The Relationship between Mindfulness and Sleep Quality is Mediated by Emotion Regulation



Department of Psychology, University of South Alabama, Mobile, AL 36695, USA
*
Author to whom correspondence should be addressed.
Psychiatry Int. 2020, 1(2), 42-66; https://0-doi-org.brum.beds.ac.uk/10.3390/psychiatryint1020007
Submission received: 3 September 2020
/
Revised: 23 September 2020
/
Accepted: 13 October 2020
/
Published: 21 October 2020
Abstract
:Background: Sleep is critical to a person’s overall physical and mental health. The current study investigated the relationship between mindfulness and sleep quality, to determine if this relationship is influenced by emotion regulation and perceived stress. Method: Three hundred sixty-seven undergraduate students responded to five self-report measures, (1) The Cognitive and Affective Mindfulness Scale (CAMS-R), (2) The Impact of Event Scale (IES-R), (3) The Five Facet Mindfulness Questionnaire (FFMQ), (4) The Emotion Regulation Questionnaire (ERQ), and (5) The Pittsburgh Sleep Quality Index (PSQI). Results: Results revealed (1) sleep quality was predicted by the presence of hyperarousal, acting with awareness, and the CAMS-R, (2) the Impact of Event Scale was moderately positively correlated with a person’s global score on the Pittsburgh Sleep Quality Index, and (3) the relationship between mindfulness and sleep quality was mediated by hyperarousal. Conclusions: Together, our findings suggest that higher levels of intrusive thoughts, avoidance, and hyperarousal are correlated with lower overall sleep quality, and the use of mindfulness techniques such as acting with awareness and being non-reacting to negative thoughts or hyperarousal may help predict an individual’s sleep quality.
1. Introduction
Sleep is one of the most critical determinants of a person’s physical and mental health. If a person does not get proper sleep, then there is an increased risk of anxiety or depression. A loss of sleep can also result in a weakened immune system [1]. Furthermore, Palmer et al. (2018) [1] suggest that poor sleep quality is one the biggest public health problems in the United States, particularly among adolescents. Moreover, sleep quality has also been shown to greatly influence cognitive performance [2,3,4,5,6]. Given the importance of sleep quality for optimal cognitive function and health outcomes, it is critical to enhance our understanding of factors associated with good quality sleep. The current study examines candidate emotional and cognitive factors from the research literature that may help us to explain the variability in individuals’ sleep quality.
Palmer and Alfano (2017) [7] suggest that emotion regulation is crucial for achieving restful sleep and achieving higher overall psychological health. Emotion regulation is typically defined as the internal and external processes that occur when coping with an emotion, and when these processes occur, they can have a positive or negative impact on someone’s overall emotional perception during their pursuit of a goal [8,9]. Emotion regulation is a process that occurs in stages and usually has genetic and biological components, but emotion regulation may be improved with practice or training [8,9,10,11]. One influential technique for promoting emotion regulation and self-awareness is mindfulness meditation and related therapies [10,12,13]. In a related study, Thompson & Waltz (2010) [14] surveyed 378 undergraduates on self-report measures of PTSD, mindfulness, experiential avoidance, thought suppression, and avoidance coping. In their results they found that the experiential non-judgment aspects of mindfulness accounted for a unique portion of the variance in avoidance coping.
This study investigates how mindfulness is correlated with sleep quality. The construct of mindfulness is complex, but can best be described by the following features: using the present moment, deep breathing, quieting the thoughts, and non-judgment—all of which reduce cognitive pressure on a person [10,15]. These constructs provide a basis for the current study, and the purpose of the current study is to provide an extension of the current literature regarding how mindfulness and emotion regulation correlate with sleep quality.
1.1. Homeostasis: The Circadian Drive
Research has shown there are many underlying cognitive factors that influence a person’s sleep quality such as the presence of psychiatric disorders or emotion regulation difficulties [1,7]. Individual differences such as circadian drive are going to influence a person’s reported sleep quality [16]. The circadian drive controls a person’s onset of wakefulness and sleep. Circadian clocks are localized in the suprachiasmatic nucleus and the ventrolateral pre-optic nucleus and are synchronized to environmental cues known as zeitgeibers—some of which are light exposure throughout the day, meals, and exercise [16]. The circadian clock monitors the amount of adenosine in the brain, which is a by-product of staying awake. However, there are other environmental factors contributing to poor sleep by desynchronizing the homeostasis of the individual—which can include the work schedule of the individual, the consistency of their daily sleep schedule, how much light they are exposed to before bed, caffeine intake, and alcohol intake [16]. When there is significant desynchrony in the circadian drive it can result in sleep disorders such as insomnia. Insomnia is the inability to fall asleep or stay asleep [17]; furthermore, insomnia and sleep loss can have many negative side effects such as daytime drowsiness which can further lead to slowed cognition [3], and a plethora of negative consequences such as irritability and impeded emotion regulation [1,7].
1.2. Sleep Quality, Mental Health, and Emotion
Sleep plays a critical role in mental health across a person’s lifespan. Furthermore, disrupted sleep slows neurocognitive functioning, and poor sleep is a risk factor and common symptom for a wide variety of psychiatric disorders—most notably anxiety. People with anxiety are more prone to sleep loss, and consequently experience, higher arousal, and more frequent negative emotions. People with anxiety also experience less positive emotions, and as a result they have more difficulty regulating their emotions—which is a paramount issue in psychopathology [7].
1.3. Mindfulness and Emotion Regulation
Findings suggest state mindfulness increases psychological well-being if used consistently over time, and leads to a less stressed disposition [16]. Mindfulness is a non-judgmental and attentive focus on the present and is a healthy way to cope with emotions through a process collectively called emotion regulation. Arch and Craske (2006) [15] found mindfulness leads to lower negative affect, lower emotional reactivity, and lower emotional volatility whereas Garland et al. (2015) [17] found that mindfulness promotes emotion regulation by enhancing cognitive reappraisal.
The use of mindfulness is mostly associated with meditation practices, but it is also frequently implemented in psychotherapy practices [13]. Findings have speculated mindfulness can be implemented into everyday life as mindfulness has a focus on the emotional experiences associated with a particular event [13]. Mindfulness increases activation in the frontal cortex and is associated with emotion modulating areas such as the prefrontal cortex and anterior cingulate cortex—which are important areas for executive control. Lutz et al. (2014) [13] found individuals who use mindfulness exhibited reduced activation in emotional processing areas such as: the amygdala and parahippocampal gyrus when they were presented with negative stimuli. Reduced activation in emotional processing areas indicates healthy emotion regulation, which has been linked to good overall sleep quality [18].
1.4. Emotion Regulation and Sleep Quality
Sleep quality is usually defined as how well a person is sleeping and is assessed by the frequency and severity of sleep onset issues, sleep duration, sleep disturbances, the use of sleeping medications, and daytime drowsiness [18,19,20,21,22,23]. Sleep quality is complicated to measure, but one of the most common scales used to measure sleep quality is the Pittsburgh Sleep Quality Index (PSQI). The PSQI has several advantages because it uses quantitative and qualitative data to determine sleep dysfunctions over the span of a month, and it calculates a simple number to illustrate the severity of sleep issues—indicating poor sleep quality [19].
Increased sleep disturbances and poor sleep quality negatively impact quality of life and has been linked to physical and mental illness [19]. Poor sleep quality has also been linked to negative emotional consequence [23] where poor sleep quality is associated with unhealthy coping and good sleep quality is associated with healthy coping [18]. At a neurobiological level, sleep loss and poor sleep quality lead to decreased connectivity in the medial prefrontal cortex and the ventral anterior cingulate, which suggests there could be problems in monitoring and inhibiting emotional control [7]. Palmer and Alfano (2017) [7] present a meta-analysis where they discuss a framework speculating that emotion regulation involves stages: (1) situation selection, (2) situational modification, (3) attentional deployment, (4) cognitive change, and (5) response modulation. Palmer and Alfano call for further research to explain the specific points in the process of emotion regulation that are the most susceptible to causing sleep loss. How a person regulates their emotions can have a positive or negative impact on their stress levels, stress response, and their overall mood [24].
1.5. Coping: Intrusiveness, Avoidance, Arousal, and Sleep Quality
Stress impacts a person’s mood, causing the person’s mood to decline to a more negative state, and eventually leading to sleep being compromised [24]. Cognitive arousal has been associated with poor and disrupted sleep, and the coping behaviors people use to combat this arousal are important to a person’s sleep quality [24]. Cognitive arousal can manifest into anxiety and depression, which is attributed to stress, and unmanaged stress can lead to sleep problems [12].
Research has suggested sleep related difficulties have been linked to higher fatigue levels, higher stress levels, a compromised immune system, and an overall poorer quality of life [24]. Hoyt et al. (2009) [24] found the use avoidance coping was significantly related to sleep issues. Intrusive thoughts and avoidance behaviors are commonly experienced when a person experiences stressful life events, or when a person is going through bereavement or depression [22]. Negative intrusive thoughts have been said to be linked to lower ratios of delta waves and increased sleep latency periods, where there is an increased frequency of non-rapid eye movement (NREM)sleep and more beta waves, which are associated with wakefulness—coupled with less delta waves, which are associated with deeper levels of sleep [22]. Thus, stressful events elicit intrusive thoughts and avoidance associated with physiological arousal, which elicits the fight or flight response, where there is an increased activity in the sympathetic nervous system. The increased neural activity causes cognitive pressure, therefore having a negative impact on sleep quality [22]. Research suggests mindfulness techniques can be an effective method for coping with the cognitive pressure associated with stress [10,15,16,17].
Payne, et al. (2019) [25] present a meta-analysis in which they detail how intrusive thoughts have been the underlying basis for revisiting stressful memories, and they discuss the prevalence of intrusive thoughts. Pooled analyses from seven studies of intrusive memory prevalence suggested individuals with depression who typically have higher emotion regulation difficulties are more likely to experience intrusive thoughts or intrusive memories. Roemer and Orsillo (2002) [26] present a research proposal in which they highlight how the psychopathology of generalized anxiety disorder can influence the response to a traumatic event. They assert that acceptance (a major aspect of mindfulness) based treatments with cognitive behavioral therapy can actually have a higher efficacy when helping patients who present with anxiety disorders obtain better outcomes. Cowdrey and Park (2012) [27] examined the associations between disorder rumination, mindfulness, avoidance, and physical symptoms related to their eating disorders. Their regressions revealed that rumination on intrusive thoughts can predict the severity of a person’s eating disorder symptoms and lays a foundation for exploring for how to address various issues in coping with unwanted thoughts, and how to manage unwanted thoughts.
1.6. Mindfulness and Sleep Quality
Findings indicate the hypothesis that mindful emotion regulation is a key process contributing to positive overall physical and mental health as a result of the use of mindfulness techniques [10,15,16,17]. Mindfulness works to target many different outcomes including sleep quality [12]. A study by Greeson et al. (2018) [12] found increased mindfulness was associated with decreased sleep disturbances (r = −0.21, p = 0.004) and improved stress related symptoms (r = −0.38, p < 0.001). Their partial correlations revealed there were changes in pre-post intrusive thoughts and avoidance behaviors, and the changes accounted for up to 32% of the correlation between the change in the use of mindfulness and change in sleep disturbances; it accounted for up to 30% of the correlation between mindfulness change and the change in physical stress symptoms. Their results illustrate the stress reducing effects of mindfulness are due to the improvements in preservative cognition and improvements in emotion regulation, which have been shown to be two cognitive processes that occur across different stress-related disorders [12].
1.7. Mindfulness and Emotion
Arch and Craske (2006) [15] used a mindfulness based breathing induction, and they examined how it would impact participants’ emotional reactions to picture slides. They compared a 15-min recorded mindfulness based induction against a 15-min recorded induction of unfocused attention and worry. The focused breathing induction group maintained positive reactions to the pictures whereas the unfocused group exhibited more worried reactions to the pictures. The focused breathing induction group exhibited lower negative affect and decreased overall emotional volatility to the post induction pictures than the unfocused group. The worry group was seen to have a more overall negative affect, so their findings further suggest that mindfulness can be associated with adaptive responses to an unpleasant emotion.
Garland et al. (2015) [17] examined whether state and practice of mindfulness could help people regulate their emotions more efficiently. They placed participants into one of three groups: (1) mindfulness, (2) suppression, and (3) mind wandering. Participants’ cognitive reappraisal was measured by the Emotion Regulation Questionnaire (ERQ). The participants practiced for a week, and then took the ERQ scale again. Participants in the mindfulness group reported higher levels of state mindfulness than the other two groups. Their path analysis revealed there is an indirect effect between mindfulness and reappraisal by way of state mindfulness. Garland’s finding further suggests repeated mindfulness based stress reduction predicts increases in cognitive reappraisal over time and suggests mindfulness can be associated with improvements in emotion regulation through cognitive reappraisal.
Greeson et al. (2018) [12] conducted an observational study where they examined participants during an eight-week period where they studied rumination, intrusive thoughts, and emotion regulation: measured through avoidance, thought suppression, emotion suppression, and cognitive reappraisal. They predicted mindfulness would positively predict health related outcomes such as sleep quality and stress related symptoms.
Kiken et al. (2015) [16] examined individual paths in state mindfulness during the utilization of mindfulness based stress reduction while relating it to trait mindfulness and distress. They ran an eight-week intervention where participants reported their state mindfulness after meditating. The participants reported pre-intervention and post-intervention measures of trait mindfulness and symptoms of psychological distress, and through the researchers’ latent growth models, they found using mindfulness predicted lower stress levels.
1.8. Emotion Regulation and Sleep
Markarian et al. (2013) [23] examined the relationship between the behavioral activation system and the behavioral inhibition system and linked the relationship to emotion regulation difficulties and sleep quality using structural equation models. They found that emotion regulation difficulties were positively related to anxiety and stress symptoms, and they found differential relationships between emotion regulation difficulties, stress symptoms, and anxiety symptoms among good quality and poor sleep quality sleepers.
Palmer et al. (2018) [1] investigated how sleep problems in adolescence are associated with various emotion regulation strategies utilizing a logistic regression and structural models. They utilized a sample of roughly 10,000 from the United States. Participants were given a pre-screen interview to determine if they qualified for mood or anxiety disorders. Participants provided sleep reports, emotion regulation reports, and reports of their current stress levels. Adolescents who reported lower sleep levels were more likely to report more difficulties in emotion regulation strategies; these individuals who reported lower sleep quality also reported uses of fewer problem solving strategies and greater avoidance, suppression, rumination, and acceptance.
Liu et al. (2018) [28] conducted a study in which they were looking to examine the mediating effects of rumination and the moderating effects of self-control in the association between mindfulness and sleep quality. They sampled 1196 adolescents utilizing self-report measures of mindfulness, rumination, self-control, and sleep quality. Results showed a negative link between mindfulness and poor sleep quality. Mindfulness was negatively associated with rumination and positively associated with poor sleep quality. The results also showed self-control as a moderator between the direct link of mindfulness and poor sleep quality and the indirect link of rumination.
Murnieks et al. (2019) [29] ran two studies where they found sleep and mindfulness exercises both provide ways for entrepreneurs to combat exhaustion. They also found mindfulness and sleep quality influence each other; so as one increases, the effectiveness of the other decreases. Rash et al. (2019) [30] conducted a meta-analysis where they studied mindfulness-based therapies for sleep disturbances. Based on research, they assert that mindfulness-based treatments can influence sleep quality through altering psychological flexibility of a person through variables such as awareness, acceptance, motivation, and change readiness, which are efficient at reducing insomnia’s symptoms and improving adults’ overall sleep quality.
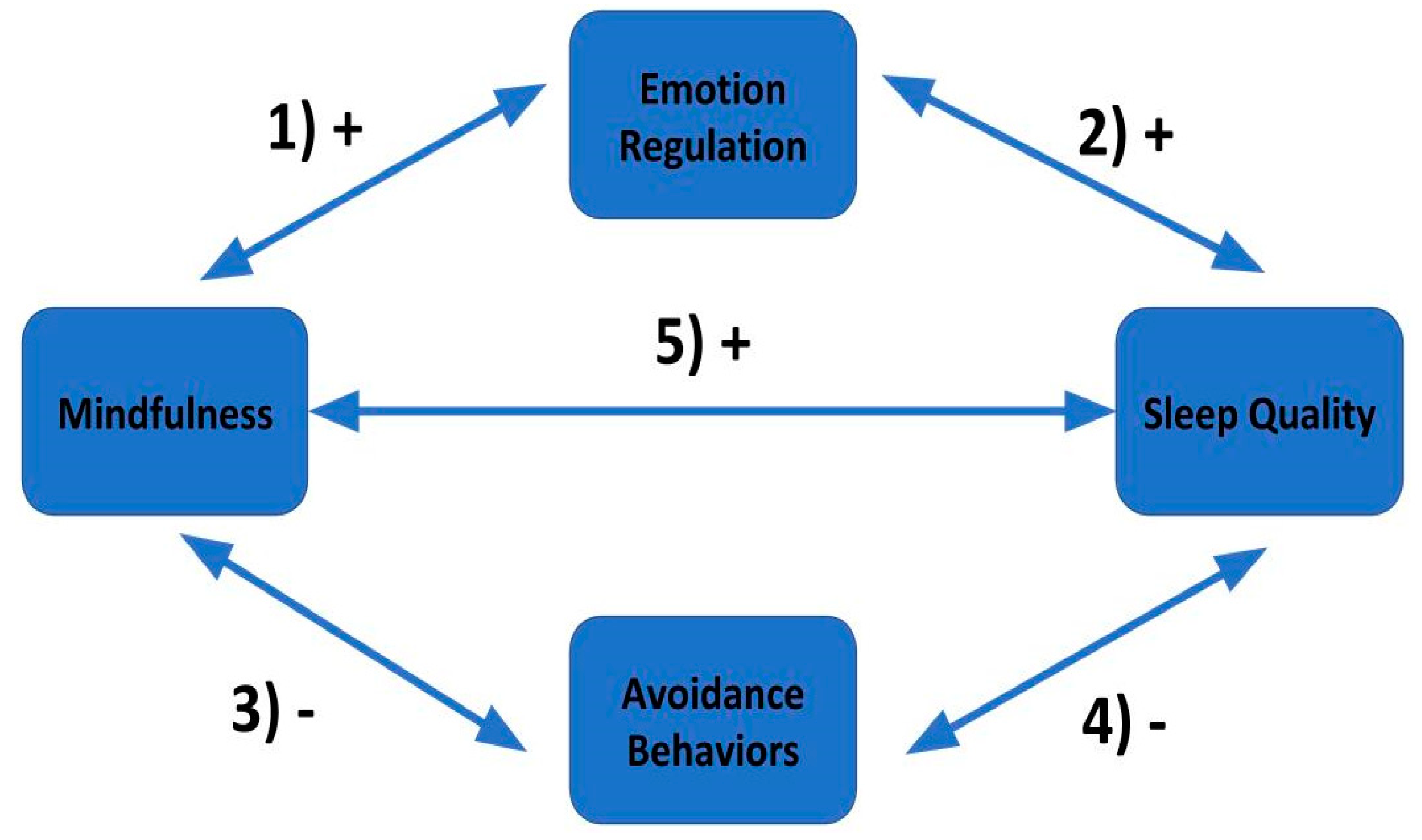
Based on existing theory and prior research discussed, we constructed a hypothetical model to illustrate our hypotheses (see Figure 1).
1.9. Hypotheses
Hypothesis 1: Based on previous findings, we hypothesize that mindfulness, as assessed by the Five Facet Mindfulness Questionnaire (FFMQ) and the Cognitive and Affective Mindfulness Scale (CAMS-R), will positively correlate with reports of healthy emotion regulation as assessed by the ERQ [12,15,16,17].
Hypothesis 2: Based on previous findings, we hypothesize that emotion regulation, as assessed by the ERQ, will positively correlate with overall individual sleep quality, as assessed by the PSQI [1,7,23].
Hypothesis 3: Based on previous findings, we hypothesize mindfulness, as assessed by the FFMQ and CAMS-R, will negatively correlate with reports of intrusive thoughts and avoidance behaviors, as assessed by the Impact of Event Scale (IES) [14,25,26,27].
2. Participants, Materials, and Procedure
2.1. Participants
Our sample included three hundred sixty-seven undergraduates enrolled in various psychology courses at a mid-sized southeastern university in the United States (age M = 19.3 years old, SD = 3.4 years, gender = 73.3% f and 26.7% male). In terms of self-reported ethnicity, 284 were White, 65 were African American/Black, 28 were Asian or Pacific Islander, and 22 reported as “Other” or Did not Report. The majority of our participants (378) reported no current psychiatric diagnoses or medications, with 30 (8.17%) reporting a current diagnosis of Depression and taking a prescription anti-depressant, with only 3 declining to answer. Subjects reported normal or corrected to normal vision and hearing. No female participants reported being pregnant at the time of the survey. Additionally, only 14 (3.8%) reported having been diagnosed with attention deficit disorder as a child.
2.2. Materials
The materials for this study included items from 5 self-report inventories and well as a demographic questionnaire, the results of which are reported above in the Participants section. The inventories were administered using the Qualtrics survey software package and analyzed in IBM SPSS 25, and IBM AMOS 25.
2.2.1. Pittsburgh Sleep Quality Index (PSQI)
The PSQI uses a Likert scale and has 3 parts. The PSQI assesses sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbance, use of sleeping medications, and daytime dysfunction. The PSQI is designed to represent areas examined by clinicians when individuals report with sleep complaints, and it has adequate construct and internal consistency reliability, high correlations have been found [19]. In this study internal consistency was adequate for the PSQI (Cronbach’s α = 0.69) and the ESS (α = 0.70) total scores. PSQI daytime dysfunction and sleep medications components were weakly associated with the total score, but their removal did not notably improve internal consistency. PSQI and ESS totals were associated with each other and with theoretically related variables (i.e., actigraphic variables, depressive symptoms, mobility/instrumental activities of daily living, health-related quality of life) in expected directions. The PSQI differentiated participants reporting no sleep disorder from those reporting particular disorders more reliably than the ESS.
2.2.2. Cognitive and Affective Mindfulness Scale (CAMS-R)
The CAMS-R has 10 items and measures mindfulness, distress, well-being, emotion regulation, and problem solving—where the statements are looking at the constructs of attention: regulating attention so it is focused on immediate experience and the present moment; present focus: openness to the present; awareness: being in the moment; and acceptance: having non-judgment towards experiences. The CAMS-R asks participants to rate their level agreement with 10 items on a Likert scale ranging from 1 (rarely/not at all) to 4 (almost always). The CAMS-R includes statements such as “It is easy for me to concentrate on what I am doing.”; “I try to notice my thoughts without judging them.”; and “I can accept things I cannot change.” The CAMS-R demonstrated quality internal consistency, and there was evidence of convergent and discriminant validity with the measures of mindfulness, distress, well-being, emotion regulation, and problem solving [10]. Cronbach’s alpha was found to be acceptable to good in both the Ch-CAMS-R (0.67) and the CAMSR (0.66).
2.2.3. Five Facet Mindfulness Questionnaire (FFMQ)
The FFMQ has 39 items and measures the constructs of observation, description, awareness, and non-judgment. The FFMQ asks participants to respond to 39 items on a Likert scale ranging from 1 (rarely/not at all) to 5 (very often or always true). The FFMQ includes items such as: “When I’m walking, I deliberately notice the sensations of my body moving.”; “I criticize myself for having irrational or inappropriate emotions.”; and “When I have distressing thoughts or images, I ‘step back’ and am aware of the thought or image without getting taken over by it.” The FFMQ examines the facet structure of the process of mindfulness, so it is specifically looking at the individual sub-components of mindfulness. The FFMQ has been found to yield useful information about the nature of mindfulness and its relation to other variables and constructs. The FFMQ has been found to be well related to and well correlated with the CAMS-R [31]. In this normative study, the internal consistency of each FFMQ factor and for the total scale was in the acceptable range (Observing α = 0.84, Describing α = 0.91, Act with Awareness α = 0.90, Nonjudgment α = 0.93, Nonreactivity α = 0.86, total FFMQ α = 0.93). After controlling for age and education, Act with Awareness (β = −0.28), Nonjudgment (β = −0.27), and Nonreactivity (β = −0.22) were predictive of depression (although statistically significant (p < 0.05), the relationship between Observing and depression symptoms was in the opposite than expected direction (β = 0.10)), and Describing (β = 0.13), Act with Awareness (β = 0.18), Nonjudgment (β = 0.17), and Nonreactivity (β = 0.21) were predictive of satisfaction with life.
2.2.4. Impact of Event Scale (IES-R)
The IES-R has 22 items and measures intrusion, avoidance, and arousal. The IES-R asks participants to respond to a Likert scale from 0 (not at all) to 4 (extremely). The scale includes statements such as: “I had trouble staying asleep.”; “Pictures about it popped into my mind.”; and “Reminders of it caused me to have physical reactions, such as sweating, trouble breathing, nausea, or pounding heart.” The IES-R more effectively assesses the general construct of traumatic stress [32], yet the scale has shown to hold test–retest reliability across trials and remains supported across different magnitudes of various life events [33]. The Impact of IES-R Scale scores are formed for the three subscales, which reflect intrusion (8 items), avoidance (8 items), and hyperarousal (6 items), and show a high degree of intercorrelation (rs = 0.52 to 0.87. High levels of internal consistency have been previously reported (Intrusion: Cronbach’s alpha = 0.87 to 0.94, Avoidance: Cronbach’s alpha = 0.84 to 0.87, Hyperarousal: Cronbach’s alpha = 0.79 to 0.91 [32]. Test–retest reliability, collected across a 6-month interval, ranged from 0.89 to 0.94. We requested for participants to provide us with the date range in which the event occurred.
2.2.5. Emotion Regulation Questionnaire (ERQ)
The ERQ has 10 items and measures the constructs of cognitive reappraisal and emotional suppression. Items 1–6 are target reappraisal, and items 7–10 target suppression. The ERQ asks participants to respond on a Likert scale from 1 (strongly disagree) to 7 (strongly agree). The ERQ includes statements such as “When I want to feel more positive emotion (such as joy or amusement), I change what I’m thinking about.”; “I control my emotions by not expressing them.”; and “I control my emotions by changing the way I think about the situation I’m in.” The ERQ has exhibited strong and sound internal consistency and reliability; it has shown to be stable over a twelve-month period. In all samples, ERQ cognitive reappraisal (α = 0.89–0.90) and expressive suppression (α = 0.76–0.80) scores had acceptable to excellent levels of internal consistency reliability (20). The ERQ has shown consistent construct and convergent validity, and the questionnaire has been a hallmark measure of emotion regulation during several stages of development [8].
2.3. Procedure
The five scales were selected then inserted into Qualtrics. Once the scales were manually inserted into Qualtrics, then the surveys were randomized and linked to SONA Systems. There was a passive online data collection process over a two-month period. The participants completed the surveys on their own time, and the results were immediately posted in Qualtrics once completed. All data were exported from Qualtrics to SPSS, and then analyses were executed using SPSS and SPSS AMOS. A data analysis plan was followed after the completion of the data collection.
The data analysis plan consisted of (1) analysis of data quality where we looked for missing cases, outliers, normality, skewness, and kurtosis (see Table 1); (2) item analysis on a scale by scale basis where we obtained the descriptive statistics of each scale’s individual items (see Appendices A, B, and C); (3) construct analyses to determine whether a particular construct had adequate reliability and validity for use with the current sample; (4) exploratory factor analyses; (5) confirmatory factor analyses; (6) stepwise regression to predict sleep quality; and (7) an A X B test for the mediation of hyperarousal.
3. Results
3.1. Analysis of Data Quality
The raw data was initially problematic, suffering from high amounts of skewness and kurtosis, so in order to normalize our data, we utilized rank ordering and then used the inverse normal transformation function in SPSS. The complete list of normalized descriptives are listed in Table 1 below. When it comes to the average total score of our outcome variable: sleep quality (as assessed by the PSQI), M = 13.80, SE = 0.22.
3.2. Analyses by Construct
An exploratory factor analysis was conducted to assess each construct. We used principal axis factoring, a promax rotation, and a kappa of 4. We then conducted a KMO test of sampling adequacy, obtained a Cronbach’s Alpha, and examined the factor loadings after asking SPSS to suppress eigenvalues below 0.3. Interested readers are referred to Appendix A for the descriptive results by item for the Impact of Events Scale, Five Facet Mindfulness Questionnaire, and the Emotion Regulation Questionnaire, respectively.
3.2.1. CAMS-R Exploratory Factor Analysis
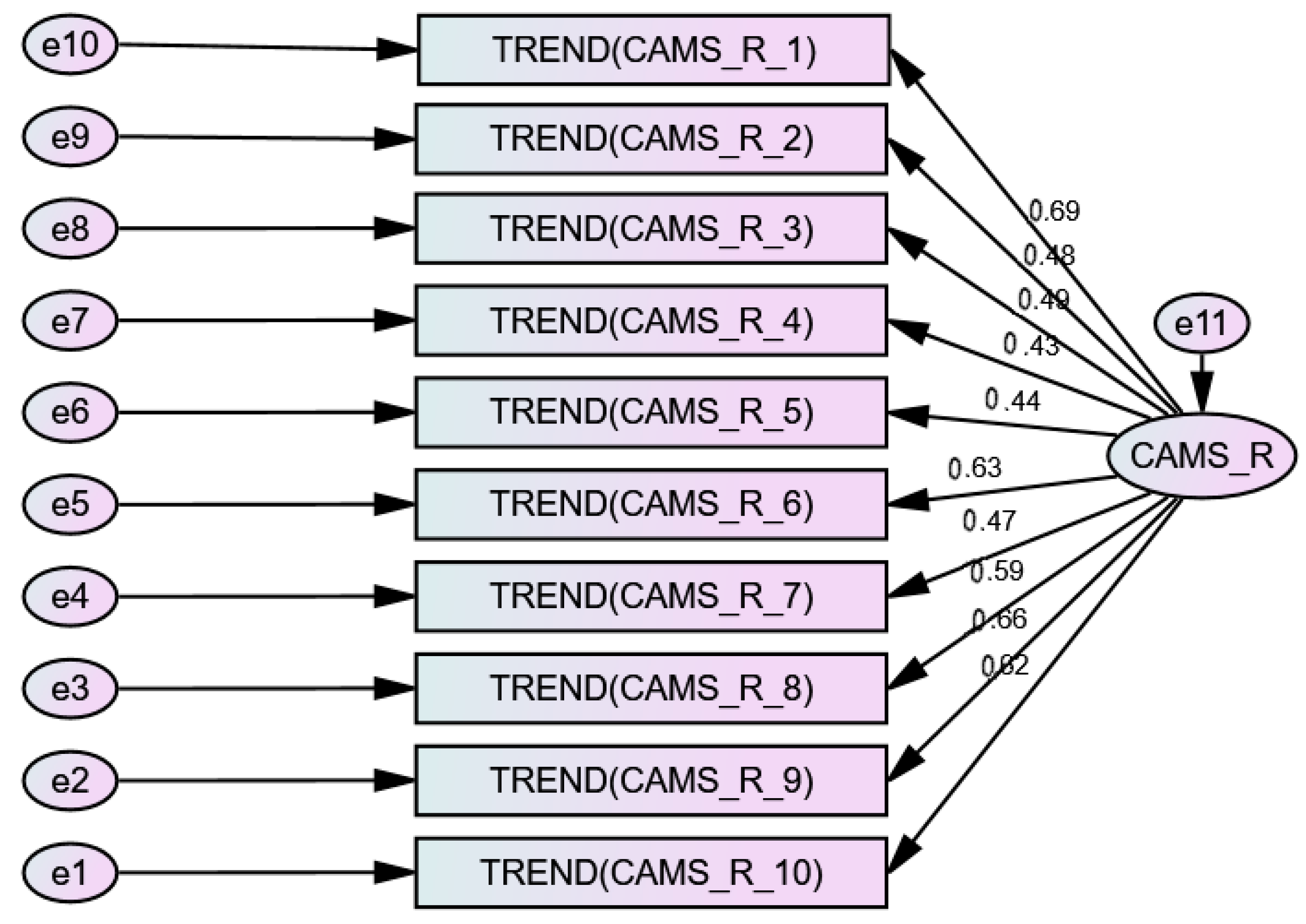
We conducted a Kaiser–Meyer–Olkin Measure Test of Sampling Adequacy which yielded a KMO = 0.825 We then ran a Cronbach’s alpha test of reliability, which yielded a value of 0.807. The total variance of the CAMS-R was explained by three factors, with 37.53% of the total scale variance being accounted for by factor 1. We then conducted a confirmatory factor analysis using SPSS AMOS to test two models of the CAMS-R items. Model one was a three factor solution, which yielded a chi-squared (35) of 248.893, p < 0.001. Rejecting this null hypothesis is problematic, as it reflects (1) the data contain covariance information that speak against the three factor model, and (2) the researcher should explain model-data discrepancies that exceed those expected by sampling error. The goodness of fit index (GFI) value was 0.867 (>0.95 is ideal), and the root-mean-squared error of approximation (RMSEA) was 0.129 (with <0.05 being ideal), indicating that the model could and should be improved. We then attempted to fit a one factor model, and it performed better, although not perfectly. The chi-squared value was better at, chi-squared (29) = 82.895, p < 0.001. The GFI was superior at 0.957, and the RMSEA was at a more manageable 0.07. Modification indices were added to the model only when they improved model fit, and for neighboring items that clearly could share covariance based upon their item wording. This model is shown below in Figure 2. (Exploratory Factor Analysis (EFA) is a statistical approach for determining the correlation among the variables in a dataset. This type of analysis provides a factor structure (a grouping of variables based on strong correlations). In general, an EFA prepares the variables to be used for cleaner structural equation modeling. An EFA should always be conducted for new datasets. The beauty of an EFA over a CFA (confirmatory) is that no a priori theory about which items belong to which constructs is applied. This means the EFA will be able to spot problematic variables much more easily than the CFA [34].)
3.2.2. IES Exploratory Factor Analysis
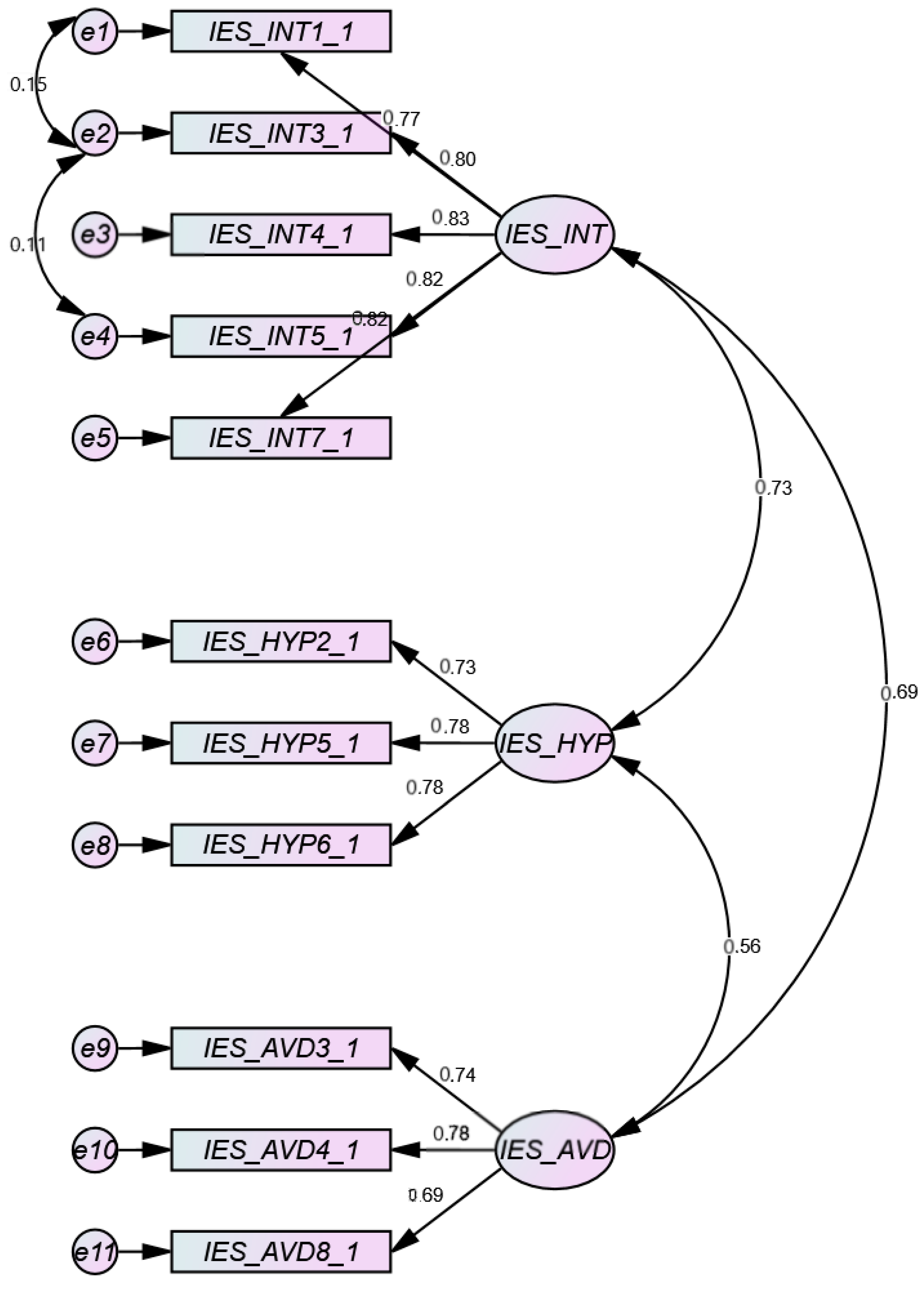
We conducted a Kaiser–Meyer–Olkin measure test of sampling adequacy which yielded a KMO = 0.945. We then ran a Cronbach’s alpha test of reliability, which yielded a value of 0.939 indicating high scale reliability. The total variance of the IES was explained by three total factors, with 45.21% of the total scale variance being accounted for by factor 1. We then conducted a Confirmatory Factor Analysis using SPSS AMOS to test two models of the IES items. The constructed model produced a three factor solution, which yielded a chi-squared (39) of 45.183, p = 0.229. The goodness of fit index (GFI) value was 0.978 (>0.95 is ideal), and the root-mean-squared error of approximation (RMSEA) was 0.021 (with <0.05 being ideal), indicating that the model fits really well. This model is shown below in Figure 3.
3.2.3. FFMQ Exploratory Factor Analysis
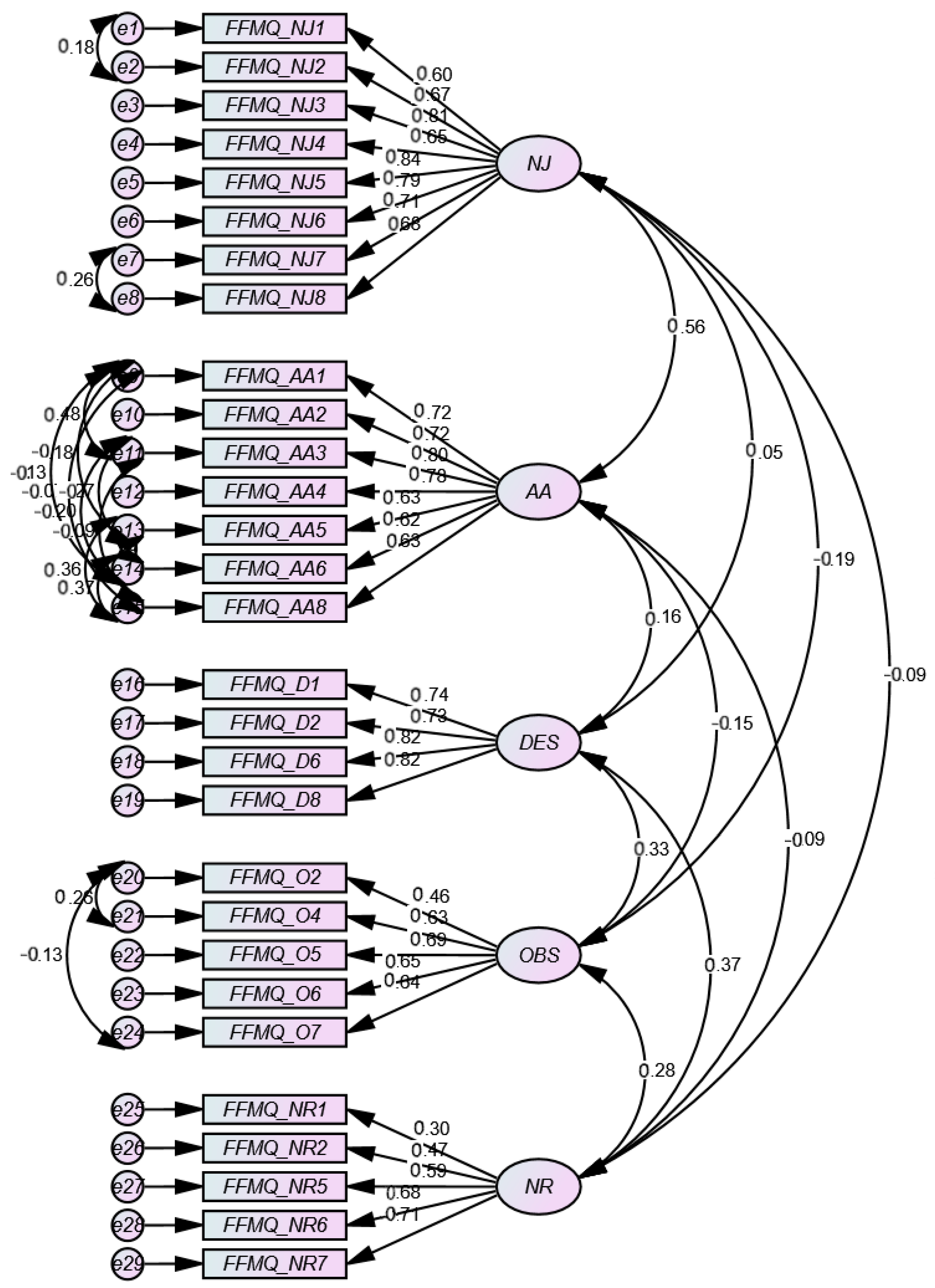
We conducted a Kaiser–Meyer–Olkin measure test of sampling adequacy which yielded KMO = 0.873. We then ran a Cronbach’s alpha test of reliability, which yielded a value of 0.845 indicating high reliability. The total variance of the FFMQ was explained by five total factors, with 13.55% of the total scale variance being accounted for by factor 2. We then conducted a confirmatory factor analysis using SPSS AMOS to test a model of the FFMQ items. The constructed model produced a five factor solution, which yielded a chi-squared (353) of 621.570, p < 0.001. The goodness of fit index (GFI) value was 0.901 (>0.95 is ideal), and the root-mean-squared error of approximation (RMSEA) was 0.046 (with <0.05 being ideal), indicating that the model fits well. This model is shown below in Figure 4.
3.2.4. ERQ Exploratory Factor Analysis
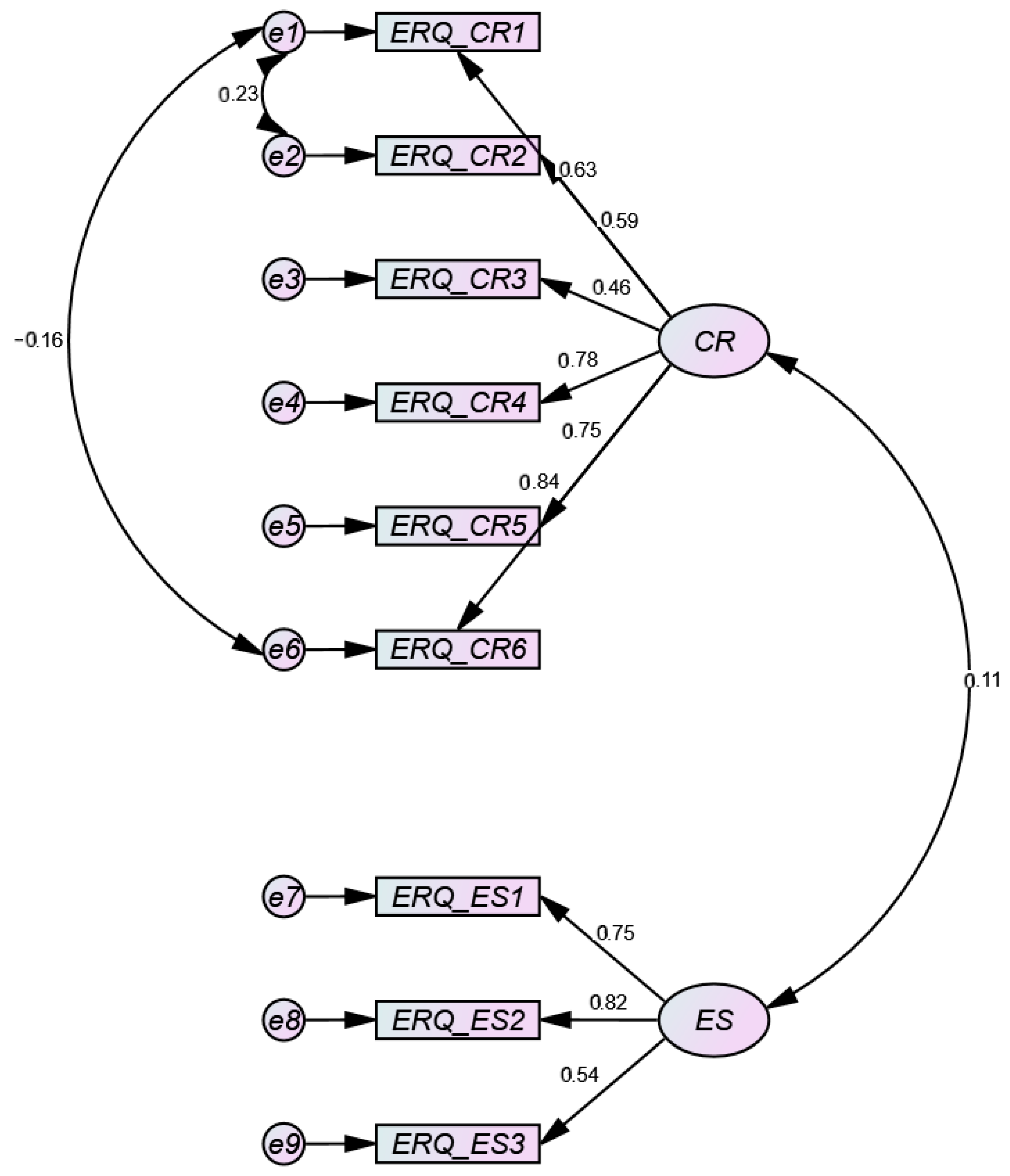
We conducted a Kaiser–Meyer–Olkin measure test of sampling adequacy, which yielded a KMO = 0.815. We then ran a Bartlett’s test of sphericity, which yielded p = 0.000, Cronbach’s alpha test of reliability yielded a value of 0.757 indicating moderately high reliability. The total variance of the ERQ was explained by two total factors, with 38.10% of the total scale variance being accounted for by factor 1. We then conducted a confirmatory factor analysis using SPSS AMOS to test a model of the ERQ items. The constructed model produced a two factor solution, which yielded a chi-squared (24) of 24.205, p = 0.450. The goodness of fit index (GFI) value was 0.986 (>0.95 is ideal), and the root-mean-squared error of approximation (RMSEA) was 0.005 (with <0.05 being ideal), indicating that the model fits well. This model is shown below in Figure 5.
3.2.5. Total Variance
The three variables that contributed to the most scale variance were hyperarousal from the IES, acting with awareness from the FFMQ, and non-reaction from the FFMQ. Together, the participants’ emotional experiences and mindfulness contributed to 26.3% of the total variance.
3.2.6. Correlational Analyses
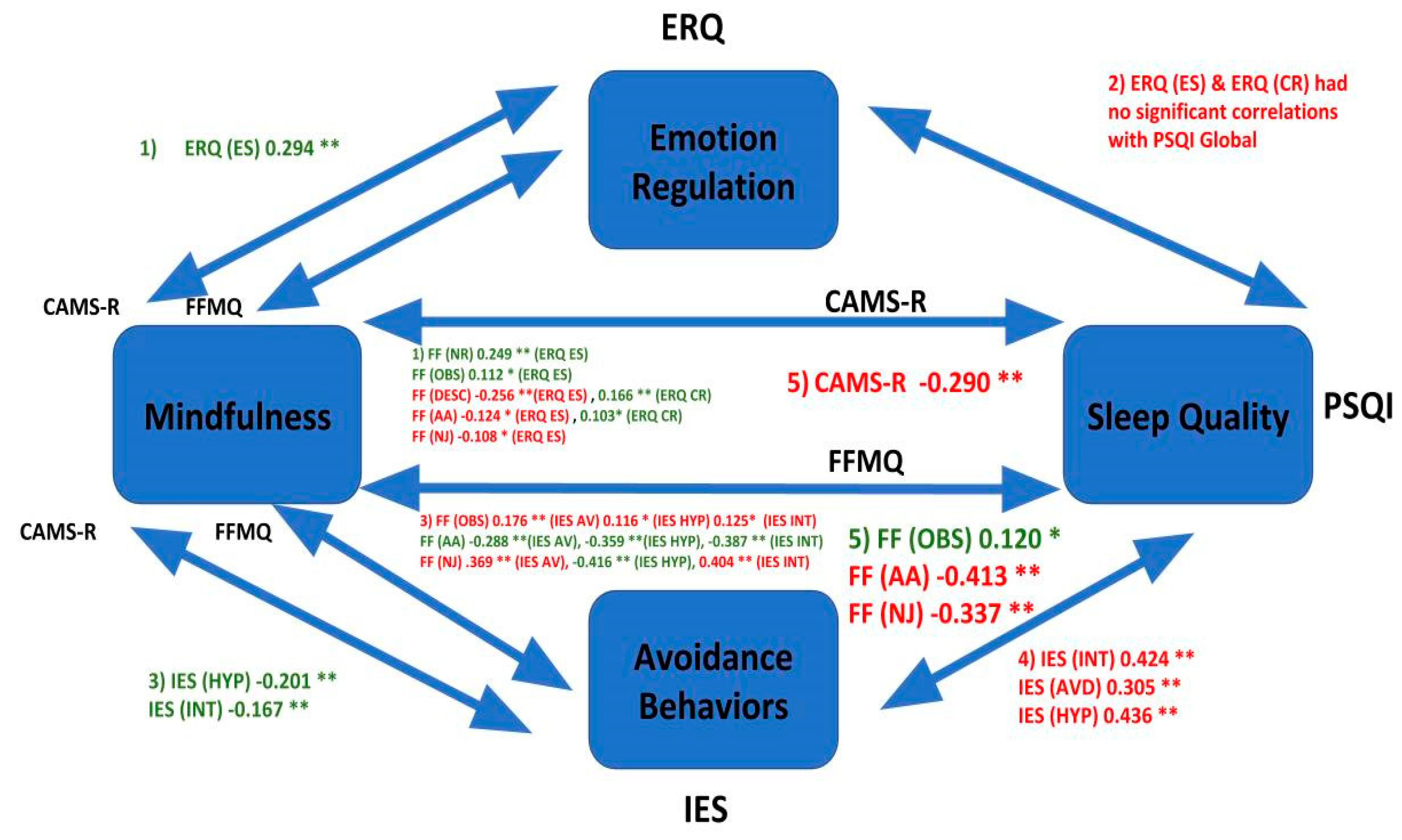
All of the scales correlated well within their own constructs, but when we correlated the scales with one another the scales did not correlate well. Our analyses revealed only moderately significant correlations between the IES subscales of intrusive thoughts, avoidance, and hyperarousal and participants’ global reported scores on the PSQI (see Table 2). Correlations were moderately positive among all three constructs on the IES and the PSQI global score: intrusive thoughts r(367) = 0.424, p < 0.01, avoidance r(367) = 0.305, p < 0.01, hyperarousal r(367) = 0.436, p < 0.01 (see Table 2). Intrusive thoughts, avoidance, and hyperarousal are contributing to much of the relationship between experiencing a stressful event and an individual’s sleep quality. The correlational findings, by hypothesis, are listed in Figure 6 (below). This figure should be compared to Figure 1 that lists the original hypotheses. The results in the Figure that appear in green are congruent with the hypotheses from Figure 1, whereas the hypotheses in red are incongruent with the initial hypotheses.
3.2.7. Stepwise Regression
We conducted a stepwise regression to predict sleep quality using several predictors that emerged well from the correlational analyses. We used variables that were significantly correlated with PSQI, all having correlation coefficients of 0.28 or higher. The variables included were CAMS-R total Score, the IES Avoidance, Intrusiveness, and Hyperarousal subscale, as well as the Act with Awareness and Non-judging subscales from the FFMQ. A stepwise procedure was utilized, with a requirement for probability of F less than 0.05 to enter, and greater than or equal to 0.1 to remove a candidate variable from the model. Three steps were produced, with the first including only the variable of hyperarousal from the IES. The IES accounted for 18.8% of the variance in PSQI (R2 adjusted). See Table 3 below for the model summary. The second step of the model introduced the Act with Awareness subscale of the FFMQ, which added 7.65 additional explained variance, and finally step 3 introduced the CAMS-R total score to the model, explaining an additional 0.9% of the variance. The total amount of variance explained by the model was 26.9%, using the adjusted r squared value, f(3, 363) = 45.822, p < 0.001, as shown in Table 4 below. Table 5 (below) displays the Coefficients of the Regression Model.
3.2.8. Hyperarousal as a Mediator
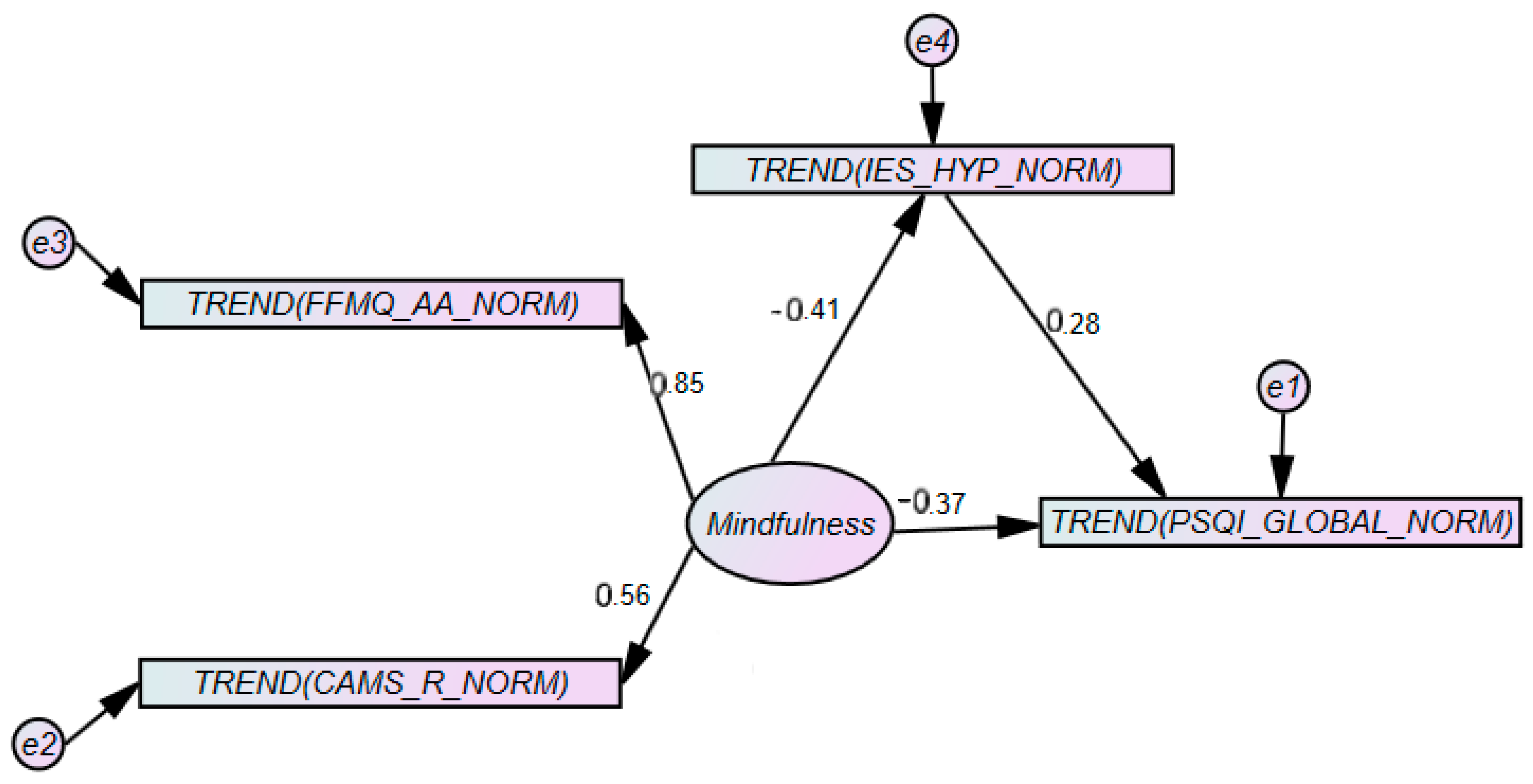
The finding of three variables that explained significant variance in sleep quality lead to the modification of our initial model as presented above. A simplified structural model was constructed and tested using the IES Hyperarousal (HYP) scale, the FFMQ Act with Awareness Scale (AA), the PSQI, and the CAMS-R. Based on the literature reviewed above, we tested two models: (1) that Mindfulness, a latent construct modeled as explaining both the CAMS-R and FFMQ’s AA, would contribute to the PSQI directly; and that the relationship between Mindfulness and PSQI would be mediated by IES (HYP). The values from the first model are seen below in Figure 7. This simple model yielded a small chi-square indicating preliminary evidence the model is less likely to contain covariance information not supported by the model, chi-square (1) = 1.160, p = 0.281. The resulting model yielded good fit as indicated by a cmin/df of 1.160, a comparative fit index (CFI) of 0.999, a goodness of fit index (GFI) of 0.998, an adjusted goodness of fit index (AGFI) of 0.984, and root mean square residual (RMR) of 0.011, and a root mean square error of approximation (RMSEA) of 0.021.
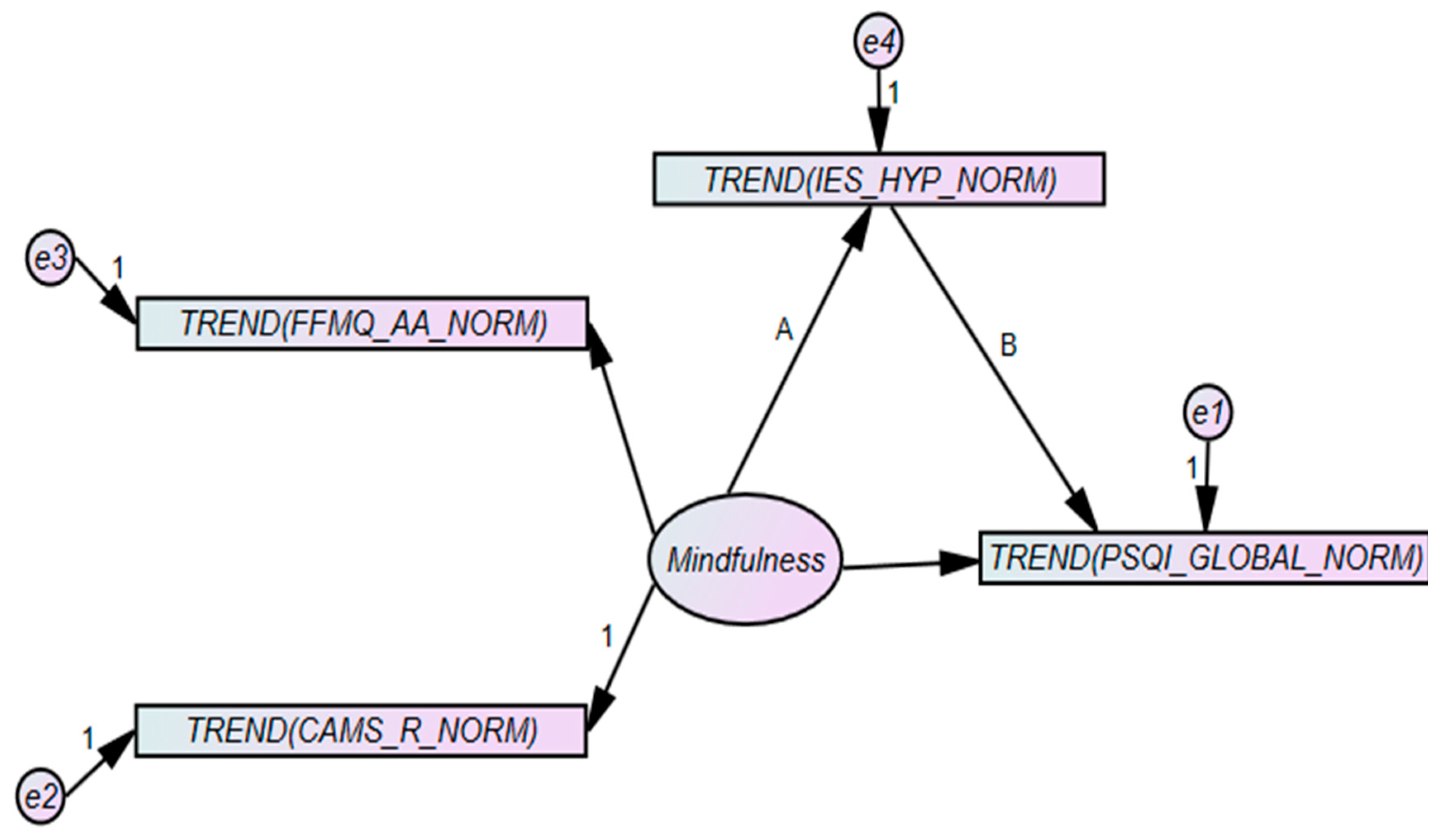
We conducted a test of the mediation effect using bootstrapping to create bias-corrected 95% confidence intervals, which yielded a standardized indirect effect (A × B) of −2.105, p = 0.001, indicating a significant mediation effect of hyperarousal on the relationship between mindfulness and the PSQI (See Figure 8).
4. Discussion
The purpose of the current study was to extend the existing literature and assess the factors contributing to a person’s sleep quality, and based on existing theory, we constructed five different hypotheses. To revisit the hypotheses, (1) we hypothesized mindfulness, as assessed by the FFMQ and the CAMS-R, would positively correlate with reports of healthy emotion regulation as assessed by the ERQ [12,15,16,17]. (2) Emotion regulation, as assessed by the ERQ, would positively correlate with overall individual sleep quality, as assessed by the PSQI [1,7,23]. (3) Mindfulness, as assessed by the FFMQ and CAMS-R, would negatively correlate with reports of intrusive thoughts and avoidance behaviors, as assessed by the IES [14,25,26,27]. (4) Reports of intrusive thoughts and avoidance behaviors, as assessed by the IES, would negatively correlate with overall individual sleep quality, as assessed by the PSQI [1,7,23]. (5) Mindfulness, as assessed by the FFMQ and CAMS-R, would positively correlate with overall individual sleep quality, as assessed by the PSQI [28,29,30].
The current study was a cross-sectional survey, so our conclusions are strictly correlational. We found that no single finding completely agreed with our original five hypotheses, but rather most of our findings partially agreed with our hypotheses. A potential reason why this partial disagreement occurred is because we partitioned the scales into their sub-constructs and correlated them separately; we did not look at the scales holistically. The only scales we looked at holistically were the CAMS-R and the PSQI. Hypothesis 4 turned out to be the complete opposite of what we had expected, but after we looked at the IES and PSQI again, we found that higher scores on the IES and PSQI denoted worse outcomes; so in hindsight, it makes sense as to why the scores from the IES and PSQI positively correlated with one another.
First, when it comes to the correlation between mindfulness and emotion regulation: The CAMS-R was weakly positively correlated with the ERQ’s emotional suppression (ES) subscale. The FFMQ’s non-reacting (NR) and observing (OBS) subscales were weakly positively correlated with the ES subscale of the ERQ. The describe (DESC), acting with awareness (AA), and non-judging (NJ) subscales of the FFMQ were weakly negatively correlated with the ES subscale of the ERQ. The FFMQ (DESC and AA) was weakly positively correlated with cognitive reappraisal (CR) from the ERQ.
Next, when it comes to the correlation between emotion regulation and sleep quality, there were no significant correlations between the ES and CR subscales of the ERQ and the PSQI. Third, when it comes to the correlation between mindfulness (as assessed by the CAMS-R and the FFMQ) and the IES: the hyperarousal (HYP) and intrusive thoughts (INT) subscales of the IES were weakly negatively correlated with the CAMS-R. The FFMQ (OBS) was found to be negatively correlated with IES (INT, AVD, and HYP). The FFMQ (AA) was negatively correlated with all three subscales of the IES, and the FFMQ (NJ) was found to be positively correlated with IES (AVD and INT), but negatively correlated with the IES (HYP).
Furthermore, the FFMQ (AA) was found to be negatively correlated with all three subscales of the IES (INT, AVD, and HYP). The FFMQ (OBS) was positively correlated with the PSQI, whereas AA and NJ were found to be negatively correlated with the PSQI. Lastly, when it comes to the correlation between mindfulness (as assessed by the CAMS-R and the FFMQ) and sleep quality (as assessed by the PSQI)—which was the main outcome we were interested in: we found the CAMS-R to be negatively correlated with the PSQI, and the FFMQ (OBS, AA, and NJ) was found to be negatively correlated with the PSQI, yet it is important to note the other subscales of the FFMQ (NR and DESC) were not found to be significantly correlated with the PSQI global score.
The results of the current study suggest intrusion, avoidance, and hyperarousal correlate with a person’s overall sleep quality [24]; however, our results suggest mindfulness is correlated with decreases in sleep disturbances and improvements in a person’s sleep quality through acting with awareness and being non-judgmental towards oneself following the experience of an event [28,29,30]. Our findings further suggest mindfulness is positively correlated with sleep quality by altering a person’s psychological flexibility through variables such as: awareness—through the process of accepting present feelings in a non-judgmental way [30]. If a person is trying to block out hyperarousal while falling asleep, then using mindfulness traits such as acting with awareness may help, but further research is needed in order for our results to gain support. The results of the current study agree with the literature suggesting the use of various mindfulness techniques are positively linked to a person’s sleep quality when hyperaroused; thus, further suggesting mindfulness correlates with reduced hyperarousal and faster sleep onsets [1,12,23,28,29,30].
Given our findings that hyperarousal mediated the relationship between mindfulness (as assessed by the CAMS-R and the FFMQ) and sleep quality (as assessed by the PSQI), our results agree with the prior findings suggesting that poor sleep quality is related to poor methods of regulating emotions and that hyperarousal contributes to a high amount of variance when examining the relationship between the constructs of mindfulness, emotion regulation, and sleep quality [12,18,24]. Although our results are promising, further research is needed to strengthen the findings of the current study.
There were a few limitations to the current study, which included (1) an overwhelmingly female sample; and (2) there was an accidental omission of one question from the ERQ, which unbalanced the number of intended cognitive reappraisal and emotional suppression items, which consequently could have played a minor role in how the measure performed overall. It is still unclear in our results if there are true gender differences in how mindfulness techniques improve sleep quality as our sample was overwhelmingly female, and because gender differences were not a focus of our study. When it comes to future directions, our results point us towards revisiting our theoretical model and using the model as the basis of future studies.
For future studies, we can use the same participants and record their responses to the measures over three different time periods, and we could look to see if there is a significant difference in how the participants respond. Once a stronger theoretical framework is established in the literature, other future directions could include (1) obtaining a more even sample of males and females—focusing on gender differences; (2) using different mindfulness scales to see if the measures continue to predict sleep quality; (3) using a different emotion regulation scale because the ERQ did not perform as well as we anticipated; and (4) sampling from an older population of people to examine whether or not our results will generalize to different age groups—as our sample was university undergraduates.
5. Conclusions
Although our findings were not exactly as we predicted, our findings help close the gap in the current literature regarding how mindfulness correlates with sleep quality, and our findings help explain factors that predict the variability in sleep quality, such as a person’s total score on the CAMS-R; their frequency of reporting intrusive thoughts, avoidance, and hyperarousal on the IES; and their frequency of reporting acting with awareness, non-judgment, and non-reaction on the FFMQ. Mindfulness-based interventions have been efficacious at reducing the symptoms of insomnia and improving sleep quality among adults when compared with psychological placebos and waitlist control conditions [30]. Rash and colleagues, however, point to the need for research that evaluates mediators and moderators of intervention effects in an attempt to identify empirically supported processes of change linking mindfulness-bases interventions and sleep outcomes. The current research furthers this objective by identifying hyperarousal as a key contributor and showing that aspects of mindfulness moderate the relationship between hyperarousal and sleep quality. One possible clinical implication of this work is that in order to be effective, mindfulness-based interventions that emphasize acting with awareness and affective regulation must deal with physiological hyperarousal first and foremost before attempting to move into cognitive mindfulness exercises. One form that this might take would the integration of exercise therapies to the standard talk therapy of mindfulness-based treatment for Insomnia [35]. The efficacy of yoga-based therapies is promising, as reviewed by Mustian and colleagues [36]. Further research should be conducted to determine which therapies are most effective at reducing hyperarousal and preventing the recurrence of hyperarousal in patients with insomnia.
Author Contributions
Conceptualization, G.T. and J.S.-T.; methodology, G.T. and J.S.-T.; software, J.S.-T.; validation, J.S.-T.; formal analysis, G.T. and J.S.-T.; investigation, G.T.; resources, J.S.-T.; data curation, J.S.-T.; writing—original draft preparation, G.T.; writing—review and editing, G.T. and J.S.-T.; visualization, G.T. and J.S.-T.; supervision, J.S.-T.; project administration, G.T.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table A1.
Descriptives of the Impact of Event Scale.
| Descriptive Statistics | |||||
|---|---|---|---|---|---|
| N | Minimum | Maximum | Mean | Std. Deviation | |
| Any reminder brought back feelings about it. | 367 | 1 | 5 | 3.08 | 1.247 |
| I had trouble staying asleep. | 366 | 1 | 5 | 2.38 | 1.349 |
| Other things kept making me think about it. | 366 | 1 | 5 | 2.88 | 1.261 |
| I felt irritable and angry. | 367 | 1 | 5 | 2.65 | 1.391 |
| I avoided letting myself get upset when I thought about it or was reminded of it. | 367 | 1 | 5 | 2.81 | 1.221 |
| I thought about it when I didn’t mean to. | 367 | 1 | 5 | 3.16 | 1.271 |
| I felt as if it didn’t happen or wasn’t real. | 366 | 1 | 5 | 2.34 | 1.416 |
| I stayed away from reminders of it. | 364 | 1 | 5 | 2.89 | 1.383 |
| Pictures about it popped into my mind. | 367 | 1 | 5 | 3.02 | 1.378 |
| I was jumpy or easily startled. | 366 | 1 | 5 | 2.02 | 1.294 |
| I tried not to think about it. | 366 | 1 | 5 | 3.37 | 1.334 |
| I was aware that I still had lots of feelings about it, but I didn’t deal with them. | 365 | 1 | 5 | 3.04 | 1.41 |
| My feelings about it were kind of numb. | 367 | 1 | 5 | 2.65 | 1.361 |
| I found myself acting or feeling like I was back at the time. | 366 | 1 | 5 | 2.33 | 1.279 |
| I had trouble falling asleep. | 367 | 1 | 5 | 2.45 | 1.449 |
| I had waves of strong feelings about it. | 366 | 1 | 5 | 2.97 | 1.456 |
| I tried to remove it from my memory. | 367 | 1 | 5 | 2.78 | 1.513 |
| I had trouble concentrating. | 367 | 1 | 5 | 2.63 | 1.375 |
| Reminders of it caused me to have physical reactions, such as sweating, trouble breathing, nausea, or pounding heart. | 364 | 1 | 5 | 2.19 | 1.448 |
| I had dreams about it. | 366 | 1 | 5 | 2.5 | 1.524 |
| I felt watchful and on-guard. | 366 | 1 | 5 | 2.31 | 1.398 |
| I tried not to talk about it. | 366 | 1 | 5 | 2.98 | 1.474 |
| Valid N (listwise) | 353 |
Table A2.
Descriptives of the Five Facet Mindfulness Questionnaire.
| Descriptive Statistics | |||||
|---|---|---|---|---|---|
| N | Minimum | Maximum | Mean | Std. Deviation | |
| When I’m walking, I deliberately notice the sensations of my body moving. | 367 | 1 | 5 | 2.49 | 1.096 |
| I’m good at finding words to describe my feelings. | 367 | 1 | 5 | 2.9 | 1.14 |
| I criticize myself for having irrational or inappropriate emotions. | 367 | 1 | 5 | 2.97 | 1.23 |
| I perceive my feelings and emotions without having to react to them. | 366 | 1 | 5 | 2.88 | 0.988 |
| When I do things, my mind wanders off and I’m easily distracted. | 367 | 1 | 5 | 2.74 | 1.156 |
| When I take a shower or bath, I stay alert to the sensations of water on my body. | 364 | 1 | 5 | 2.87 | 1.261 |
| I can easily put my beliefs, opinions, and expectations into words. | 365 | 1 | 5 | 3.14 | 1.122 |
| I don’t pay attention to what I’m doing because I’m daydreaming, worrying, or otherwise distracted. | 366 | 1 | 5 | 3.17 | 1.193 |
| I watch my feelings without getting lost in them. | 367 | 1 | 5 | 2.78 | 1.017 |
| I tell myself I shouldn’t be feeling the way I’m feeling. | 363 | 1 | 5 | 2.85 | 1.255 |
| I notice how foods and drinks affect my thoughts, bodily sensations, and emotions. | 367 | 1 | 5 | 2.86 | 1.34 |
| It’s hard for me to find the words to describe what I’m thinking. | 367 | 1 | 5 | 3.18 | 1.212 |
| I am easily distracted. | 367 | 1 | 5 | 2.85 | 1.257 |
| I believe some of my thoughts are abnormal or bad and I shouldn’t think that way. | 364 | 1 | 5 | 3.25 | 1.307 |
| I pay attention to sensations, such as the wind in my hair or sun on my face. | 367 | 1 | 5 | 3.06 | 1.256 |
| I have trouble thinking of the right words to express how I feel about things. | 367 | 1 | 5 | 3.16 | 1.156 |
| I make judgments about whether my thoughts are good or bad. | 366 | 1 | 5 | 2.79 | 1.123 |
| I find it difficult to stay focused on what’s happening in the present. | 366 | 1 | 5 | 3.27 | 1.201 |
| When I have distressing thoughts or images, I “step back” and am aware of the thought or image without getting taken over by it. | 366 | 1 | 5 | 2.84 | 1.138 |
| I pay attention to sounds, such as clocks ticking, birds chirping, or cars passing. | 365 | 1 | 5 | 3.04 | 1.332 |
| In difficult situations, I can pause without immediately reacting. | 364 | 1 | 5 | 2.9 | 1.12 |
| When I have a sensation in my body, it’s difficult for me to describe it because I can’t find the right words. | 366 | 1 | 5 | 3.49 | 1.102 |
| It seems I am “running on automatic” without much awareness of what I’m doing | 364 | 1 | 5 | 3.19 | 1.262 |
| When I have distressing thoughts or images, I feel calm soon after. | 366 | 1 | 5 | 2.46 | 1.074 |
| I tell myself that I shouldn’t be thinking the way I’m thinking. | 365 | 1 | 5 | 3.11 | 1.262 |
| I notice the smells and aromas of things. | 365 | 1 | 5 | 3.42 | 1.178 |
| Even when I’m feeling terribly upset, I can find a way to put it into words. | 363 | 1 | 5 | 2.8 | 1.146 |
| I rush through activities without being really attentive to them. | 366 | 1 | 5 | 3.36 | 1.084 |
| When I have distressing thoughts or images I am able just to notice them without reacting | 366 | 1 | 5 | 2.68 | 1.023 |
| I think some of my emotions are bad or inappropriate and I shouldn’t feel them. | 364 | 1 | 5 | 3.33 | 1.262 |
| I notice visual elements in art or nature, such as colors, shapes, textures, or patterns of light and shadow. | 365 | 1 | 5 | 3.11 | 1.25 |
| My natural tendency is to put my experiences into words. | 365 | 1 | 5 | 2.77 | 1.234 |
| When I have distressing thoughts or images, I just notice them and let them go. | 366 | 1 | 5 | 2.66 | 1.083 |
| I do jobs or tasks automatically without being aware of what I’m doing. | 364 | 1 | 5 | 3.2 | 1.152 |
| When I have distressing thoughts or images, I judge myself as good or bad, depending what the thought/image is about. | 366 | 1 | 5 | 3.26 | 1.225 |
| I pay attention to how my emotions affect my thoughts and behavior. | 364 | 1 | 5 | 3.34 | 1.106 |
| I can usually describe how I feel at the moment in considerable detail. | 366 | 1 | 5 | 2.87 | 1.155 |
| I find myself doing things without paying attention. | 366 | 1 | 5 | 3.09 | 1.149 |
| I disapprove of myself when I have irrational ideas. | 365 | 1 | 5 | 3.25 | 1.222 |
| Valid N (listwise) | 336 |
Table A3.
Descriptives of the Emotion Regulation Questionnaire.
| Descriptive Statistics | |||||
|---|---|---|---|---|---|
| N | Minimum | Maximum | Mean | Std. Deviation | |
| When I want to feel more positive emotion (such as joy or amusement), I change what I’m thinking about. | 366 | 2 | 7 | 5.3333 | 1.25331 |
| I keep my emotions to myself. | 364 | 1 | 7 | 4.5769 | 1.74619 |
| When I want to feel less negative emotions (such as sadness or anger), I change what I’m thinking about. | 361 | 1 | 7 | 5.0277 | 1.52727 |
| When I’m faced with a stressful situation, I make myself think about it in a way that helps me stay calm. | 361 | 1 | 7 | 4.7535 | 1.63389 |
| I control my emotions by not expressing them. | 355 | 1 | 7 | 4.0282 | 1.94393 |
| When I want to feel more positive emotion, I change the way I’m thinking about the situation. | 364 | 1 | 7 | 5.0714 | 1.46788 |
| I control my emotions by changing the way I think about the situation I’m in. | 362 | 1 | 7 | 4.7541 | 1.53186 |
| When I am feeling negative emotions, I make sure not to express them. | 359 | 1 | 7 | 3.8552 | 1.85544 |
| When I want to feel less negative emotion, I change the way I’m thinking about the situation. | 363 | 1 | 7 | 4.8209 | 1.54434 |
| Valid N (listwise) | 337 |
References
- Palmer, C.A.; Oosterhoff, B.; Bower, J.L.; Kaplow, J.B.; Alfano, C.A. Associations among adolescent sleep problems, emotion regulation, and affective disorders: Findings from a nationally representative sample. J. Psychiatr. Res. 2018, 96, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Backhaus, J.; Junghanns, K. Daytime naps improve procedural motor memory. Sleep Med. 2006, 7, 508–512. [Google Scholar] [CrossRef]
- Debarnot, U.; Castellani, E.; Valenza, G.; Sebastiani, L.; Guillot, A. Daytime naps improve motor imagery learning. Cogn. Affect. Behav. Neurosci. 2011, 11, 541–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doran, S.M.; Van Dongen, H.P.A.; Dinges, D.F. Sustained attention performance during sleep deprivation: Evidence of state instability. Arch. Ital. De Biol. 2001, 139, 253–267. [Google Scholar]
- Lo, J.C.; Groeger, J.A.; Santhi, N.; Arbon, E.L.; Lazar, A.S.; Hasan, S.; von Schantz, M.; Archer, S.N.; Dijk, D.-J. Effects of Partial and Acute Total Sleep Deprivation on Performance across Cognitive Domains, Individuals and Circadian Phase. PLoS ONE 2012, 7, e45987. [Google Scholar] [CrossRef] [Green Version]
- MacDonald, K.J.; Lockhart, H.A.; Storace, A.C.; Emrich, S.M.; Cote, K.A. A daytime nap enhances visual working memory performance and alters event-related delay activity. Cogn. Affect. Behav. Neurosci. 2018, 18, 1105–1120. [Google Scholar] [CrossRef]
- Palmer, C.A.; Alfano, C.A. Sleep and emotion regulation: An organizing, integrative review. Sleep Med. Rev. 2017, 31, 6–16. [Google Scholar] [CrossRef] [PubMed]
- Gullone, E.; Taffe, J. The Emotion Regulation Questionnaire for Children and Adolescents (ERQ–CA): A psychometric evaluation. Psychol. Assess. 2012, 24, 409–417. [Google Scholar] [CrossRef]
- Thompson, R.A. Emotion Regulation: A theme in Search of Definition. Monogr. Soc. Res. Child. Dev. 1994, 59, 25–52. [Google Scholar] [CrossRef]
- Feldman, G.; Hayes, A.; Kumar, S.; Greeson, J.; Laurenceau, J.-P. Mindfulness and Emotion Regulation: The Development and Initial Validation of the Cognitive and Affective Mindfulness Scale-Revised (CAMS-R). J. Psychopathol. Behav. Assess. 2007, 29, 177–190. [Google Scholar] [CrossRef]
- Gross, J.J.; John, O.P. Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. J. Personal. Soc. Psychol. 2003, 85, 348–362. [Google Scholar] [CrossRef] [PubMed]
- Greeson, J.M.; Zarrin, H.; Smoski, M.J.; Brantley, J.G.; Lynch, T.R.; Webber, D.M.; Hall, M.H.; Suarez, E.C.; Wolever, R.Q. Mindfulness Meditation Targets Transdiagnostic Symptoms Implicated in Stress-Related Disorders: Understanding Relationships between Changes in Mindfulness, Sleep Quality, and Physical Symptoms. Evid. Based Complementary Altern. Med. 2018, 2018, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lutz, J.; Herwig, U.; Opialla, S.; Hittmeyer, A.; Jäncke, L.; Rufer, M.; Grosse Holtforth, M.; Brühl, A.B. Mindfulness and emotion regulation—An fMRI study. Soc. Cogn. Affect. Neurosci. 2014, 9, 776–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, B.L.; Waltz, J. Mindfulness and experiential avoidance as predictors of posttraumatic stress disorder avoidance symptom severity. J. Anxiety Disord. 2010, 24, 409–415. [Google Scholar] [CrossRef]
- Arch, J.J.; Craske, M.G. Mechanisms of mindfulness: Emotion regulation following a focused breathing induction. Behav. Res. Ther. 2006, 44, 1849–1858. [Google Scholar] [CrossRef] [PubMed]
- Kiken, L.G.; Garland, E.L.; Bluth, K.; Palsson, O.S.; Gaylord, S.A. From a state to a trait: Trajectories of state mindfulness in meditation during intervention predict changes in trait mindfulness. Personal. Individ. Differ. 2015, 81, 41–46. [Google Scholar] [CrossRef] [Green Version]
- Garland, E.L.; Hanley, A.; Farb, N.A.; Froeliger, B. State Mindfulness During Meditation Predicts Enhanced Cognitive Reappraisal. Mindfulness 2015, 6, 234–242. [Google Scholar] [CrossRef] [PubMed]
- Germain, A.; Caroff, K.; Buysse, D.J.; Shear, M.K. Sleep quality in complicated grief. J. Traum. Stress 2005, 18, 343–346. [Google Scholar] [CrossRef]
- Carpenter, J.S.; Andrykowski, M.A. Psychometric evaluation of the pittsburgh sleep quality index. J. Psychosom. Res. 1998, 45, 5–13. [Google Scholar] [CrossRef]
- Hall, M.; Kupfer, D.J. Intrusive thoughts and avoidance behaviors are associated with sleep disturbances in bereavement-related depression. Depress. Anxiety 1997, 7, 106–112. [Google Scholar] [CrossRef]
- Hall, M.; Baum, A.; Buysse, D.J.; Prigerson, H.G.; Kupfer, D.J.; Reynolds, C.F. Sleep as a Mediator of the Stress-Immune Relationship. Psychosom. Med. 1998, 60, 48–51. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.; Buysse, D.J.; Nowell, P.D.; Nofzinger, E.A.; Houck, P.; Reynolds, C.F.; Kupfer, D.J. Symptoms of Stress and Depression as Correlates of Sleep in Primary Insomnia. Psychosom. Med. 2000, 62, 227–230. [Google Scholar] [CrossRef] [PubMed]
- Markarian, S.A.; Pickett, S.M.; Deveson, D.F.; Kanona, B.B. A model of BIS/BAS sensitivity, emotion regulation difficulties, and depression, anxiety, and stress symptoms in relation to sleep quality. Psychiatry Res. 2013, 210, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Hoyt, M.A.; Thomas, K.S.; Epstein, D.R.; Dirksen, S.R. Coping Style and Sleep Quality in Men with Cancer. Ann. Behav. Med. 2009, 37, 88–93. [Google Scholar] [CrossRef] [Green Version]
- Payne, A.; Kralj, A.; Young, J.; Meiser-Stedman, R. The prevalence of intrusive memories in adult depression: A meta-analysis. J. Affect. Disord. 2019, 253, 193–202. [Google Scholar] [CrossRef] [Green Version]
- Roemer, L.; Orsillo, S.M. Expanding Our Conceptualization of and Treatment for Generalized Anxiety Disorder: Integrating Mindfulness/Acceptance-Based Approaches With Existing Cognitive-Behavioral Models. Clin. Psychol. Sci. Pract. 2006, 9, 54–68. [Google Scholar] [CrossRef]
- Cowdrey, F.A.; Park, R.J. The role of experiential avoidance, rumination and mindfulness in eating disorders. Eat. Behav. 2012, 13, 100–105. [Google Scholar] [CrossRef]
- Liu, Q.-Q.; Zhou, Z.-K.; Yang, X.-J.; Kong, F.-C.; Sun, X.-J.; Fan, C.-Y. Mindfulness and sleep quality in adolescents: Analysis of rumination as a mediator and self-control as a moderator. Personal. Individ. Differ. 2018, 122, 171–176. [Google Scholar] [CrossRef]
- Murnieks, C.Y.; Arthurs, J.D.; Cardon, M.S.; Farah, N.; Stornelli, J.; Michael Haynie, J. Close your eyes or open your mind: Effects of sleep and mindfulness exercises on entrepreneurs’ exhaustion. J. Bus. Ventur. 2019, S0883902617305281. [Google Scholar] [CrossRef]
- Rash, J.A.; Kavanagh, V.A.J.; Garland, S.N. A Meta-Analysis of Mindfulness-Based Therapies for Insomnia and Sleep Disturbance. Sleep Med. Clin. 2019, 14, 209–233. [Google Scholar] [CrossRef]
- Baer, R.A.; Smith, G.T.; Hopkins, J.; Krietemeyer, J.; Toney, L. Using Self-Report Assessment Methods to Explore Facets of Mindfulness. Assessment 2006, 13, 27–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Creamer, M.; Bell, R.; Failla, S. Psychometric properties of the Impact of Event Scale—Revised. Behav. Res. Ther. 2003, 41, 1489–1496. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, M.; Wilner, N.; Alvarez, W. Impact of Event Scale: A Measure of Subjective Stress. Psychosom. Med. 1979, 41, 209–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaskin, J. Gaskination’s StatWiki. S.E.M. 2020. Available online: http://statwiki.kolobkreations.com (accessed on 5 November 2020).
- Ong, J.C. Mindfulness-Based Therapy for Insomnia; American Psychological Association: Washington, DC, USA, 2017; p. 233. ISBN 978-1-4338-2241-4. [Google Scholar]
- Mustian, K.M.; Janelsins, M.; Peppone, L.J.; Kamen, C. Yoga for the Treatment of Insomnia among Cancer Patients: Evidence, Mechanisms of Action, and Clinical Recommendations. Oncol. Hematol. Rev. 2014, 10, 164–168. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Theoretical Model. Note: Hypothesis numbers are indicated above, with the predicted correlational valences.
Figure 1.
Theoretical Model. Note: Hypothesis numbers are indicated above, with the predicted correlational valences.

Figure 2.
Confirmatory Factor Analysis for the Cognitive and Affective Mindfulness Scale (CAMS-R) scale showing modifications made to the error term covariances.
Figure 2.
Confirmatory Factor Analysis for the Cognitive and Affective Mindfulness Scale (CAMS-R) scale showing modifications made to the error term covariances.

Figure 3.
Confirmatory Factor Analysis for the Impact of Event Scale (IES) scale showing modifications made to the error term covariances.
Figure 3.
Confirmatory Factor Analysis for the Impact of Event Scale (IES) scale showing modifications made to the error term covariances.

Figure 4.
Confirmatory Factor Analysis for the Five Facet Mindfulness Questionnaire (FFMQ) scale showing modifications made to the error term covariances.
Figure 4.
Confirmatory Factor Analysis for the Five Facet Mindfulness Questionnaire (FFMQ) scale showing modifications made to the error term covariances.

Figure 5.
Confirmatory Factor Analysis for the Emotion Regulation Questionnaire (ERQ) scale showing modifications made to the error term covariances.
Figure 5.
Confirmatory Factor Analysis for the Emotion Regulation Questionnaire (ERQ) scale showing modifications made to the error term covariances.

Figure 6.
Basic Model with results of correlational analyses. Note: The hypotheses are numbered accordingly from 1–5 and the correlations listed in green indicate the resulting correlation satisfied the hypotheses in the theoretical model, and the two correlates are denoted by parentheses. The correlations listed in red indicate they did not satisfy the correlational hypotheses in the theoretical model. Subscales were not listed if they did not show a significant bivariate correlation. Note: ** Correlation is significant at the 0.01 level, p < 0.01. Note: * Correlation is significant at the 0.05 level, p < 0.05.
Figure 6.
Basic Model with results of correlational analyses. Note: The hypotheses are numbered accordingly from 1–5 and the correlations listed in green indicate the resulting correlation satisfied the hypotheses in the theoretical model, and the two correlates are denoted by parentheses. The correlations listed in red indicate they did not satisfy the correlational hypotheses in the theoretical model. Subscales were not listed if they did not show a significant bivariate correlation. Note: ** Correlation is significant at the 0.01 level, p < 0.01. Note: * Correlation is significant at the 0.05 level, p < 0.05.

Figure 7.
Test of the model that IES (HYP) (hyperarousal) will mediate the relationship between Mindfulness and PSQI, Step 1, direct effect.
Figure 7.
Test of the model that IES (HYP) (hyperarousal) will mediate the relationship between Mindfulness and PSQI, Step 1, direct effect.

Figure 8.
Test of the model that CAMS-R will mediate the relationship between IES and PSQI, Step 2, indirect effect.
Figure 8.
Test of the model that CAMS-R will mediate the relationship between IES and PSQI, Step 2, indirect effect.

Table 1.
Descriptives statistics for all constructs as computed after factor analytic construct analyses.
Table 1.
Descriptives statistics for all constructs as computed after factor analytic construct analyses.
| N | Mean | Skewness | Kurtosis | |||||
|---|---|---|---|---|---|---|---|---|
| Measure | Statistic | Statistic | Std. Error | Std. Deviation | Statistic | Std. Error | Statistic | Std. Error |
| PSQI_GLOBAL_NORM | 367 | 13.80 | 0.22 | 4.21 | 0.06 | 0.13 | −0.09 | 0.25 |
| IES_AVD_NORM | 367 | 2.70 | 0.05 | 0.91 | 0.08 | 0.13 | −0.30 | 0.25 |
| IES_HYP_NORM | 367 | 1.93 | 0.04 | 0.85 | 0.08 | 0.13 | −0.30 | 0.25 |
| IES_INT_NORM | 367 | 2.55 | 0.05 | 0.90 | 0.08 | 0.13 | −0.30 | 0.25 |
| ERQ_ES_NORM | 367 | 3.26 | 0.06 | 1.16 | 0.05 | 0.13 | −0.08 | 0.25 |
| ERQ_CR_NORM | 367 | 3.13 | 0.04 | 0.73 | 0.05 | 0.13 | −0.08 | 0.25 |
| FFMQ_NR_NORM | 366 | 0.93 | 0.01 | 0.25 | 0.00 | 0.13 | −0.17 | 0.25 |
| FFMQ_OBS_NORM | 366 | 1.75 | 0.03 | 0.50 | 0.00 | 0.13 | −0.17 | 0.25 |
| FFMQ_DESC_NORM | 366 | 2.65 | 0.04 | 0.78 | 0.00 | 0.13 | −0.17 | 0.25 |
| FFMQ_AA_NORM | 366 | 2.67 | 0.04 | 0.77 | 0.00 | 0.13 | −0.17 | 0.25 |
| FFMQ_NJ_NORM | 366 | 2.28 | 0.04 | 0.70 | 0.00 | 0.13 | −0.17 | 0.25 |
| Valid N (listwise) | 363 | |||||||
Note. Data suffered from widespread problems with high kurtosis and skewness and so were rank ordered and then transformed using the inverse normal transform function in IBM SPSS Statistics V. 26. PSQI_GLOBAL_NORM = Pittsburgh Sleep Quality Index Global Sleep Quality Score, normalized; IES_AVD_NORM = Avoidance subscale of IES, normalized; IES_HYP_NORM = Hyperarousal subscale of the IES, normalized; IES_INT_NORM = Intrusive thoughts subscale of IES, normalized; ERQ_ES_NORM = Emotion suppression subscale of ERQ, normalized; ERQ CR_NORM = Cognitive reappraisal subscale of the ERQ, normalized; FFMQ_NR_NORM = Non-reacting subscale of the FFMQ, normalized; FFMQ_OBS_NORM = Observe subscale of the FFMQ, normalized; FFMQ_DESC_NORM = Description subscale of the FFMQ, normalized; FFMQ_AA_NORM = Acting with awareness subscale of the FFMQ, normalized; FFMQ_NJ_NORM = Non-judging subscale of the FFMQ, normalized.
Table 2.
Correlations between all Constructs.
| n | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. CAMS_R | Pearson Correlation | 367 | 1 | −0.290 ** | −0.070 | −0.201 ** | −0.167 ** | −0.088 | 0.294 ** | 0.277 ** | 0.128 * | 0.517 ** | 0.474 ** | 0.310 ** |
| 2. PSQI_GLOBAL | Pearson Correlation | 367 | −0.290 ** | 1 | 0.305 ** | 0.436 ** | 0.424 ** | 0.093 | −0.051 | −0.079 | 0.120 * | −0.096 | −0.413 ** | −0.337 ** |
| 3. IES_AVD | Pearson Correlation | 367 | −0.070 | 0.305 ** | 1 | 0.727 ** | 0.792 ** | 0.145 ** | 0.067 | 0.085 | 0.176 ** | −0.016 | −0.288 ** | −0.369 ** |
| 4. IES_HYP | Pearson Correlation | 367 | −0.201 ** | 0.436 ** | 0.727 ** | 1 | 0.860 ** | 0.015 | −0.048 | −0.026 | 0.116 * | −0.067 | −0.359 ** | −0.416 ** |
| 5. IES_INT | Pearson Correlation | 367 | −0.167 ** | 0.424 ** | 0.792 ** | 0.860 ** | 1 | 0.039 | −0.008 | −0.016 | 0.125 * | −0.029 | −0.378 ** | −0.404 ** |
| 6. ERQ_ES | Pearson Correlation | 367 | −0.088 | 0.093 | 0.145 ** | 0.015 | 0.039 | 1 | 0.171 ** | 0.060 | −0.070 | −0.256 ** | −0.124 * | −0.108 * |
| 7. ERQ_CR | Pearson Correlation | 367 | 0.294 ** | −0.051 | 0.067 | −0.048 | −0.008 | 0.171 ** | 1 | 0.249 ** | 0.112 * | 0.166 ** | 0.103 * | −0.013 |
| 8. FFMQ_NR | Pearson Correlation | 367 | 0.277 ** | −0.079 | 0.085 | −0.026 | −0.016 | 0.060 | 0.249 ** | 1 | 0.383 ** | 0.440 ** | −0.105 * | −0.111 * |
| 9. FFMQ_OBS | Pearson Correlation | 367 | 0.128 * | 0.120 * | 0.176 ** | 0.116 * | 0.125 * | −0.070 | 0.112 * | 0.383 ** | 1 | 0.380 ** | −0.150 ** | −0.206 ** |
| 10. FFMQ_DESC | Pearson Correlation | 367 | 0.517 ** | −0.096 | −0.016 | −0.067 | −0.029 | −0.256 ** | 0.166 ** | 0.440 ** | 0.380 ** | 1 | 0.190 ** | 0.069 |
| 11. FFMQ_AA | Pearson Correlation | 367 | 0.474 ** | −0.413 ** | −0.288 ** | −0.359 ** | −0.378 ** | −0.124 * | 0.103 * | −0.105 * | −0.150 ** | 0.190 ** | 1 | 0.613 ** |
| 12. FFMQ_NJ | Pearson Correlation | 367 | 0.310 ** | −0.337 ** | −0.369 ** | −0.416 ** | −0.404 ** | −0.108 * | −0.013 | −0.111 * | −0.206 ** | 0.069 | 0.613 ** | 1 |
** Correlation is significant at the 0.01 level 2-tailed). * Correlation is significant at the 0.05 level 2-tailed) Note: PSQI_GLOBAL_NORM = Pittsburgh Sleep Quality Index Global Sleep Quality Score, normalized ES_AVD_NORM = Avoidance subscale of IES, after normalization IES_HYP_NORM = Hyperarousal subscale of the IES, after normalized IES_INT_NORM = Intrusive thoughts subscale of IES, normalized ERQ_ES_NORM = Emotion suppression subscale of ERQ, normalized ERQ CR_NORM = Cognitive reappraisal subscale of the ERQ, normalized FFMQ_NR_NORM = Non-reacting subscale of the FFMQ, normalized FFMQ_OBS_NORM = Observe subscale of the FFMQ, normalized FFMQ_DESC_NORM = Description subscale of the FFMQ, normalized FFMQ_AA_NORM = Acting with awareness subscale of the FFMQ, normalized FFMQ_NJ_NORM = Non-judging subscale of the FFMQ, normalized.
Table 3.
Model Summary.
| Predictor | ∆R2 | β | Total R2 |
|---|---|---|---|
| Step 1 Control: IES (HYP) | 0.190 ** | 0.436 ** | 0.188 ** |
| Step 2 IES (HYP) FFMQ (AA) | 0.076 ** | 0.330 ** −0.295 ** | 0.262 ** |
| Step 3 IES (HYP) FFMQ (AA) CAMS-R | 0.009 * | 0.326 ** −0.245 ** −0.108 * | 0.269 * |
| n1 = 365 n2 = 364 n3 = 363 |
** Test is significant at the 0.01 level, p < 0.01, * Test is significant at the 0.05 levels, p < 0.05. Note: IES (HYP) = hyperarousal subscale of IES, FFMQ (AA) = acting with awareness subscale of FFMQ.
Table 4.
ANOVA Table for Linear Regression.
| Measure | df | F |
|---|---|---|
| Model 1 Constant IES (HYP) | 1 | F(1, 365) = 85.04 ** |
| Model 2 IES (HYP) FFMQ (AA) | 2 | F(2, 364) = 65.83 ** |
| Model 3 IES (HYP) FFMQ (AA) CAMS-R n = 366 | 3 | F(3, 363) = 45.82 ** |
** Test is significant at the 0.01 level, p < 0.01.
Table 5.
Coefficients of the Regression Model.
| Measure | Unst. Coefficients β | Std. Error | t | Zero Order | Partial Correlations | Semi-Partial Correlations |
|---|---|---|---|---|---|---|
| Constant | 9.626 | 4.93 | 19.522 ** | |||
| IES (HYP) | 2.165 | 0.234 | 9.247 ** | 0.436 | 0.436 | 0.436 |
| Constant | 14.939 | 0.986 | 15.152 ** | |||
| IES (HYP) | 1.639 | 0.239 | 6.852 ** | 0.436 | 0.338 | 0.308 |
| FFMQ (AA) | −1.607 | 0.262 | −6.131 ** | −0.413 | −0.306 | −0.275 |
| Constant | 16.476 | 1.218 | 13.522 ** | |||
| IES (HYP) | 1.620 | 0.238 | 6.800 ** | 0.436 | 0.336 | −0.304 |
| FFMQ (AA) | −1.336 | 0.290 | −4.599 ** | −0.413 | −0.235 | −0.206 |
| CAMS-R | −1.089 | 0.512 | −2.128 * | −0.290 | −0.111 | −0.095 |
** Test is significant at the 0.01 level, p < 0.01, ** Test is significant at the 0.05 level, p < 0.05.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Talley, G.; Shelley-Tremblay, J. The Relationship between Mindfulness and Sleep Quality is Mediated by Emotion Regulation. Psychiatry Int. 2020, 1, 42-66. https://0-doi-org.brum.beds.ac.uk/10.3390/psychiatryint1020007
AMA Style
Talley G, Shelley-Tremblay J. The Relationship between Mindfulness and Sleep Quality is Mediated by Emotion Regulation. Psychiatry International. 2020; 1(2):42-66. https://0-doi-org.brum.beds.ac.uk/10.3390/psychiatryint1020007
Chicago/Turabian StyleTalley, Garrett, and John Shelley-Tremblay. 2020. "The Relationship between Mindfulness and Sleep Quality is Mediated by Emotion Regulation" Psychiatry International 1, no. 2: 42-66. https://0-doi-org.brum.beds.ac.uk/10.3390/psychiatryint1020007