Functional Outcome in Patients with Dural Arteriovenous Fistulae after Surgical Treatment


Department of Neurosurgery, Klinikum rechts der Isar, Technical University Munich, 22, 81675 Munich, Germany
*
Author to whom correspondence should be addressed.
Surgeries 2020, 1(2), 54-62; https://0-doi-org.brum.beds.ac.uk/10.3390/surgeries1020007
Submission received: 20 September 2020
/
Revised: 16 October 2020
/
Accepted: 19 October 2020
/
Published: 22 October 2020
Abstract
:Spinal dural arterio-venous fistulas (SDAVF) are rare vascular pathologies. Degree of symptom improvement after surgery remains unclear. We evaluated surgically treated SDAVF patients for functional outcome and symptom improvement. Retrospective inclusion of consecutive patients treated surgically in our department between 2007–2019. We measured functional outcome using the McCormick Scale and modified Japanese Orthopaedic Association (mJOA) score. We included 27 patients with a median follow-up of 8.8 months (IQR 27.8). Mean age was 61.8 years (SD 8.4), 40.7% were female. Most frequent location was the thoracic spine in 15 (55.6%) followed by lumbar in 8 (29.6%), cervical in 3 (11.1%) and sacral spine in one patient (3.7%). Most common presenting symptom was progressive myelopathy (24/27 patients, 88.9%). In all patients the SDAVF was completely resected; however, four patients (14.8%) required a second surgery. Six patients (22.2%) deteriorated immediately after surgery with five recovering to baseline upon discharge. On discharge, presenting symptoms had improved in 17 patients (63%); 8/25 patients (32%) had a McCormick score of 1. Twenty (74.1%) continued to improve on follow-up. In total 23/27 patients (85.2%) improved. In the univariable analysis mJOA score on admission was associated with mJOA score on follow-up (coefficient 0.6, 95%CI 0.4–0.81, p < 0.001), whereas age was inversely associated (coefficient −0.1, 95%CI −0.19–0.01, p = 0.08). Untreated SDAVF leads to progressive myelopathy which may result in considerable disability. Surgical disconnection and resection provides a safe treatment option with low perioperative morbidity and excellent chances for symptom improvement or progression prevention.
1. Introduction
Spinal dural arteriovenous fistulas (DAVF) are a rare form of vascular malformation, but the most common vascular malformation of the spinal cord despite its low incidence [1,2]. Men are more commonly affected with a 5:1 ratio, mean age at diagnoses ranges between 55–60, the most frequent location is the thoracolumbar spine [3]. High cervical SDAVF occur in about 2% [4].
The exact aetiology remains unknown; however, it is believed that they are acquired lesions although they are sometimes already found in the perinatal period [5]. Factors associated with the development of SDAVF are venous hypertension, as well as venous thrombosis [6,7]. A previous study found that most SDAVF seem to occur spontaneously, or at least no obvious reason is found, but a traumatic cause cannot be ruled out in many cases [8]. The location of the AV shunt is inside the dura where arterial blood from a radiculomeningeal artery enters a radicular vein, close to the spinal nerve [5]. They are generally fed by a branch of the segmental radicular artery supplying the dura; the venous drainage occurs by a corresponding radicular vein [9]. Compromise of the venous outflow is caused by pressure of the radicular artery to the draining vein leading to congestion of the spinal cord by a diminished AV gradient and a decreased drainage of normal veins consecutively frequently causing progressive myelopathy [10,11,12]. Other symptoms that have been described are lumbar back pain and radicular pain [13]. Symptoms are often ascending. In exceptionally rare cases the SDAVF might cause a subarachnoid haemorrhage; it seems to occur only in SDAVF at the level of the foramen magnum [14]. Even though previous reports and reviews exist, information on longer-term outcome after surgical treatment remains limited.
Our aim is to retrospectively review our dataset for all surgically treated cases of SDAVF and to evaluate early and late postoperative functional outcome with a special emphasis on myelopathy.
2. Materials and Methods
2.1. Data Collection
Hospital Based Cohort Study
We retrospectively reviewed prospectively collected clinical and radiological databases of patients with SDAVF treated in our neurosurgical unit between 2009–2020. Our inclusion criteria were patient over 18 years with proven SDAVF who were treated by surgical removal of the fistula. Patient treated by endovascular intervention only were excluded. We collected data on patient demographic, previous medical history, imaging, discharge data and, where available, follow-up data from electronical medical records. Our primary outcome was to evaluate the functional outcome on follow-up with the secondary outcome being functional outcome at discharge.
Except for patients presenting with subarachnoid haemorrhage, we measured functional outcome using the modified McCormick Scale as well as the modified Japanese Orthopaedic Association (mJOA) score on admission as well as at discharge and follow-up [15,16]. The McCormick Scale is divided into 1 = neurologically intact, 2 = mild motor or sensory deficit, but functional independence, 3 = moderate deficit and limitation of function, 4 = severe motor or sensory deficit, dependent, 5 = paraplegia or quadriplegia [17].
2.2. Statistical Analysis
Categorical variables will be presented as count and percentage, continuous variables as mean with standard deviation (SD). For association analysis we used the nonparametric Wilcoxon matched-pairs signed-ranks test as well as logistic regression where appropriate. All testing was done at a 0.05 significance level.
Statistical analysis was done using STATA 15 (StataCorp. 2011. Stata Statistical Software: Release 15. StataCorp LP, College Station, TX, USA).
2.3. Ethical Approval
The data collection was approved by the local Ethics Committee (reference: 271/20 S-EB). All procedures performed in studies involving human participants were in accordance with the ethical standards of the local Ethics Committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study, formal consent is not required.
3. Results
3.1. Hospital-Based Cohort Study
We identified 27 patients which were treated surgically for a SDAVF at our institution between January 2007 and March 2019. See Table 1 for baseline characteristics. Mean age was 61.8 years (SD 8.4) and 40.7% were female. Most frequent location was the thoracic spine in 15 (55.6%) followed by the lumbar spine in 8 (29.6%), the cervical spine in 3 (11.1%) and the sacral spine in one patient (3.7%). Most patients presented with progressive myelopathy (24/27, 88.9%); 8/25 patients also reported painful sensations (32%). Three patients (11.1%) reported to have undergone previous spinal interventions and one patient (3.7%) reported a major trauma in his past medical history. Two patients (7.4%) presented with acute symptom onset and decreased Glasgow Coma Scale of 9 and 3, respectively. Computed tomography (CT) scan showed an acute subarachnoid haemorrhage in both patients, one needing a temporary extraventricular drain (EVD) due to acute hydrocephalus. Both patients were diagnosed with foramen magnum SDAVF. These two patients were excluded from the McCormick Scale and mJOA score evaluation.
Only in one patient, the SDAVF was an incidental finding, as imaging had been conducted due to an unrelated cause.
3.2. Treatment
In three patients (11.1%), the SDAVF was embolized before surgery: two of them underwent embolization in an external hospital prior to admission to our clinic. The third patient was treated for a ruptured cranio-cervical fistula and received endovascular embolization to reduce the intraoperative haemorrhage risk. Surgery was performed mainly via hemilaminectomy/-laminoplasty of the according level with opening of the dura, coagulation and disconnection of the fistula point. Complete removal was then verified by means of a microdoppler and postoperative angiography performed within 48 h after surgery. All patients were monitored during the intervention using electrophysiological monitoring. Complete resection was achieved in all patients; however, in four patients (14.8%), a second surgical intervention was required to achieve a complete resection as a rest was seen in the postoperative angiography. Six patients (22.2%) deteriorated immediately after surgery of whom five recovered back to their baseline level within 48 h. Postoperative imaging showed an epidural haematoma in three of these cases. In one case the patient underwent revision surgery for evacuation of the haematoma. One patient had a persistent cerebrospinal fluid leak and underwent surgery for closure of the leak.
3.3. Functional Outcome on Discharge and Follow-Up
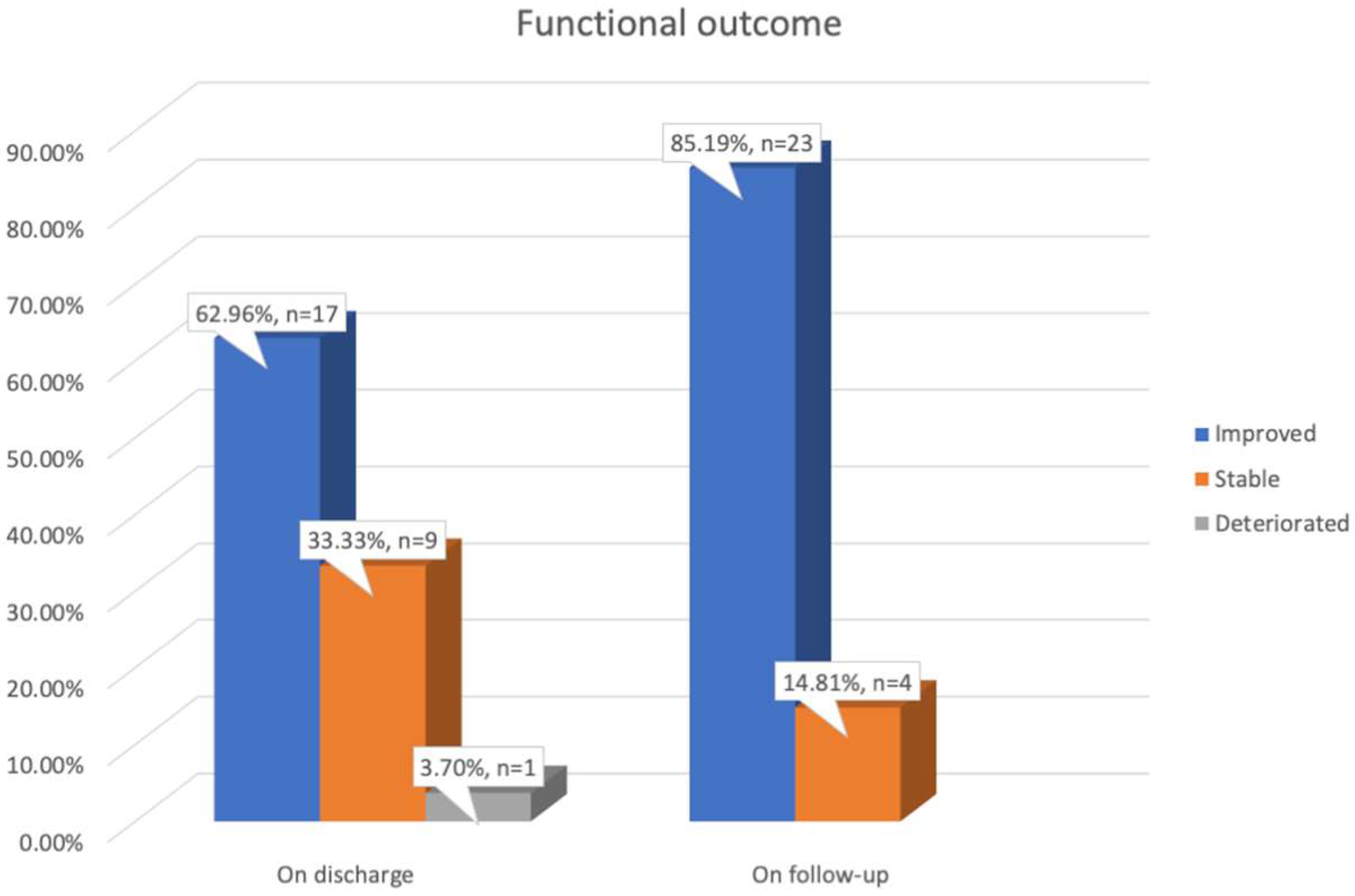
On discharge, presenting symptoms had significantly improved in 17 patients (63%). Excluding patients presenting with a subarachnoid haemorrhage; 8/25 patients (32%) had a McCormick Scale of 1 and 5 (20%) of 2; the mean mJOA score was 14.2 (SD 2.8). Follow-up was available for all patients. The median time to follow-up was 8.8 months (IQR 27.8, minimum 0.5, maximum 99). On follow-up, 19 patients (70.4%) continued to improve. Overall, 23/27 patients (85.2%) had improved between surgery and discharge or follow-up (see Figure 1). One patient who had deteriorated after surgery had not recovered to his presurgical functional level when discharged. This patient showed back to baseline recovery upon follow-up, but no improvement compared to the presurgical functional state.
Objective functional improvement comparing preoperative mJOA and mJOA score at follow-up as well as preoperative McCormick Scale and McCormick Scale on follow-up were both significant (p < 0.001 and p = 0.02, respectively). Both patients presenting with subarachnoid haemorrhage improved significantly when comparing their preoperative and postoperative state with one patient regaining consciousness and being able to mobilize.
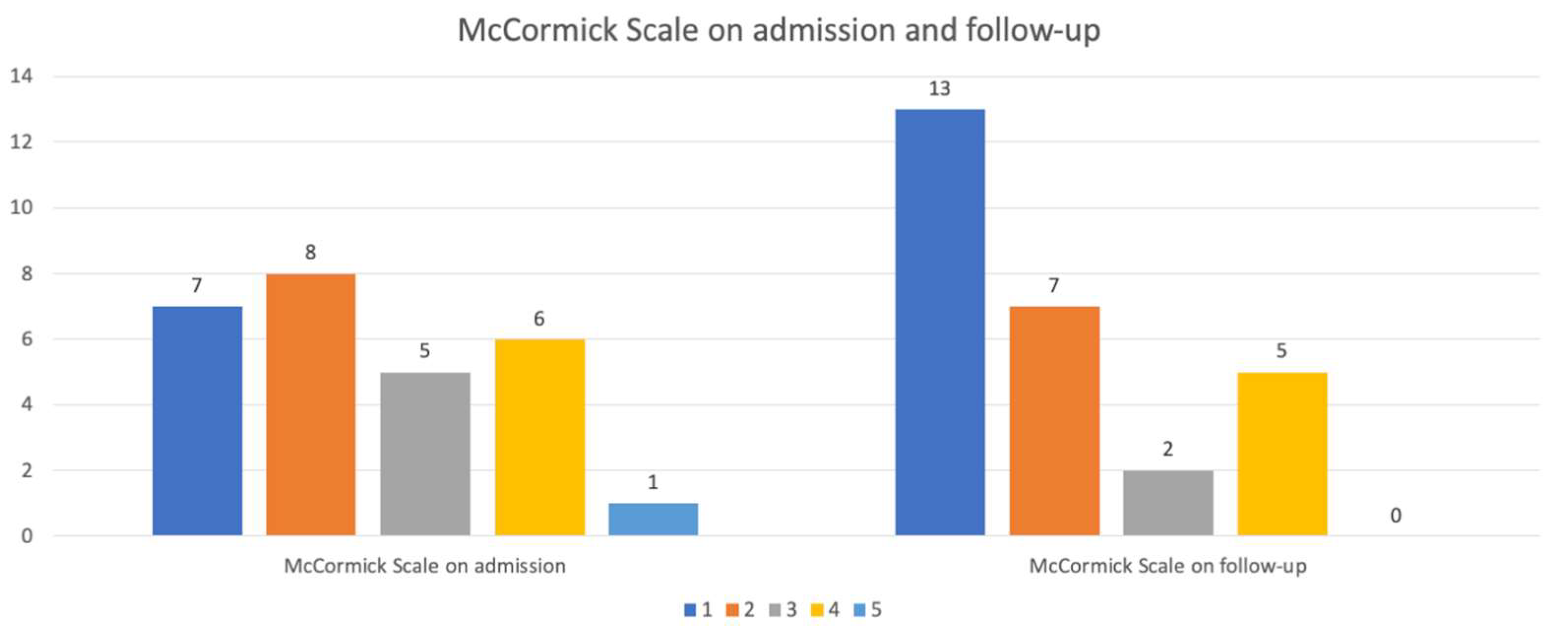
Six out of the 25 patients (24%) demonstrated a mJOA score of 18 and 7 (28%) a value on the McCormick Scale of 1 indicating no remaining symptoms or only mild remaining dysaesthesia. No patient with a mJOA score of <16 achieved a score of 18 on follow-up and only one patient with a McCormick Scale value of 4 on admission had a value of 1 on follow-up, indicating no remaining neurological symptoms. See Figure 2 for comparison of the McCormick Scale on admission and on follow-up.
In the univariable analysis the mJOA score on admission was directly associated with mJOA score on follow-up (coefficient 0.6, 95%CI 0.4–0.81, p < 0.001). We found evidence, that age was inversely associated with the mJOA score on follow-up; however, this finding was not statistically significant (coefficient −0.1, 95%CI −0.19–0.01, p = 0.08)
4. Discussion
In our hospital cohort study, we analysed functional outcome using the mJOA score and McCormick Scale in patients treated surgically for SDAVF. The most common presenting symptom was progressive myelopathy and the most frequent location was the thoracic spine. Already on discharge, presenting symptoms had improved in 17 patients (63%). Twenty patients (74.1%) continued to improve on follow-up. Overall, 23 patients (85.2%) improved. mJOA score on admission was directly associated with mJOA score on follow-up, whereas age was inversely associated with the mJOA score on follow-up.
The four patients (14.8%), who did not improve from a functional point of view, the progression of the disease was halted, and patients remained neurologically stable on follow-up, confirming previously reported data [8]. Additionally, we demonstrated that patients with higher mJOA score on admission had higher mJOA scores on follow-up. These observations indicate the importance of early surgery of oligosymptomatic patients as it at least allows to preserve the neurological status and ambulatory independence in daily life and in the majority of cases even improves symptoms of myelopathy. The risk of transient postoperative morbidity was 14.8% and the rate of remaining neurological impairment attributable to surgical intervention was 0%, which indicates that surgical resection provides a safe treatment option with relatively low perioperative morbidity and good chances for improvement or myelopathy progression prevention.
A recent meta-analysis compared outcome between surgically and endovascular treated patients [18]. They found an improved outcome for SDAVF in surgically compared to endovascular treated patients [18]. Improvement of symptoms following complete occlusion has been reported in about two-third of patients with sensory symptoms improving less frequently [19]. The improvement rate was higher in our cohort: overall, 85.2% reported a significant improvement of symptoms [19]. We confirm previous rates of complete occlusion: in our cohort, we achieved a 100% occlusion rate compared to a previously reported occlusion rate of about 98% [20], although four patients required a second surgical intervention to achieve complete occlusion.
Discussion in the literature about the best treatment option for SDAVF is ongoing. Surgical occlusion rate has been reported to be significantly higher reaching up to 98–100% compared to endovascular occlusion rate ranging between 25–75% [19,20,21]. One of the main issues with endovascular occlusion is the fact that embolization material needs to pass through the nidus and reach the venous site. Only if this can be achieved endovascular occlusion appears to be efficient [22]. A recent meta-analysis showed increasing occlusion rates with endovascular treatment compared to older publications [18,20,23]. This might be due to different reasons. The higher success rate reported in the meta-analysis conducted by Goyal et al. compared with previous studies and meta-analyses might be due to advances in endovascular techniques [18]. It might, however, also just demonstrate a more realistic success rate due to a larger number of patients [18]. Still, the reported failure rate of 19.8% with endovascular occlusion was significantly higher, compared to 2.8% with surgical occlusion; the late recurrence rate of 11.2%, was much higher with endovascular occlusion compared to 1.6% with surgical occlusion [18]. The rate of complications in both treatment groups did not differ significantly [18]. We are not able to draw any direct comparison between endovascular and surgical treatment as, according to our clinical standard based on the above-mentioned literature data, we operate all patients presenting with SDAVF.
Two of our patients presented with subarachnoid haemorrhage. Subarachnoid haemorrhage is a very rare presentation form for patients suffering from SDAVF and was previously described only in SDAVF of the craniocervical junction, which is in accordance with our observation [24,25]. One of our patients suffering a subarachnoid haemorrhage from SDAVF at the craniocervical junction had a favourable outcome with complete recovery and no remaining symptoms. The second patient, however, remained functionally dependent on follow-up. Patients suffering from subarachnoid haemorrhage due to an underlying SDAVF are thought to have a good functional outcome [24]. As SDAVF is a relatively rare pathology and subarachnoid haemorrhage from a SDAVF is even rarer we cannot draw any conclusion regarding the prediction of functional neurological outcome.
Our study does have limitations: this was a retrospective study. Information about the functional state of patients was deducted from discharge and outpatient clinic letters potentially leading to reporting bias. To establish the full extent of a patient’s functional state more accurately, this should ideally be addressed in a prospective study. Furthermore, due to the retrospective nature of the study, we were not able to collect information on symptom duration. Longer symptom duraiton might be a presumably negative predictor for postoperative functional recovery. This needs to be evaluated in future, prospectively conducted studies. Although we do report on a considerable large dataset, we are not able to provide any insights into the aetiology of this disease. Of note, one of our patients reported a significant previous trauma to approximately the level of later SDAVF and three patients reported to have undergone previous spinal interventions.
We were able to show that surgery is a safe treatment option significantly improving functional outcome in patients suffering from SDAVF in most cases or at least preventing functional deterioration. Additionally, we demonstrated an association between mJOA score on admission and patients age on functional outcome.
To gain more insight in factors influencing functional outcome, as well as natural history of SDAVF, an international registry for this pathology is needed.
5. Conclusions
Untreated SDAVF leads to progressive myelopathy which may result in considerable disability. In cases with advanced myelopathy a complete recovery is often not possible even after surgical intervention, but improvement of functional state is achievable in most patients. Surgical disconnection and resection provide a safe treatment option with low perioperative morbidity and excellent chances for improvement or at least prevention of myelopathy progression.
Author Contributions
Conceptualization, I.C.H., M.W., V.M.B. and B.M.; methodology I.C.H. and M.W.; formal analysis, I.C.H.; writing—original draft preparation, I.C.H. and M.W.; writing—review and editing, I.C.H., M.W., V.M.B. and B.M.; supervision, M.W. and B.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
Declaration
Some of the results pertinent to this manuscript were reported at the “14. Deutscher Wirbelsäulenkongress”. The manuscript itself however has not been published anywhere else [26].
References
- Spetzler, F.R.; Detwiler, P.W.; Riina, H.A.; Porter, R.W. Modified Classification of Spinal Cord Vascular Lesions. J. Neurosurg. 2002, 96, 145–156. [Google Scholar] [CrossRef] [Green Version]
- Ropper, E.A.; Gross, B.A.; Du, R. Surgical Treatment of Type I Spinal Dural Arteriovenous Fistulas. Neurosurg. Focus 2012, 32, E3. [Google Scholar] [CrossRef]
- Jellema, K.; Tijssen, C.C.; van Gijn, J. Spinal Dural Arteriovenous Fistulas: A Congestive Myelopathy That Initially Mimics a Peripheral Nerve Disorder. Brain 2006, 129, 3150–3164. [Google Scholar] [CrossRef] [PubMed]
- Reinges, M.H.; Thron, A.; Mull, M.; Huffmann, B.C.; Gilsbach, J.M. Dural Arteriovenous Fistulae at the Foramen Magnum. J. Neurol. 2001, 248, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Krings, T.; Geibprasert, S. Spinal Dural Arteriovenous Fistulas. AJNR Am. J. Neuroradiol. 2009, 30, 639–648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terada, T.; Higashida, R.T.; Halbach, V.V.; Dowd, C.F.; Tsuura, M.; Komai, N.; Wilson, C.B.; Hieshima, G.B. Development of Acquired Arteriovenous Fistulas in Rats Due to Venous Hypertension. J. Neurosurg. 1994, 80, 884–889. [Google Scholar] [CrossRef] [Green Version]
- Herman, J.M.; Spetzler, R.F.; Bederson, J.B.; Kurbat, J.M.; Zabramski, J.M. Genesis of a Dural Arteriovenous Malformation in a Rat Model. J. Neurosurg. 1995, 83, 539–545. [Google Scholar] [CrossRef]
- Aghakhani, N.; Parker, F.; David, P.; Lasjaunias, P.; Tadie, M. Curable Cause of Paraplegia: Spinal Dural Arteriovenous Fistulae. Stroke 2008, 39, 2756–2759. [Google Scholar] [CrossRef] [Green Version]
- Sorenson, T.; Giordan, E.; Cannizzaro, D.; Lanzino, G. Surgical Ligation of Spinal Dural Arteriovenous Fistula. Acta Neurochir. 2018, 160, 191–194. [Google Scholar] [CrossRef]
- Endo, T.; Endo, H.; Sato, K.; Matsumoto, Y.; Tominaga, T. Surgical and Endovascular Treatment for Spinal Arteriovenous Malformations. Neurol. Med. Chir. 2016, 56, 457–464. [Google Scholar] [CrossRef] [Green Version]
- Kataoka, H.; Miyamoto, S.; Nagata, I.; Ueba, T.; Hashimoto, N. Venous Congestion Is a Major Cause of Neurological Deterioration in Spinal Arteriovenous Malformations. Neurosurgery 2001, 48, 1224–1229. [Google Scholar]
- Hurst, R.W.; Kenyon, L.C.; Lavi, E.; Raps, E.C.; Marcotte, P. Spinal Dural Arteriovenous Fistula: The Pathology of Venous Hypertensive Myelopathy. Neurology 1995, 45, 1309–1313. [Google Scholar] [CrossRef] [PubMed]
- Jellema, K.; Canta, L.R.; Tijssen, C.C.; van Rooij, W.J.; Koudstaal, P.J.; van Gijn, J. Spinal Dural Arteriovenous Fistulas: Clinical Features in 80 Patients. J. Neurol. Neurosurg. Psychiatry. 2003, 74, 1438–1440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kai, Y.; Hamada, J.; Morioka, M.; Yano, S.; Mizuno, T.; Kuratsu, J. Arteriovenous Fistulas at the Cervicomedullary Junction Presenting with Subarachnoid Hemorrhage: Six Case Reports with Special Reference to the Angiographic Pattern of Venous Drainage. AJNR Am. J. Neuroradiol. 2005, 26, 1949–1954. [Google Scholar] [PubMed]
- Manzano, G.; Green, B.A.; Vanni, S.; Levi, A.D. Contemporary Management of Adult Intramedullary Spinal Tumors-Pathology and Neurological Outcomes Related to Surgical Resection. Spinal Cord 2008, 46, 540–546. [Google Scholar] [CrossRef]
- Benzel, E.C.; Lancon, J.; Kesterson, L.; Hadden, T. Cervical Laminectomy and Dentate Ligament Section for Cervical Spondylotic Myelopathy. J. Spinal Disord. 1991, 4, 286–295. [Google Scholar] [CrossRef]
- McCormick, P.C.; Torres, R.; Post, K.D.; Stein, B.M. Intramedullary Ependymoma of the Spinal Cord. J. Neurosurg. 1990, 72, 523–532. [Google Scholar] [CrossRef]
- Goyal, A.; Cesare, J.; Lu, V.M.; Alvi, M.A.; Kerezoudis, P.; Brinjikji, W.; Nasr, D.; Lanzino, G.; Bydon, M. Outcomes Following Surgical Versus Endovascular Treatment of Spinal Dural Arteriovenous Fistula: A Systematic Review and Meta-Analysis. J. Neurol. Neurosurg. Psychiatry. 2019, 90, 1139–1146. [Google Scholar] [CrossRef]
- Van Dijk, J.M.; TerBrugge, K.G.; Willinsky, R.A.; Farb, R.I.; Wallace, M.C. Multidisciplinary Management of Spinal Dural Arteriovenous Fistulas: Clinical Presentation and Long-Term Follow-up in 49 Patients. Stroke 2002, 33, 1578–1583. [Google Scholar] [CrossRef] [Green Version]
- Steinmetz, M.P.; Chow, M.M.; Krishnaney, A.A.; Andrews-Hinders, D.; Benzel, E.C.; Masaryk, T.J.; Mayberg, M.R.; Rasmussen, P.A. Outcome after the Treatment of Spinal Dural Arteriovenous Fistulae: A Contemporary Single-Institution Series and Meta-Analysis. Neurosurgery 2004, 55, 77–87. [Google Scholar] [CrossRef]
- Niimi, Y.; Berenstein, A.; Setton, A.; Neophytides, A. Embolization of Spinal Dural Arteriovenous Fistulae: Results and Follow-Up. Neurosurgery 1997, 40, 675–682. [Google Scholar] [CrossRef] [PubMed]
- Sherif, C.; Gruber, A.; Bavinzski, G.; Standhardt, H.; Widhalm, G.; Gibson, D.; Richling, B.; Knosp, E. Long-Term Outcome of a Multidisciplinary Concept of Spinal Dural Arteriovenous Fistulae Treatment. Neuroradiology 2008, 50, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Bakker, N.A.; Uyttenboogaart, M.; Luijckx, G.J.; Eshghi, O.S.; Mazuri, A.; Metzemaekers, J.D.; Groen, R.J.; Van Dijk, J.M. Recurrence Rates after Surgical or Endovascular Treatment of Spinal Dural Arteriovenous Fistulas: A Meta-Analysis. Neurosurgery 2015, 77, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Fassett, D.R.; Rammos, S.K.; Patel, P.; Parikh, H.; Couldwell, W.T. Intracranial Subarachnoid Hemorrhage Resulting from Cervical Spine Dural Arteriovenous Fistulas: Literature Review and Case Presentation. Neurosurg. Focus 2009, 26, E4. [Google Scholar] [CrossRef]
- Aviv, R.I.; Shad, A.; Tomlinson, G.; Niemann, D.; Teddy, P.J.; Molyneux, A.J.; Byrne, J.V. Cervical Dural Arteriovenous Fistulae Manifesting as Subarachnoid Hemorrhage: Report of Two Cases and Literature Review. AJNR Am. J. Neuroradiol. 2004, 25, 854–858. [Google Scholar]
- Julia Wrenczycki.14. Deutscher Wirbelsäulenkongress. Eur. Spine J. 2019, 28, 2660–2758. [Google Scholar] [CrossRef]
Figure 1.
Neurological state on discharge and on follow-up (improved vs. stable vs. deteriorated).
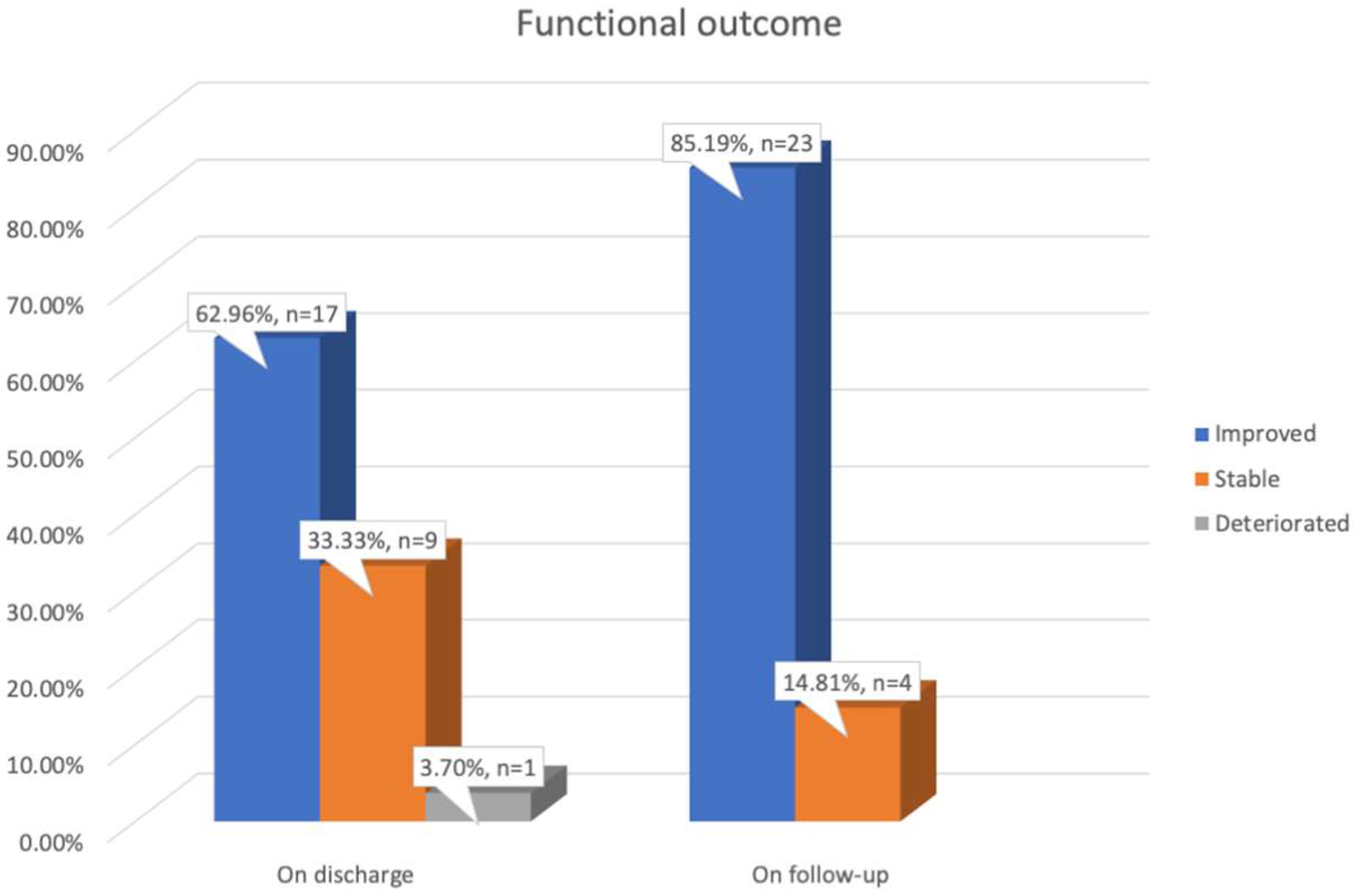
Figure 2.
McCormick Scale on admission compared to McCormick Scale on follow-up.

{kind=link}
{kind=link}
Table 1.
Baseline and outcome characteristics.
| Variable | Overall Cohort |
|---|---|
| Age, mean (SD) | 61.8 (8.4 SD) |
| Sex, N (%) | |
| 16 (59.3%) |
| 11 (40.7) |
| Symptoms N (%) | |
| 24 (88.9) |
| 10/25 (40) |
| 13/25 (52) |
| 9/25 (36) |
| 11/25 (44) |
| 8/25 (32) |
| 6/25 (24) |
| 2/25 (8) |
| 1/25 (4) |
| 2 (7.4) |
| Past medical history, N (%) | |
| 9 (33.3) |
| 2 (7.4) |
| 3 (11.1) |
| 1 (3.7) |
| Location, N (%) | |
| 3 (11.1) |
| 15 (55.6) |
| 8 (29.6) |
| 1 (3.7) |
| Duration of hospitalization, mean (SD) | 10.1 (6.8) |
| Functional state | |
| Cohort for spinal scores | 25/27 |
| mJOA score on admission, mean (SD) | 14 (2.9) |
| McCormick Scale on admission, N (%) | |
| 6 (24) |
| 8 (32) |
| 5 (20) |
| 6 (24) |
| mJOA score on discharge, mean (SD) | 14.2 (2.8) |
| McCormick Scale on discharge, N (%) | |
| 8 (32) |
| 5 (20) |
| 7 (28) |
| 4 (16) |
| 1 (4) |
| mJOA score on FU, mean (SD) | 15.5 (2.2) |
| McCormick Scale on FU, N (%) | |
| 12 (48) |
| 7 (28) |
| 2 (8) |
| 4 (16) |
FU = follow-up; mJOA = modified Japanese Orthopaedic Association; N = number; SD = standard deviation.
Table 2.
Predictors of dichotomized mJOA score on follow-up.
| Univariable Analysis | |||
|---|---|---|---|
| Coefficient | 95% CI | p-Value | |
| Age, mean (SD), N(%) | −0.1 | −0.19–0.01 | 0.08 |
| Female Sex, N(%) | −0.87 | −2.73–0.99 | 0.35 |
| Worsening after surgery | 0.85 | −1.3–3 | 0.42 |
| mJOA score on admission | 0.6 | 0.4–0.81 | <0.001 |
CI = confidence interval, mJOA = modified Japanese Orthopaedic Association, N = number, SD = standard deviation.
Table 3.
Predictors of McCormick Scale score on follow-up.
| Univariable Analysis | |||
|---|---|---|---|
| OR | 95%CI | p-Value | |
| Age, mean (SD), N(%) | 1.11 | 0.99–1.24 | 0.06 |
| Female Sex, N(%) | 0.4 | 0.09–1.85 | 0.24 |
CI = confidence interval, OR = Odds ratio, N = number, SD = standard deviation.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Hostettler, I.C.; Butenschoen, V.M.; Meyer, B.; Wostrack, M. Functional Outcome in Patients with Dural Arteriovenous Fistulae after Surgical Treatment. Surgeries 2020, 1, 54-62. https://0-doi-org.brum.beds.ac.uk/10.3390/surgeries1020007
AMA Style
Hostettler IC, Butenschoen VM, Meyer B, Wostrack M. Functional Outcome in Patients with Dural Arteriovenous Fistulae after Surgical Treatment. Surgeries. 2020; 1(2):54-62. https://0-doi-org.brum.beds.ac.uk/10.3390/surgeries1020007
Chicago/Turabian StyleHostettler, Isabel C, Vicki M Butenschoen, Bernhard Meyer, and Maria Wostrack. 2020. "Functional Outcome in Patients with Dural Arteriovenous Fistulae after Surgical Treatment" Surgeries 1, no. 2: 54-62. https://0-doi-org.brum.beds.ac.uk/10.3390/surgeries1020007