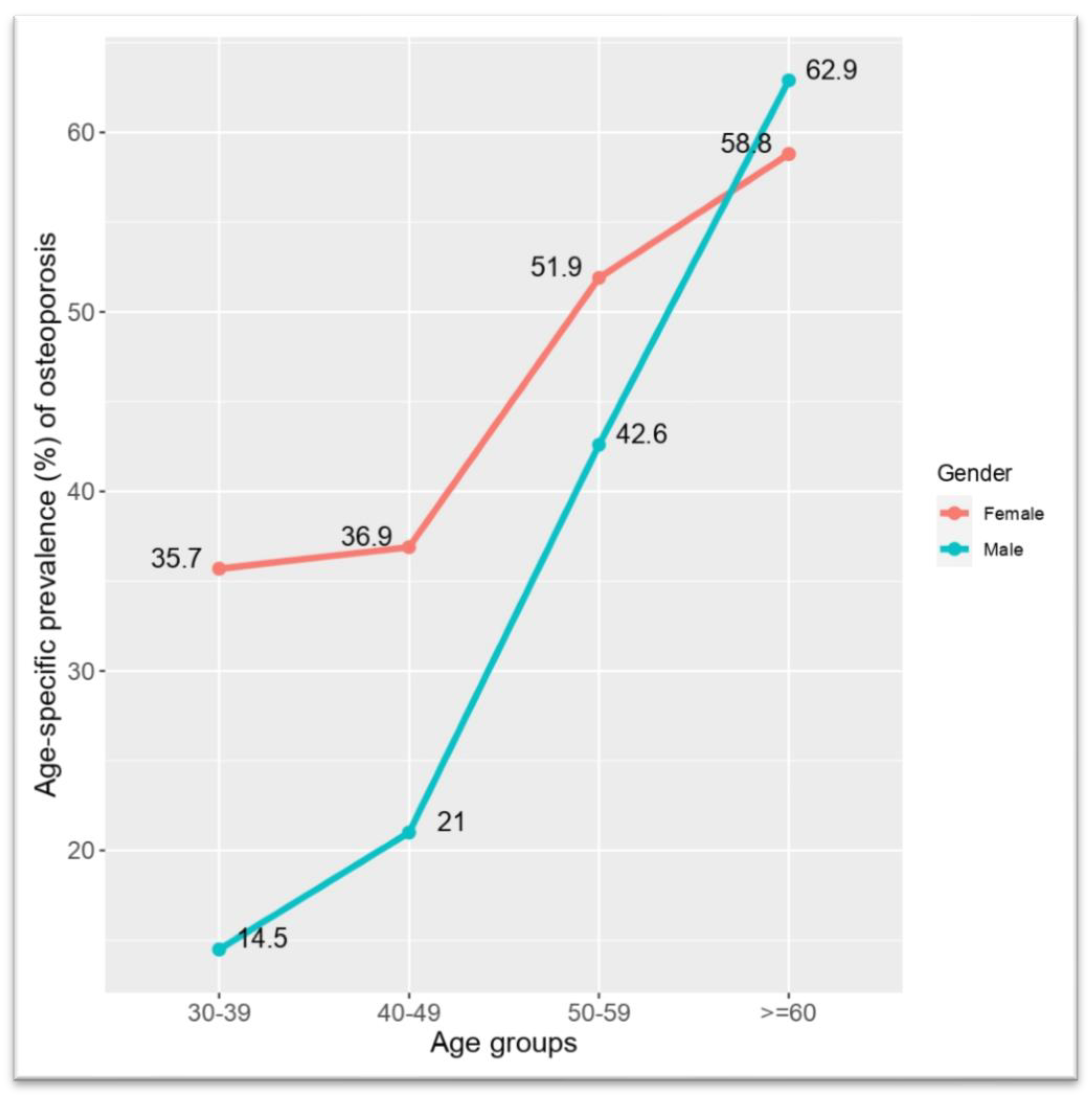
3.3. Age, Gender, and Osteoporosis Prevalence
3.4. Multivariable Linear Regression Models
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| RO | Risk of Osteoporosis; |
| ORF | Osteoporosis-Related Fractures |
| DXA | Dual-energy X-ray absorptiometry |
| QUS | Qualitative Ultrasound |
| BMI | Body Mass Index |
| BUA | Broadband Ultrasonic Attenuation; |
| REC | Research Ethics Committee |
References
- Sozen, T.; Ozisik, L.; Calik Basaran, N. An overview and management of osteoporosis. Eur. J. Rheumatol. 2017, 4, 46–56. [Google Scholar] [CrossRef]
- Wright, N.C.; Looker, A.C.; Saag, K.G.; Curtis, J.R.; Delzell, E.S.; Randall, S.; Dawson-Hughes, B. The Recent Prevalence of Osteoporosis and Low Bone Mass in the United States Based on Bone Mineral Density at the Femoral Neck or Lumbar Spine. J. Bone Miner. Res. 2014, 29, 2520–2526. [Google Scholar] [CrossRef] [Green Version]
- Kling, J.M.; Clarke, B.L.; Sandhu, N.P. Osteoporosis Prevention, Screening, and Treatment: A Review. J. Women's Health 2014, 23, 563–572. [Google Scholar] [CrossRef]
- Khan, A.H.; Jafri, L.; Ahmed, S.; Noordin, S. Osteoporosis and its perspective in Pakistan: A review of evidence and issues for addressing fragility fractures. Ann. Med. Surg. 2018, 29, 19–25. Available online: www.elsevier.com/locate/amsu (accessed on 5 January 2020). [CrossRef] [PubMed]
- Vondracek, S.F. Diagnosis and management of osteoporosis in the older senior. Clin. Interv. Aging. 2009, 4, 121. Available online: http://www.dovepress.com/diagnosis-and-management-of-osteoporosis-in-the-older-senior-peer-reviewed-article-CIA (accessed on 5 January 2020). [CrossRef] [PubMed] [Green Version]
- Nuti, R.; Brandi, M.L.; Checchia, G.; Di Munno, O.; Dominguez, L.; Falaschi, P.; Fiore, C.E.; Iolascon, G.; Maggi, S.; Michieli, R.; et al. Guidelines for the management of osteoporosis and fragility fractures. Intern. Emerg. Med. 2018, 14, 85–102. [Google Scholar] [CrossRef] [Green Version]
- Leibson, C.L.; ScD, A.N.A.T.; Gabriel, S.E.; Bs, J.E.R.; Melton, L.J. Mortality, Disability, and Nursing Home Use for Persons with and without Hip Fracture: A Population-Based Study. J. Am. Geriatr. Soc. 2002, 50, 1644–1650. [Google Scholar] [CrossRef]
- Vochteloo, A.J.H.; Van Vliet-Koppert, S.T.; Maier, A.; Tuinebreijer, W.E.; Röling, M.L.; De Vries, M.R.; Bloem, R.M.; Nelissen, R.; Pilot, P. Risk factors for failure to return to the pre-fracture place of residence after hip fracture: A prospective longitudinal study of 444 patients. Arch. Orthop. Trauma Surg. 2012, 132, 823–830. [Google Scholar] [CrossRef] [Green Version]
- Rajendran, K.; Suthakaran, P.K.; Nair, L.; Rajaram, L.; Kalappan, M.; Sivanesan, M. Evaluation of osteoporosis using calcaneal QUS and FRAX score as a screening tool in a semi urban tertiary care hospital of South India. Int. J. Adv. Med. 2015, 341–345. [Google Scholar] [CrossRef]
- Steiner, B.; Dimai, H.P.; Steiner, H.; Cirar, S.; Fahrleitner-Pammer, A. Prescreening for Osteoporosis With Quantitative Ultra-sound in Postmenopausal White Women. J. Ultrasound Med. 2019, 38, 1553–1559. [Google Scholar] [CrossRef] [Green Version]
- Prastowo, N.A.; Ali, S.; Haryono, I.R. A Population-based Study on Bone Mineral Density Using Dual-Energy X-Ray Absorp-tiometry (DEXA) in Postmenopausal Women in Jakarta, Indonesia. Int J. Osteoporos Metab Disord. 2018, 11, 1–6. [Google Scholar] [CrossRef]
- Chin, K.-Y.; Ima-Nirwana, S. Calcaneal Quantitative Ultrasound as a Determinant of Bone Health Status: What Properties of Bone Does It Reflect? Int. J. Med. Sci. 2013, 10, 1778–1783. Available online: http://www.medsci.org1778 (accessed on 22 December 2019). [CrossRef] [Green Version]
- Burke, É.; Carroll, R.; ‘O’Dwyer, M.; Walsh, J.B.; McCallion, P.; McCarron, M. Quantitative examination of the bone health status of older adults with intellectual and developmental disability in Ireland: A cross-sectional nationwide study. BMJ Open 2019, 9, e026939. Available online: http://0-bmjopen-bmj-com.brum.beds.ac.uk/ (accessed on 22 December 2019). [CrossRef]
- Frost, M.L.; Blake, G.M.; Fogelman, I. Quantitative Ultrasound and Bone Mineral Density Are Equally Strongly Associated with Risk Factors for Osteoporosis. J. Bone Miner. Res. 2001, 16, 406–416. [Google Scholar] [CrossRef]
- Rhee, Y.; Lee, J.; Jung, J.Y.; Lee, J.E.; Park, S.Y.; Kim, Y.M.; Lee, S.; Choi, H.S.; Kim, S.H.; Lim, S.-K. Modifications of T-Scores by Quantitative Ultrasonography for the Diagnosis of Osteoporosis in Koreans. J. Korean Med. Sci. 2009, 24, 232–236. [Google Scholar] [CrossRef]
- Moayyeri, A.; Adams, J.E.; Adler, R.A.; Krieg, M.-A.; Hans, D.; Compston, J.; Lewiecki, E.M. Quantitative ultrasound of the heel and fracture risk assessment: An updated meta-analysis. Osteoporos. Int. 2011, 23, 143–153. [Google Scholar] [CrossRef]
- Begum, S.M.; Begum, R.; Alam, R. Bone Mineral Density and Osteoporosis in Women of Rural and Urban Dwellers. Bangladesh J. Nucl. Med. 2017, 18, 39–42. [Google Scholar] [CrossRef] [Green Version]
- Misra, A. Ethnic-Specific Criteria for Classification of Body Mass Index: A Perspective for Asian Indians and American Diabetes Association Position Statement. Diabetes Technol. Ther. 2015, 17, 667–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navickas, R.; Petric, V.-K.; Feigl, A.B.; Seychell, M. Multimorbidity: What Do We Know? What Should We Do? J. Comorbidity 2016, 6, 4–11. [Google Scholar] [CrossRef] [PubMed]
- NIH State-of-the-Science Conference Statement on management of menopause-related symptoms. NIH Consens. State Sci. Statements 2005, 22, 1–38.
- Chan, M.Y.; Nguyen, N.D.; Center, J.R.; Eisman, J.A.; Nguyen, T.V. Quantitative ultrasound and fracture risk prediction in non-osteoporotic men and women as defined by WHO criteria. Osteoporos. Int. 2013, 24, 1015–1022. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/22878531 (accessed on 20 March 2020). [CrossRef]
- Kanis, J.A. Diagnosis of osteoporosis and assessment of fracture risk. Lancet 2002, 359, 1929–1936. [Google Scholar] [CrossRef]
- Kruger, M.C.; Todd, J.M.; Schollum, L.M.; Kuhn-Sherlock, B.; McLean, D.W.; Wylie, K. Bone health comparison in seven Asian coun-tries using calcaneal ultrasound. BMC Musculoskelet. Disord. 2013, 14, 81. Available online: http://0-www-biomedcentral-com.brum.beds.ac.uk/1471-2474/14/81 (accessed on 6 January 2020). [CrossRef] [PubMed] [Green Version]
- Lee, C.N.Y.; Lam, S.C.; Tsang, A.Y.K.; Ng, B.T.Y.; Leung, J.C.Y.; Chong, A.C.Y. Preliminary investigation on prevalence of osteoporosis and osteopenia: Should we tune our focus on healthy adults? Jpn. J. Nurs. Sci. 2014, 12, 232–248. [Google Scholar] [CrossRef] [PubMed]
- Black, D.M.; Rosen, C.J. Postmenopausal Osteoporosis. N. Engl. J. Med. 2016, 374, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Thulkar, J.; Singh, S.; Sharma, S.; Thulkar, T. Preventable risk factors for osteoporosis in postmenopausal women: Systematic review and meta-analysis. J. Mid-Life Health 2016, 7, 108. [Google Scholar] [CrossRef] [PubMed]
- Pasco, J.A.; Lane, S.E.; Brennan, S.L.; Timney, E.N.; Bucki-Smith, G.; Dobbins, A.G.; Nicholson, G.C.; Kotowicz, M.A. Fracture risk among older men: Osteopenia and osteoporosis defined using cut-points derived from female versus male reference data. Osteoporos. Int. 2013, 25, 857–862. [Google Scholar] [CrossRef]
- Bonnick, S.L. Osteoporosis in men and women. Clin. Cornerstone 2006, 8, 28–39. [Google Scholar] [CrossRef]
- Cawthon, P.M. Gender Differences in Osteoporosis and Fractures. Clin. Orthop. Relat. Res. 2011, 469, 1900–1905. [Google Scholar] [CrossRef] [Green Version]
- Kadam, N.; Chiplonkar, S.; Khadilkar, A.; Khadilkar, V. Prevalence of osteoporosis in apparently healthy adults above 40 years of age in Pune City, India. Indian J. Endocrinol Metab. 2018, 22, 67. [Google Scholar]
- Nelson, R.E.; Willson, T.; Nelson, S.; Newbold, J.; LaFleur, J. The clinical epidemiology of male osteoporosis: A review of the recent literature. Clin. Epidemiol. 2015, 7, 65–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiao, D.; Liu, X.; Tu, R.; Zhang, X.; Qian, X.; Zhang, H.; Jiang, J.; Tian, Z.; Wang, Y.; Dong, X.; et al. Gender-specific prevalence and influencing factors of osteopenia and osteoporosis in Chinese rural population: The Henan Rural Cohort Study. BMJ Open 2020, 10, e028593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, P.; Li, Z.; Hu, Y. Prevalence of osteoporosis in China: A meta-analysis and systematic review. BMC Public Health 2016, 16, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Khosla, S. Pathogenesis of Age-Related Bone Loss in Humans. Med. Sci. Cite J. J. Gerontol A Biol. Sci. Med. Sci. 2013, 68, 1226–1235. [Google Scholar] [CrossRef] [Green Version]
- Lane, N.E. Glucocorticoid-Induced Osteoporosis: New Insights into the Pathophysiology and Treatments. Curr. Osteoporos. Rep. 2019, 17, 1–7. [Google Scholar] [CrossRef]
- Alswat, K.A. Gender Disparities in Osteoporosis. J. Clin. Med. Res. 2017, 9, 382–387. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Sun, F.; Li, Y.; Tang, Z.; Ma, L. Multimorbidity in Community-Dwelling Older Adults in Beijing: Prevalence and Trends, 2004–2017. J. Nutr. Health Aging 2020, 25, 116–119. [Google Scholar] [CrossRef]
- Puth, M.-T.; Klaschik, M.; Schmid, M.; Weckbecker, K.; Münster, E. Prevalence and comorbidity of osteoporosis—A cross-sectional analysis on 10,660 adults aged 50 years and older in Germany. BMC Musculoskelet. Disord. 2018, 19, 144. [Google Scholar] [CrossRef]
- Farhat, G.N.; Cauley, J.A. The link between osteoporosis and cardiovascular disease. Clin. Cases Mineral. Bone Metabolism. 2008, 5, 19–34. [Google Scholar]
- Khan, T.S.; Fraser, L.A. Type 1 diabetes and osteoporosis: From molecular pathways to bone phenotype. J. Osteoporosis. 2015, 2015, 174186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Laet, C.; Kanis, J.A.; Odén, A.; Johanson, H.; Johnell, O.; Delmas, P.; Eisman, J.A.; Kroger, H.; Fujiwara, S.; Garnero, P.; et al. Body mass index as a predictor of fracture risk: A me-ta-analysis. Osteoporos. Int. 2005, 16, 1330–1338. [Google Scholar] [CrossRef] [PubMed]
- Strozyk, D.; Gress, T.M.; Breitling, L.P. Smoking and bone mineral density: Comprehensive analyses of the third National Health and Nutrition Examination Survey (NHANES III). Arch. Osteoporos. 2018, 13, 16. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Factors | Risk of Osteoporosis | Total (% within Total) | p-Value * | |
|---|---|---|---|---|
| No (%) | Yes (%) | |||
| All | 330 (62.7) | 196 (37.3) | 526 (100) | |
| Gender | 0.003 | |||
| Male | 168 (69.7) | 73 (30.3) | 241 (45.8) | |
| Female | 162 (56.8) | 123 (43.2) | 285 (54.2) | |
| Marital status | 1.000 | |||
| Married | 303 (62.7) | 180 (37.3) | 483 (91.8) | |
| Not married | 27 (62.7) | 16 (37.3) | 43 (8.2) | |
| Age (Years) | <0.001 | |||
| 30–39 | 145 (73.2) | 53 (26.8) | 198 (37.6) | |
| 40–49 | 90 (70.9) | 37 (29.1) | 127 (24.1) | |
| 50–59 | 61 (53.0) | 54 (47.0) | 115 (21.9) | |
| ≥60 | 34 (39.5) | 52 (60.5) | 86 (16.4) | |
| BMI | 0.397 | |||
| Underweight | 5 (45.5) | 6 (55.5) | 11 (2.1) | |
| Normal | 149 (65.9) | 77 (34.1) | 226 (43.0) | |
| Overweight | 132 (60.3) | 87 (39.7) | 219 (41.6) | |
| Obese | 44 (62.9) | 26 (37.1) | 70 (13.3) | |
| Physical Activity | 0.536 | |||
| Sedentary | 228 (64.0) | 128 (36.0) | 356 (67.7) | |
| Light | 68 (61.8) | 42 (38.2) | 110 (20.9) | |
| Moderate-vigorous | 34 (56.7) | 26 (43.3) | 60 (11.4) | |
| Sleeping arrangement | 0.077 | |||
| Hard bed | 265 (60.9) | 170 (39.1) | 435 (82.7) | |
| Foam bed | 65 (71.4) | 26 (28.3) | 91 (17.3) | |
| Education | 0.182 | |||
| Masters and above | 77 (62.6) | 46 (37.4) | 123 (23.4) | |
| Bachelor level | 60 (70.6) | 25 (29.4) | 85 (16.2) | |
| Elementary to secondary | 170 (62.3) | 103 (37.7) | 273 (51.9) | |
| Illiterate | 23 (51.1) | 22 (48.9) | 45 (8.6) | |
| Smoker | 0.864 | |||
| No | 276 (63.0) | 162 (37.0) | 438 (83.3) | |
| Yes | 54 (61.4) | 34 (38.6) | 88 (16.7) | |
| Diabetes | 0.003 | |||
| No | 281 (65.8) | 146 (34.2) | 427 (81.2) | |
| Yes | 49 (49.5) | 50 (50.5) | 99 (18.8) | |
| Cardiovascular disease | <0.001 | |||
| No | 321 (66.2) | 164 (37.8) | 485 (92.2) | |
| Yes | 9 (22.0) | 32 (78.0) | 41 (7.8) | |
| Multi-morbidity | <0.001 | |||
| No | 328 (64.8) | 178 (35.2) | 506 (96.2) | |
| Yes | 2 (10.0) | 18 (90.0) | 20 (3.8) | |
| Variables | Categories | Model 1 (All Data) * | Model 2 (Female Data) * | Model 3 (Male Data) * |
|---|---|---|---|---|
| Gender | Female | 1.92, (1.30–2.86), 0.001 | - | - |
| Male | Reference | |||
| Age | 30–39 | Reference | ||
| 40–49 | 1.13, (0.68–1.87), 0.624 | 0.99, (0.32–2.83), 0.977 | 1.06, (0.56–2.00), 0.852 | |
| 50–59 | 2.31, (1.40–3.84), 0.001 | 1.98, (0.55–6.78), 0.282 | 1.66, (0.84–3.29), 0.143 | |
| ≥60 | 3.51, (2.02–6.17), <0.001 | 4.18, (1.03–16.94), 0.044 | 2.01, (0.99–4.10), 0.510 | |
| Multi-morbidity | Yes | 9.16, (2.48–59.36), <0.001 | 7.34, (1.18–42.73) 0.072 | 10.0, (1.82–87.09), 0.031 |
| No | Reference | |||
| BMI | Normal | Reference | ||
| Obese | 1.16, (0.63–2.11), 0.628 | 1.44, (0.59–3.50), 0.419 | 0.98, (0.38–2.39), 0.957 | |
| Overweight | 1.23, (0.81–1.85), 0.332 | 1.44, (0.70–3.02), 0.327 | 1.27, (0.75–2.13), 0.368 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ali, M.; Uddin, Z.; Hossain, A. Prevalence and Patterns of Risk of Osteoporosis in Bangladeshi Adult Population: An Analysis of Calcaneus Quantitative Ultrasound Measurements. Osteology 2021, 1, 187-196. https://0-doi-org.brum.beds.ac.uk/10.3390/osteology1040018
Ali M, Uddin Z, Hossain A. Prevalence and Patterns of Risk of Osteoporosis in Bangladeshi Adult Population: An Analysis of Calcaneus Quantitative Ultrasound Measurements. Osteology. 2021; 1(4):187-196. https://0-doi-org.brum.beds.ac.uk/10.3390/osteology1040018
Chicago/Turabian StyleAli, Mohammad, Zakir Uddin, and Ahmed Hossain. 2021. "Prevalence and Patterns of Risk of Osteoporosis in Bangladeshi Adult Population: An Analysis of Calcaneus Quantitative Ultrasound Measurements" Osteology 1, no. 4: 187-196. https://0-doi-org.brum.beds.ac.uk/10.3390/osteology1040018