Sexual Dysfunction in Diabetic Women: An Update on Current Knowledge

 , , , and
, , , and
Abstract
:1. Introduction
2. Physiology of the Female Sexual Response
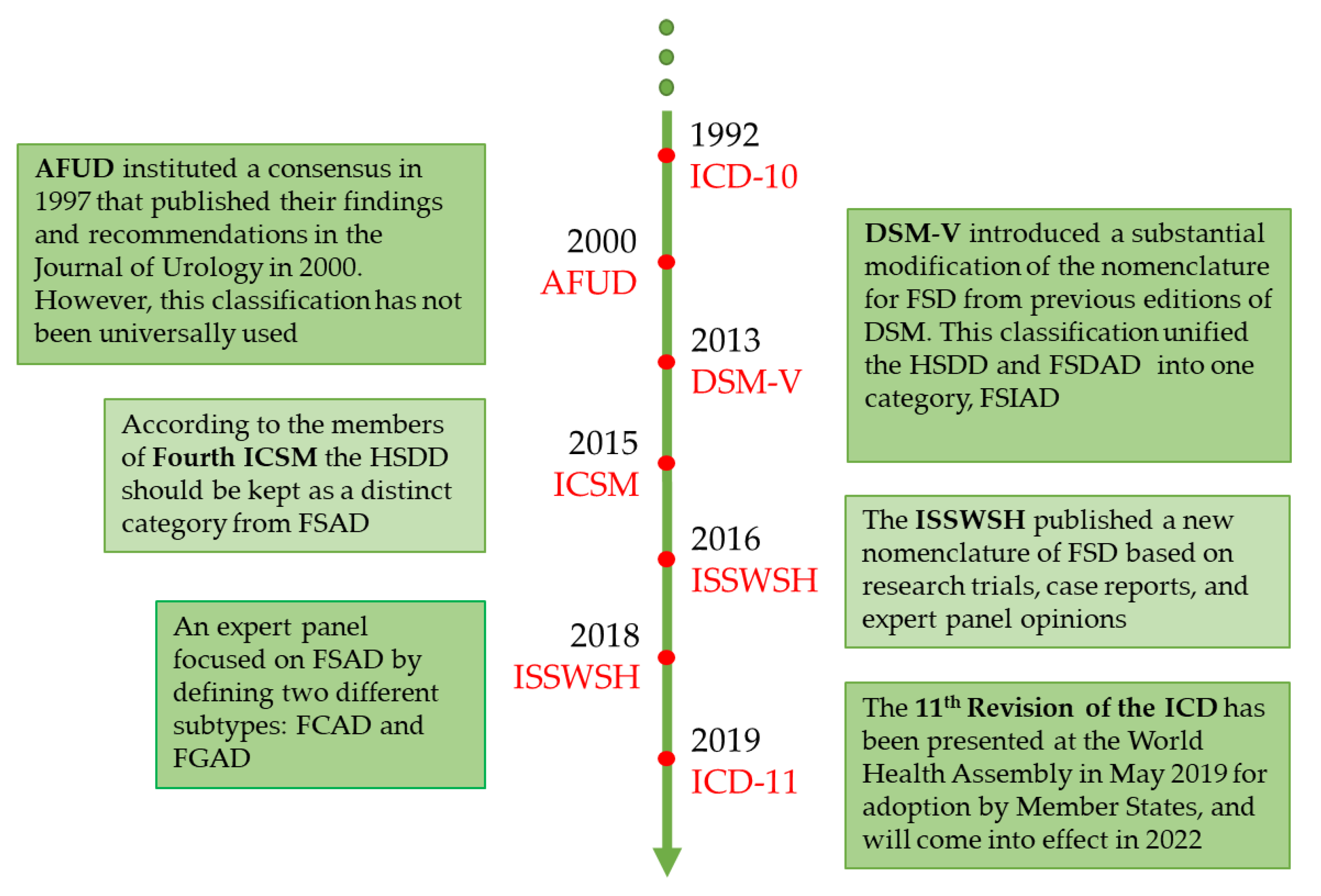
3. Female Sexual Dysfunction
4. Sexual Dysfunctions in Women with Diabetes Mellitus
4.1. Epidemiology
4.2. Pathogenesis
4.2.1. Psychological Factors
4.2.2. Organic Factors
4.3. Diagnosis
4.4. Treatment
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. IDF Diabetes Atlas Committee. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahmanian, E.; Salari, N.; Mohammadi, M.; Jalali, R. Evaluation of sexual dysfunction and female sexual dysfunction indicators in women with type 2 diabetes: A systematic review and meta-analysis. Diabetol. Metab. Syndr. 2019, 11, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laumann, E.O.; Paik, A.; Rosen, R.C. Sexual dysfunction in the United States: Prevalence and predictors. JAMA 1999, 281, 537–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gülmezoglu, A.M.; Souza, J.P.; Khanna, J.; Carroli, G.; Hofmeyr, G.J.; Wolomby-Molombo, J.J.; Mittal, S.; Lumbiganon, P.; Cheng, L. The WHO Reproductive Health Library: A Cochrane window on sexual and reproductive health. Cochrane Database Syst. Rev. 2013, 10, ED000070. [Google Scholar] [CrossRef]
- Masters, E.H.; Johnson, V.E. Human Sexual Response; Little Brown & Co.: Boston, MA, USA, 1966. [Google Scholar]
- Kaplan, H.S. The New Sex Therapy; Bailliere Tindall: London, UK, 1974. [Google Scholar]
- Basson, R. Women’s sexual dysfunction: Revised and expanded definitions. CMAJ 2005, 172, 1327–1333. [Google Scholar] [CrossRef] [Green Version]
- Berman, J.R. Physiology of female sexual function and dysfunction. Int. J. Impot. Res. 2005, 17 (Suppl. 1), S44–S51. [Google Scholar] [CrossRef] [Green Version]
- D’Amati, G.; di Gioia, C.R.; Bologna, M.; Giordano, D.; Giorgi, M.; Dolci, S.; Jannini, E.A. Type 5 phosphodiesterase expression in the human vagina. Urology 2002, 60, 191–195. [Google Scholar] [CrossRef]
- Corona, G.; Isidori, A.M.; Aversa, A.; Bonomi, M.; Ferlin, A.; Foresta, C.; La Vignera, S.; Maggi, M.; Pivonello, R.; Vignozzi, L.; et al. Male and female sexual dysfunction in diabetic subjects: Focus on new antihyperglycemic drugs. Rev. Endocr. Metab. Disord. 2020, 21, 57–65. [Google Scholar] [CrossRef]
- Shifren, J.L.; Monz, B.U.; Russo, P.A.; Segreti, A.; Johannes, C.B. Sexual problems and distress in United States women: Prevalence and correlates. Obstet Gynecol. 2008, 112, 970–978. [Google Scholar] [CrossRef] [Green Version]
- Dennerstein, L.; Koochaki, P.; Barton, I.; Graziottin, A. Hypoactive sexual desire disorder in menopausal women: A survey of Western European women. J. Sex. Med. 2006, 3, 212–222. [Google Scholar] [CrossRef]
- Parish, S.J.; Meston, C.M.; Althof, S.E.; Clayton, A.H.; Goldstein, I.; Goldstein, S.W.; Heiman, J.R.; McCabe, M.P.; Segraves, R.T.; Simon, J.A. Toward a more evidence-based nosology and nomenclature for female sexual dysfunctions-part III. J. Sex. Med. 2019, 16, 452–462. [Google Scholar] [CrossRef] [PubMed]
- Parish, S.J.; Hahn, S.R.; Goldstein, S.W.; Giraldi, A.; Kingsberg, S.A.; Larkin, L.; Minkin, M.J.; Brown, V.; Christiansen, K.; Hartzell-Cushanick, R.; et al. The international society for the study of women’s sexual health process of care for the identification of sexual concerns and problems in women. Mayo Clin. Proc. 2019, 94, 842–856. [Google Scholar] [CrossRef] [PubMed]
- Reed, G.M.; Drescher, J.; Krueger, R.B.; Atalla, E.; Cochran, S.D.; First, M.B.; Cohen-Kettenis, P.T.; Arango-de Montis, I.; Parish, S.J.; Cottler, S.; et al. Disorders related to sexuality and gender identity in the ICD-11: Revising the ICD-10 classification based on current scientific evidence, best clinical practices, and human rights considerations. World Psychiatry 2016, 15, 205–221. [Google Scholar] [CrossRef] [Green Version]
- Parish, S.J.; Goldstein, A.T.; Goldstein, S.W.; Goldstein, I.; Pfaus, J.; Clayton, A.H.; Giraldi, A.; Simon, J.A.; Althof, S.E.; Bachmann, G.; et al. Toward a more evidence-based nosology and nomenclature for female sexual dysfunctions: Part II. J. Sex. Med. 2016, 13, 1888–1906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zamponi, V.; Mazzilli, R.; Bitterman, O.; Olana, S.; Iorio, C.; Festa, C.; Giuliani, C.; Mazzilli, F.; Napoli, A. Association between type 1 diabetes and female sexual dysfunction. BMC Womens Health 2020, 20, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cortelazzi, D.; Marconi, A.; Guazzi, M.; Cristina, M.; Zecchini, B.; Veronelli, A.; Cattalini, C.; Innocenti, A.; Bosco, G.; Pontiroli, A.E. Sexual dysfunction in pre-menopausal diabetic women: Clinical, metabolic, psychological, cardiovascular, and neurophysiologic correlates. Acta Diabetol. 2013, 50, 911–917. [Google Scholar] [CrossRef]
- Pontiroli, A.E.; Cortelazzi, D.; Morabito, A. Female sexual dysfunction and diabetes: A systematic review and meta-analysis. J. Sex. Med. 2013, 10, 1044–1051. [Google Scholar] [CrossRef]
- Meeking, D.R.; Fosbury, J.A.; Cummings, M.H. Sexual dysfunction and sexual health concerns in women with diabetes. Pract. Diabetes 2013, 30, 327–331. [Google Scholar] [CrossRef]
- Enzlin, P.; Mathieu, C.; Van Den Bruel, A.; Vanderschueren, D.; Demyttenaere, K. Prevalence and predictors of sexual dysfunction in patients with type 1 diabetes. Diabetes Care 2003, 26, 409–414. [Google Scholar] [CrossRef] [Green Version]
- Esposito, K.; Maiorino, M.I.; Bellastella, G.; Giugliano, F.; Romano, M.; Giugliano, D. Determinants of female sexual dysfunction in type 2 diabetes. Int. J. Impot. Res. 2010, 179–184. [Google Scholar] [CrossRef] [Green Version]
- Schram, M.T.; Baan, C.A.; Pouwer, F. Depression and quality of life in patients with diabetes: A systematic review from the European depression in diabetes (EDID) research consortium. Curr. Diabetes Rev. 2009, 5, 112–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, S.H.; Rizvi, S. Sexual dysfunction, depression, and the impact of antidepressants. J. Clin. Psychopharmacol. 2009, 29, 157–164. [Google Scholar] [CrossRef] [PubMed]
- La Torre, A.; Giupponi, G.; Duffy, D.; Conca, A. Sexual dysfunction related to psychotropic drugs: A critical review—Part I: Antidepressants. Pharmacopsychiatry 2013, 46, 191–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Torre, A.; Conca, A.; Duffy, D.; Giupponi, G.; Pompili, M.; Grözinger, M. Sexual dysfunction related to psychotropic drugs: A critical review part II: Antipsychotics. Pharmacopsychiatry 2013, 46, 201–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Torre, A.; Giupponi, G.; Duffy, D.M.; Pompili, M.; Grözinger, M.; Kapfhammer, H.P.; Conca, A. Sexual dysfunction related to psychotropic drugs: A critical review. Part III: Mood stabilizers and anxiolytic drugs. Pharmacopsychiatry 2014, 47, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nyirjesy, P.; Sobel, J.D. Genital mycotic infections in patients with diabetes. Postgrad. Med. 2013, 125, 33–46. [Google Scholar] [CrossRef]
- Rantell, A.; Apostolidis, A.; Anding, R.; Kirschner-Hermanns, R.; Cardozo, L. How does lower urinary tract dysfunction affect sexual function in men and women? ICI-RS 2015-Part 1. Neurourol. Urodyn. 2017, 36, 949–952. [Google Scholar] [CrossRef]
- Maiorino, M.I.; Bellastella, G.; Esposito, K. Diabetes and sexual dysfunction: Current perspectives. Diabetes Metab. Syndr. Obes. 2014, 7, 95–105. [Google Scholar] [CrossRef] [Green Version]
- Park, K.; Ryu, S.B.; Park, Y.I.; Ahn, K.; Lee, S.N.; Nam, J.H. Diabetes mellitus induces vaginal tissue fibrosis by TGF-beta 1 expression in the rat model. J. Sex Marital Ther. 2001, 27, 577–587. [Google Scholar] [CrossRef]
- Park, K.; Ahn, K.; Chang, J.S.; Lee, S.E.; Ryu, S.B.; Park, Y.I. Diabetes induced alteration of clitoral hemodynamics and structure in the rabbit. J. Urol. 2002, 168, 1269–1272. [Google Scholar] [CrossRef]
- Kim, N.N.; Stankovic, M.; Cushman, T.T.; Goldstein, I.; Munarriz, R.; Traish, A.M. Streptozotocin-induced diabetes in the rat is associated with changes in vaginal hemodynamics, morphology and biochemical markers. BMC Physiol. 2006, 6, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wincze, J.P.; Albert, A.; Bansal, S. Sexual arousal in diabetic females: Physiological and self-report measures. Arch. Sex. Behav. 1993, 22, 587–601. [Google Scholar] [CrossRef] [PubMed]
- Maseroli, E.; Fanni, E.; Cipriani, S.; Scavello, I.; Pampaloni, F.; Battaglia, C.; Fambrini, M.; Mannucci, E.; Jannini, E.A.; Maggi, M.; et al. Cardiometabolic risk and female sexuality: Focus on clitoral vascular resistance. J. Sex. Med. 2016, 13, 1651–1661. [Google Scholar] [CrossRef]
- Vicari, E.; Di Pino, L.; La Vignera, S.; Fratantonio, E.; Signorelli, S.; Battiato, C.; Calogero, A.E. Peak systolic velocity in patients with arterial erectile dysfunction and peripheral arterial disease. Int. J. Impot. Res. 2006, 18, 175–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maseroli, E.; Scavello, I.; Vignozzi, L. Cardiometabolic risk and female sexuality-part ii. understanding (and overcoming) gender differences: The key role of an adequate methodological approach. Sex. Med. Rev. 2018, 6, 525–534. [Google Scholar] [CrossRef]
- Duby, J.J.; Campbell, R.K.; Setter, S.M.; White, J.R.; Rasmussen, K.A. Diabetic neuropathy: An intensive review. Am. J. Health Syst. Pharm. 2004, 61, 160–173; quiz 175–176. [Google Scholar] [CrossRef]
- Kalra, B.; Kalra, S.; Bajaj, S. Vulvodynia: An unrecognized diabetic neuropathic syndrome. Indian J. Endocrinol. Metab. 2013, 17, 787–789. [Google Scholar] [CrossRef]
- Semmens, J.P.; Wagner, G. Estrogen deprivation and vaginal function in postmenopausal women. JAMA 1982, 248, 445–448. [Google Scholar] [CrossRef]
- Garzo, V.G.; Dorrington, J.H. Aromatase activity in human granulosa cells during follicular development and the modulation by follicle-stimulating hormone and insulin. Am. J. Obstet. Gynecol. 1984, 148, 657–662. [Google Scholar] [CrossRef]
- Nestler, J.E.; Strauss, J.F. Insulin as an effector of human ovarian and adrenal steroid metabolism. Endocrinol. Metab. Clin. N. Am. 1991, 20, 807–823. [Google Scholar] [CrossRef]
- Ozawa, S.; Iguchi, T.; Takemura, K.K.; Bern, H.A. Effect of certain growth factors on proliferation in serum-free collagen gel culture of vaginal epithelial cells from prepuberal mice exposed neonatally to diethylstilbestrol. Proc. Soc. Exp. Biol. Med. 1991, 198, 760–763. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, A.; Urushitani, H.; Watanabe, H.; Sato, T.; Iguchi, T.; Kobayashi, T.; Ohta, Y. Comparison of estrogen responsive genes in the mouse uterus, vagina and mammary gland. J. Vet. Med. Sci. 2007, 69, 725–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhasin, S.; Enzlin, P.; Coviello, A.; Basson, R. Sexual dysfunction in men and women with endocrine disorders. Lancet 2007, 369, 597–611. [Google Scholar] [CrossRef]
- Reddy, M.; Godsland, I.F.; Barnard, K.D.; Herrero, P.; Georgiou, P.; Thomson, H.; Johnston, D.G.; Oliver, N.S. Glycemic variability and its impact on quality of life in adults with type 1 diabetes. J. Diabetes Sci. Technol. 2015, 10, 60–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosen, R.; Brown, C.; Heiman, J.; Leiblum, S.; Meston, C.; Shabsigh, R.; Ferguson, D.; D’Agostino, R. The Female Sexual Function Index (FSFI): A multidimensional self-report instrument for the assessment of female sexual function. J. Sex Marital Ther. 2000, 26, 191–208. [Google Scholar] [CrossRef] [PubMed]
- Isidori, A.M.; Pozza, C.; Esposito, K.; Giugliano, D.; Morano, S.; Vignozzi, L.; Corona, G.; Lenzi, A.; Jannini, E.A. Development and validation of a 6-item version of the female sexual function index (FSFI) as a diagnostic tool for female sexual dysfunction. J. Sex. Med. 2010, 7, 1139–1146. [Google Scholar] [CrossRef]
- Maseroli, E.; Fanni, E.; Fambrini, M.; Ragghianti, B.; Limoncin, E.; Mannucci, E.; Maggi, M.; Vignozzi, L. Bringing the body of the iceberg to the surface: The female sexual dysfunction index-6 (fsdi-6) in the screening of female sexual dysfunction. J. Endocrinol. Investig. 2016, 39, 401–409. [Google Scholar] [CrossRef]
- Mollaioli, D.; Di Sante, S.; Limoncin, E.; Ciocca, G.; Luca, G.; Maseroli, E.; Fanni, E.; Vignozzi, L.; Maggi, M.; Lenzi, A.; et al. Validation of a visual analogue scale to measure the subjective perception of orgasmic intensity in females: The orgasmometer-F. PLoS ONE 2018, 13, e0202076. [Google Scholar] [CrossRef] [Green Version]
- Caruso, S.; Rugolo, S.; Mirabella, D.; Intelisano, G.; Di Mari, L.; Cianci. Changes in clitoral blood flow in premenopausal women affected by type 1 diabetes after single 100-mg administration of sildenafil. Urology 2006, 68, 161–165. [Google Scholar] [CrossRef]
- Woodard, T.L.; Diamond, M.P. Physiologic measures of sexual function in women: A review. Fertil. Steril. 2009, 92, 19–34. [Google Scholar] [CrossRef] [Green Version]
- Bond, D.S.; Wing, R.R.; Vithiananthan, S.; Sax, H.C.; Roye, G.D.; Ryder, B.A.; Pohl, D.; Giovanni, J. Significant resolution of female sexual dysfunction after bariatric surgery comparative study. Surg. Obes. Relat. Dis. 2011, 7, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giugliano, F.; Maiorino, M.I.; Di Palo, C.; Autorino, R.; De Sio, M.; Giugliano, D.; Esposito, K. Adherence to mediterranean diet and sexual function in women with type 2 diabetes. J. Sex. Med. 2010, 7, 1883–1890. [Google Scholar] [CrossRef] [PubMed]
- Wing, R.R.; Bond, D.S.; Gendrano, I.N.; Wadden, T.; Bahnson, J.; Lewis, C.E.; Brancati, F.; Schneider, S.; Kitabchi, A.E.; Van Dorsten, B.; et al. Effect of intensive lifestyle intervention on sexual dysfunction in women with type 2 diabetes: Results from an ancillary look AHEAD study randomized controlled trial diabetes care. Diabetes Care 2013, 36, 2937–2944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Islam, R.M.; Bell, R.J.; Green, S.; Page, M.J.; Davis, S.R. Safety and efficacy of testosterone for women: A systematic review and meta-analysis of randomised controlled trial data. Lancet Diabetes Endocrinol. 2019, 7, 754–766. [Google Scholar] [CrossRef]
- Davis, S.R.; Baber, R.; Panay, N.; Bitzer, J.; Cerdas Perez, S.; Islam, R.M.; Kaunitz, A.M.; Kingsberg, S.A.; Lambrinoudaki, I.; Liu, J.; et al. Global consensus position statement on the use of testosterone therapy for women. Climacteric. 2019, 22, 429–434. [Google Scholar] [CrossRef] [Green Version]
- Rowen, T.S.; Davis, S.R.; Parish, S.; Simon, J.; Vignozzi, L. Methodological Challenges in Studying Testosterone Therapies for Hypoactive Sexual Desire Disorder in Women. J. Sex. Med. 2020, 17, 585–594. [Google Scholar] [CrossRef]
- Chivers, M.L.; Rosen, R.C. Phosphodiesterase type 5 inhibitors and female sexual response: Faulty protocols or paradigms? J. Sex. Med. 2010, 7, 858–872. [Google Scholar] [CrossRef]
- Portman, D.; Palacios, S.; Nappi, R.E.; Mueck, A.O. Ospemifene, a non-oestrogen selective oestrogen receptor modulator for the treatment of vaginal dryness associated with postmenopausal vulvar and vaginal atrophy: A randomised, placebo-controlled, phase III trial. Maturitas 2014, 78, 91–98. [Google Scholar] [CrossRef]
- Katz, M.; DeRogatis, L.R.; Ackerman, R.; Hedges, P.; Lesko, L.; Garcia, M., Jr.; Sand, M. BEGONIA trial investigators. Efficacy of flibanserin in women with hypoactive sexual desire disorder: Results from the BEGONIA trial. J. Sex. Med. 2013, 10, 1807–1815. [Google Scholar] [CrossRef]


{kind=link}
| ICD | DSM | ICSM | ISSWSH | ||
|---|---|---|---|---|---|
| ICD-10 | ICD-11 (Proposed) | DSM-V | Fourth ICSM | ISSWSH-2016 | ISSWSH-2018 |
| 1. Lack or loss of sexual desire | Hypoactive sexual desire dysfunction | 1. Female sexual interest/arousal disorder | 1. Hypoactive sexual desire dysfunction | 1.Hypoactive sexual desire disorder | 1.Hypoactive sexual desire disorder |
| 2. Sexual aversion | Recommended for deletion | 2. Female orgasmic disorder | 2. Female sexual arousal dysfunction | 2. Female genital arousal disorder | 2. Female sexual arousal disorder: -Female cognitive arousal disorder -Female genital arousal disorder |
| 3. Lack of sexual enjoyment | Female sexual arousal dysfunction | 3. Genito-pelvic/penetration disorder | 3. Female orgasmic dysfunction | 3. Persistent genital arousal disorder | 3. Persistent genital arousal disorder |
| 4.Failure of sexual response | 4. Female genital-pelvic pain dysfunction | 4. Female orgasm disorders | 4. Female orgasm disorders | ||
| 5. Orgasmic dysfunction | Orgasmic dysfunction | 5. Persistent genital arousal disorder | 5. Female orgasmic illness syndrome | 5. Female orgasmic illness syndrome | |
| 6. Non organic vaginismus | Sexual pain penetration disorder | 6. Postcoital syndrome (Postorgasmic illness syndrome) | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barbagallo, F.; Mongioì, L.M.; Cannarella, R.; La Vignera, S.; Condorelli, R.A.; Calogero, A.E. Sexual Dysfunction in Diabetic Women: An Update on Current Knowledge. Diabetology 2020, 1, 11-21. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology1010002
Barbagallo F, Mongioì LM, Cannarella R, La Vignera S, Condorelli RA, Calogero AE. Sexual Dysfunction in Diabetic Women: An Update on Current Knowledge. Diabetology. 2020; 1(1):11-21. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology1010002
Chicago/Turabian StyleBarbagallo, Federica, Laura M. Mongioì, Rossella Cannarella, Sandro La Vignera, Rosita A. Condorelli, and Aldo E. Calogero. 2020. "Sexual Dysfunction in Diabetic Women: An Update on Current Knowledge" Diabetology 1, no. 1: 11-21. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology1010002