
Patellar Instability in Pediatric Patients: Review of the Literature


1
Department of Orthopaedic and Trauma Surgery, Magna Graecia University of Catanzaro, 88100 Catanzaro, Italy
2
Department of Orthopedics and Traumatology, Hacettepe University Hospital, Ankara 06230, Turkey
*
Author to whom correspondence should be addressed.
†
Authors contributed equally to this paper.
Osteology 2021, 1(4), 197-208; https://0-doi-org.brum.beds.ac.uk/10.3390/osteology1040019
Submission received: 30 July 2021
/
Revised: 18 October 2021
/
Accepted: 22 October 2021
/
Published: 24 October 2021
(This article belongs to the Special Issue Feature Papers in Osteology)
{kind=link}
Abstract
:Patellar instability is a common pathology of the knee in pediatric patients. The management of this condition can be a challenge for the orthopedic surgeon, and a comprehensive understanding of the anatomy and biomechanics of the structures around the knee is of utmost importance in formulating a treatment plan. Predisposing factors can be related to: trochlear and patellar morphological abnormalities, ligamentous stabilizers, limb geometries in the axial plane, and patellar height abnormalities. Traditionally, first-time dislocators have been treated non-operatively; however, recent evidence suggests that certain factors are related to recurrent instability, and surgical treatment may be considered even after the first dislocation. It is important to keep in mind that younger children with open physes are not suitable candidates for certain surgical techniques. In this comprehensive review, we aimed to focus on the most up-to-date information on this topic and emphasize the importance of individualizing the treatment of pediatric patients.
1. Introduction
Patellar instability is one of the most common knee pathologies in the skeletally immature population and comprises several different conditions, such as acute dislocations, subluxations, recurrent instability episodes, and congenital dislocations. The annual incidence of acute dislocations under the age of 16 was reported as 43 in 100,000 [1], and the highest risk was found to be among females between the ages 10 and 17 [2]. A recent United States national database study by Poorman et al. [3] showed that the number of hospital admissions is steadily increasing every year.
Patellar dislocations occur almost exclusively laterally. Medial dislocations are very rare and mainly associated with iatrogenic excessive lateral retinacular releases [4]. More than 30% of the patients with an acute dislocation experience recurrent instability episodes [5,6], which predisposes the patellofemoral joint to further damage. Up to 73% of the patients undergoing surgical treatment exhibited cartilage damage of varying severity [7]. These injuries might have a significant impact on the patient’s life, such as physical activity modifications and decreased physical fitness [8].
As a part of the increasing awareness towards pediatric orthopedic injuries, the number of surgically treated patellar dislocations in the pediatric and adolescent population has also increased more than two-fold [9]. With an increasing rate of participation and intensity of sports among the pediatric population, the proper treatment of patellar instability will certainly become more important in the future. The purpose of this review is to summarize the current knowledge on the pathophysiology, evaluation, and treatment of pediatric patellar instability.
2. Pathophysiology and Predisposing Factors
Diagnosing the possible predisposing factors in a patient with patellar instability is the most critical step in the management of this disorder. There are four possible underlying factors: trochlear and patellar morphological abnormalities, ligamentous stabilizers, limb geometries in the axial plane, and patellar height [10]. When evaluating a patient, it must be kept in mind that, in 58.3% of recurrent dislocators, more than one of these factors could be identified in magnetic resonance imaging (MRI) [11], so each one of these anatomical predispositions must be carefully identified, and their role in instability must be identified.
3. Trochlear and Patellar Morphology
Normal patellofemoral movement is guided by the concave trochlear groove and convex patellar articular surface. This articulation has a complex structure that takes its shape in the early phases of embryologic development [12] and is not significantly affected by mechanical factors. The risk of patellar instability increases if the constraint provided by the trochlear groove during the knee range of motion is inadequate. The two main abnormalities in bony morphology are trochlear and patellar dysplasia.
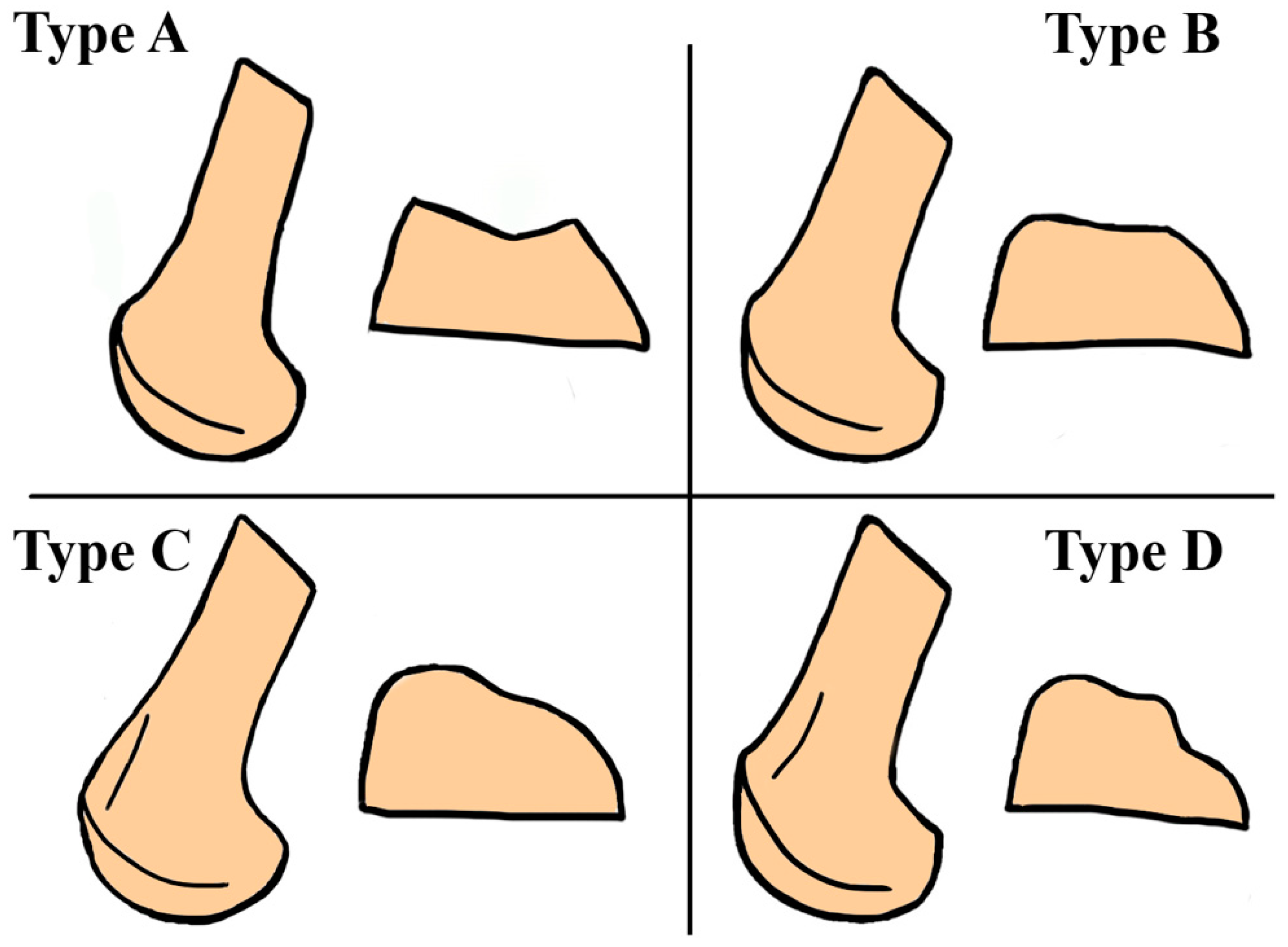
Trochlear dysplasia is an important anatomical factor causing patellar instability, and it has been reported that up to 96% of the patients with a history of patellar dislocation had signs of trochlear dysplasia [13]. This condition is characterized radiographically by the crossing sign [13] and was classified into four different types according to the radiographic and axial computed tomography (CT) appearances by DeJour et al. [14] (Figure 1). Even though it has been reported that at least one abnormal radiographic finding is present in all the patients with trochlear dysplasia and routine MRI is not necessary [15], due to incomplete trochlear ossification in the skeletally immature population, MRI is used very frequently. Recent evidence suggests that many of the parameters related to trochlear morphology show significant changes throughout skeletal growth, and the trochlea takes its final shape around the age of 12 [16].
Morphological changes of the patella are also seen in patients with patellar instability, which must be evaluated together with trochlear dysplasia. A stable movement arc between the patella and femur is necessary for the healthy development of both the trochlea and patella, as evident by the trochlear dysplasia seen in rabbits after patellar dislocation [17]. After the description of different patellar morphological characteristics by Wiberg et al. [18], most of the studies have focused on adults. A smaller medial facet and overall patellar size have been found in patients with instability [19,20].
Recent studies have focused on the possible morphological improvements seen in children with instability after surgical correction: Niu et al. [21] reported that, after a mean follow-up period of 28 months after soft-tissue surgery, the Wiberg indices of the unstable joints significantly improved, becoming comparable to controls, and Fu et al. [22] reported that early surgery before physeal closure can result in the improved sulcus angle, trochlear groove depth, and trochlear inclination.
4. Limb Geometries in the Axial Plane
Lateralization of the tibial tubercle, as measured by the tibial tubercle–trochlear groove (TT–TG) distance, is frequently investigated in the literature [4,23]. A lateralized TT results in an abnormal path taken by the extensor mechanism during the knee range of motion and creates abnormally high laterally directed vectors on the patella. The TT–TG distance was, on average, 4 mm greater in patients with pateollofemoral instability when compared to healthy controls [4].
However, careful evaluation is necessary when including the TT–TG distance in the decision-making process. Rather than pointing to a lateralized TT, abnormal TT–TG measurements may simply be secondary to rotational deformities around the knee [24] or changing degrees of knee flexion [25]. In the last decade, focus has been on the use of tibial tubercle–posterior cruciate ligament (TT–PCL) distance, as described by Seitlinger et al. [26]. With both landmarks on the tibia, this measurement eliminates the confounding factors previously mentioned. Both the TT–TG and TT–PCL distances had excellent inter- and intra-observer agreement [27], while different threshold values for the TT–PCL distance have been suggested in the literature [27,28].
Other factors to predisposed patellar instability are genu valgum, excessive femoral anteversion, and tibial torsion. If not correctly evaluated and addressed, these factors may result in inferior clinical outcomes after surgical treatment: Zhang et al. [29] reported that the group with >30° femoral anteversion had worse Kujala, Lysholm, and IKDC scores when compared to the groups with less anteversion. Franciozi et al. [30] reported that, in patients with surgically treated recurrent patellar instability, the group with higher femoral anteversion had worse Kujala scores, and less improvement was gained by surgery. All these morphological factors play important roles in patellofemoral stability, and, adding to the complexity of the issue, these factors are significantly correlated with each other, as recently reported by Imhoff et al. [31]. Detailed knowledge of the lower extremity anatomy and thorough patient evaluation are necessary for correct decision-making.
5. Ligamentous Stabilizers
On the medial side of the patella, the medial patellofemoral ligament (MPFL) functions as the primary soft tissue restraint to lateral translation and has a mean tensile strength of 208 N [32]. Despite being responsible for 50% of the medial stabilization, recent investigations have discovered that other soft tissue structures play important roles as well. A cadaveric study by Philippot et al. [33] showed that the MPFL provides the majority of the lateral restraint in the first 30° of knee motion, while other more distal structures, such as the medial patellotibial ligament (MPTL) and medial patellomeniscal ligament (MPML), also play important roles in higher degrees of flexion and take on nearly 50% of the restraint. It has also been shown that the MPFL is not the only proximal medial restraint, and, together with the medial quadriceps tendon femoral ligament (MQTFL), should be considered as the proximal medial patellar restraints (PMPR) [34]. While anatomical and biomechanical studies elaborate on these secondary ligamentous restraints, their clinical implications are yet to be discovered.
The MPFL is torn in more than 90% of the children with lateral patellar dislocations [35]. Previous studies in the literature determined that, in most of the cases, the injury is on the femoral side [2,36]. However, most of these studies include both children and adults. A study by Askenberger et al. [35] included 74 patients in the pediatric age group with first-time lateral patellar dislocations: 99% of the patients had an MPFL injury, among which 60% were patellar-sided, 35% were multifocal, and 4% were femoral-sided. The same study confirmed similar rates with arthroscopic examination as well. As is evident from these results, skeletally immature patients are more prone to patellar-sided injuries.
Among the soft tissue factors contributing to patellar instability, generalized joint laxity (GJL) is mostly overlooked. Patients can be assessed for hyperlaxity by using the Beighton scoring system [37]. Despite anecdotal referrals, studies examining the relationship between GJL and patellar instability are not numerous. Nomura et al. [38] compared 82 patients with recurrent patellar dislocations to age and sex matched controls: 24% of the patients had GJL compared to 10% of the controls (p = 0.013). Patients must be evaluated for this condition and, if necessary, informed that the results of the treatment may be different than for the general population [39].
6. Patellar Height
Patella alta is another important risk factor for patellar instability. Many different methods have been used in the literature for the assessment of patellar height, and the Insall–Salvati method is most frequently used in adults [40]. Because of the anatomical and radiographical differences of the immature skeleton, only the Koshino (KI) and Caton–Dexchamps (CDI) indices are applicable in children [41]. In a study by Thevenin-Lemoine et al. [42], the CDI showed excellent inter- and intra-observer reliability, with a mean value of 1.27 ± 0.25 at 6 to 7 years, which decreases to 1.07 ± 0.18 at 14 to 15 years of age. A CDI of greater than 1.2 is generally accepted as patella alta; however, it must be kept in mind that patellar height indices show significant changes with age.
7. Classification
Other than the acute traumatic dislocations, patellar instability can be classified into five different categories, as proposed by Chotel et al. [43].
7.1. Congenital Dislocations
The congenital dislocation of the patella is rarely seen [44]. This condition is usually bilateral and associated with certain syndromes, such as Rubinstein–Taybi, Williams–Beuren, and nail–patella syndrome [45]. Its characteristic features are a flexion contracture and valgus deformity at the knee, and external tibial torsion. Conservative treatment is not considered an option, and early surgery yields better results [46].
7.2. Permanent Dislocation
This condition usually occurs after walking and before 5 years of age. The patellar height is normal, but the quadriceps is shortened. A rounded lateral trochlea and a single-facet patella is usually detected. The child may have difficulty walking, and knee flexion may be limited [43].
7.3. Habitual Dislocation in Flexion
In this condition, the patella dislocates during flexion and relocates during extension, unlike chronic dislocations that never reduce without an intervention [47]. The underlying factors are generally implicated as a short vastus lateralis or lateral retinaculum, or an abnormal iliotibial band attachment. Genu valgum may accompany the patellar instability. Surgical methods are generally employed in the treatment, which include quadriceps lengthenings and lateral retinacular releases.
7.4. Habitual Dislocation in Extension
This condition is characterized by the dislocation or subluxation of the patella only when the knee is at full or near-full extension. The patella relocates into the trochlea with flexion [43].
7.5. Episodic/Recurrent Instability
This is the most common type of patellar instability seen in children [48]. The symptoms begin near adolescence, and there is a female predominance. The dislocations occur without significant trauma, but there is usually an inciting event, such as a sports injury. The patient’s major complaint is patellar apprehension; pain is only occasional. Most of the patients have several predisposing factors [44], and family history may be positive.
Another classification system has been proposed by Parikh et al. [49] that divides this condition into four different types: type 1 is first-time dislocation, type 2 is reccurent instability (the most common form), type 3 is dislocatable patella, and type 4 is a dislocated patella.
8. Treatment Options
- Non-Operative Treatment
Traditionally, the most common initial treatment for first-time dislocations without an osteochondral fragment, osseous MPFL avulsion, or meniscal tear is non-operative management [48,50]. This has also been reported as a consensus decision by a group of experts on patellofemoral joint studies (International Patellofemoral Study Group) [51].
The non-operative management protocol can be divided into different stages: (1) resolution of pain and swelling, (2) recovery of joint motion and flexibility, (3) recovery of muscle strength, (4) recovery of motor patterns and coordination, and (5) return to sporting activities [52]. Most centers initially start with a period of immobilization, for which the duration varies considerably. In a study by Hilber et al. [53]. where functional rehabilitation programmes were compared, it has been reported that the full range of motion (ROM) was allowed after a mean of 5.7 weeks, and the use of a brace during this period is also common, as advised by 66.6% of the centers. Physical therapy includes quadriceps isometric strengthenings, with a special focus on vastus medialis obliquus (VMO) exercises, which then progresses to gluteal and core exercises [44]. Ligamentous laxity may be seen in these patients, and, in this case, effective control should be achieved with balance exercises to prevent reccurent dislocations. Gait disturbances may also occur after the dislocation, which is a defence mechanism to prevent pain and apprehension; gait exercises must also be employed [52]. A return to sports after a controlled physical therapy regimen usually takes at least 3 months.
- Early Surgery?
Recently, the traditional approach of conservative treatment for first-time dislocations has been under scrutiny. A study by Magnussen et al. [54] reported that, at a mean period of 3.4 years after the primary dislocation, only 26.4% of the non-surgically managed patients could return to the desired sporting activities without any limitations despite the fact that 73.1% did not have further dislocations. Considerable re-dislocation rates of up to 71% have also been reported by several studies [52]. The rate of recurrence has been significantly lower in the surgically treated group (25%) when compared to conservatively treated patients (36.4%), as reported by Longo et al. [55]. With an increasing amount of studies in the literature comparing conservative and surgical treatments in primary patellar dislocations, several meta-analyses have also been performed in recent years [56,57,58]. Pagliazzi et al. [58] included 510 patients from 10 randomized controlled trials (RCTs) and reported that the surgically treated group had better Kujala scores in the short-term, while the scores were similar in the long-term. A lower rate of recurrence was also reported in the surgical group at short-term follow-up, with a risk rate of 0.40 (95% confidence interval (CI) 0.25 to 0.66; p < 0.001); no significant difference was found at mid-term. Migliorini et al. [57] analyzed the data of 654 patients from 12 studies: the surgically treated group had better Kujala scores (mean difference: 9.99%; 95% CI: 2.85 to 17.13; p = 0.006) and lower redislocation rates (odds ratio(OR): 0.41; 95% CI: 0.27 to 0.62; p < 0.0001). Currently, none of these meta-analyses focus specifically on pediatric patients.
The results obtained from the meta-analyses clearly show that a certain group of patients might benefit from early surgery. However, there is no consensus on how to identify those patients who are at a higher risk of recurrent dislocations. Huntington et al. [59] recently evaluated the risk factors for reccurent instability in a meta-analysis of 17 studies. A total of 28 different factors were investigated by those studies, and, after the pooled analysis, the significant risk factors were determined as: younger age (OR: 2.61, p < 0.00001), open physes (OR: 2.72, p < 0.00001), trochlear dysplasia (OR: 4.15, p = 0.009), elevated TT–TG distance (OR: 2.87, p < 0.00001), and patella alta (OR: 2.38, p = 0.004). Hevesi et al. [60] developed the recurrent instability of the patella (RIP) score in an effort to identify the high-risk patients. The variables included in the scoring system are age, skeletal immaturity, trochlear dysplasia, and TT–TG/patellar length (PL) ratios. The patients are stratified into low, intermediate, and high-risk groups according to their total scores. Further studies are required to reach a consensus on how to determine the population that will benefit the most from early surgery.
- Surgical Treatment
8.1. Proximal Stabilization Techniques
The MPFL reconstruction is currently the most frequently utilized technique for the surgical stabilization of pediatric patellar instabilities. Multiple different technqiues have been described for this procedure: various types of grafts (autografts or allografts) in anatomic or non-anatomic fashion, and different fixation methods (interference screw, suspensory, suture anchor) have all been used [48]. Combining MPFL reconstruction with bony procedures is popular in adults with anatomical predispositions [61]; however, in children with open physes, these combinations are not applicable.
Kumar et al. [62] compared the use of autografts and allografts retrospectively in their study: they included 59 adolescents with a mean age of 15.2 years and found no difference in the return to sports, pain scores, or incidences of failure at a mean follow-up of 4.1 years. Fixation techniques have also been compared by Lenschow et al. [63]: a comparison of 3.5-mm titanium anchor, transosseous polyester suture, interference screws, medial bone bridge, and transpatellar tunnels revealed that the load to failure of the bone bridge technique was significantly lower than the other four, and also lower than the native MPFL.
Non-isometric attachment sites have been linked to inferior results; therefore, the landmarks used for reconstruction are worthy of attention [48]. The femoral origin of the MPFL is midway between the medial epicondyle and adductor tubercle in adults, which is radiographically identified as Schottle’s point [64]. In children, the close proximity of this region to the distal femoral physis makes it technically demanding to use during reconstruction procedures. A cadaveric study by Farrow et al. [65] showed that the MPFL attachment was, on average, 8.5 mm distal to the medial aspect of the distal femoral physis. Considering the undulating nature of the distal femoral physis, when opening a tunnel, the guide must be directed distal and anterior to minimize a potential risk of injury to the physis [66]. To completely avoid the physis, different techniques, such as the adductor sling [67] and the quadriceps turn-down [68], have been proposed, with limited use.
Repairing the torn MPFL is also discussed as a valid option by several studies. Bryant et al. [69] compared the results of repair and reconstruction and reported that MPFL repair achieved comparable redisclocation rates. In a study by Askenberger et al. [70], the results of the acute repair versus conservative management for pediatric first-time dislocators were compared and, while MPFL repair successfully reduced the redislocation rates, no significant improvement was achieved in the functional results.
Medial reefing is another procedure that can be used in selected cases with fewer complications than reconstruction [66]. However, as a non-anatomic procedure, its efficacy in preventing recurrent dislocations has been questioned. In a recent study, Ahrend et al. [71] found a recurrence rate of 34.5% and emphasized that, before considering reefing, MRI-based measurements, such as patellar height, TT–TG distance, patellar tilt, and lateral trochlea index, must be carefully evaluated.
8.2. Distal Stabilization Techniques
Patients with an increased TT–TG distance, or with patella alta, may benefit significantly from distal realignment procedures. In adolescents with closed physes, various osteotomy techniques described for adults can be used safely [72]; however, in younger children with open physes, different techniques have been developed [73].
The Roux–Goldthwait procedure was described over a century ago and has recently been modified by Marsh et al. [74]: in the original technique, the patellar tendon is split and the lateral half is transferred below the medial half, onto the periosteum, and, in the modificiation, a lateral retinacular release was also performed. In the same study on thirty knees, after a modified Roux–Goldthwait procedure, based on Insall criteria, twenty-six of the knees achieved an excellent result, three a good result, and one a fair result. In an effort to perform a systematic review of the literature considering this procedure, Felli et al. [75] found that, among several different studies, only 8.6% of the patients underwent an isolated Roux–Goldthwait procedure; the remaining patients underwent either a modified version or combined procedures that are more frequently utilized nowadays.
The Galeazzi technique was originally described in 1922 [76]. In this technique, the semitendinosus tendon is harvested and reattached onto the medial side of the patella obliquely. Several modified techniques have also been described [77,78]. Grannatt et al. [79] retrospectively evaluated the results of 34 knees after the Galeazzi procedure and reported a recurrent instability rate of 82%. Owing to these results, the isolated use of this technique is infrequent.
In a study by Grammont et al. [80], a patellar tendon realignment technique was described in which the tendon is sharply dissected distally from the apophysis and reattached medially. Kraus et al. [81] reported the results of 65 skeletally immature knees after a modified Grammont procedure and found no growth disturbances with the moderate prevention of recurrent dislocations.
Currently, these distal realignment techniques are more frequently utilized as a part of combined procedures. Oliva et al. [82] reported the results of the 3-in-1 procedure, which is the combination of the lateral release, vastus medialis obliquus muscle advancement, and transfer of the medial third of the patellar tendon to the medial collateral ligament. At a mean follow-up of 3.8 years, only 1 of 25 knees had a recurrent dislocation, which was after a motor vehicle accident. Danino et al. [83] recently reported the results of the 4-in-1 procedure (which stands for extensive lateral release, Roux–Goldthwait procedure, Galeazzi procedure, and VMO advancement combined) for the treatment of congenital and habitual disclocatons: in a total of 46 knees with a mean follow-up of 51.6 months, 18% had recurrent instability.
Recently, together with an increasing interest in the anatomy and functions of the distal medial patellar restraints (MPML and MPTL), the reconstruction of these ligaments has also been investigated by several studies. These secondary restraints become more important in patellar stability in higher degrees of knee flexion [84]. In a cadaveric study, Ambra et al. [85] demonstrated that MPTL reconstruction failed to provide sufficient restraint against lateral patellar translation, when compared to MPFL reconstruction. The results of the combined procedures are more promising: a systematic review by Aicale et al. [86] examined nine studies reporting on combined MPFL and MPTL reconstruction and mentioned good and excellent results overall. These combined procedures may be more frequently used in the future, especially in recalcitrant cases.
8.3. Trochleoplasty
In patients with trochlear dysplasia, the rate of recurrence is higher for patellar instability. Trochleoplasty aims to change the trochlear morphology and achieve better stabilization throughout the range of motion. In adults and adolescents with closed physes, this procedure can be applied safely [87]. However, in children with open physes, routine trochleoplasty techniques can create a transphyseal fracture and result in growth disturbances and, therefore, are not recommended.
Pesenti et al. [88] described a lateral wedge augmentation trochleoplasty technique that avoids the physeal plate and, therefore, can be safely applied in children. They reported no recurrent patellar dislocations; however, several concerning outcomes were noted, such as anteror knee pain in three patients and osteoarthritis in four patients. The authors suggested that other techniques should be employed whenever possible.
8.4. Growth Guidance
In patients with mechanical axis abnormalities, correction techniques depend on the patient’s age. Older children can benefit from osteotomies [50]. Guided growth techniques are recommended in patients with open physes.
Hemiepiphysiodesis techniques can be applied either with or without an MPFL reconstruction. In a report by Tan et al. [89], only four of the twenty patients had recurrent patellar instability after isolated hemiepiphysiodesis. For combined MPFL reconstruction and hemiepiphysiodesis, Parikh et al. [90] reported encouraging results in their preliminary study: six of the seven patients achieved satisfactory patellar stabilization.
- Treatment Options: Pros and Cons
With an increasing number of pediatric patients hospitalized for patellar dislocations [3], correct decision-making between conservative and surgical treatment options is of utmost importance. Conservative measures have the advantage of achieving higher functional scores despite a higher risk of redislocations [70]. To avoid physeal injuries and surgery-related morbidities, non-operative measures can still be considered as the method of choice for the majority of first-time dislocators without large osteochondral fragments.
In the case of recurrent dislocations, surgery is generally performed to prevent functional decline, further joint injury, including patellofemoral osteoarthritis, and possible isolation from peers [8,91,92,93]. Complications are infrequent but include the failure of the procedure resulting in further dislocations, inability to return to sports, infections, and quadriceps weakness [48].
9. Conclusions
The management of patellar instability in the pediatric age group is a challenging task. The increased participation in sports and overall activity levels in this population bring along the expectation of early functional recovery. Moreover, in younger children with an immature skeleton, some of the most frequently used surgical techniques cannot be applied due to possible physeal injury.
Recurrent instability is an important factor, and a younger age at the first dislocation is a risk factor for recurrent episodes. Therefore, the thorough evaluation of the patient and correct identification of the predisposing factors is crucial. The traditional approach of not operating on a first-time dislocator is increasingly being questioned. It can be assumed that the paradigm is shifting towards early surgery on a carefully selected subset of patients. The definition of that particular patient group is unclear, so further clinical evidence is required.
A comprehensive understanding of the anatomy and biomechanics of the structures around the knee is of utmost importance in formulating a treatment plan for these patients. Among the many different surgical methods, choosing the one that best fits the patient’s needs requires experience and is of paramount importance for the long-term success of the treatment.
Author Contributions
Conceptualization, F.F. and G.H.; methodology, F.F. and R.M.C.; software, R.M.C.; validation, F.F. and G.H.; investigation, R.M.C. and F.F.; resources, R.M.C.; data curation, R.M.C. and G.H.; writing-original draft preparation, R.M.C., F.F. and G.H.; writing-review and editing, F.F. and G.H.; visualization, R.M.C.; supervision, G.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Nietosvaara, Y.; Aalto, K.; Kallio, P.E. Acute patellar dislocation in children: Incidence and associated osteochondral fractures. J. Pediatr. Orthop. 1994, 14, 513–515. [Google Scholar] [CrossRef]
- Fithian, D.C.; Paxton, E.W.; Stone, M.L.; Silva, P.; Davis, D.K.; Elias, D.A.; White, L. Epidemiology and natural history of acute patellar dislocation. Am. J. Sports Med. 2004, 32, 1114–1121. [Google Scholar] [CrossRef] [PubMed]
- Poorman, M.J.; Talwar, D.; Sanjuan, J.; Baldwin, K.D.; Sutliff, N.; Franklin, C.C. Increasing hospital admissions for patellar instability: A national database study from 2004 to 2017. Phys. Sportsmed. 2020, 48, 215–221. [Google Scholar] [CrossRef]
- Khormaee, S.; Kramer, D.E.; Yen, Y.M.; Heyworth, B.E. Evaluation and management of patellar instability in pediatric and adolescent athletes. Sports Health 2015, 7, 115–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christensen, T.C.; Sanders, T.L.; Pareek, A.; Mohan, R.; Dahm, D.L.; Krych, A.J. Risk Factors and Time to Recurrent Ipsilateral and Contralateral Patellar Dislocations. Am. J. Sports Med. 2017, 45, 2105–2110. [Google Scholar] [CrossRef] [PubMed]
- Lewallen, L.W.; McIntosh, A.L.; Dahm, D.L. Predictors of recurrent instability after acute patellofemoral dislocation in pediatric and adolescent patients. Am. J. Sports Med. 2013, 41, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Luhmann, S.J.; Smith, J.C.; Schootman, M.; Prasad, N. Recurrent Patellar Instability: Implications of Preoperative Patellar Crepitation on the Status of the Patellofemoral Articular Cartilage. J. Pediatr. Orthop. 2019, 39, 33–37. [Google Scholar] [CrossRef]
- Schneider, D.K.; Grawe, B.; Magnussen, R.A.; Ceasar, A.; Parikh, S.N.; Wall, E.J.; Colosimo, A.J.; Kaeding, C.C.; Myer, G.D. Outcomes After Isolated Medial Patellofemoral Ligament Reconstruction for the Treatment of Recurrent Lateral Patellar Dislocations: A Systematic Review and Meta-analysis. Am. J. Sports Med. 2016, 44, 2993–3005. [Google Scholar] [CrossRef] [Green Version]
- McFarlane, K.H.; Coene, R.P.; Feldman, L.; Miller, P.E.; Heyworth, B.E.; Kramer, D.E.; Kocher, M.S.; Yen, Y.-M.; Milewski, M.D. Increased incidence of acute patellar dislocations and patellar instability surgical procedures across the United States in paediatric and adolescent patients. J. Child. Orthop. 2021, 15, 149–156. [Google Scholar] [CrossRef]
- Duppe, K.; Gustavsson, N.; Edmonds, E.W. Developmental Morphology in Childhood Patellar Instability: Age-dependent Differences on Magnetic Resonance Imaging. J. Pediatr. Orthop. 2016, 36, 870–876. [Google Scholar] [CrossRef]
- Steensen, R.N.; Bentley, J.C.; Trinh, T.Q.; Backes, J.R.; Wiltfong, R.E. The prevalence and combined prevalences of anatomic factors associated with recurrent patellar dislocation: A magnetic resonance imaging study. Am. J. Sports Med. 2015, 43, 921–927. [Google Scholar] [CrossRef] [PubMed]
- Glard, Y.; Jouve, J.L.; Garron, E.; Adalian, P.; Tardieu, C.; Bollini, G. Anatomic study of femoral patellar groove in fetus. J. Pediatr. Orthop. 2005, 25, 305–308. [Google Scholar] [PubMed]
- Dejour, H.; Walch, G.; Nove-Josserand, L.; Guier, C. Factors of patellar instability: An anatomic radiographic study. Knee Surg. Sports Traumatol. Arthrosc. 1994, 2, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Dejour, D.; Saggin, P. The sulcus deepening trochleoplasty-the Lyon’s procedure. Int. Orthop. 2010, 34, 311–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lippacher, S.; Reichel, H.; Nelitz, M. Radiological criteria for trochlear dysplasia in children and adolescents. J. Pediatr. Orthop. B. 2011, 20, 341–344. [Google Scholar] [CrossRef] [PubMed]
- Trivellas, M.; Kelley, B.; West, N.; Jackson, N.J.; Beck, J.J. Trochlear Morphology Development: Study of Normal Pediatric Knee MRIs. J. Pediatr. Orthop. 2021, 41, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Wang, Q.; Wang, F.; Zhang, Y.; Ma, L.; Dong, J. Femoral trochlear dysplasia after patellar dislocation in rabbits. Knee 2013, 20, 485–489. [Google Scholar] [CrossRef]
- Wiberg, G. Roentgenographic and anatomic studies on the femoropatellar joint. Acta. Orthop. Scand. 1941, 12, 90. [Google Scholar]
- Barnett, A.J.; Gardner, R.O.; Lankester, B.J.; Wakeley, C.J.; Eldridge, J.D. Magnetic resonance imaging of the patella: A comparison of the morphology of the patella in normal and dysplastic knees. J. Bone Jt. Surg. Br. Vol. 2007, 89, 761–765. [Google Scholar] [CrossRef]
- Fucentese, S.F.; von Roll, A.; Koch, P.P.; Epari, D.R.; Fuchs, B.; Schottle, P.B. The patella morphology in trochlear dysplasia--a comparative MRI study. Knee 2006, 13, 145–150. [Google Scholar] [CrossRef]
- Niu, J.; Qi, Q.; Hao, K.; Lin, W.; Piao, K.; Wang, F. The morphology of patella changed significantly after soft tissue correction for children with recurrent patella dislocation. BMC. Musculoskelet. Disord. 2020, 21, 833. [Google Scholar] [CrossRef] [PubMed]
- Fu, K.; Duan, G.; Liu, C.; Niu, J.; Wang, F. Changes in femoral trochlear morphology following surgical correction of recurrent patellar dislocation associated with trochlear dysplasia in children. Bone Jt. J. 2018, 100, 811–821. [Google Scholar] [CrossRef] [PubMed]
- Pennock, A.T.; Alam, M.; Bastrom, T. Variation in tibial tubercle-trochlear groove measurement as a function of age, sex, size, and patellar instability. Am. J. Sports Med. 2014, 42, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Tensho, K.; Akaoka, Y.; Shimodaira, H.; Takanashi, S.; Ikegami, S.; Kato, H.; Saito, N. What Components Comprise the Measurement of the Tibial Tuberosity-Trochlear Groove Distance in a Patellar Dislocation Population? J. Bone Jt. Surg. Am. 2015, 97, 1441–1448. [Google Scholar] [CrossRef] [PubMed]
- Marquez-Lara, A.; Andersen, J.; Lenchik, L.; Ferguson, C.M.; Gupta, P. Variability in Patellofemoral Alignment Measurements on MRI: Influence of Knee Position. AJR. Am. J. Roentgenol. 2017, 208, 1097–1102. [Google Scholar] [CrossRef]
- Seitlinger, G.; Scheurecker, G.; Hogler, R.; Labey, L.; Innocenti, B.; Hofmann, S. Tibial tubercle-posterior cruciate ligament distance: A new measurement to define the position of the tibial tubercle in patients with patellar dislocation. Am. J. Sports Med. 2012, 40, 1119–1125. [Google Scholar] [CrossRef]
- Xu, Z.; Zhang, H.; Yan, W.; Qiu, M.; Zhang, J.; Zhou, A. Validating the Role of Tibial Tubercle-Posterior Cruciate Ligament Distance and Tibial Tubercle-Trochlear Groove Distance Measured by Magnetic Resonance Imaging in Patients With Patellar Dislocation: A Diagnostic Study. Arthroscopy 2021, 37, 234–242. [Google Scholar] [CrossRef] [PubMed]
- Brady, J.M.; Rosencrans, A.S.; Shubin Stein, B.E. Use of TT-PCL versus TT-T.G. Curr. Rev. Musculoskelet. Med. 2018, 11, 261–265. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhang, H.; Song, G.; Zheng, T.; Ni, Q.; Feng, H. Increased femoral anteversion is associated with inferior clinical outcomes after MPFL reconstruction and combined tibial tubercle osteotomy for the treatment of recurrent patellar instability. Knee. Surg. Sports Traumatol. Arthrosc. 2020, 28, 2261–2269. [Google Scholar] [CrossRef]
- Franciozi, C.E.; Ambra, L.F.; Albertoni, L.J.; Debieux, P.; Rezende, F.C.; Oliveira, M.A.; Ferreira, M.D.C.; Luzo, M.V.M. Increased Femoral Anteversion Influence Over Surgically Treated Recurrent Patellar Instability Patients. Arthroscopy 2017, 33, 633–640. [Google Scholar] [CrossRef]
- Imhoff, F.B.; Funke, V.; Muench, L.N.; Sauter, A.; Englmaier, M.; Woertler, K.; Imhoff, A.B.; Feucht, M.J. The complexity of bony malalignment in patellofemoral disorders: Femoral and tibial torsion, trochlear dysplasia, TT-TG distance, and frontal mechanical axis correlate with each other. Knee. Surg. Sports Traumatol. Arthrosc. 2020, 28, 897–904. [Google Scholar] [CrossRef] [PubMed]
- Amis, A.A.; Firer, P.; Mountney, J.; Senavongse, W.; Thomas, N.P. Anatomy and biomechanics of the medial patellofemoral ligament. Knee 2003, 10, 215–220. [Google Scholar] [CrossRef]
- Philippot, R.; Boyer, B.; Testa, R.; Farizon, F.; Moyen, B. The role of the medial ligamentous structures on patellar tracking during knee flexion. Knee. Surg. Sports Traumatol. Arthrosc. 2012, 20, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Chahla, J.; Smigielski, R.; LaPrade, R.F.; Fulkerson, J.P. An Updated Overview of the Anatomy and Function of the Proximal Medial Patellar Restraints (Medial Patellofemoral Ligament and the Medial Quadriceps Tendon Femoral Ligament). Sports Med. Arthrosc. Rev. 2019, 27, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Askenberger, M.; Arendt, E.A.; Ekstrom, W.; Voss, U.; Finnbogason, T.; Janarv, P.M. Medial Patellofemoral Ligament Injuries in Children with First-Time Lateral Patellar Dislocations: A Magnetic Resonance Imaging and Arthroscopic Study. Am. J. Sports Med. 2016, 44, 152–158. [Google Scholar] [CrossRef] [Green Version]
- Nomura, E.; Horiuchi, Y.; Inoue, M. Correlation of MR imaging findings and open exploration of medial patellofemoral ligament injuries in acute patellar dislocations. Knee 2002, 9, 139–143. [Google Scholar] [CrossRef]
- Smits-Engelsman, B.; Klerks, M.; Kirby, A. Beighton score: A valid measure for generalized hypermobility in children. J. Pediatr. 2011, 158, 119–123.e4. [Google Scholar] [CrossRef]
- Nomura, E.; Inoue, M.; Kobayashi, S. Generalized joint laxity and contralateral patellar hypermobility in unilateral recurrent patellar dislocators. Arthroscopy 2006, 22, 861–865. [Google Scholar] [CrossRef]
- Howells, N.R.; Eldridge, J.D. Medial patellofemoral ligament reconstruction for patellar instability in patients with hypermobility: A case control study. J. Bone Jt. Surg. Br. Volume 2012, 94, 1655–1659. [Google Scholar] [CrossRef]
- Insall, J.; Salvati, E. Patella position in the normal knee joint. Radiology 1971, 101, 101–104. [Google Scholar] [CrossRef]
- Rethlefsen, S.A.; Barrett, K.K.; Wren, T.A.L.; Blumstein, G.; Gargiulo, D.; Ryan, D.D.; Kay, R.M. Reliability of patellar height indices in children with cerebral palsy and spina bifida. J. Child. Orthop. 2017, 11, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Thevenin-Lemoine, C.; Ferrand, M.; Courvoisier, A.; Damsin, J.P.; Ducou le Pointe, H.; Vialle, R. Is the Caton-Deschamps index a valuable ratio to investigate patellar height in children? J. Bone Jt. Surg. Am. 2011, 93, 35. [Google Scholar] [CrossRef] [PubMed]
- Chotel, F.; Berard, J.; Raux, S. Patellar instability in children and adolescents. Orthop. Traumatol. Surg. Res. 2014, 100, S125–S137. [Google Scholar] [CrossRef] [Green Version]
- Hasler, C.C.; Studer, D. Patella instability in children and adolescents. EFORT Open. Rev. 2016, 1, 160–166. [Google Scholar] [CrossRef]
- Maia Rosa, J.; Carvalho, A.D.; Coutinho, L.L.; Esteves, J.; Pereira, P.; Vilaca, A. Surgical Treatment for Congenital Dislocation of the Patella in a Young Adult: A Case Report. JBJS Case Connect. 2019, 9, e0196. [Google Scholar] [CrossRef] [PubMed]
- Wada, A.; Fujii, T.; Takamura, K.; Yanagida, H.; Surijamorn, P. Congenital dislocation of the patella. J. Child Orthop. 2008, 2, 119–123. [Google Scholar] [CrossRef] [Green Version]
- Kwak, J.H.; Sim, J.A.; Kim, N.K.; Lee, B.K. Surgical treatment of habitual patella dislocation with genu valgum. Knee Surg. Relat. Res. 2011, 23, 177–179. [Google Scholar] [CrossRef] [PubMed]
- Popkin, C.A.; Bayomy, A.F.; Trupia, E.P.; Chan, C.M.; Redler, L.H. Patellar Instability in the Skeletally Immature. Curr. Rev. Musculoskelet. Med. 2018, 11, 172–181. [Google Scholar] [CrossRef]
- Parikh, S.N.; Lykissas, M.G. Classification of Lateral Patellar Instability in Children and Adolescents. Orthop. Clin. North. Am. 2016, 47, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Vellios, E.E.; Trivellas, M.; Arshi, A.; Beck, J.J. Recurrent Patellofemoral Instability in the Pediatric Patient: Management and Pitfalls. Curr. Rev. Musculoskelet. Med. 2020, 13, 58–68. [Google Scholar] [CrossRef]
- Liu, J.N.; Steinhaus, M.E.; Kalbian, I.L.; Post, W.R.; Green, D.W.; Strickland, S.M.; Stein, B.E.S. Patellar Instability Management: A Survey of the International Patellofemoral Study Group. Am. J. Sports Med. 2018, 46, 3299–3306. [Google Scholar] [CrossRef]
- Rund, J.M.; Hinckel, B.B.; Sherman, S.L. Acute Patellofemoral Dislocation: Controversial Decision-Making. Curr. Rev. Musculoskelet. Med. 2021, 14, 82–87. [Google Scholar] [CrossRef]
- Hilber, F.; Pfeifer, C.; Memmel, C.; Zellner, J.; Angele, P.; Nerlich, M.; Kerschbaum, M.; Popp, D.; Baumann, F.; Krutsch, W. Early functional rehabilitation after patellar dislocation-What procedures are daily routine in orthopedic surgery? Injury 2019, 50, 752–757. [Google Scholar] [CrossRef] [PubMed]
- Magnussen, R.A.; Verlage, M.; Stock, E.; Zurek, L.; Flanigan, D.C.; Tompkins, M.; Agel, J.; Arendt, E.A. Primary patellar dislocations without surgical stabilization or recurrence: How well are these patients really doing? Knee. Surg. Sports Traumatol. Arthrosc. 2017, 25, 2352–2356. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Ciuffreda, M.; Locher, J.; Berton, A.; Salvatore, G.; Denaro, V. Treatment of Primary Acute Patellar Dislocation: Systematic Review and Quantitative Synthesis of the Literature. Clin. J. Sport. Med. 2017, 27, 511–523. [Google Scholar] [CrossRef] [PubMed]
- Fu, Z.; Zhu, Z.; Chen, H.; Zhang, S. Surgical treatment is better than non-surgical treatment for primary patellar dislocation: A meta-analysis of randomized controlled trials. Arch. Orthop. Trauma. Surg. 2020, 140, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Migliorini, F.; Driessen, A.; Quack, V.; Gatz, M.; Tingart, M.; Eschweiler, J. Surgical versus conservative treatment for first patellofemoral dislocations: A meta-analysis of clinical trials. Eur. J. Orthop. Surg. Traumatol. 2020, 30, 771–780. [Google Scholar] [CrossRef]
- Pagliazzi, G.; Napoli, F.; Previtali, D.; Filardo, G.; Zaffagnini, S.; Candrian, C. A Meta-analysis of Surgical Versus Nonsurgical Treatment of Primary Patella Dislocation. Arthroscopy 2019, 35, 2469–2481. [Google Scholar] [CrossRef]
- Huntington, L.S.; Webster, K.E.; Devitt, B.M.; Scanlon, J.P. Feller J.A.; Factors Associated with an Increased Risk of Recurrence After a First-Time Patellar Dislocation: A Systematic Review and Meta-analysis. Am. J. Sports Med. 2020, 48, 2552–2562. [Google Scholar] [CrossRef]
- Hevesi, M.; Heidenreich, M.J.; Camp, C.L.; Hewett, T.E.; Stuart, M.J.; Dahm, D.L.; Krych, A.J. The Recurrent Instability of the Patella Score: A Statistically Based Model for Prediction of Long-Term Recurrence Risk After First-Time Dislocation. Arthroscopy 2019, 35, 537–543. [Google Scholar] [CrossRef]
- Longo, U.G.; Berton, A.; Salvatore, G.; Migliorini, F.; Ciuffreda, M.; Nazarian, A.; Denaro, V. Medial Patellofemoral Ligament Reconstruction Combined with Bony Procedures for Patellar Instability: Current Indications, Outcomes, and Complications. Arthroscopy 2016, 32, 1421–1427. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.; Bastrom, T.P.; Dennis, M.M.; Pennock, A.T.; Edmonds, E.W. Adolescent Medial Patellofemoral Ligament Reconstruction: A Comparison of the Use of Autograft Versus Allograft Hamstring. Orthop. J. Sports Med. 2018, 6, 2325967118774272. [Google Scholar] [CrossRef] [Green Version]
- Lenschow, S.; Schliemann, B.; Gestring, J.; Herbort, M.; Schulze, M.; Kosters, C. Medial patellofemoral ligament reconstruction: Fixation strength of 5 different techniques for graft fixation at the patella. Arthroscopy 2013, 29, 766–773. [Google Scholar] [CrossRef]
- Schottle, P.B.; Schmeling, A.; Rosenstiel, N.; Weiler, A. Radiographic landmarks for femoral tunnel placement in medial patellofemoral ligament reconstruction. Am. J. Sports Med. 2007, 35, 801–804. [Google Scholar] [CrossRef] [PubMed]
- Farrow, L.D.; Alentado, V.J.; Abdulnabi, Z.; Gilmore, A.; Liu, R.W. The relationship of the medial patellofemoral ligament attachment to the distal femoral physis. Am. J. Sports Med. 2014, 42, 2214–2218. [Google Scholar] [CrossRef] [PubMed]
- Andrish, J. Surgical Options for Patellar Stabilization in the Skeletally Immature Patient. Sports Med. Arthrosc. Rev. 2017, 25, 100–104. [Google Scholar] [CrossRef]
- Alm, L.; Krause, M.; Mull, C.; Frosch, K.H.; Akoto, R. Modified adductor sling technique: A surgical therapy for patellar instability in skeletally immature patients. Knee 2017, 24, 1282–1288. [Google Scholar] [CrossRef]
- Noyes, F.R.; Albright, J.C. Reconstruction of the medial patellofemoral ligament with autologous quadriceps tendon. Arthroscopy 2006, 22, 904.e1-t. [Google Scholar] [CrossRef]
- Bryant, J.; Pandya, N. Medial patellofemoral ligament repair restores stability in pediatric patients when compared to reconstruction. Knee 2018, 25, 602–608. [Google Scholar] [CrossRef]
- Askenberger, M.; Bengtsson Mostrom, E.; Ekstrom, W.; Arendt, E.A.; Hellsten, A.; Mikkelsen, C.; Janarv, P.-M. Operative Repair of Medial Patellofemoral Ligament Injury Versus Knee Brace in Children with an Acute First-Time Traumatic Patellar Dislocation: A Randomized Controlled Trial. Am. J. Sports Med. 2018, 46, 2328–2340. [Google Scholar] [CrossRef]
- Ahrend, M.D.; Eisenmann, T.; Herbst, M.; Gueorguiev, B.; Keller, G.; Schmidutz, F.; Döbele, S.; Schröter, S.; Ihle, C. Increased tibial tubercle-trochlear groove and patellar height indicate a higher risk of recurrent patellar dislocation following medial reefing. Knee. Surg. Sports Traumatol. Arthrosc. 2021. [Google Scholar] [CrossRef]
- Longo, U.G.; Rizzello, G.; Ciuffreda, M.; Loppini, M.; Baldari, A.; Maffulli, N.; Denaro, V. Elmslie-Trillat, Maquet, Fulkerson, Roux Goldthwait, and Other Distal Realignment Procedures for the Management of Patellar Dislocation: Systematic Review and Quantitative Synthesis of the Literature. Arthroscopy 2016, 32, 929–943. [Google Scholar] [CrossRef] [PubMed]
- Schlichte, L.M.; Sidharthan, S.; Green, D.W.; Parikh, S.N. Pediatric Management of Recurrent Patellar Instability. Sports Med. Arthrosc. Rev. 2019, 27, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Marsh, J.S.; Daigneault, J.P.; Sethi, P.; Polzhofer, G.K. Treatment of recurrent patellar instability with a modification of the Roux-Goldthwait technique. J. Pediatr. Orthop. 2006, 26, 461–465. [Google Scholar] [CrossRef]
- Felli, L.; Capello, A.G.; Lovisolo, S.; Chiarlone, F.; Alessio-Mazzola, M. Goldthwait technique for patellar instability: Surgery of the past or here to stay procedure? A systematic review of the literature. Musculoskelet. Surg. 2019, 103, 107–113. [Google Scholar] [CrossRef]
- Galeazzi, R. Nuove appliccazioni del trapianto musculare e tendineo [in Italian]. Ard. Di Orthop. Milano 1922, 38, 8. [Google Scholar]
- Nietosvaara, Y.; Paukku, R.; Palmu, S.; Donell, S.T. Acute patellar dislocation in children and adolescents. Surgical technique. J. Bone Jt. Surg. Am. 2009, 91 Pt 1 (Suppl. 2), 139–145. [Google Scholar] [CrossRef]
- Giordano, M.; Falciglia, F.; Aulisa, A.G.; Guzzanti, V. Patellar dislocation in skeletally immature patients: Semitendinosous and gracilis augmentation for combined medial patellofemoral and medial patellotibial ligament reconstruction. Knee. Surg. Sports Traumatol. Arthrosc. 2012, 20, 1594–1598. [Google Scholar] [CrossRef]
- Grannatt, K.; Heyworth, B.E.; Ogunwole, O.; Micheli, L.J.; Kocher, M.S. Galeazzi semitendinosus tenodesis for patellofemoral instability in skeletally immature patients. J. Pediatr. Orthop. 2012, 32, 621–625. [Google Scholar] [CrossRef]
- Grammont, P.M.; Latune, D.; Lammaire, I.P. Treatment of subluxation and dislocation of the patella in the child. Elmslie technic with movable soft tissue pedicle (8 year review). Orthopade 1985, 14, 229–238. [Google Scholar]
- Kraus, T.; Lidder, S.; Svehlik, M.; Rippel, K.; Schneider, F.; Eberl, R.; Linhart, W. Patella re-alignment in children with a modified Grammont technique. Acta Orthop. 2012, 83, 504–510. [Google Scholar] [CrossRef] [PubMed]
- Oliva, F.; Ronga, M.; Longo, U.G.; Testa, V.; Capasso, G.; Maffulli, N. The 3-in-1 procedure for recurrent dislocation of the patella in skeletally immature children and adolescents. Am. J. Sports Med. 2009, 37, 1814–1820. [Google Scholar] [CrossRef] [PubMed]
- Danino, B.; Deliberato, D.; Abousamra, O.; Singh, S.; Klingele, K. Four-in-one Extensor Realignment for the Treatment of Obligatory or Fixed, Lateral Patellar Instability in Skeletally Immature Knee. J. Pediatr. Orthop. 2020, 40, 503–508. [Google Scholar] [CrossRef]
- Hinckel, B.B.; Lipinski, L.; Arendt, E.A. Concepts of the Distal Medial Patellar Restraints: Medial Patellotibial Ligament and Medial Patellomeniscal Ligament. Sports Med. Arthrosc. Rev. 2019, 27, 143–149. [Google Scholar] [CrossRef]
- Ambra, L.F.; Franciozi, C.E.; Phan, A.; Faloppa, F.; Gomoll, A.H. Isolated MPTL reconstruction fails to restore lateral patellar stability when compared to MPFL reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2021, 29, 793–799. [Google Scholar] [CrossRef] [PubMed]
- Aicale, R.; Maffulli, N. Combined medial patellofemoral and medial patellotibial reconstruction for patellar instability: A PRISMA systematic review. J. Orthop. Surg. Res. 2020, 15, 529. [Google Scholar] [CrossRef]
- Longo, U.G.; Vincenzo, C.; Mannering, N.; Ciuffreda, M.; Salvatore, G.; Berton, A.; Denaro, V. Trochleoplasty techniques provide good clinical results in patients with trochlear dysplasia. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 2640–2658. [Google Scholar] [CrossRef] [PubMed]
- Pesenti, S.; Blondel, B.; Armaganian, G.; Parratte, S.; Bollini, G.; Launay, F.; Jouve, J.-L. The lateral wedge augmentation trochleoplasty in a pediatric population: A 5-year follow-up study. J. Pediatr. Orthop. B 2017, 26, 458–464. [Google Scholar] [CrossRef]
- Tan, S.H.S.; Tan, L.Y.H.; Lim, A.K.S.; Hui, J.H. Hemiepiphysiodesis is a potentially effective surgical management for skeletally immature patients with patellofemoral instability associated with isolated genu valgum. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 845–849. [Google Scholar] [CrossRef]
- Parikh, S.N.; Redman, C.; Gopinathan, N.R. Simultaneous treatment for patellar instability and genu valgum in skeletally immature patients: A preliminary study. J. Pediatr. Orthop. B 2019, 28, 132–138. [Google Scholar] [CrossRef]
- Atkin, D.M.; Fithian, D.C.; Marangi, K.S.; Stone, M.L.; Dobson, B.E.; Mendelsohn, C. Characteristics of patients with primary acute lateral patellar dislocation and their recovery within the first 6 months of injury. Am. J. Sports Med. 2000, 28, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Thomee, P.; Thomee, R.; Karlsson, J. Patellofemoral pain syndrome: Pain, coping strategies and degree of well-being. Scand. J. Med. Sci. Sports 2002, 12, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Maenpaa, H.; Lehto, M.U. Patellofemoral osteoarthritis after patellar dislocation. Clin. Orthop. Relat. Res. 1997, 339, 156–162. [Google Scholar]
Figure 1.
Trochlear dysplasia classification by DeJour et al. [14]. Type A: shallow trochlea with the crossing sign. Type B: flat or convex trochlea; crossing sign and trochlear spur are present. Type C: asymmetric trochlear facets; crossing sign and double-contour signs are present. Type D: crossing sign, supratrochlear spur, and double-contour signs are all present; vertical cliff pattern can be seen.
Figure 1.
Trochlear dysplasia classification by DeJour et al. [14]. Type A: shallow trochlea with the crossing sign. Type B: flat or convex trochlea; crossing sign and trochlear spur are present. Type C: asymmetric trochlear facets; crossing sign and double-contour signs are present. Type D: crossing sign, supratrochlear spur, and double-contour signs are all present; vertical cliff pattern can be seen.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Familiari, F.; Cetik, R.M.; Huri, G. Patellar Instability in Pediatric Patients: Review of the Literature. Osteology 2021, 1, 197-208. https://0-doi-org.brum.beds.ac.uk/10.3390/osteology1040019
AMA Style
Familiari F, Cetik RM, Huri G. Patellar Instability in Pediatric Patients: Review of the Literature. Osteology. 2021; 1(4):197-208. https://0-doi-org.brum.beds.ac.uk/10.3390/osteology1040019
Chicago/Turabian StyleFamiliari, Filippo, Riza Mert Cetik, and Gazi Huri. 2021. "Patellar Instability in Pediatric Patients: Review of the Literature" Osteology 1, no. 4: 197-208. https://0-doi-org.brum.beds.ac.uk/10.3390/osteology1040019