Sex-Gender Differences in Diabetic Retinopathy

 and
and
Abstract
:1. Introduction
2. Methods
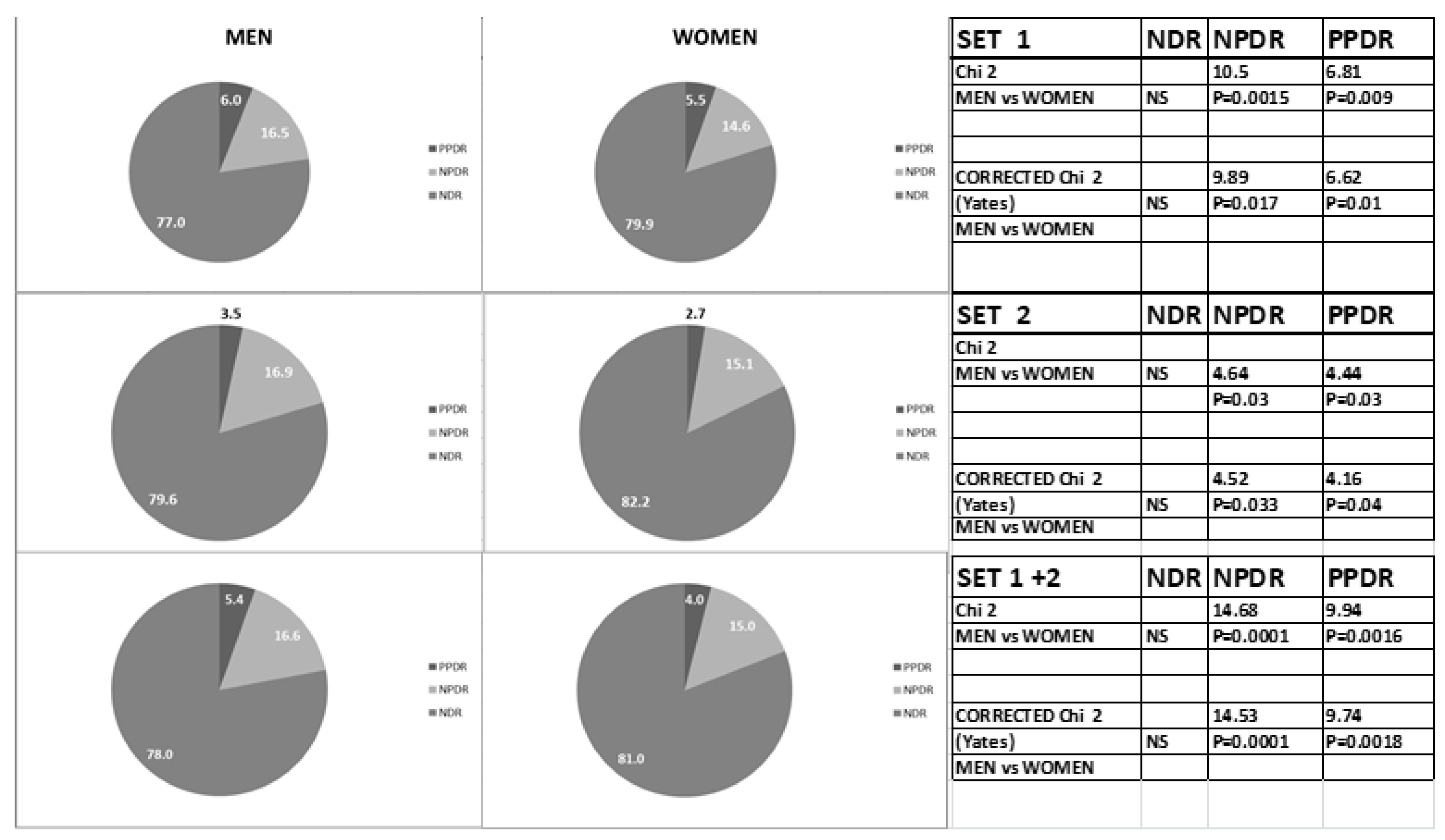
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zhang, X.; Saaddine, J.B.; Chou, C.F.; Cotch, M.F.; Cheng, Y.J.; Geiss, L.S.; Gregg, E.W.; Albright, A.L.; Klein, B.E.K.; Klein, R. Prevalence of diabetic retinopathy in the United States, 2005–2008. JAMA 2010, 304, 649–656. [Google Scholar] [CrossRef] [PubMed]
- Lachin, J.M.; White, N.H.; Hainsworth, D.P.; Sun, W.; Cleary, P.A.; Nathan, D.M. Effect of intensive diabetes therapy on the progression of diabetic retinopathy in patients with type 1 diabetes: 18 years of follow-up in the DCCT/EDIC. Diabetes 2015, 64, 631–642. [Google Scholar] [PubMed] [Green Version]
- Schanzlin, D.J.; Jay, W.H.; Fritz, K.J.; Tripathi, R.C.; Gonen, B. Hemoglobin A1 and diabetic retinopathy. Am. J. Ophthalmol. 1979, 88, 1032–1038. [Google Scholar] [CrossRef]
- Kaewput, W.; Thongprayoon, C.; Rangsin, R.; Ruangkanchanasetr, P.; Mao, M.A.; Cheungpasitporn, W. Associations of renal function with diabetic retinopathy and visual impairment in type 2 diabetes: A multicenter nationwide cross-sectional study. World J. Nephrol. 2019, 8, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Jenchitr, W.; Samaiporn, S.; Lertmeemongkolchai, P.; Chongwiriyanurak, T.; Anujaree, P.; Chayaboon, D.; Pohikamjorn, A. Prevalence of diabetic retinopathy in relation to duration of diabetes mellitus in community hospitals of Lampang. J. Med. Assoc. Thai 2004, 87, 1321–1326. [Google Scholar] [PubMed]
- Associazione Medici Diabetologi and Società Italiana di Diabetologia (Ed.) Standard Italiani per la Cura del Diabete Mellito AMD-SID; Associazione Medici Diabetologi and Società Italiana di Diabetologia: Rome, Italy, 2016; Available online: http://www.siditalia.it/pdf/Standard%20di%20Cura%20AMD%20-%20SID%202018_protetto.pdf (accessed on 27 April 2018).
- Campesi, I.; Franconi, F.; Seghieri, G.; Meloni, M. Sex-gender-related therapeutic approaches for cardiovascular complications associated with diabetes. Pharm. Res. 2017, 119, 195–207. [Google Scholar] [CrossRef]
- Franconi, F.; Campesi, I.; Occhioni, S.; Tonolo, G. Sex-gender differences in diabetes vascular complications and treatment. Endocr. Metab. Immune Disord. Drug Targets 2012, 12, 179–196. [Google Scholar] [CrossRef]
- Seghieri, G.; Policardo, L.; Anichini, R.; Franconi, F.; Campesi, I.; Cherchi, S.; Tonolo, G. aThe Effect of Sex and Gender on Diabetic Complications. Curr. Diabetes Rev. 2016, 13, 148–160. [Google Scholar] [CrossRef]
- Al-Rubeaan, K.; Abu El-Asrar, A.M.; Youssef, A.M.; Subhani, S.N.; Ahmad, N.A.; Al-Sharqawi, A.H.; Almutlaq, H.M.; David, S.K.; Alnaqeb, D. Diabetic retinopathy and its risk factors in a society with a type 2 diabetes epidemic: A Saudi National Diabetes Registry-based study. Acta Ophthalmol. 2015, 93, e140–e147. [Google Scholar] [CrossRef]
- Pradeepa, R.; Anitha, B.; Mohan, V.; Ganesan, A.; Rema, M. Risk factors for diabetic retinopathy in a South Indian Type 2 diabetic population--the Chennai Urban Rural Epidemiology Study (CURES) Eye Study 4. Diabet Med. 2008, 25, 536–542. [Google Scholar] [CrossRef]
- Rani, P.K.; Raman, R.; Chandrakantan, A.; Pal, S.S.; Perumal, G.M.; Sharma, T. Risk factors for diabetic retinopathy in self-reported rural population with diabetes. J. Postgrad. Med. 2009, 55, 92–96. [Google Scholar] [PubMed]
- Kashani, A.H.; Zimmer-Galler, I.E.; Shah, S.M.; Dustin, L.; Do, D.V.; Eliott, D.; Haller, J.A.; Nguyen, Q.D. Retinal thickness analysis by race, gender, and age using Stratus OCT. Am. J. Ophthalmol. 2010, 149, 496–502 e1. [Google Scholar] [CrossRef] [Green Version]
- Hammes, H.P.; Welp, R.; Kempe, H.P.; Wagner, C.; Siegel, E.; Holl, R.W. Risk Factors for Retinopathy and DME in Type 2 Diabetes-Results from the German/Austrian DPV Database. PLoS ONE 2015, 10, e0132492. [Google Scholar] [CrossRef] [PubMed]
- Constable, I.J.; Knuiman, M.W.; Welborn, T.A.; Cooper, R.L.; Stanton, K.M.; McCann, V.J.; Grose, G.C. Assessing the risk of diabetic retinopathy. Am. J. Ophthalmol. 1984, 97, 53–61. [Google Scholar] [CrossRef]
- West, K.M.; Ahuja, M.M.; Bennett, P.H.; Grab, B.; Grabauskas, V.; Mateo-de-Acosta, O.; Fuller, J.H.; Jarrett, R.J.; Keen, H.; Kosaka, K.; et al. Interrelationships of microangiopathy, plasma glucose and other risk factors in 3583 diabetic patients: A multinational study. Diabetologia 1982, 22, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, A.D.; Harris-Hayes, M.; Schootman, M. Epidemiology of diabetes and diabetes-related complications. Phys. Ther. 2008, 88, 1254–1264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kajiwara, A.; Miyagawa, H.; Saruwatari, J.; Kita, A.; Sakata, M.; Kawata, Y.; Oniki, K.; Yoshida, A.; Jinnouchi, H.; Nakagawa, K. Gender differences in the incidence and progression of diabetic retinopathy among Japanese patients with type 2 diabetes mellitus: A clinic-based retrospective longitudinal study. Diabetes Res. Clin. Pr. 2014, 103, e7–e10. [Google Scholar] [CrossRef] [PubMed]
- Pirart, J. Diabetes mellitus and its degenerative complications: A prospective study of 4,400 patients observed between 1947 and 1973 (author’s transl). Diabete Metab 1977, 3, 97–107. [Google Scholar]
- Jervell, J.; Moe, N.; Skjaeraasen, J.; Blystad, W.; Egge, K. Diabetes mellitus and pregnancy--management and results at Rikshospitalet, Oslo, 1970–1977. Diabetologia 1979, 16, 151–155. [Google Scholar] [CrossRef]
- Moloney, J.B.; Drury, M.I. The effect of pregnancy on the natural course of diabetic retinopathy. Am. J. Ophthalmol. 1982, 93, 745–756. [Google Scholar] [CrossRef]
- Solomon, S.D.; Chew, E.; Duh, E.J.; Sobrin, L.; Sun, J.K.; VanderBeek, B.L.; Wykoff, C.C.; Gardner, T.W. Diabetic retinopathy: A position statement by the American Diabetes Association. Diabetes Care 2017, 40, 412–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madendag, Y.; Acmaz, G.; Atas, M.; Sahin, E.; Tayyar, A.T.; Madendag, I.C.; Ozdemir, F.; Senol, V. The effect of oral contraceptive pills on the macula, the retinal nerve fiber layer, and choroidal thickness. Med. Sci. Monit. 2015, 23, 5657–5661. [Google Scholar] [CrossRef] [Green Version]
- Marino, M.; Masella, R.; Bulzomi, P.; Campesi, I.; Malorni, W.; Franconi, F. Nutrition and human health from a sex-gender perspective. Mol. Asp. Med. 2011, 32, 1–70. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.W.; van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Ellis, D.; Burgess, P.I.; Kayange, P. Management of diabetic retinopathy. Malawi Med. J. 2013, 25, 116–120. [Google Scholar]
- Hu, G. Gender difference in all-cause and cardiovascular mortality related to hyperglycaemia and newly-diagnosed diabetes. Diabetologia 2003, 46, 608–617. [Google Scholar] [CrossRef] [PubMed]
- Yau, J.W.; Rogers, S.L.; Kawasaki, R.; Lamoureux, E.L.; Kowalski, J.W.; Bek, T.; Chen, S.; Dekker, J.M.; Fletcher, A.E.; Grauslund, J.; et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care 2012, 35, 556–564. [Google Scholar] [CrossRef] [Green Version]
- Disoteo, O.; Grimaldi, F.; Papini, E.; Attanasio, R.; Tonutti, L.; Pellegrini, M.A.; Guglielmi, R.; Borretta, G. State-of-the-Art Review on Diabetes Care in Italy. Ann. Glob. Health 2015, 81, 803–813. [Google Scholar] [CrossRef]
- Segato, T.; Midena, E.; Grigoletto, F.; Zucchetto, M.; Fedele, D.; Piermarocchi, S.; Crepaldi, G. The epidemiology and prevalence of diabetic retinopathy in the Veneto region of north east Italy. Veneto Group for Diabetic Retinopathy. Diabetes Med. 1991, 8, S11–S16. [Google Scholar] [CrossRef]
- Porta, M.; Taulaigo, A.V. The changing role of the endocrinologist in the care of patients with diabetic retinopathy. Endocrine 2014, 46, 199–208. [Google Scholar] [CrossRef]
- Cruciani, F.; Abdolrahimzadeh, S.; Vicari, A.; Amore, F.M.; Di Pillo, S.; Mazzeo, L. Causes of blind certification in an Italian province and comparison with other European countries. Clin. Ter. 2010, 161, e11–e16. [Google Scholar]
- Mazhar, K.; Varma, R.; Choudhury, F.; McKean-Cowdin, R.; Shtir, C.J.; Azen, S.P. Severity of diabetic retinopathy and health-related quality of life: The Los Angeles Latino Eye Study. Ophthalmology 2011, 118, 649–655. [Google Scholar] [CrossRef] [Green Version]
- De Block, C.E.; De Leeuw, I.H.; Van Gaal, L.F. Impact of overweight on chronic microvascular complications in type 1 diabetic patients. Diabetes Care 2005, 28, 1649–1655. [Google Scholar] [CrossRef] [Green Version]
- Kostev, K.; Rathmann, W. Diabetic retinopathy at diagnosis of type 2 diabetes in the UK: A database analysis. Diabetologia 2013, 56, 109–111. [Google Scholar] [CrossRef]
- Hammes, H.P.; Kerner, W.; Hofer, S.; Kordonouri, O.; Raile, K.; Holl, R.W. Diabetic retinopathy in type 1 diabetes-a contemporary analysis of 8,784 patients. Diabetologia 2011, 54, 1977–1984. [Google Scholar] [CrossRef] [Green Version]
- Raman, R.; Rani, P.K.; Reddi Rachepalle, S.; Gnanamoorthy, P.; Uthra, S.; Kumaramanickavel, G.; Sharma, T. Prevalence of diabetic retinopathy in India: Sankara Nethralaya Diabetic Retinopathy Epidemiology and Molecular Genetics Study report 2. Ophthalmology 2009, 116, 311–318. [Google Scholar] [CrossRef]
- Stratton, I.M.; Kohner, E.M.; Aldington, S.J.; Turner, R.C.; Holman, R.R.; Manley, S.E.; Matthews, D.R. UKPDS 50: Risk factors for incidence and progression of retinopathy in Type II diabetes over 6 years from diagnosis. Diabetologia 2001, 44, 156–163. [Google Scholar] [CrossRef] [Green Version]
- Mehlsen, J.; Erlandsen, M.; Poulsen, P.L.; Bek, T. Identification of independent risk factors for the development of diabetic retinopathy requiring treatment. Acta Ophthalmol. 2011, 89, 515–521. [Google Scholar] [CrossRef]
- Kaiser, A.; Vollenweider, P.; Waeber, G.; Marques-Vidal, P. Prevalence, awareness and treatment of type 2 diabetes mellitus in Switzerland: The CoLaus study. Diabet. Med. 2012, 29, 190–197. [Google Scholar] [CrossRef]
- Maahs, D.M.; West, N.A.; Lawrence, J.M.; Mayer-Davis, E.J. Epidemiology of type 1 diabetes. Endocrinol. Metab. Clin. N. Am. 2010, 39, 481–497. [Google Scholar] [CrossRef] [Green Version]
- Awa, W.L.; Fach, E.; Krakow, D.; Welp, R.; Kunder, J.; Voll, A.; Zeyfang, A.; Wagner, C.; Schütt, M.; Boehm, B.; et al. Type 2 diabetes from pediatric to geriatric age: Analysis of gender and obesity among 120,183 patients from the German/Austrian DPV database. Eur. J. Endocrinol. 2012, 167, 245–254. [Google Scholar] [CrossRef]
- Cunningham-Myrie, C.; Younger-Coleman, N.; Tulloch-Reid, M.; McFarlane, S.; Francis, D.; Ferguson, T.; Gordonstrachan, G.; Wilks, R. Diabetes mellitus in Jamaica: Sex differences in burden, risk factors, awareness, treatment and control in a developing country. Trop. Med. Int. Health 2013, 18, 1365–1378. [Google Scholar] [CrossRef] [Green Version]
- Matthews, D.R.; Stratton, I.M.; Aldington, S.J.; Holman, R.R.; Kohner, E.M. Risks of progression of retinopathy and vision loss related to tight blood pressure control in type 2 diabetes mellitus: UKPDS 69. Arch. Ophthalmol. 2004, 122, 1631–1640. [Google Scholar]
- Errera, M.H.; Kohly, R.P.; da Cruz, L. Pregnancy-associated retinal diseases and their management. Surv. Ophthalmol. 2013, 58, 127–142. [Google Scholar] [CrossRef]
- Negrato, C.A.; Mattar, R.; Gomes, M.B. Adverse pregnancy outcomes in women with diabetes. Diabetol. Metab. Syndr. 2012, 4, 41. [Google Scholar] [CrossRef] [Green Version]
- Lauszus, F.; Klebe, J.G.; Bek, T. Diabetic retinopathy in pregnancy during tight metabolic control. Acta Obs. Gynecol. Scand. 2000, 79, 367–370. [Google Scholar] [CrossRef]
- Rossi, M.C.; Cristofaro, M.R.; Gentile, S.; Lucisano, G.; Manicardi, V.; Mulas, M.F.; Napoli, A.; Nicolucci, A.; Pellegrini, F.; Suraci, C.; et al. Sex disparities in the quality of diabetes care: Biological and cultural factors may play a different role for different outcomes: A cross-sectional observational study from the AMD Annals initiative. Diabetes Care 2013, 36, 3162–3168. [Google Scholar] [CrossRef] [Green Version]
- Policardo, L.; Seghieri, G.; Francesconi, P.; Anichini, R.; Franconi, F.; Seghieri, C.; del Prato, S. Gender difference in diabetes-associated risk of first-ever and recurrent ischemic stroke. J. Diabetes Complicat. 2015, 29, 713–717. [Google Scholar] [CrossRef]
- Barrett-Connor, E.; Ferrara, A. Isolated postchallenge hyperglycemia and the risk of fatal cardiovascular disease in older women and men. The Rancho Bernardo Study. Diabetes Care 1998, 21, 1236–1239. [Google Scholar] [CrossRef]
- Ozawa, G.Y.; Bearse, M.A., Jr.; Adams, A.J. Male-female differences in diabetic retinopathy? Curr. Eye Res. 2015, 40, 234–246. [Google Scholar] [CrossRef]
- Chaturvedi, N.; Porta, M.; Klein, R.; Orchard, T.; Fuller, J.; Parving, H.H.; Bilous, R.; Sjolie, A.K. Effect of candesartan on prevention (DIRECT-Prevent 1) and progression (DIRECT-Protect 1) of retinopathy in type 1 diabetes: Randomised, placebo-controlled trials. Lancet 2008, 372, 1394–1402. [Google Scholar] [CrossRef]
- Mauer, M.; Zinman, B.; Gardiner, R.; Suissa, S.; Sinaiko, A.; Strand, T.; Drummond, K.; Donnelly, S.; Goodyer, P.; Gubler, M.C.; et al. Renal and retinal effects of enalapril and losartan in type 1 diabetes. N. Engl. J. Med. 2009, 361, 40–51. [Google Scholar] [CrossRef] [PubMed]
- Sjolie, A.K.; Klein, R.; Porta, M.; Orchard, T.; Fuller, J.; Parving, H.H.; Bilous, R.; Chaturvedi, N. Effect of candesartan on progression and regression of retinopathy in type 2 diabetes (DIRECT-Protect 2): A randomised placebo-controlled trial. Lancet 2008, 372, 1385–1393. [Google Scholar] [CrossRef]
- Wang, B.; Wang, F.; Zhang, Y.; Zhao, S.H.; Zhao, W.J.; Yan, S.L.; Wang, Y. Effects of RAS inhibitors on diabetic retinopathy: A systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2015, 3, 263–274. [Google Scholar] [CrossRef]
- Nuzzi, R.; Scalabrin, S.; Becco, A.; Panzica, G. Gonadal Hormones and Retinal Disorders: A Review. Front. Endocrinol. 2018, 9, 66. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Number | SEX | HbA1c ≤ 7% | HbA1c > 7% | HbA1c > 8% | |
|---|---|---|---|---|---|
| NRD | 5936 | MEN | 51.9% | 48.1% | 14.0% |
| 4443 | WOMEN | 48.8% | 51.2% | 14.8% | |
| NPDR | 1269 | MEN | 42.0% | 58.0% * | 18.8% ** |
| 813 | WOMEN | 33.9% | 66.1% * | 25.2% ** | |
| PPDR | 499 | MEN | 27.9% | 72.1% | 29.1% |
| 307 | WOMEN | 25.4% | 74.6% | 29.4% |
| NDR | NPDR | PPDR | ||
|---|---|---|---|---|
| Age (years) | MEN | 68.1 ± 8.6 | 74.0 ± 10.2 ₸ | 73.1 ± 8.0 ₸ |
| WOMEN | 68.8 ± 9.0 | 75.3 ± 9.9 ₡ | 73.0 ± 8.1 ₡ | |
| DD (years) | MEN | 10.1 ± 5.4 | 17.0 ± 9.9 ₸. *** | 21 ± 10 ₸ |
| WOMEN | 10.4 ± 5.4 | 20.3 ± 10.7 ₡ | 22 ± 10 ₡ | |
| BMI (kg/m2) | MEN | 29.4 ± 3.7 | 29.0 ± 6 | 30.0 ± 5.2 |
| WOMEN | 29.8 ±4.7 | 31.1 ± 12 | 31.4 ± 6.8 | |
| HbA1c (%) | MEN | 6.8 ± 0.9 * | 7.3 ± 1.4 ₸. * | 7.8 ± 1.1 ₸. * |
| WOMEN | 7.0 ± 0.9 | 7.5 ± 1.3 ₡ | 8.3 ± 1.7 ₡ | |
| Total cholesterol (mg/dL) | MEN | 162 ± 27 *** | 163 ± 35 | 156 ± 38 |
| WOMEN | 174 ± 27 | 168 ± 39 | 160 ± 39 | |
| HDL (mg/dL) | MEN | 44 ± 9 *** | 45 ± 12 *** | 42 ± 9.9 ** |
| WOMEN | 51 ± 10 | 51 ± 16 | 49 ± 13 | |
| LDL (mg/dL) | MEN | 115 ± 62 | 96 ± 46 *** | 100 ± 50 |
| WOMEN | 114 ± 4 | 110 ± 66 | 118 ± 42 | |
| TG (mg/dL) | MEN | 105 ± 32 *** | 116 ± 31 | 90 ± 28 |
| WOMEN | 104 ± 31 | 116 ± 30 | 92 ± 38 | |
| Creatinine (µmol/L) | MEN | 88.0 ± 32.4 *** | 96.0 ± 46 *** | 103.5 ± 44.9 |
| WOMEN | 74.0 ± 31.0 | 82. 8 ± 44.1 ₵ | 91.8 ± 66.7 ₵ | |
| AER (mg/L) | MEN | 32 ± 108 *** | 56 ± 159 ₸. *** | 85 ± 178 ₸. * |
| WOMEN | 26 ± 94 | 16 ± 45 | 45 ± 112 | |
| eGFR (mL/min/m2) | MEN | 77 ± 29 | 67 ± 39 | 62 ± 38 ₸ |
| WOMEN | 71 ± 26 | 60 ± 35 | 54 ± 42 ₵ |
| NDR MEN = 2331 WOMEN = 1912 | NPDR MEN = 504 WOMEN = 344 | PPDR MEN = 168 WOMEN = 103 | ||||
|---|---|---|---|---|---|---|
| HT | CKF | HT | CKF | HT | CKF | |
| MEN % | 20.3 | 6.1 | 30.3 | 6.6 | 14.8 | 11 |
| WOMEN % | 27.3 | 4.7 | 33.7 | 8.9 | 20.1 | 22.5 |
| Chi2 | p = 0.0000 | p = 0.002 | ns | ns | ns | p = 0.0000 |
| Corrected Chi2 | p = 0.0000 | p = 0.002 | ns | ns | ns | p = 0.0000 |
| SEX | MEN | WOMEN |
|---|---|---|
| N (%) | 3003 (56) | 2359 (44) |
| DIABETES THERAPY (%) | ||
| DIET | 6.5 | 5.8 |
| DIET/OHA | 61.9 | 59.3 |
| OHA + I | 12.7 | 15.2 |
| I | 18.9 | 19.7 |
| OTHER DRUG THERAPY % | ||
| ANTI HYPERTENSIVE | 62 | 59 |
| ACEI/ARB USE | 51.8 | 52.2 |
| LIPID LOWERING | 48 | 48 |
| STATIN USE | 94.1 | 92.5 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cherchi, S.; Gigante, A.; Spanu, M.A.; Contini, P.; Meloni, G.; Fois, M.A.; Pistis, D.; Pilosu, R.M.; Lai, A.; Ruiu, S.; et al. Sex-Gender Differences in Diabetic Retinopathy. Diabetology 2020, 1, 1-10. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology1010001
Cherchi S, Gigante A, Spanu MA, Contini P, Meloni G, Fois MA, Pistis D, Pilosu RM, Lai A, Ruiu S, et al. Sex-Gender Differences in Diabetic Retinopathy. Diabetology. 2020; 1(1):1-10. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology1010001
Chicago/Turabian StyleCherchi, Sara, Alfonso Gigante, Maria Anna Spanu, Pierpaolo Contini, Gisella Meloni, Maria Antonietta Fois, Danila Pistis, Rosangela M. Pilosu, Alessio Lai, Salvatore Ruiu, and et al. 2020. "Sex-Gender Differences in Diabetic Retinopathy" Diabetology 1, no. 1: 1-10. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology1010001