The Quality of Life Definition: Where Are We Going?


1
Department of Urology, Santa Chiara Regional Hospital, 38123 Trento, Italy
2
Institute of Clinical Medicine, University of Oslo, 0316 Oslo, Norway
3
Department of Urology, University of Salerno, Fisciano, 84084 Salerno, Italy
4
Department of Urology, Oslo University Hospital, 0450 Oslo, Norway
5
Institute of Clinical Medicine, University of Aarhus, 8000 Aarhus, Denmark
*
Author to whom correspondence should be addressed.
Uro 2021, 1(1), 14-22; https://0-doi-org.brum.beds.ac.uk/10.3390/uro1010003
Submission received: 5 February 2021
/
Revised: 15 February 2021
/
Accepted: 20 February 2021
/
Published: 25 February 2021
(This article belongs to the Special Issue Quality of Life and Patient Engagement: What News in Urology and Andrology?)
Abstract
:The quality of life (QoL) concept now includes new aspects related to patients’ well-being because QoL has become more of a personal perception than an an objective and measurable entity. Here, we discuss the principal aspects of QoL-related aspects in urology and andrology by using a narrative review. Some aspects concerning the QoL are essential when managing uro-andrological patients. The aim of treatments should not only include the absence of disease or symptoms relief but also the improvement of a patient’s QoL with regard to his/her internal status and relationship with others. In this sense, any therapeutic approach should be based on the patient’s perspectives and not only on the instrumental and laboratory findings. Finally, we discussed the role of a patient’s sexual partner adding an extra dimension to the patient-centerd approach as part of the QoL concept in andrology.
1. Introduction
Due to the improvements in medical care such as technical innovations, new drugs and new insights into the pathophysiology of urological diseases, the average life expectancy of patients has increased considerably in the last few decades [1]. However, improvement in life expectancy is not always linked with an improvement in quality of life (QoL). For this reason, all health-care practitioners are advised to pay attention to the QoL of urological patients [2]. In an editorial in the Annals of Internal Medicine, Elkington states, “What every physician wants for every one of his patients old or young, is not just the absence of death but life with a vibrant quality that we associate with a vigorous youth. This is nothing less than a humanistic biology that is concerned, not with material mechanisms alone, but with the wholeness of human life, with the spiritual quality of life that is unique to man” [2,3]. In this sense, all urologists and andrologists should improve their knowledge about QoL and the tools for QoL measurement. In doing so, urologists and andrologists can pioneer these ethical and professional perspectives in their respective medical fields. In everyday clinical practice, patient-centered medicine and patient engagement has a key role in improving the patient-doctor alliance and patients’ adherence to the treatment. The aim of the present paper is to give a narrative review of QoL-related aspects in urology and andrology in order to provide the reader with some simple tools to use in everyday clinical practice.
2. Materials and Methods
Search of Evidences
This narrative review aims to update QoL aspects in the urological and andrological settings, focusing on attitudes towards the concept of QoL and its implementation in everyday clinical practice.
A search was performed in PubMed, Cochrane CENTRAL, and Scopus databases for relevant publications by using the following terms "quality of life" AND “urology" OR "andrology". Two authors (TC and PV) independently reviewed the selected articles. Any disagreements among reviewers were resolved through discussion and consensus. All references cited in relevant articles were also reviewed and analyzed. The filters used included the English language. Even if this search was planned as a narrative review, our search was performed in line with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) and the recommendations of the European Association of Urology guidelines (EAU) for conducting systematic reviews and meta-analyses [4,5]. Our research identified 2403 articles of potential interest. After the first screening round, 196 articles were considered eligible for inclusion in our narrative review. Most articles (185) were published during the last 20 years. Only 5 articles were published between 1990 and 1995.
3. Results
3.1. Evolution the Quality of Life Concept
In 1947, the World Health Organization (WHO) defined QoL as a “state of complete physical, mental, and social well-being, and not merely the absence of disease and infirmity” [6]. In 1995, the WHO definition evolved as follows: “Individuals’ perceptions of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns. It is a broad ranging concept incorporating in a complex way the persons’ physical health, psychological state, level of independence, social relationships, personal beliefs, and their relationships to salient features of the environment" [7].
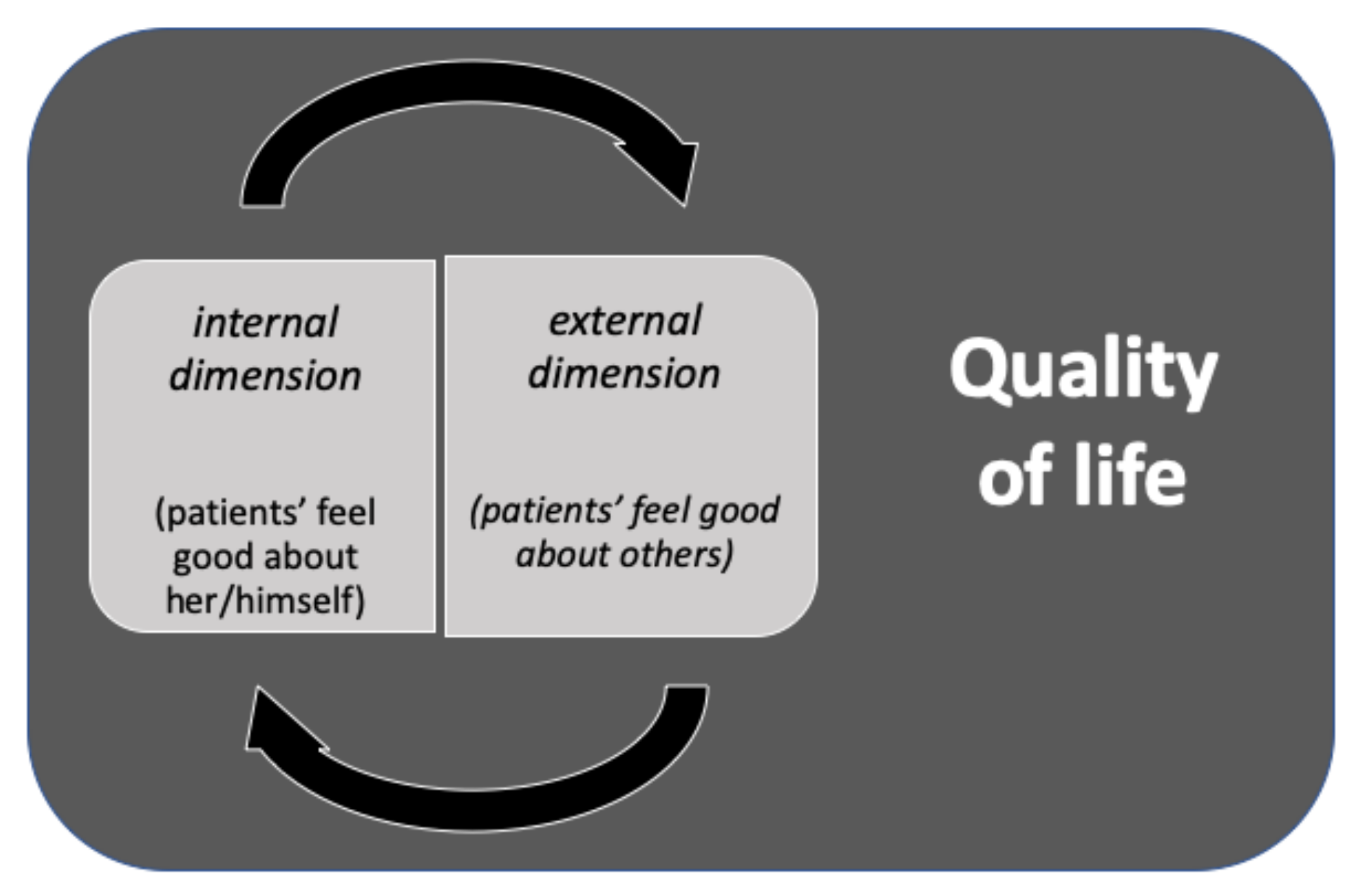
For long, this definition has been the most important and influential definition, but the concept of QoL has changed during recent years. Successively, the concept of health-related quality of life (HR-QoL) was introduced and defined as “how well a person functions in their life and his or her perceived wellbeing in physical, mental, and social domains of health” [5,6,8,9]. In other words, HR-QoL could be defined as: “Quality of life is an all-inclusive concept incorporating all factors that impact upon an individual’s life. Health-related quality of life includes only those factors that are part of an individual’s health” (Torrance [8]). Nowadays, the QoL concept includes other aspects related to a patient’s well-being. Many authors placed a greater emphasis on people’s subjective perceptions of the most important features of their lives, considering the QoL more of a personal perception and not only an objective and measurable entity. In this sense, Wenger et al. in 1984 defined QoL as “an individual’s perceptions of his or her functioning and well-being in different domains of life” [10]. This new definition of QoL takes into account what a patient thinks about his/her internal state, as well as their relationship with other people. QoL should be considered as a rich interplay and balance between how people see their internal state and how people see their relationships with other people (e.g., partner, friend, etc.). This new concept of QoL has important consequences for the management of patients affected by urological and andrological diseases. Any therapeutic approach should be considered in the light of this new and extended definition [11]. In this sense, the aim of treatment was not only to promote the absence of the disease or symptoms relief, but to improve patients’ QoL both in terms of his/her internal status and the relationship with other people [2,11]. The QoL then becomes a two-dimensional entity: an internal dimension (patients’ feel good about her/himself) and an external dimension (patients’ feel good about others) [2].
Figure 1 shows the interaction between internal and external dimensions when determining patients’ QoL.
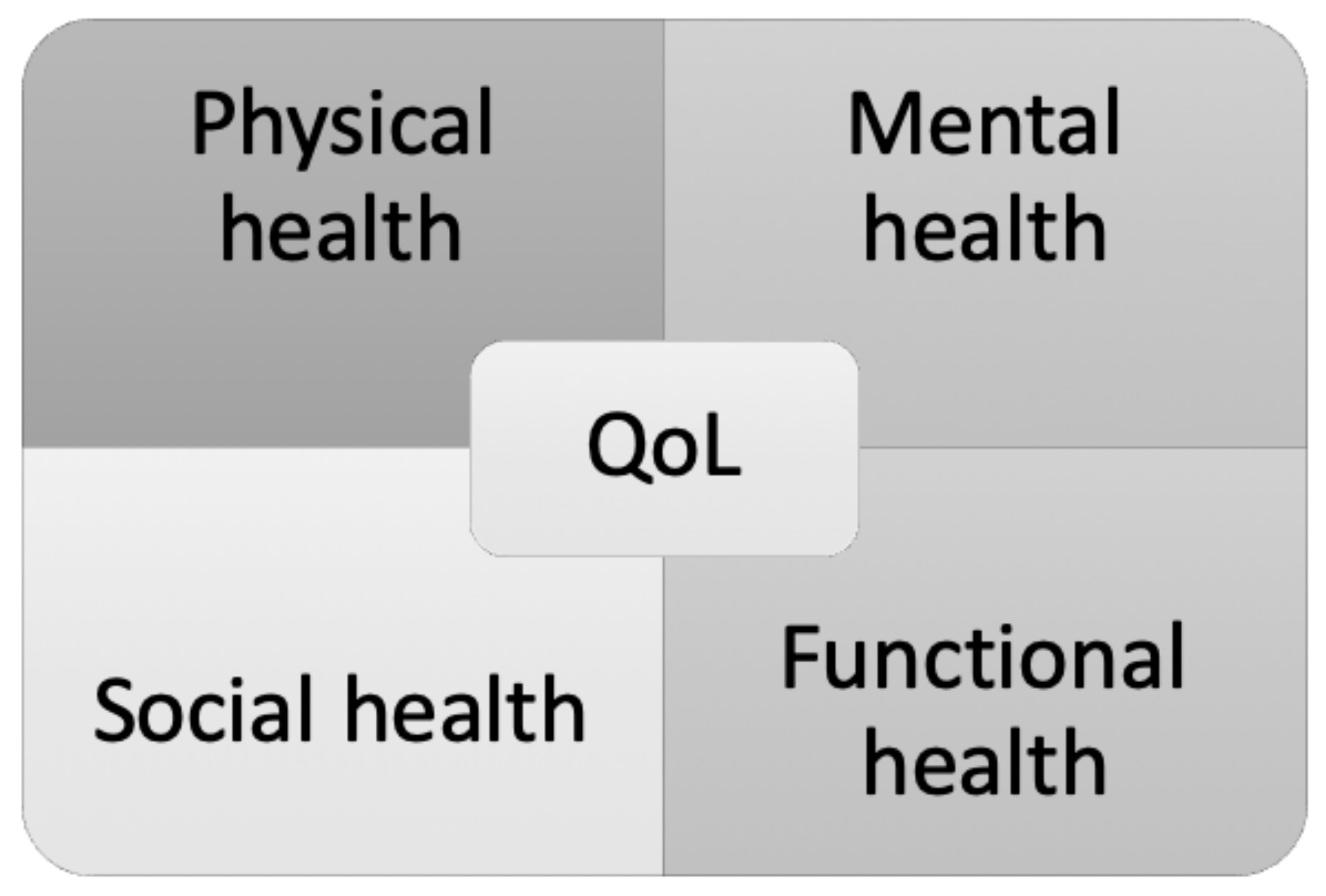
On the other hand, some authors described four broad health dimensions that summarize the specific QoL components (Figure 2) [2,12]:
- Physical health (somatic sensations, disease symptoms)
- Mental health (positive sense of well-being, nonpathological forms of psychological distress or diagnosable psychiatric disorders)
- Social health (aspects of social contacts and interactions)
- Functional health (self-care, mobility, physical activity level and social role functioning in relation to family and work).
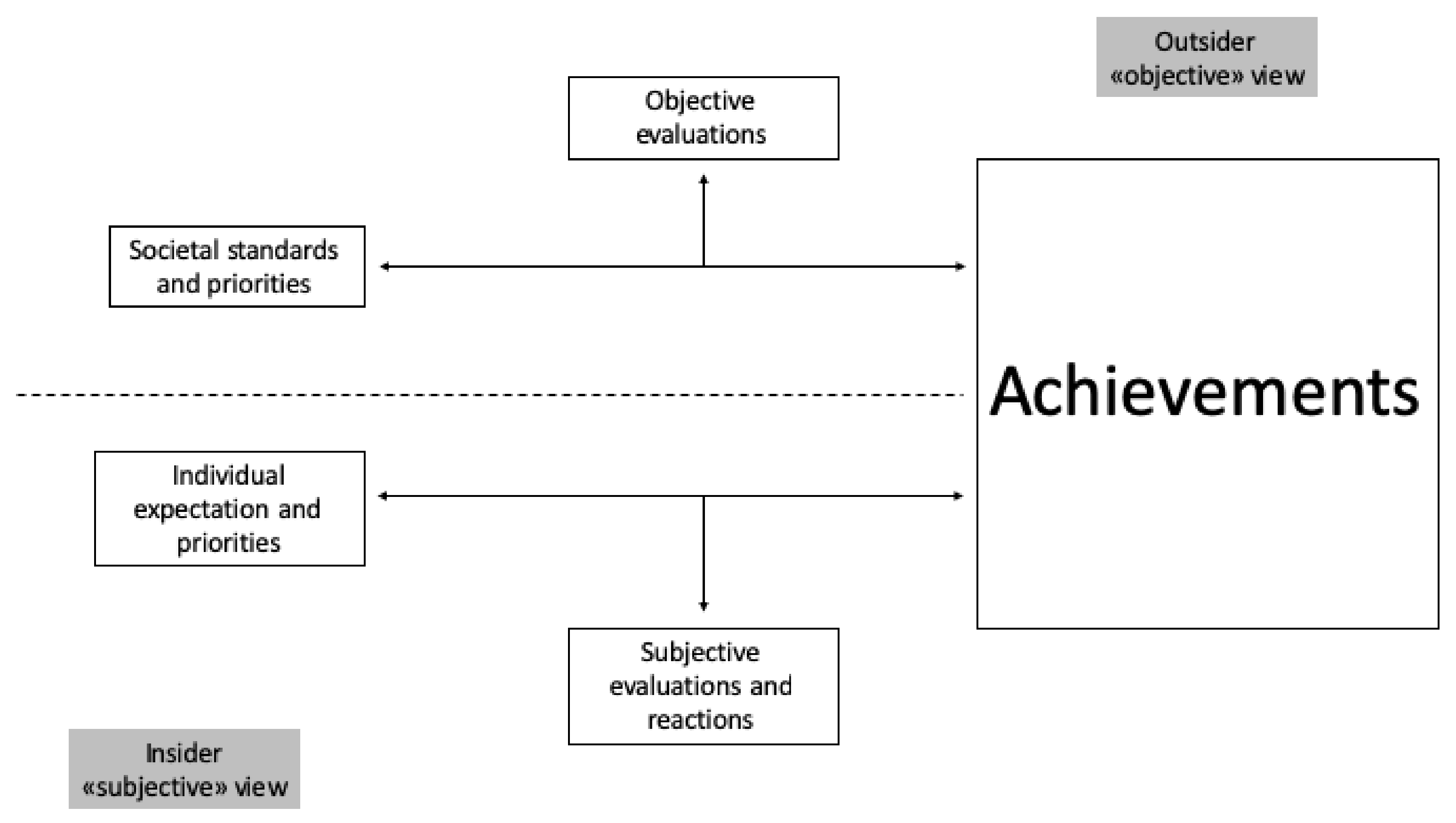
The Dijkers’s model is one of the most important examples of this concept because it summarizes all patient-related aspects that impact QoL [2,13].
Figure 3 shows a simplified representation of the Dijkers’s model.
We argue that the Dijkers’s model should also be adopted in the urological and andrological settings [13]. Indeed, uro-andrological diseases have a two-dimensional feature:
- The objective dimension (outsider)
- The subjective dimensions (insider)
In the objective dimension (outsider), we found that all observable life conditions were measurable and influenced by the relationship with other people (e.g., partners, friends) [14]. In this dimension, we found all physical functioning conditions. In the subjective dimension, we found all aspects referring to the patient’s perceptions, such as previous personal experience and perspectives.
This new concept of QoL perfectly describes patients’ expectations to any given treatment. Urological treatments are not only asked to resolve the clinical problem but improve or maintain patients’ QoL, where possible. For instance, the maintenance of urinary continence and erectile function are, together with cancer free-survival, the most important goals in the management of patients affected by prostate cancer [15]. Even if this concept seems easy to understand and consider in everyday clinical practice, the patient perspective is not always taken adequately into account [11]. This especially may occur in the management of non-oncological disease. Recently, Cai et al. demonstrated that, during management patients, affected by lower urinary tracts symptoms (LUTS), the sexual function, and sexual quality of life should be analyzed in depth because sometimes patients report LUTS instead of sexual symptoms because they feel embarrassed [16]. In this paper, Cai et al. demonstrated that an appropriate and useful therapeutic approach should be based on the patient’s perspectives and not only on the instrumental and laboratory findings. The extended definition of QoL has recently increased interest in everyday clinical practice and, for it, QoL is one of the most important endpoints included in the guidelines and recommendations of many medical societies.
3.2. The Quality of Life Concept and the Doctor–Patient Relationship
The recent evolution of the concept of QoL has positively changed the doctor–patient relationship. An increasing number of published papers demonstrates increasing interest in the concept of QoL. Over the last 5 years, about 50% of published articles on QoL (1032 out of 2403) were in the field of urology, thus demonstrating a particular interest of the scientific urological community. Schmick et al. reported, in a large survey among German urologists, that their attitude towards QoL was mainly positive, and most urologists considered QoL as a necessary part of their everyday clinical practice, even if urologists’ knowledge concerning QoL assessment, analysis, and interpretation was limited [17]. Moreover, they highlighted an important aspect that we discuss in the next section: the use of patient-reported outcome measures (PROMS) in QoL measurement [17]. Stewart considered QoL as a core element in the doctor–patient relationship [18]. She underlined that important aspects of the doctor–patient relationship are “the integration of these concepts of disease and illness with an understanding of the whole person in context, that is, an awareness of the multiple aspects of the patient’s life such as personality, developmental history, life cycle issues, the proximal context, such as family, and the distal context, such as community and physical environment” [18]. According to Stewart, the following components are essential in a patient-centered clinical approach:
- -
- Exploring both disease and the patients’ illness experience
- -
- Understanding the whole person
- -
- Finding common ground
- -
- Incorporating prevention and health promotion
- -
- Enhancing the patient-doctor relationship
- -
- Being realistic [18].
The concept of a patient-centered approach was recently introduced in urology with special focus on improving patients’ adherence to treatment and patients’ QoL. In 2018, De Nunzio demonstrated a dramatically low drug adherence and satisfaction with medical treatment among LUTS patients [19]. He highlighted the need for a patient-centered approach that aimed to improve drug adherence and other unmet needs in this area, such as adverse effects on sexual function management and the risk of disease progression [19]. No other substantial contributions in the urological or andrological field have been reported so far, even though a patient-centered approach is likely to benefit many patients in these fields. In particular, there is room for improvement in the andrological setting by increasing involvement of the patient’s sexual partner. The patient’s sexual partner adds an extra dimension to the patient-centered approach as part of the QoL concept in andrology.
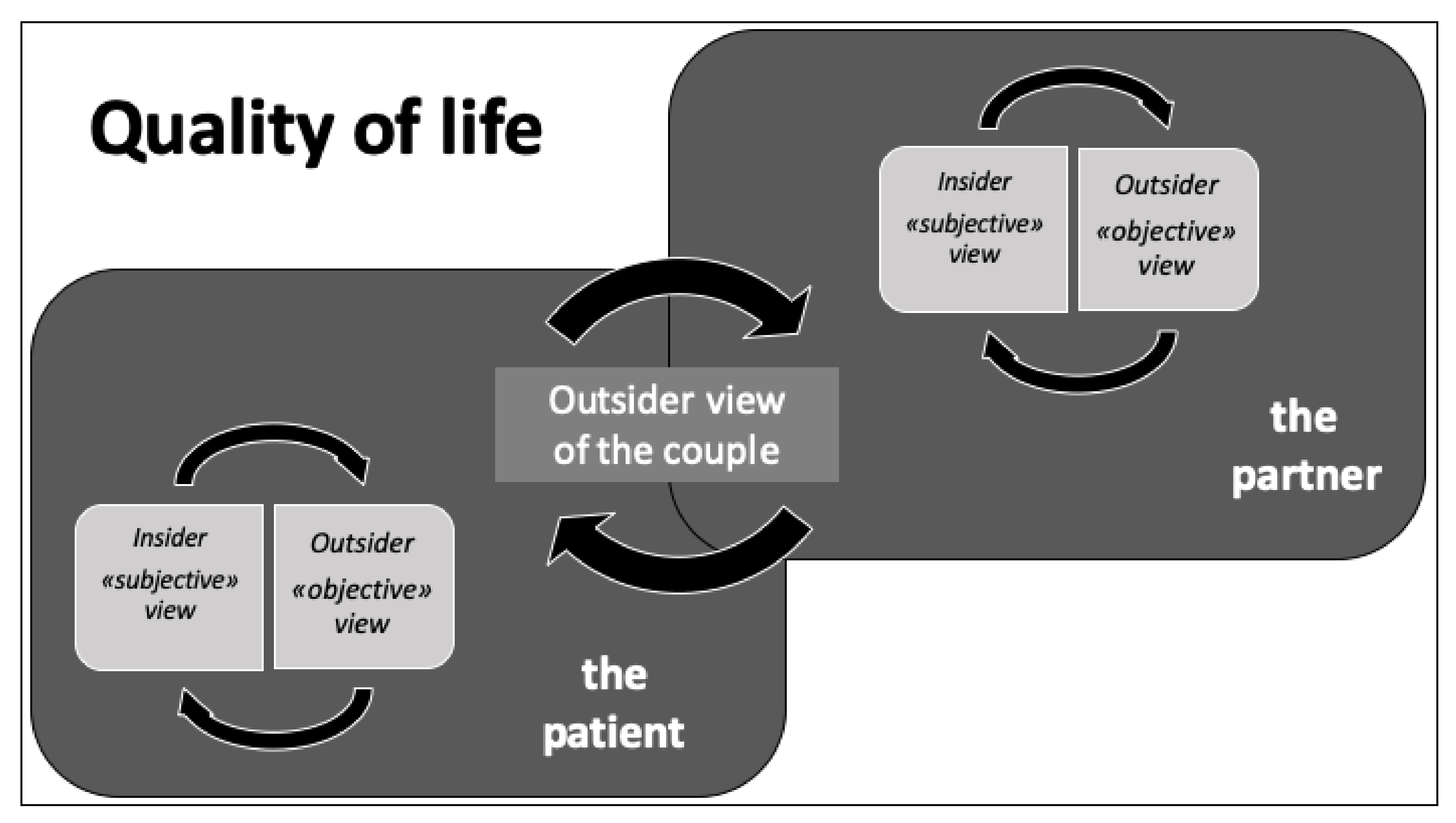
Figure 4 shows this new concept of andrological patient aspects influencing QoL: the interaction between “insider and outsider view of the patient” and “insider and outsider view of the partner”, as well as their interaction with the outsider view of the “couple”.
The partners’ sexual interest is important for a patient to recover the sexual function both in non-oncological and oncological diseases [20]. In a review article, Guercio et al. showed that mental health, physical health, quality of interpersonal communication, and patient-perceived partner support are the most important predictors of sexual satisfaction both for patients and partners in the post-prostatectomy period, demonstrating the need for further research on this topic [21].
On the other hand, cultural or religious schemata could limit the usefulness of treating patients as ’couples.’ In this sense, Asian, African, or Middle Eastern origin patients may withhold such information for cultural reasons, and lesbian, gay, bisexual, and transgender (LGBT) partners may not be so forthcoming in their disclosures for fear of stigmatization [22]. All urologists and andrologists are asked to pay particular attention to patients’ sexual orientation in order to improve adherence to the therapeutic approach. Future research in this area is needed.
3.3. Cross-Cultural and Religious Dimensions of QoL
The definition and assessment of QoL should be conducted considering various cross-cultural and religious dimensions. Several factors affecting the QoL definition are mainly determined by cultural or religious schemata, as is apparent in folk illnesses [23,24]. In urological and andrological setting, these aspects should be considered due to the fact that some diseases affect the sexual function or genitalia.
3.4. Quality of Life Assessment Tools
Due to the expansion of the concept of QoL and the raising interest for QoL in everyday clinical practice and research, there is a need for reproducible and accurate tools for its measurement. In the world of business management, there is a mantra that guides all decisions: What is not measured cannot be improved. In the last century, Lord Kelvin said that “What is not defined cannot be measured. What is not measured cannot be improved. What is not improved is always degraded” [25]. In healthcare, this principle is of crucial importance. Health professionals rely on empirical evidence to develop new treatments, optimize decision-making, save more lives. and improve patients’ quality of life [26]. Measuring a patient’s well-being after a treatment is fundamental to understand the effectiveness of that intervention [27]. QoL is not directly measurable and needs to be translated to indicators of its constituents and domains to be quantified [27]. General health perception, psychological well-being, and functioning are essential dimensions of QoL while symptoms and vitality are important causative variables [28]. Today, we have hundreds of QoL measures, many of which have been developed in recent years using generic measures that are applicable to most people, as well as specific tools for QoL measurement in people with specific clinical conditions [28]. Examples of QoL measures include the Beck Depression Inventory (BDI), the Sickness Impact Profile (SIP), and the 36-item Short Form Health Survey (SF-36) [28] (Table 1). These measures cover a wide range of aspects of life that can be adversely affected by ill health, such as physical functioning, emotional well-being, and ability to undertake work and social activities [29,30]. In a review article about the role of QoL in urological non-oncological and oncological diseases, Heldwein et al. underlined that QoL outcome measurements have become an important endpoint in urology, allowing urologists to better understand how each disease differs in different individuals [11]. Moreover, they reported that major urology society guidelines now recommend using self-report questionnaires for the most commonly used QoL measurement tools in clinical settings.
PROMs has become a valuable tool for use in everyday clinical practice as well as in research [11]. PROMs is a fundamental instrument to learn and understand the before and after condition of patients, and to put patients’ needs and preferences at the center of their care [31]. Several studies have used PROMs in a variety of generic measures of QoL to evaluate the efficacy of a treatment. PROMs is different than PRO (patient reported outcomes), which is a generic term that refers to the perspective of the patient themselves [31]. In an urological setting, the use of PROMs is common, especially when evaluating the outcome of oncological disease management. Several reviews have evaluated the scientific or psychometric properties of existing PRO questionnaires being used for patients diagnosed with prostate cancer [32]. However, even if there are many published studies that use PROMs to evaluate the QoL in prostate cancer patients, these instruments strongly focus on urinary, sexual, and bowel symptoms/function. All questionnaires include some items with a more subjective element to determine the extent to which men are concerned or bothered by a particular symptom [30]. However, no instrument includes the full range of items necessary to assess HRQL in terms of the subjective impact of physical, mental, and social aspects of prostate cancer [32].
In andrological and urological setting, no specific assessment tools for QoL of the patients’ sexual partner have been developed and validated. The Female Sexual Function Index (FSFI) was created only to assess female sexual function. A specific tool for assessing QoL of the sexual partner, independently from the partner sexual orientation, is urgently required [33].
4. Conclusions
The QoL concept now includes new aspects related to a patient’s well-being, particularly people’s subjective perceptions of the most important parts of their lives. QoL has become more of a personal perception and not only an objective and measurable entity. The aim of treatments is not only the absence of the disease or symptom relief but also to improve a patient’s QoL for his/her internal status and relationships with other people.
Any therapeutic approach should be based on patients’ perspectives rather than instrumental and laboratory findings. A patient’s sexual partner adds an extra dimension to the patient-centered approach as part of the QoL concept in andrology.
Measuring a patient’s well-being after treatment is fundamental to understanding the effectiveness of that intervention. QoL is not directly measurable and needs to be translated to indicators of its constituents and domains to be quantified.
Presently, among the many extant QoL measures, PROMs constitute a significant advance as a tool for use in the routine clinical management of individual patients and in clinical research.
Author Contributions
Conceptualization, T.C.; research, T.C. and P.V.; writing—original draft preparation, T.C.; writing—review and editing, T.E.B.J. All authors have read and agreed to the published version of the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021. [Google Scholar] [CrossRef]
- Post, M.W.M. Definitions of quality of life: What has happened and how to move on. Top. Spinal Cord Inj. Rehabil. 2014, 20, 167–180. [Google Scholar] [CrossRef]
- Elkinton, J.R. Medicine and quality of life. Ann. Intern. Med. 1966, 64, 711–714. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Köves, B.; Cai, T.; Veeratterapillay, R.; Pickard, R.; Seisen, T.; Lam, T.B.; Yuan, C.Y.; Bruyere, F.; Wagenlehner, F.; Bartoletti, R.; et al. Benefits and Harms of Treatment of Asymptomatic Bacteriuria: A Systematic Review and Meta-analysis by the European Association of Urology Urological Infection Guidelines Panel. Eur Urol. 2017, 72, 865–868. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The constitution of the World Health Organization. WHO Chron. 1947, 1, 29. [Google Scholar]
- Kaplan, R.M.; Bush, J.W. Health-related quality of life measurement for evaluation research and policy analysis. Health Psychol. 1982, 1, 61–80. [Google Scholar] [CrossRef]
- Hays, R.D.; Reeve, B.B. Measurement and Modeling of Health-Related Quality of Life. In Epidemiology and Demography in Public Health; Killewo, J., Heggenhougen, H.K., Quah, S.R., Eds.; Academic Press: San Diego, CA, USA, 2010; pp. 195–205. [Google Scholar]
- The WHOQOL Group. The World Health Organization Quality of Life assessment (WHOQOL): Position paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [Google Scholar] [CrossRef]
- Torrance, G.W. Utility approach to measuring health-related quality of life. J. Chronic Dis. 1987, 40, 593–600. [Google Scholar] [CrossRef]
- Karimi, M.; Brazier, J. Health, Health-Related Quality of Life, and Quality of Life: What is the Difference? Pharmacoeconomics 2016, 34, 645–649. [Google Scholar] [CrossRef]
- Wenger, N.K.; Mattson, M.E.; Furberg, C.D.; Elinson, J. Assessment of quality of life in clinical trials of cardiovascular therapies. Am. J. Cardiol. 1984, 54, 908–913. [Google Scholar] [CrossRef]
- Heldwein, F.L.; Sánchez-Salas, R.E.; Sánchez-Salas, R.; Teloken, P.E.; Teloken, C.; Castillo, O.; Vallancien, G. Health and quality of life in urology: Issues in general urology and urological oncology. Arch Esp Urol. 2009, 62, 519–530. [Google Scholar] [PubMed]
- Aaronson, N.K. Quantitative issues in health-related quality of life assessment. Health Policy 1988, 10, 217–230. [Google Scholar] [CrossRef]
- Dijkers, M.P.J.M. Quality of life of individuals with spinal cord injury: A review of conceptualization, measurement, and research findings. J. Rehabil. Res. Dev. 2005, 42, 87–110. [Google Scholar] [CrossRef] [PubMed]
- Wilson, I.B.; Cleary, P.D. Linking clinical variables with health-related quality of life: A conceptual model of patient outcomes. JAMA 1995, 273, 59–65. [Google Scholar] [CrossRef]
- Shevach, J.; Weiner, A.; Morgans, A.K. Quality of Life-Focused Decision-Making for Prostate Cancer. Curr. Urol. Rep. 2019, 20, 57. [Google Scholar] [CrossRef]
- Cai, T.; Morgia, G.; Carrieri, G.; Terrone, C.; Imbimbo, C.; Verze, P.; Mirone, V.; IDIProst® Gold Study Group. An improvement in sexual function is related to better quality of life, regardless of urinary function improvement: Results from the IDIProst® Gold Study. Arch. Ital. Urol. Androl. 2013, 85, 184–189. [Google Scholar] [CrossRef]
- Schmick, A.; Juergensen, M.; Rohde, V.; Katalinic, A.; Waldmann, A. Assessing health-related quality of life in urology—A survey of 4500 German urologists. BMC Urol. 2017, 17, 46. [Google Scholar] [CrossRef] [Green Version]
- Stewart, M. Reflections on the doctor–patient relationship: From evidence and experience. Br. J. Gen. Pract. 2005, 55, 793–801. [Google Scholar] [PubMed]
- De Nunzio, C.; Presicce, F.; Lombardo, R.; Trucchi, A.; Bellangino, M.; Tubaro, A.; Moja, E. Patient centered care for the medical treatment of lower urinary tract symptoms in patients with benign prostatic obstruction: A key point to improve patients’ care—A systematic review. BMC Urol. 2018, 18, 62. [Google Scholar] [CrossRef] [PubMed]
- Wittmann, D.; Carolan, M.; Given, B.; Skolarus, T.A.; An, L.; Palapattu, G.; Montie, J.E. Exploring the role of the partner in couples’ sexual recovery after surgery for prostate cancer. Support. Care Cancer 2014, 22, 2509–2515. [Google Scholar] [CrossRef]
- Guercio, C.; Mehta, A. Predictors of Patient and Partner Satisfaction Following Radical Prostatectomy. Sex. Med. Rev. 2018, 6, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Fredriksen-Goldsen, K.I.; Kim, H.J.; Shiu, C.; Goldsen, J.; Emlet, C.A. Successful Aging Among LGBT Older Adults: Physical and Mental Health-Related Quality of Life by Age Group. Gerontologist 2015, 55, 154–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guarnaccia, P.J. Anthropological perspectives. The importance of culture in the assessment of quality of life. In Quality of Life and Pharmaeconomics in Clinical Trials, 2nd ed.; Spilker, B., Ed.; Lippincott-Raven: Philadelphia, PA, USA, 1996; pp. 523–529. [Google Scholar]
- Saxena, S.; Carlson, D.; Billington, R.; Orley, J. The WHO quality of life assessment instrument (WHOQOL-Bref): The importance of its items for cross-cultural research. Qual. Life Res. 2001, 10, 711–721. [Google Scholar] [CrossRef] [PubMed]
- Diez-Cañamero, B.; Bishara, T.; Otegi-Olaso, J.R.; Minguez, R.; Fernández, J.M. Measurement of Corporate Social Responsibility: A Review of Corporate Sustainability Indexes, Rankings and Ratings. Sustainability 2020, 12, 2153. [Google Scholar] [CrossRef] [Green Version]
- Martin, L.R.; Williams, S.L.; Haskard, K.B.; DiMatteo, M.R. The challenge of patient adherence. Ther. Clin. Risk Manag. 2005, 1, 189–199. [Google Scholar]
- Kaplan, R.M.; Ries, A.L. Quality of Life: Concept and Definition. COPD J. Chronic Obstr. Pulm. Dis. 2007, 4, 263–271. [Google Scholar] [CrossRef]
- Lam, C.L.K. Subjective Quality of Life Measures—General Principles and Concepts. In Handbook of Disease Burdens and Quality of Life Measures; Preedy, V.R., Watson, R.R., Eds.; Springer: New York, NY, USA, 2010; pp. 381–399. [Google Scholar]
- Holmes, C.; Briffa, N. Patient-Reported Outcome Measures (PROMS) in patients undergoing heart valve surgery: Why should we measure them and which instruments should we use? Open Heart 2016, 3, e000315. [Google Scholar] [CrossRef] [Green Version]
- Protopapa, E.; van der Meulen, J.; Moore, C.M.; Smith, S.C. Patient-reported outcome (PRO) questionnaires for men who have radical surgery for prostate cancer: A conceptual review of existing instruments. BJU Int. 2017, 120, 468–481. [Google Scholar] [CrossRef]
- Rosen, R.; Brown, C.; Heiman, S.; Leiblum, C.; Ferguson, S.D.; D’Agostino, R. The Female Sexual Function Index (FSFI): A multidimensional self-report instrument for the assessment of female sexual function. J. Sex Martial Ther. 2000, 26, 191–208. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The interaction between internal and external dimensions when determining patients’ quality of life (QoL).
Figure 1.
The interaction between internal and external dimensions when determining patients’ quality of life (QoL).

Figure 2.
The four broad health dimensions that summarize the specific QoL components.

Figure 3.
A simplified representation of the Dijkers’s model.

Figure 4.
The new concept of andrological patient aspects influencing QoL: the interaction between “insider and outsider view of the patient” and “insider and outsider view of the partner”, as well as their interaction with the outsider view of the “couple”.
Figure 4.
The new concept of andrological patient aspects influencing QoL: the interaction between “insider and outsider view of the patient” and “insider and outsider view of the partner”, as well as their interaction with the outsider view of the “couple”.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
QoL assessment tools.
| Name | Items | Type | Area | Limitations |
|---|---|---|---|---|
| Beck Depression Inventory | 21 | Psychometric test | Depression | Influenced by physical symptom |
| Sickness Impact Profile | 136 | Psychometric test | General Health status | Accurate in chronic conditions |
| Short Form Health Survey | 36 | Psychometric test | General Health status | Accurate in chronic conditions |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Cai, T.; Verze, P.; Bjerklund Johansen, T.E. The Quality of Life Definition: Where Are We Going? Uro 2021, 1, 14-22. https://0-doi-org.brum.beds.ac.uk/10.3390/uro1010003
AMA Style
Cai T, Verze P, Bjerklund Johansen TE. The Quality of Life Definition: Where Are We Going? Uro. 2021; 1(1):14-22. https://0-doi-org.brum.beds.ac.uk/10.3390/uro1010003
Chicago/Turabian StyleCai, Tommaso, Paolo Verze, and Truls E. Bjerklund Johansen. 2021. "The Quality of Life Definition: Where Are We Going?" Uro 1, no. 1: 14-22. https://0-doi-org.brum.beds.ac.uk/10.3390/uro1010003