SARS-CoV-2 Spike Protein and Lung Vascular Cells



1
Department of Biochemistry and Molecular & Cell Biology, Georgetown University Medical Center, Washington, DC 20007, USA
2
Department of Pharmacology and Physiology, Georgetown University Medical Center, Washington, DC 20007, USA
*
Author to whom correspondence should be addressed.
J. Respir. 2021, 1(1), 40-48; https://0-doi-org.brum.beds.ac.uk/10.3390/jor1010004
Submission received: 11 December 2020
/
Revised: 22 December 2020
/
Accepted: 29 December 2020
/
Published: 31 December 2020
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is causing the current pandemic of coronavirus disease 2019 (COVID-19), and COVID-19 vaccines focus on its spike protein. However, in addition to facilitating the membrane fusion and viral entry, the SARS-CoV-2 spike protein promotes cell growth signaling in human lung vascular cells, and patients who have died of COVID-19 have thickened pulmonary vascular walls, linking the spike protein to a fatal disease, pulmonary arterial hypertension (PAH). In addition to SARS-CoV spike proteins, gp120, the viral membrane fusion protein of human immunodeficiency virus (HIV), has been reported to promote cell signaling, and long-term surviving HIV-positive patients have a high incidence of developing PAH. This article describes the findings of the SARS-CoV-2 spike protein affecting lung vascular cells and explains how the spike protein possibly increases the incidence of PAH. Since the SARS-CoV-2 spike protein will be administered to millions of people as COVID-19 vaccines, it is critical to understand the biological effects of this protein on human cells to ensure that it does not promote long-term adverse health consequences.
1. Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is causing the current pandemic of coronavirus disease 2019 (COVID-19) [1,2]. To date, over 75 million people have been infected with this virus, and COVID-19 has killed 1.7 million patients worldwide. In addition to the serious health problems, the pandemic has affected people economically, as well as sociologically, and the world awaits the means to end this horrible situation.
As a respiratory virus, the SARS-CoV-2 infection promotes severe pneumonia and acute respiratory distress syndrome [3]. One characteristic feature of the SARS-CoV-2 infection is, however, that elderly patients with pre-existing cardiovascular diseases are particularly susceptible to developing severe conditions and, ultimately, suffering death, while younger individuals only exhibit mild symptoms or are even asymptomatic when infected [2,4]. This feature of SARS-CoV-2 distinguishes it from other respiratory viruses and may serve as a basis for its profound effects. Thus, understanding these aspects of the disease could be crucial to developing therapeutic strategies to treat COVID-19.
Viruses use their membrane fusion proteins to bind to host cell receptors to facilitate entry into the cells through the process of membrane fusion and release the viral genomes [5]. The viral membrane fusion protein of SARS-CoV-2 is the spike protein, which is a Class I viral membrane fusion protein [2,6]. The host cell receptor of the SARS-CoV-2 spike protein for viral membrane fusion has been identified as angiotensin-converting enzyme 2 (ACE2) [7]. In humans, ACE2 (EC 3.4.17.23) normally functions as a peptidase enzyme that cleaves angiotensin II into angiotensin (1-7) [8]. Many cell types, including those in the lungs, arteries, heart, kidneys, and intestines, express ACE2 [9].
The SARS-CoV-2 spike protein consists of two subunits: Subunit 1 (S1) that contains the ACE2 receptor-binding domain (RBD) and Subunit 2 (S2) that participates in viral cell membrane fusion [3,6]. Since it is a well-conserved and exposed region of the virus, the spike protein has been used as the molecule to acquire immunity in the COVID-19 vaccines.
In addition to facilitating the viral entry and serving as the antigen for the vaccines, the SARS-CoV-2 spike protein elicits cell signaling in human host cells without the rest of the virus [10]. The SARS-CoV-2 spike protein is potent in affecting human pulmonary artery smooth muscle cells (PASMCs) and human pulmonary artery endothelial cells; pM levels of the recombinant protein were able to activate cell signaling. Thus, the spike protein of this virus can influence the host cells, and some of these actions could cause the pathogenesis of some diseases (Figure 1).
This review article describes the finding of the SARS-CoV-2 spike protein affecting lung vascular cells and explains how the spike protein (as a component of SARS-CoV-2, as well as the molecule used in COVID-19 vaccines) possibly increases the incidence of a fatal disease, pulmonary arterial hypertension (PAH). This article also surveys the literature to describe the current knowledge of the roles of the membrane fusion proteins of other viruses in eliciting cell signaling without the rest of the viral components to help tackle the problem of SARS-CoV-2. We conclude that it is critical to understand the biological actions of the SARS-CoV-2 spike protein in affecting human cells and possibly promoting long-term adverse health consequences, given that this protein will be administered to millions and possibly billions of people as vaccines.
2. The SARS-CoV-2 Spike Protein Activates Cell Signaling in Lung Vascular Cells
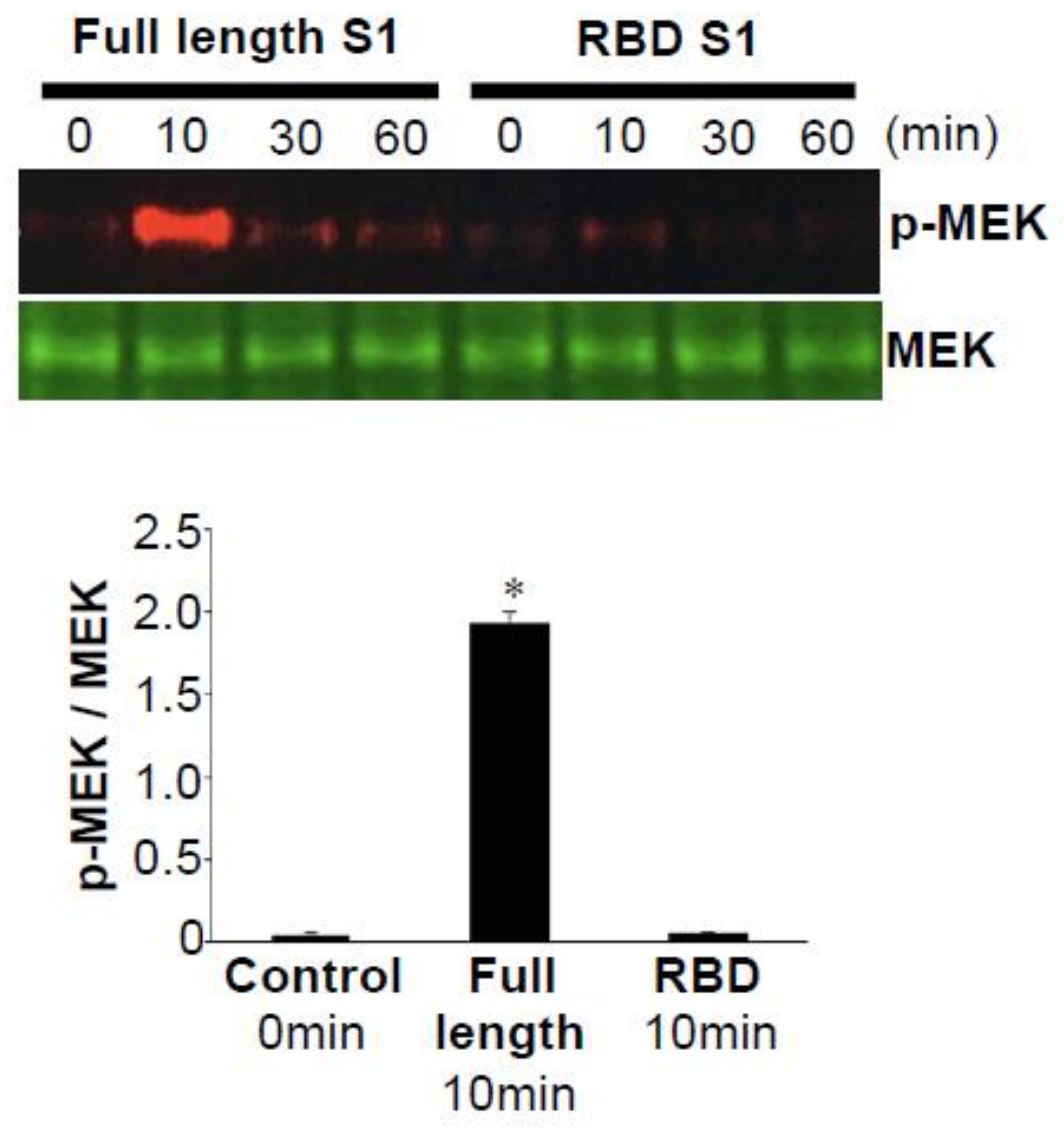
In the studies published by Suzuki et al. [10], cultured human PASMCs were treated with the recombinant full-length S1 subunit (Val16—Gln690) of the SARS-CoV-2 spike protein. As shown in Figure 2, the full-length S1 subunit of SARS-CoV-2 at a concentration as low as 130 pM strongly activated the phosphorylation of a mitogen-activated protein kinase kinase (MEK) at the Ser217 and Ser221 residues [10]. The kinetics of MEK phosphorylation promoted by the SARS-CoV-2 spike protein were consistently found to be transient, with a peak at 10 min. This fast activation suggests that it may be a receptor-mediated cell-signaling event. The recombinant SARS-CoV-2 spike protein also activated MEK in human pulmonary artery endothelial cells [10].
These results demonstrate that the SARS-CoV-2 spike protein without the rest of the virus can elicit cell signaling—specifically, the activation of the MEK/extracellular signal-regulated kinase (ERK) pathway—in human lung vascular smooth muscle and endothelial cells. The MEK/ERK pathway is a well-known cell growth mechanism [11]. Thus, this SARS-CoV-2 spike protein-mediated cell growth signaling may promote the thickening of pulmonary vessels in COVID-19. Consistently, we found that the pulmonary vessel walls of postmortem lung tissues from COVID-19 patients who died of acute respiratory distress syndrome were significantly thickened compared with those of H1N1 influenza patients who died of the same syndrome [10]. These results provide a possible link between the SARS-CoV-2 spike protein and PAH.
3. Pathology of PAH
PAH is a fatal disease without a cure that can affect both males and females of any age, including children [12,13]. It is a progressive disease, and by the time patients are diagnosed, the thickening of the pulmonary vascular walls has often already occurred. Increased resistance in the pulmonary circulation places strain on the right ventricle, which leads to right heart failure and death [12,13]. The median overall survival for patients with PAH is 2.8 years from the time of diagnosis (three-year survival: 48%) without treatment [14,15]. Even with currently available therapies, the prognosis remains poor, with a three-year survival of PAH patients reported to be only 58–75% [16,17,18,19].
4. Do the Membrane Fusion Proteins of Other Viruses Also Activate Cell Signaling in Host Cells without the Rest of the Viral Components?
As we surveyed the literature using keywords including phosphorylation, protein kinase, calcium, cAMP, and phospholipase, it was surprising to find that the recombinant viral membrane fusion proteins of SARS-CoV-1 and human immunodeficiency virus (HIV) were the only ones reported to elicit cell signaling in host cells. By contrast, an extensive literature search did not find publications showing that the recombinant viral membrane fusion proteins of other viruses, including Middle East respiratory syndrome-related coronavirus (MERS-CoV), Ebola, Zika, West Nile, dengue, herpes, and influenza, elicit cell signaling events in cultured host cells.
SARS-CoV (now known as SARS-CoV-1) caused the SARS outbreak in 2002–2004 [20]. Its spike protein, which is 76–78% identical to that of SARS-CoV-2 [21], has been reported to activate the casein kinase II-dependent activation of the ERK pathway through ACE2 in the A549 human lung epithelial cell line [22]. This pathway activated by the SARS-CoV-1 spike protein also caused the upregulation of monocyte chemoattractant protein-1 (MCP-1) expression and release. This study demonstrated that ACE2 (which is a peptidase, not a cell signaling receptor) could also act as a receptor for cell signaling only in response to the spike protein, reinforcing the idea that host human lung cells are sufficiently sensitive to be affected by this viral membrane fusion protein. In addition, MCP-1 has been shown to be increased in PAH patients [23], providing another link between the spike protein and PAH.
The treatment of human brain microvascular endothelial cells with the recombinant HIV-1 gp120 protein was found to activate signal transducer and activator of transcription 1 (STAT1) and induce interleukin (IL)-6 and IL-8 secretion [24]. These gp120-induced IL-6 and IL-8 secretion processes were inhibited by a STAT1 inhibitor [24]. Similarly, gp120 activated the STAT3/IL-6 axis of cell signaling in human monocyte-derived dendritic cells [25]. Hioe et al. [26] reported that HIV-1 gp120 was sufficient to trigger leukocyte function antigen-1 (LFA-1) activation in T cells in a CD4-dependent manner.
The HIV gp120 protein has also been shown to activate cell signaling without the rest of the HIV components in pulmonary vascular cells, as described below, and this viral membrane fusion protein appears to play a crucial role in the development of PAH.
5. HIV Increases the Incidence of PAH
HIV-associated PAH occurs in approximately one out of 200 HIV-infected patients [27,28,29,30], which is 100–500 times higher than the prevalence of PAH in individuals without HIV. A large prospective study of 7648 patients with HIV from 2004 to 2005—after the introduction of potent antiretroviral therapy (ART)—showed a prevalence of right-heart catheterization-confirmed HIV-PAH of 0.5% [30]. These findings are similar to those studies performed before the use of effective ART. Thus, ART does not seem to have altered the prevalence of HIV-associated PAH, providing evidence for the direct role of HIV and/or its molecular components in promoting the pathogenesis of PAH.
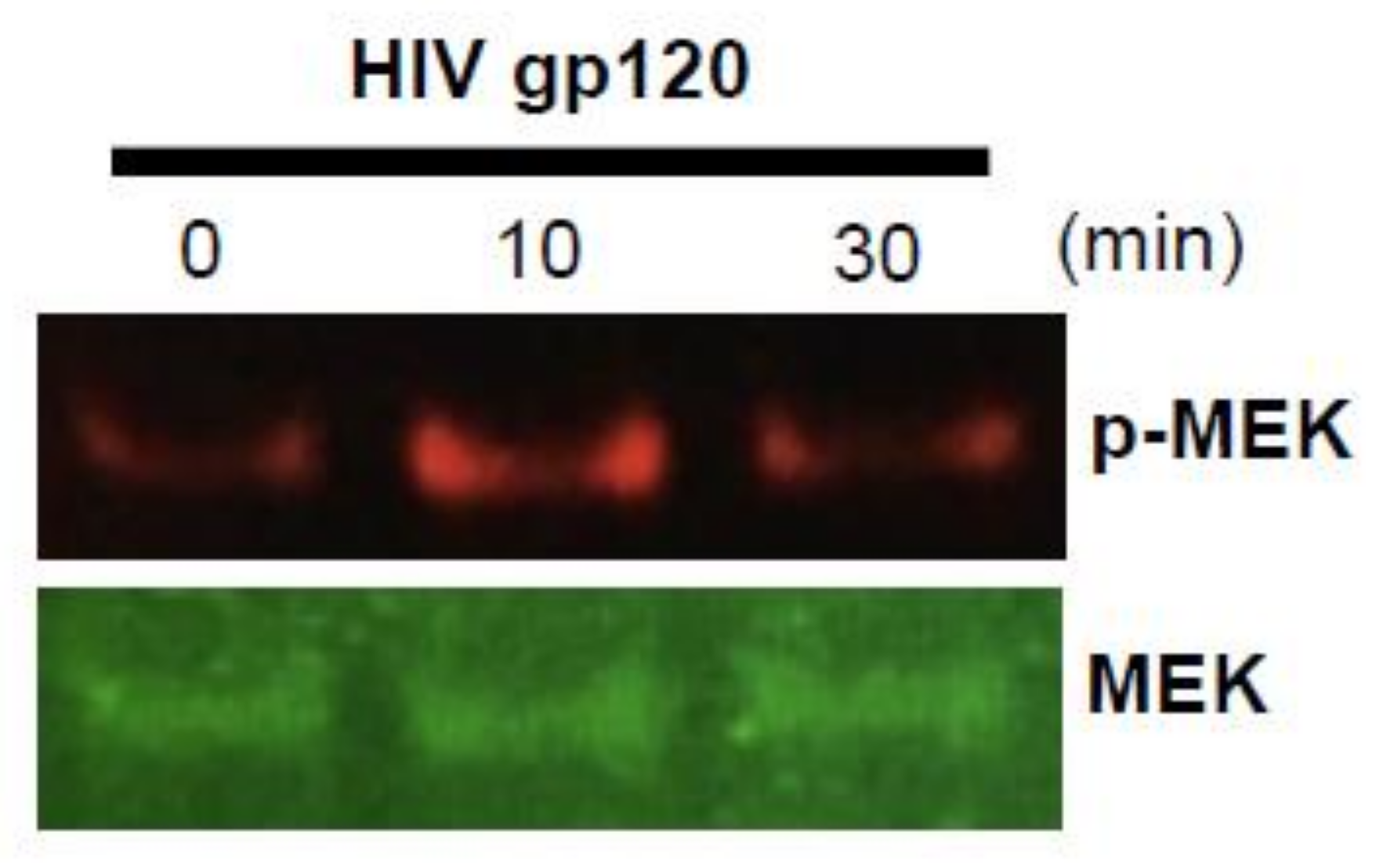
The viral membrane fusion protein of HIV, gp120, has been shown to activate the cell signaling pathway for the induction of tissue factor expression through chemokine receptors, protein kinase C, mitogen-activated protein kinases, and reactive oxygen species in human vascular smooth muscle cells [31]. Since the tissue factor has been implicated in the pathogenesis of PAH [32,33], these findings provided a possible link between gp120 and PAH. Figure 3 shows our experimental results demonstrating that recombinant HIV gp120 at 80 pM activated MEK in human PASMCs. Additionally, in human PAMSCs, gp120 at 100 pM increased the intracellular calcium and induced cell growth [34]. These effects of gp120 were inhibited by an inhibitor of CCR5, a coreceptor for cellular HIV entry, providing the causal link between gp120 signaling and PASMC growth. Further, in CCR5-deficient mice, hypoxic pulmonary hypertension was abrogated [34]. In human lung microvascular endothelial cells, gp120 promoted apoptosis and the secretion of endothelin-1, which mediate the development of PAH [35]. These results suggest that the membrane fusion protein of HIV, gp120, likely participates in the development of PAH.
6. Are Individuals Infected with SARS-CoV-2 Predisposed to Developing PAH?
Our results showed that the SARS-CoV-2 spike protein activated cell growth signaling in human PASMCs and in human pulmonary artery endothelial cells and that patients who died of COVID-19 exhibited thickened pulmonary vascular walls [10], which may suggest that the spike protein predisposes individuals infected with SARS-CoV-2 to develop PAH in the future. SARS-CoV-2 infection and exposure to the spike protein may trigger cell signaling events, promoting the pathogenesis of PAH in both patients who survived severe COVID-19 conditions, as well as individuals who exhibited mild symptoms or even were asymptomatic. Coincidentally, the only other virus whose membrane fusion protein has been shown to activate cell signaling (i.e., HIV) also predisposes infected patients to develop PAH. Further experimentations and careful clinical observations for PAH in relation to SARS-CoV-2 and COVID-19 are, thus, warranted.
7. COVID-19 Vaccines and PAH
COVID-19 vaccines currently under consideration, including RNA vaccines (BNT162b2 and mRNA-1273) [36,37,38], viral vector-based vaccines (AZD1222 and Ad26.COV2.S) [39,40], and recombinant protein (NVX-CoV2373) [41], all introduce the SARS-CoV-2 spike protein into the human body. Whether the spike protein elicits cell signaling in host cells and exerts adverse events such as promoting PAH is a question raised in response to the experimental results in cultured cells [10]. RNA and viral vector-based vaccines use human host cells to produce the spike protein; thus, the intracellular spike protein will be produced. The intracellular effects of this foreign molecule on human cells have not been defined.
BNT162b2 encodes the full-length spike protein of SARS-CoV-2 with two proline mutations [36,37], while its sister vaccine BNT162b1 encodes only the RBD of the SARS-CoV-2 spike protein, trimerized by the addition of a T4 fibritin foldon domain [42,43]. Our experiments also revealed that, in contrast to the full-length S1 subunit (Val16—Gln690) of the SARS-CoV-2 spike protein that activated cell signaling, the S1 RBD (Arg319—Phe541) did not elicit such events [10]. Figure 2 shows that, while the full-length S1 subunit strongly activated MEK, the S1 RBD did not activate MEK in human PASMCs [10]. Similarly, the full-length S1 subunit, but not the RBD-only containing S1 subunit, of the SARS-CoV-2 spike protein promoted the phosphorylation of MEK in human pulmonary artery endothelial cells [10]. Thus, the RBD-only protein such as the one encoded by the BNT162b1 vaccine may not impose the risk of developing PAH. Further work is needed to understand the effects of various SARS-CoV-2 spike protein segments on human host cells in order to develop the most efficacious and safe vaccines without long-term adverse consequences.
8. Conclusions
This analysis suggests that the SARS-CoV-2 spike protein and HIV gp120 have the capacity to trigger cell biological events that may lead to the development of pulmonary vascular remodeling and, perhaps, clinically significant PAH, a fatal condition. Given the observations that cells sensitively respond to the spike protein at pM concentrations in cultured cells [10], it is likely that the SARS-CoV-2 spike protein not only facilitates the viral entry and serves to acquire immunity as an antigen for vaccines but, also, targets host cells and may exert adverse effects (Figure 4). Further experiments should be performed to address the possible effects of the SARS-CoV-2 spike protein on developing PAH. The effects of the SARS-CoV-2 spike protein on the cells of other tissues/organs, such as those of the systemic vasculature, heart, and brain, should also be investigated. Given that this protein will be administered as vaccines to millions and possibly billions of people, it is critical to understand the extracellular and intracellular effects of the SARS-CoV-2 spike protein on human cells that may promote long-term adverse health consequences.
Author Contributions
Conceptualization, Y.J.S.; validation, S.J.S. and Y.J.S.; investigation, S.J.S. and Y.J.S.; resources, Y.J.S.; writing—original draft preparation, S.J.S. and Y.J.S.; writing—review and editing, S.J.S. and Y.J.S.; visualization, S.J.S. and Y.J.S.; supervision, Y.J.S.; project administration, Y.J.S.; and funding acquisition, Y.J.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the National Institutes of Health (NIH), grant numbers R21AI142649, R03AG059554, and R03AA026516 to Y.S. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.-M.; Wang, W.; Song, Z.-G.; Hu, Y.; Tao, Z.-W.; Tian, J.-H.; Pei, Y.-Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Mohanty, S.K.; Satapathy, A.; Naidu, M.M.; Mukhopadhyay, S.; Sharma, S.; Barton, L.M.; Stroberg, E.; Duval, E.J.; Pradhan, D.; Tzankov, A.; et al. Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) and coronavirus disease 19 (COVID-19)—Anatomic pathology perspective on current knowledge. Diagn. Pathol. 2020, 15, 103. [Google Scholar] [CrossRef]
- White, J.M.; Delos, S.E.; Brecher, M.; Schornberg, K. Structures and Mechanisms of Viral Membrane Fusion Proteins: Multiple Variations on a Common Theme. Crit. Rev. Biochem. Mol. Biol. 2008, 43, 189–219. [Google Scholar] [CrossRef] [Green Version]
- Walls, A.C.; Park, Y.J.; Tortorici, M.A.; Wall, A.; McGuire, A.T.; Veesler, D. Structure, function, and antigenicity of the SARS-CoV-2 spike glycoprotein. Cell 2020, 181, 281–292. [Google Scholar] [CrossRef]
- Yan, R.; Zhang, Y.; Li, Y.; Xia, L.; Guo, Y.; Zhou, Q. Structural basis for the recognition of SARS-CoV-2 by full-length human ACE2. Science 2020, 367, 1444–1448. [Google Scholar] [CrossRef] [Green Version]
- Gheblawi, M.; Wang, K.; Viveiros, A.; Nguyen, Q.; Zhong, J.; Turner, A.J.; Raizada, M.K.; Grant, M.B.; Oudit, G.Y. Angiotensin-converting enzyme 2: SARS-CoV-2 receptor and regulator of the renin-angiotensin system: Celebrating the 20th anniversary of the discovery of ACE2. Circ. Res. 2020, 126, 1456–1474. [Google Scholar] [CrossRef]
- Hamming, I.; Timens, W.; Bulthuis, M.L.C.; Lely, A.T.; Navis, G.J.; Van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef]
- Suzuki, Y.J.; Nikolaienko, S.I.; Dibrova, V.A.; Dibrova, Y.V.; Vasylyk, V.M.; Novikov, M.Y.; Shults, N.V.; Gychka, S.G. SARS-CoV-2 spike protein-mediated cell signaling in lung vascular cells. Vasc. Pharmacol. 2020, 106823. [Google Scholar] [CrossRef]
- Zhang, W.; Liu, H.T. MAPK signal pathways in the regulation of cell proliferation in mammalian cells. Cell Res. 2002, 12, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Delcroix, M.; Naeije, R. Optimising the management of pulmonary arterial hypertension patients: Emergency treatments. Eur. Respir. Rev. 2010, 19, 204–211. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, V.V.; Shah, S.J.; Souza, R.; Humbert, M. Management of Pulmonary Arterial Hypertension. J. Am. Coll. Cardiol. 2015, 65, 1976–1997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Alonzo, G.E.; Barst, R.J.; Ayres, S.M.; Bergofsky, E.H.; Brundage, B.H.; Detre, K.M.; Fishman, A.P.; Goldring, R.M.; Groves, B.M.; Kernis, J.T.; et al. Survival in Patients with Primary Pulmonary Hypertension. Results from a national prospective registry. Ann. Intern. Med. 1991, 115, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Runo, J.R.; Loyd, J.E. Primary pulmonary hypertension. Lancet 2003, 361, 1533–1544. [Google Scholar] [CrossRef] [Green Version]
- Benza, R.L.; Miller, D.P.; Frost, A.; Barst, R.J.; Krichman, A.M.; McGoon, M.D. Analysis of the Lung Allocation Score Estimation of Risk of Death in Patients with Pulmonary Arterial Hypertension Using Data From the REVEAL Registry. Transplantation 2010, 90, 298–305. [Google Scholar] [CrossRef]
- Humbert, M.; Sitbon, O.; Yaici, A.; Montani, D.; O’Callaghan, D.S.; Jais, X.; Parent, F.; Savale, L.; Natali, D.; Gunther, S.; et al. Survival in incident and prevalent cohorts of patients with pulmonary arterial hypertension. Eur. Respir. J. 2010, 36, 549–555. [Google Scholar] [CrossRef] [Green Version]
- Thenappan, T.; Shah, S.J.; Rich, S.S.; Tian, L.; Archer, S.L.; Gombergmaitland, M. Survival in pulmonary arterial hypertension: A reappraisal of the NIH risk stratification equation. Eur. Respir. J. 2009, 35, 1079–1087. [Google Scholar] [CrossRef] [Green Version]
- Olsson, K.M.; Delcroix, M.; Ghofrani, H.A.; Tiede, H.; Huscher, D.; Speich, R.; Grünig, E.; Staehler, G.; Rosenkranz, S.; Halank, M.; et al. Anticoagulation and Survival in Pulmonary Arterial Hypertension: Results From the Comparative, Prospective Registry of Newly Initiated Therapies for Pulmonary Hypertension (COMPERA). Circulation 2014, 129, 57–65. [Google Scholar] [CrossRef] [Green Version]
- Cherry, J.D. The chronology of the 2002–2003 SARS mini pandemic. Paediatr. Respir. Rev. 2004, 5, 262–269. [Google Scholar] [CrossRef]
- Wan, Y.; Shang, J.; Graham, R.; Baric, R.S.; Li, F. Receptor recognition by the novel coronavirus from Wuhan: An analysis based on decade-long structural studies of SARS coronavirus. J. Virol. 2020, 94, e00120–e00127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, I.-Y.; Chang, S.-C.; Wu, H.-Y.; Yu, T.-C.; Wei, W.-C.; Lin, S.; Chien, C.-L.; Chang, M.-F. Upregulation of the Chemokine (C-C Motif) Ligand 2 via a Severe Acute Respiratory Syndrome Coronavirus Spike-ACE2 Signaling. J. Virol. 2010, 84, 7703–7712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Itoh, T.; Nagaya, N.; Ishibashi-Ueda, H.; Kyotani, S.; Oya, H.; Sakamaki, F.; Kimura, H.; Nakanishi, N. Increased plasma monocyte chemoattractant protein-1 level in idiopathic pulmonary arterial hypertension. Respirology 2006, 11, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Akhter, S.; Chaudhuri, A.; Kanmogne, G.D. HIV-1 gp120 induces cytokine expression, leukocyte adhesion, and transmigration across the blood–brain barrier: Modulatory effects of STAT1 signaling. Microvasc. Res. 2009, 77, 212–219. [Google Scholar] [CrossRef] [Green Version]
- Del Cornò, M.; Donninelli, G.; Varano, B.; Da Sacco, L.; Masotti, A.; Gessani, S. HIV-1 gp120 Activates the STAT3/Interleukin-6 Axis in Primary Human Monocyte-Derived Dendritic Cells. J. Virol. 2014, 88, 11045–11055. [Google Scholar] [CrossRef] [Green Version]
- Hioe, C.E.; Tuen, M.; Vasiliver-Shamis, G.; Alvarez, Y.; Prins, K.C.; Banerjee, S.; Nadas, A.; Cho, M.W.; Dustin, M.L.; Kachlany, S.C. HIV Envelope gp120 Activates LFA-1 on CD4 T-Lymphocytes and Increases Cell Susceptibility to LFA-1-Targeting Leukotoxin (LtxA). PLoS ONE 2011, 6, e23202. [Google Scholar] [CrossRef] [Green Version]
- Isasti, G.; Moreno, T.; Pérez, I.; Cabrera, F.; Palacios, R.; Santos, J. High Prevalence of Pulmonary Arterial Hypertension in a Cohort of Asymptomatic HIV-Infected Patients. AIDS Res. Hum. Retrovir. 2013, 29, 231–234. [Google Scholar] [CrossRef]
- Mehta, N.J.; Khan, I.A.; Mehta, R.N.; Sepkowitz, D.A. HIV-Related pulmonary hypertension: Analytic review of 131 cases. Chest 2000, 118, 1133–1141. [Google Scholar] [CrossRef] [Green Version]
- Pellicelli, A.; Barbaro, G.; Palmieri, F.; Girardi, E.; D’Ambrosio, C.; Rianda, A.; Barbarini, G.; Frigiotti, D.; Borgia, M.C.; Petrosillo, N. Primary Pulmonary Hypertension in HIV Patients: A Systematic Review. Angiology 2001, 52, 31–41. [Google Scholar] [CrossRef]
- Sitbon, O.; Lascoux-Combe, C.; Delfraissy, J.-F.; Yeni, P.G.; Raffi, F.; De Zuttere, D.; Gressin, V.; Clerson, P.; Sereni, D.; Simonneau, G. Prevalence of HIV-related Pulmonary Arterial Hypertension in the Current Antiretroviral Therapy Era. Am. J. Respir. Crit. Care Med. 2008, 177, 108–113. [Google Scholar] [CrossRef]
- Schecter, A.D.; Berman, A.B.; Yi, L.; Mosoian, A.; McManus, C.M.; Berman, J.W.; Klotman, M.E.; Taubman, M.B. HIV envelope gp120 activates human arterial smooth muscle cells. Proc. Natl. Acad. Sci. USA 2001, 98, 10142–10147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, T.A.; Witt, T.A.; Pan, S.; Mueske, C.S.; Kleppe, L.S.; Holroyd, E.W.; Champion, H.C.; Simari, R.D. Tissue Factor Pathway Inhibitor Overexpression Inhibits Hypoxia-Induced Pulmonary Hypertension. Am. J. Respir. Cell Mol. Biol. 2010, 43, 35–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, R.J.; Meoli, D.F.; Swarthout, R.F.; Kallop, D.Y.; Galaria, I.I.; Harvey, J.L.; Miller, C.M.; Blaxall, B.C.; Hall, C.M.; Pierce, R.A.; et al. Plexiform-like lesions and increased tissue factor expression in a rat model of severe pulmonary arterial hypertension. Am. J. Physiol. Cell. Mol. Physiol. 2007, 293, L583–L590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amsellem, V.; Lipskaia, L.; Abid, S.; Poupel, L.; Houssaini, A.; Quarck, R.; Marcos, E.; Mouraret, N.; Parpaleix, A.; Bobe, R.; et al. CCR5 as a treatment target in pulmonary arterial hypertension. Circulation 2014, 130, 880–891. [Google Scholar] [CrossRef]
- Kanmogne, G.D.; Primeaux, C.; Grammas, P. Induction of apoptosis and endothelin-1 secretion in primary human lung endothelial cells by HIV-1 gp120 proteins. Biochem. Biophys. Res. Commun. 2005, 333, 1107–1115. [Google Scholar] [CrossRef]
- Walsh, E.E.; Frenck, R.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. RNA-Based COVID-19 Vaccine BNT162b2 Selected for a Pivotal Efficacy Study. medRxiv 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.08.17.20176651v2 (accessed on 28 August 2020). [CrossRef]
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and immunogenicity of two RNA-based Covid-19 vaccine candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef]
- Jackson, L.A.; Anderson, E.J.; Rouphael, N.G.; Roberts, P.C.; Makhene, M.; Coler, R.N.; McCullough, M.P.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; et al. An mRNA vaccine against SARS-CoV-2—Preliminary report. N. Engl. J. Med. 2020, 383, 1920–1931. [Google Scholar] [CrossRef]
- Folegatti, P.M.; Ewer, K.J.; Aley, P.K.; Angus, B.; Becker, S.; Belij-Rammerstorfer, S.; Bellamy, D.; Bibi, S.; Bittaye, M.; Clutterbuck, E.A.; et al. Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine against SARS-CoV-2: A preliminary report of a phase 1/2, single-blind, randomised controlled trial. Lancet 2020, 396, 467–478. [Google Scholar] [CrossRef]
- Mercado, N.B.; Zahn, R.; Wegmann, F.; Loos, C.; Chandrashekar, A.; Yu, J.; Liu, J.; Peter, L.; McMahan, K.; Tostanoski, L.H.; et al. Single-shot Ad26 vaccine protects against SARS-CoV-2 in rhesus macaques. Nature 2020, 586, 583–588. [Google Scholar] [CrossRef]
- Guebre-Xabier, M.; Patel, N.; Tian, J.-H.; Zhou, B.; Maciejewski, S.; Lam, K.; Portnoff, A.D.; Massare, M.J.; Frieman, M.B.; Piedra, P.A.; et al. NVX-CoV2373 vaccine protects cynomolgus macaque upper and lower airways against SARS-CoV-2 challenge. Vaccine 2020, 38, 7892–7896. [Google Scholar] [CrossRef] [PubMed]
- Mulligan, M.J.; Lyke, K.E.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Raabe, V.; Bailey, R.; Swanson, K.A.; et al. Phase I/II study of COVID-19 RNA vaccine BNT162b1 in adults. Nature 2020, 586, 589–593. [Google Scholar] [CrossRef] [PubMed]
- Sahin, U.; Muik, A.; Derhovanessian, E.; Vogler, I.; Kranz, L.M.; Vormehr, M.; Baum, A.; Pascal, K.; Quandt, J.; Maurus, D.; et al. COVID-19 vaccine BNT162b1 elicits human antibody and T H 1 T cell responses. Nature 2020, 586, 594–599. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Actions of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spike protein. In addition to facilitating SARS-CoV-2 entry into host cells and serving as the basis for the vaccine development, the spike protein of this virus also influences the host cells by activating cell signaling. Spike protein-mediated cell signaling could have adverse consequences.
Figure 1.
Actions of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spike protein. In addition to facilitating SARS-CoV-2 entry into host cells and serving as the basis for the vaccine development, the spike protein of this virus also influences the host cells by activating cell signaling. Spike protein-mediated cell signaling could have adverse consequences.

Figure 2.
Full-length SARS-CoV-2 spike protein subunit 1 (S1), but not the receptor-binding domain (RBD)-only containing S1 protein, activates mitogen-activated protein kinase kinase (MEK) phosphorylation. Human pulmonary artery smooth muscle cells (PASMCs) were treated with the recombinant full-length S1 subunit (Val16—Gln690) or the RBD region of the S1 subunit (Arg319—Phe541). Cell lysates were prepared and subjected to Western blotting using antibodies against phosphorylated MEK (p-MEK) and the MEK protein. The bar graph represents means ± SEM. * Significantly different from the 0-min control at p < 0.05 (Taken from Suzuki et al. [10]).
Figure 2.
Full-length SARS-CoV-2 spike protein subunit 1 (S1), but not the receptor-binding domain (RBD)-only containing S1 protein, activates mitogen-activated protein kinase kinase (MEK) phosphorylation. Human pulmonary artery smooth muscle cells (PASMCs) were treated with the recombinant full-length S1 subunit (Val16—Gln690) or the RBD region of the S1 subunit (Arg319—Phe541). Cell lysates were prepared and subjected to Western blotting using antibodies against phosphorylated MEK (p-MEK) and the MEK protein. The bar graph represents means ± SEM. * Significantly different from the 0-min control at p < 0.05 (Taken from Suzuki et al. [10]).

Figure 3.
HIV gp120 activates MEK phosphorylation. Human PASMCs (purchased from ScienCell Research Laboratories, Carlsbad, CA, USA) were treated with the recombinant HIV gp120 (Glu31-Arg494, Accession# AAT67478.1; Catalog # 40403-V08H, SinoBiological, Wayne, PA, USA) at 80 pM. Cell lysates were prepared and subjected to Western blotting using antibodies against phosphorylated MEK (p-MEK) and the MEK protein (Cell Signaling Technology, Danvers, MA, USA).
Figure 3.
HIV gp120 activates MEK phosphorylation. Human PASMCs (purchased from ScienCell Research Laboratories, Carlsbad, CA, USA) were treated with the recombinant HIV gp120 (Glu31-Arg494, Accession# AAT67478.1; Catalog # 40403-V08H, SinoBiological, Wayne, PA, USA) at 80 pM. Cell lysates were prepared and subjected to Western blotting using antibodies against phosphorylated MEK (p-MEK) and the MEK protein (Cell Signaling Technology, Danvers, MA, USA).

Figure 4.
What are the consequences of the SARS-CoV-2 spike protein? Through SARS-CoV-2 infection and the COVID-19 vaccination, the spike protein is about to become a part of the human body. Some vaccines will also produce the intracellular spike protein in human cells. We need to know the biological actions of this protein that is new to human physiology.
Figure 4.
What are the consequences of the SARS-CoV-2 spike protein? Through SARS-CoV-2 infection and the COVID-19 vaccination, the spike protein is about to become a part of the human body. Some vaccines will also produce the intracellular spike protein in human cells. We need to know the biological actions of this protein that is new to human physiology.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Suresh, S.J.; Suzuki, Y.J. SARS-CoV-2 Spike Protein and Lung Vascular Cells. J. Respir. 2021, 1, 40-48. https://0-doi-org.brum.beds.ac.uk/10.3390/jor1010004
AMA Style
Suresh SJ, Suzuki YJ. SARS-CoV-2 Spike Protein and Lung Vascular Cells. Journal of Respiration. 2021; 1(1):40-48. https://0-doi-org.brum.beds.ac.uk/10.3390/jor1010004
Chicago/Turabian StyleSuresh, Sri Jayalakshmi, and Yuichiro Justin Suzuki. 2021. "SARS-CoV-2 Spike Protein and Lung Vascular Cells" Journal of Respiration 1, no. 1: 40-48. https://0-doi-org.brum.beds.ac.uk/10.3390/jor1010004