PANS/PANDAS: Clinical Experience in IVIG Treatment and State of the Art in Rehabilitation Approaches

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
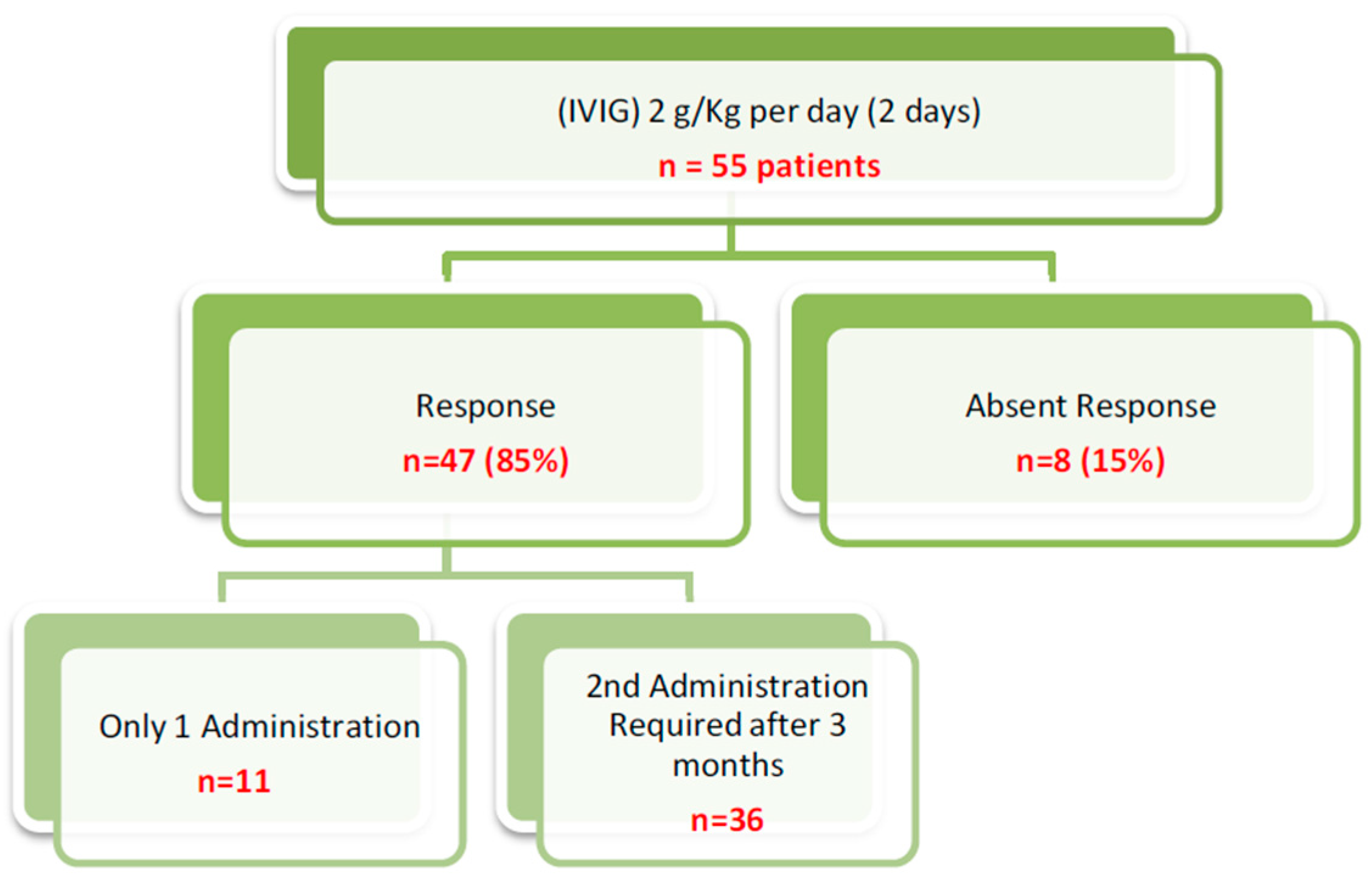
3. Results
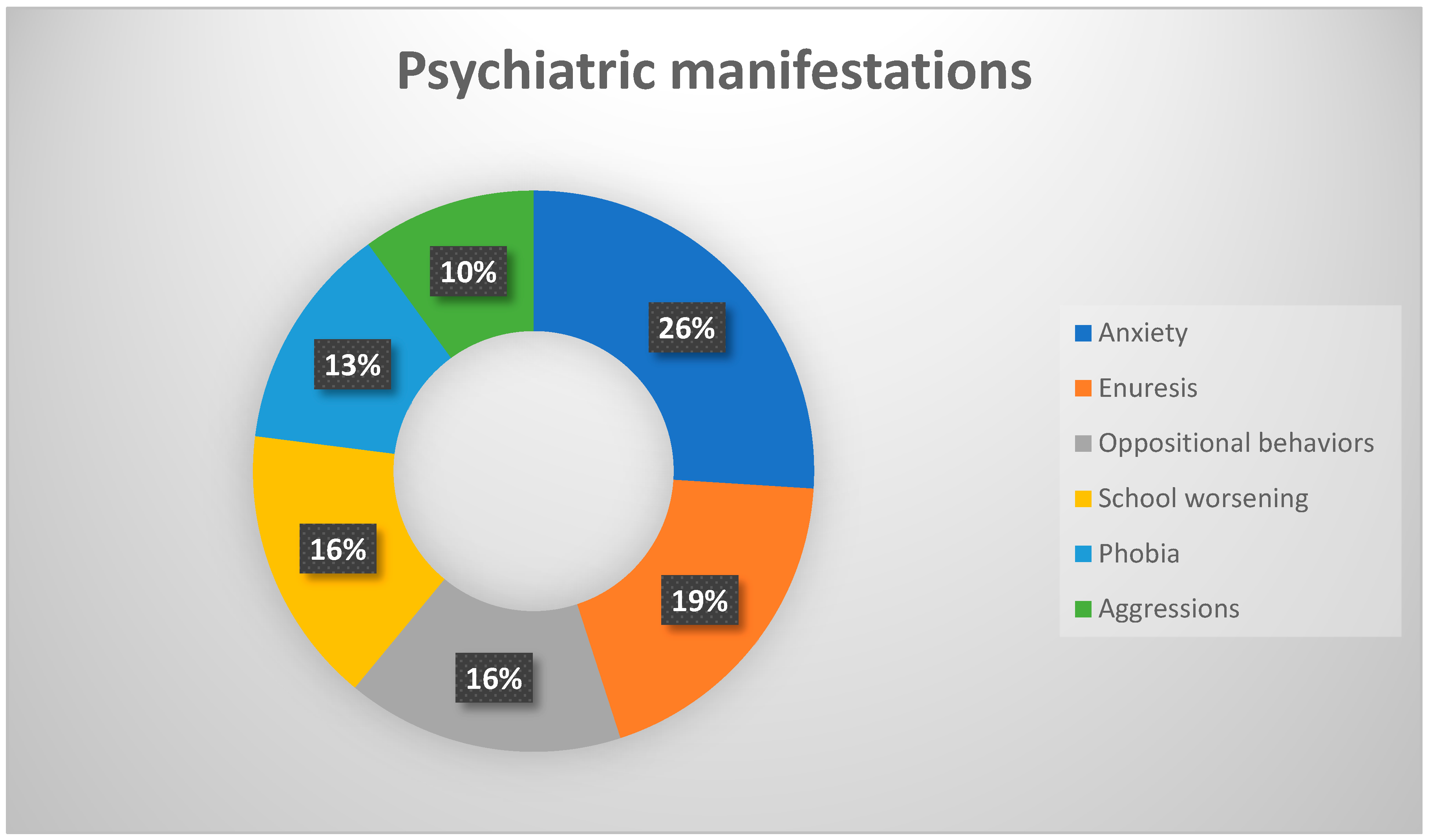
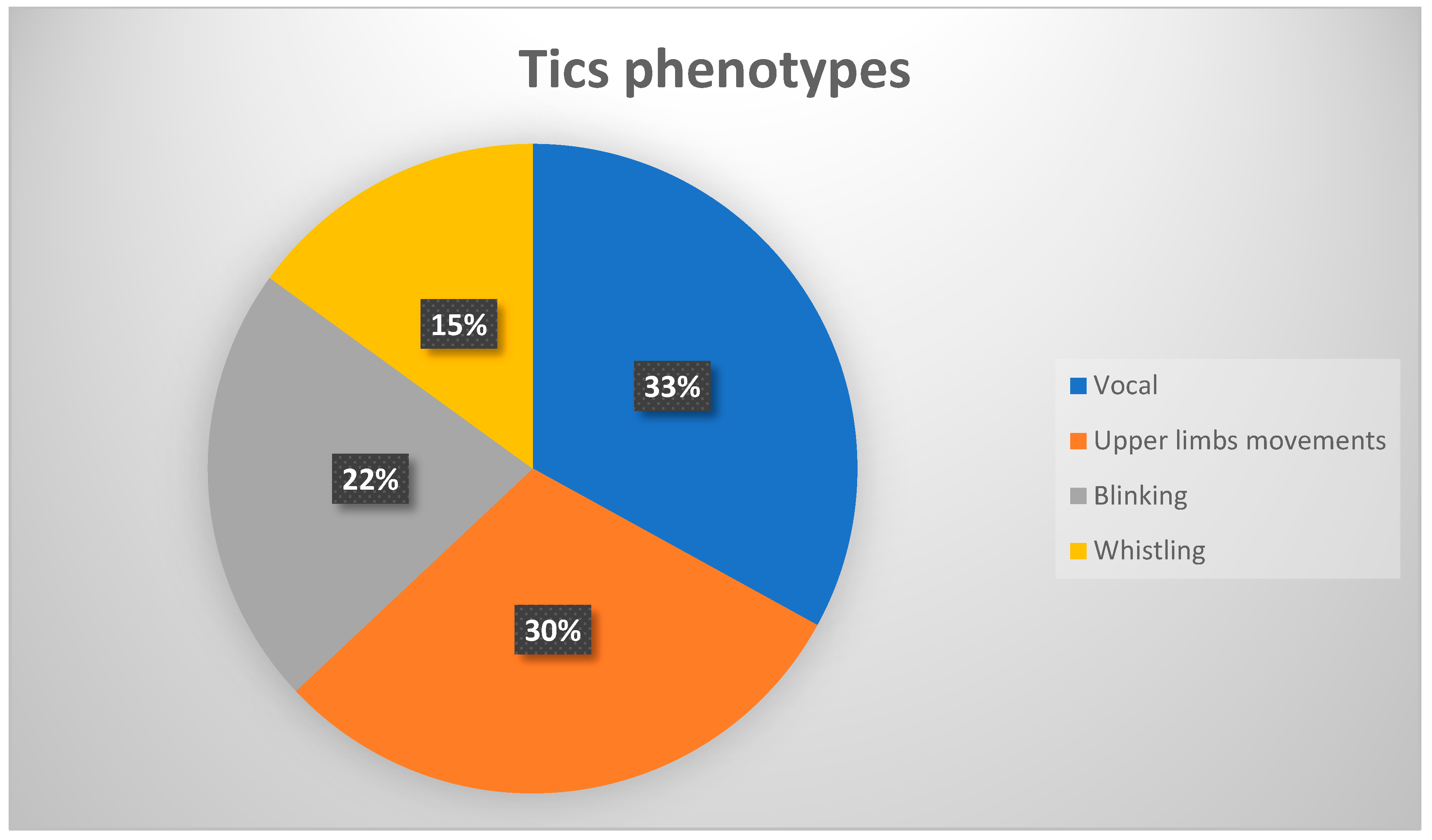
3.1. Clinical
3.2. Laboratory
3.3. Other Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Swedo, S.E.; Leonard, H.L.; Garvey, M.; Mittleman, B.; Allen, A.J.; Perlmutter, S.; Lougee, L.; Dow, S.; Zamkoff, J.; Dubbert, B.K. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections: Clinical description of the first 50 cases. Am. J. Psychiatry. 1998, 155, 264–271. [Google Scholar] [CrossRef]
- Frankovich, J.; Thienemann, M.; Pearlstein, J.; Crable, A.; Brown, K.; Chang, K. Multidisciplinary clinic dedicated to treating youth with pediatric acute-onset neuropsychiatric syndrome: Presenting characteristics of the first 47 consecutive patients. J. Child Adolesc. Psychopharmacol. 2015, 25, 38–47. [Google Scholar] [CrossRef] [Green Version]
- Swedo, S.E.; Seidlitz, J.; Kovacevic, M.; Latimer, M.E.; Hommer, R.; Lougee, L.; Grant, P. Clinical presentation of pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections in research and community settings. J. Child Adolesc. Psychopharmacol. 2015, 25, 26–30. [Google Scholar] [CrossRef] [Green Version]
- Macerollo, A.; Martino, D. Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS): An Evolving Concept. Tremor Other Hyperkinet Mov. 2013, 3. [Google Scholar] [CrossRef]
- Pavone, P.; Parano, E.; Rizzo, R.; Trifiletti, R.R. Autoimmune neuropsychiatric disorders associated with streptococcal infection: Sydenham chorea, PANDAS, and PANDAS variants. J. Child Neurol. 2006, 21, 727–736. [Google Scholar] [CrossRef] [PubMed]
- Singer, H.S.; Gilbert, D.L.; Wolf, D.S.; Mink, J.W.; Kurlan, R. Moving from PANDAS to CANS. J. Pediatr. 2012, 160, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, M.W. Post-streptococcal autoimmune sequelae: Rheumatic fever and beyond. In Streptococcus Pyogenes: Basic Biology to Clinical Manifestations; Ferretti, J.J., Stevens, D.L., Fischetti, V.A., Eds.; University of Oklahoma Health Sciences Center: Oklahoma City, OK, USA, 2016. [Google Scholar]
- Swedo, S.E.; Leckman, J.; Rose, N. From research subgroup to clinical syndrome: Modifying the PANDAS criteria to describe PANS (pediatric acute-onset neuropsychiatric syndrome). Pediatr. Ther. 2012, 2, 1–8. [Google Scholar] [CrossRef]
- Baj, J.; Sitarz, S.; Forma, A.; Wròblewska, K.; Juchnowicz, H.K. Alterations in the Nervous System and Gut Microbiota after B-Hemolytic Streptococcus Group A Infection—Characteristics and Diagnostic Criteria of PANDAS Recognition. Int. J. Mol. Sci. 2020, 21, 1476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, K.; Frankovich, J.; Cooperstock, M.; Cunningham, M.W.; Latimer, M.E.; Murphy, T.K.; Pasternack, M.; Thienemann, M.; Williams, K.; Walter, J.; et al. PANS Collaborative Consortium. Clinical evaluation of youth with pediatric acute-onset neuropsychiatric syndrome (PANS): Recommendations from the 2013 PANS Consensus Conference. J. Child Adolesc. Psychopharmacol. 2015, 3–13. [Google Scholar] [CrossRef] [Green Version]
- Pavone, P.; Rapisarda, V.; Serra, A.; Nicita, F.; Spalice, A.; Parano, E.; Rizzo, R.; Maiolino, L.; Di Mauro, P.; Vitaliti, G.; et al. Pediatric autoimmune neuropsychiatric disorder associated with group a streptococcal infection: The role of surgical treatment. Int. J. Immunopathol. Pharm. 2014, 27, 371–378. [Google Scholar]
- Sigra, S.; Hesselmark, E.; Bejerot, S. Treatment of PANDAS and PANS: A systematic review. Neurosci. Biobehav. Rev. 2018, 86, 51–65. [Google Scholar] [CrossRef] [PubMed]
- Perlmutter, S.J.; Leitman, S.F.; Garvey, M.A.; Hamburger, S.; Feldman, E.; Leonard, H.L.; Swedo, S.E. Therapeutic plasma exchange and intravenous immunoglobulin for obsessive-compulsive disorder and tic disorders in childhood. Lancet 1999, 354, 1153–1158. [Google Scholar] [CrossRef]
- Williams, K.A.; Swedo, S.E.; Farmer, C.A.; Grantz, H.; Grant, P.J.; D’Souza, P.; Hommer, R.; Katsovich, L.; King, R.A.; Leckman, J.F. Randomized, Controlled Trial of Intravenous Immunoglobulin for Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections. J. Am. Acad. Child Adolesc. Psychiatry. 2016, 55, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Kovacevic, M.; Grant, P.; Swedo, S.E. Use of intravenous immunoglobulin in the treatment of twelve youths with pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections. J. Child Adolesc. Psychopharmaco 2015, 25, 65–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frankovich, J.; Swedo, S.; Murphy, T. Clinical Management of Pediatric Acute-Onset Neuropsychiatric Syndrome: Part II-Use of Immunomodulatory Therapies. J. Child. Adolesc. Psychopharmacol. 2017, 27, 574–593. [Google Scholar] [CrossRef]
- Swedo, S.E.; Leonard, H.L.; Schapiro, M.B.; Casey, B.J.; Mannheim, G.B.; Lenane, M.C. Sydenham’s chorea: Physical and psychological symptoms of St Vitus dance. Pediatrics 1993, 91, 706–713. [Google Scholar] [PubMed]
- Pavone, P.; Falsaperla, R.; Nicita, F.; Zecchini, A.; Battaglia, C.; Spalice, A.; Iozzi, L.; Parano, E.; Vitaliti, G.; Verrotti, A.; et al. Pediatric Autoimmune Neuropsychiatric Disorder Associated with Streptococcal Infection (PANDAS): Clinical Manifestations, IVIG Treatment Outcomes, Results from a Cohort of Italian Patients. NNBN 2018, 8, 854–860. [Google Scholar] [CrossRef]
- Spinello, C.; Laviola, G.; Macri, S. Pediatric Autoimmune Disorders Associated with Streptococcal Infections and Tourette’s Syndrome in Preclinical Studies. Front. Neuroendocrinol. 2016, 10, 310. [Google Scholar] [CrossRef]
- Hommer, R.E.; Buckley, A.; Swedo, S.E. New onset sleep disturbances and PSG findings in children with acute or subacute neuro-psychiatric changes. In Abstract Submitted to 2014 AACAP Annual Meeting; AACAP: Washington, DC, USA, 2014. [Google Scholar]
- Citak, E.C.; Gucuyener, K.; Karabacak, N.I.; Serdaroğlu, A.; Okuyaz, C.; Aydin, K. Functional brain imaging in Sydenham’s chorea and streptococcal tic disorders. J. Child. Neurol. 2004, 19, 387–390. [Google Scholar] [CrossRef]
- Kumar, A.; Williams, M.T.; Chugani, H.T. Evaluation of basal ganglia and thalamic inflammation in children with pediatric autoimmune neuropsychiatric disorders associated with streptococcal infection and Tourette syndrome: A positron emission tomographic (PET) study using 11C-[R]-PK11195. J. Child Neurol. 2015, 30, 749–756. [Google Scholar] [CrossRef]
- Pediatric OCD Treatment Study (POTS) Team. Cognitive-behavior therapy, sertraline, and their combination for children and adolescents with obsessive-compulsive disorder: The Pediatric OCD Treatment Study (POTS) randomized controlled trial. JAMA 2004, 292, 1969–1976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hollis, C.; Pennant, M.; Cuenca, J.; Glazebrook, C.; Kendall, T.; Whittington, C.; Stockton, S.; Larsson, L.; Bunton, P.; Dobson, S.; et al. Clinical effectiveness and patient perspectives of different treatment strategies for tics in children and adolescents with Tourette syndrome: A systematic review and qualitative analysis. Health Technol. Assess. Rep. 2016, 20, 1–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grant, J.E. Clinical practice: Obsessive-compulsive disorder. N. Engl. J. Med. 2014, 371, 646–653. [Google Scholar] [CrossRef] [PubMed]
- Murphy, T.K.; Kurlan, R.; Leckman, J. The immunobiology of Tourette’s disorder, pediatric autoimmune neuropsychiatric disorders associated with Streptococcus, and related disorders: A way forward. J. Child Adolesc. Psychopharmacol. 2010, 20, 317–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gamucci, A.; Uccella, S.; Sciarretta, L.; D’Apruzzo, M.; Calevo, M.G.; Mancardi, M.M.; Veneselli, E.; De Grandis, E. PANDAS and PANS: Clinical, Neuropsychological, and Biological Characterization of a Monocentric Series of Patients and Proposal for a Diagnostic Protocol. J. Child Adolesc. Psychopharmacol. 2019, 29, 305–312. [Google Scholar] [CrossRef] [Green Version]
- Okumura, R.; Yamazaki, S.; Ohashi, T.; Magara, S.; Tohyama, J.; Sakuma, H.; Hayashi, M.; Saitoh, A. Neuropsychiatric Disorder Associated with Group G Streptococcus Infection. Case. Rep. Pediatr. 2018, 23. [Google Scholar] [CrossRef] [Green Version]
- Cocuzza, S.; Marino, S.; Gulino, A.; Pustorino, E.; Murabito, P.; Maniaci, A.; Sabino, L.; Taibi, R.; Di Luca, M.; Falsaperla, R.; et al. ENT involvement and orobuccal movements’ disorders in Pandas patients: Assessment and rehabilitations tools. Eur. Rev. Med. Pharm. Sci. 2019, 23, 4110–4117. [Google Scholar]
- Sokol, M.S. Infection-triggered anorexia nervosa in children: Clinical description of four cases. J. Child Adolesc. Psychopharmacol. 2000, 10, 133–145. [Google Scholar] [CrossRef]
- Tona, J.T.; Bhattacharjya, S.; Calaprice, D. Impact, of PANS and PANDAS exacerbations on occupational performance: A mixed-methods study. Am. J. Occup. Ther. 2017, 71, 7103220020P1–7103220020P9. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Severity Grade | Total Score |
|---|---|
| Subclinical | 0–7 |
| Mild | 8–15 |
| Moderate | 16–23 |
| Severe | 24–31 |
| Extreme | 32–40 |
| Severity Grade | Start | After IVIG |
|---|---|---|
| Subclinical | 0 | 12 |
| Mild | 0 | 22 |
| Moderate | 0 | 9 |
| Severe | 0 | 4 |
| Extreme | 55 | 8 |
| Patients | Patients |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pavone, P.; Falsaperla, R.; Cacciaguerra, G.; Sapuppo, A.; Chiaramonte, R.; Lubrano, R.; Messina, G.; Sciuto, S.; Sabino, L.; Cocuzza, S.; et al. PANS/PANDAS: Clinical Experience in IVIG Treatment and State of the Art in Rehabilitation Approaches. NeuroSci 2020, 1, 75-84. https://0-doi-org.brum.beds.ac.uk/10.3390/neurosci1020007
Pavone P, Falsaperla R, Cacciaguerra G, Sapuppo A, Chiaramonte R, Lubrano R, Messina G, Sciuto S, Sabino L, Cocuzza S, et al. PANS/PANDAS: Clinical Experience in IVIG Treatment and State of the Art in Rehabilitation Approaches. NeuroSci. 2020; 1(2):75-84. https://0-doi-org.brum.beds.ac.uk/10.3390/neurosci1020007
Chicago/Turabian StylePavone, Piero, Raffaele Falsaperla, Giovanni Cacciaguerra, Annamaria Sapuppo, Rita Chiaramonte, Riccardo Lubrano, Giulia Messina, Sarah Sciuto, Luca Sabino, Salvatore Cocuzza, and et al. 2020. "PANS/PANDAS: Clinical Experience in IVIG Treatment and State of the Art in Rehabilitation Approaches" NeuroSci 1, no. 2: 75-84. https://0-doi-org.brum.beds.ac.uk/10.3390/neurosci1020007