
What Is the Capacity of Individuals with Schizophrenia and Bipolar Disorder to Make Healthcare Decisions? An Exploratory Study of the Views of Patients, Psychiatrists, and Family Caregivers—A Survey on Decisional Capacity in Mental Health

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
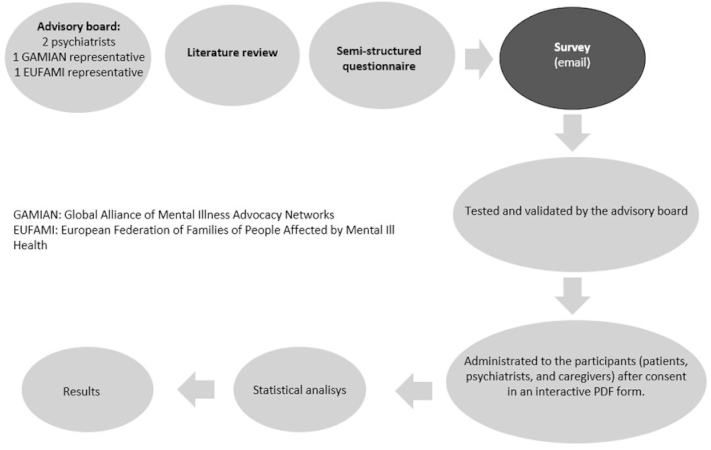
2.1. Design of Study
2.2. Selection of Participants
2.3. Questionnaire
2.4. Survey and Data Processing
3. Results
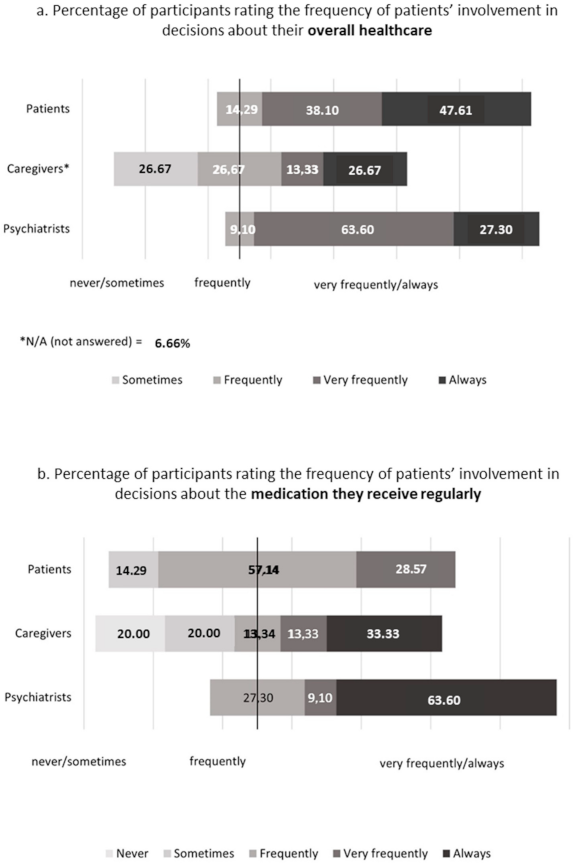
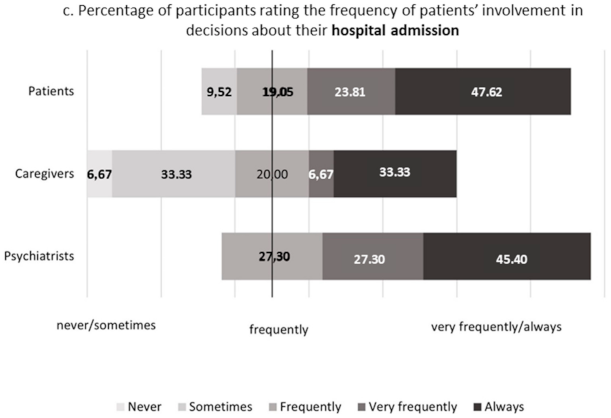
3.1. Participants’ Perceptions of Schizophrenia or Bipolar Disorder Patients’ Involvement in Everyday Life Healthcare Decisions
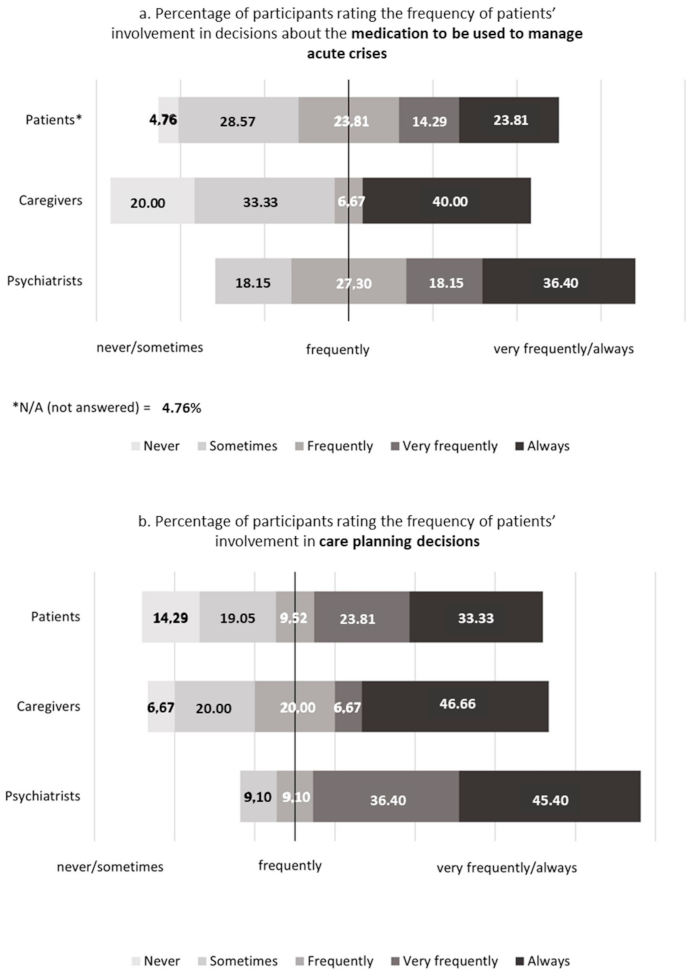
3.2. Participants’ Perceptions of Schizophrenia or Bipolar Disorder Patients’ Involvement in Decisions about Managing Acute Crises and Care Planning
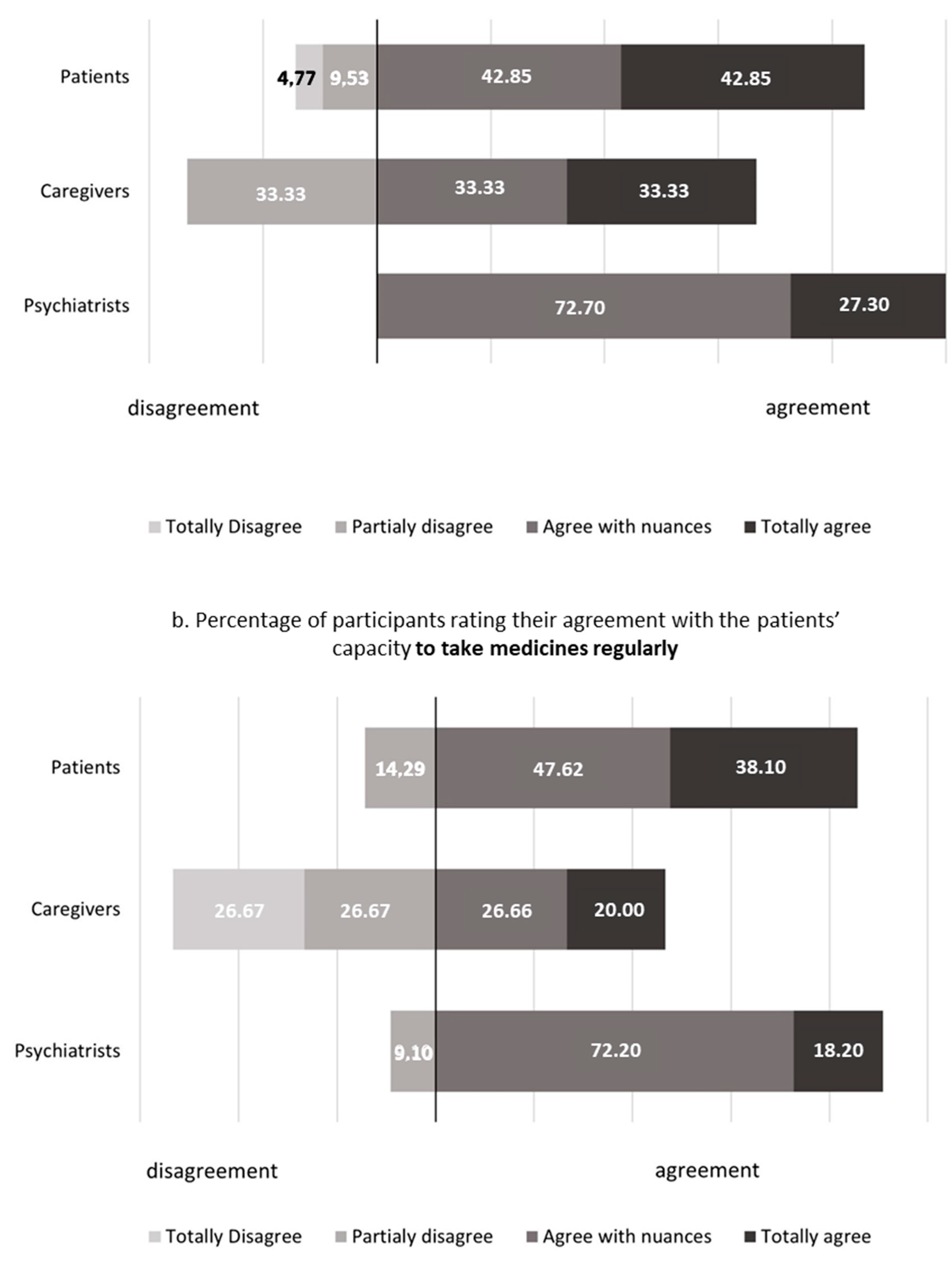
3.3. Participants’ Agreement on Schizophrenia or Bipolar Disorder Patients’ Capacity for Discussing and Following Their Psychiatric Treatment
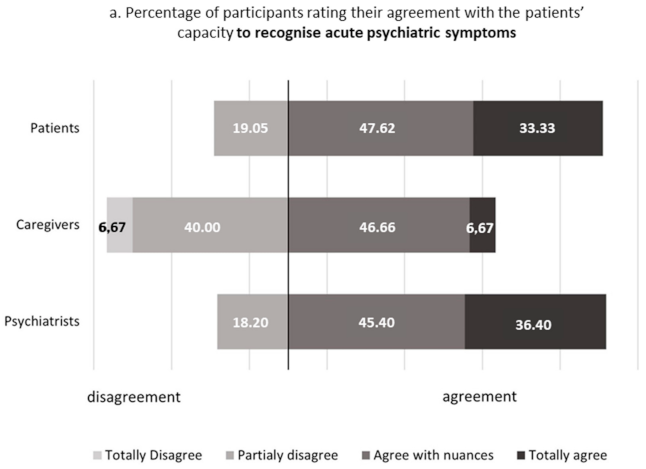
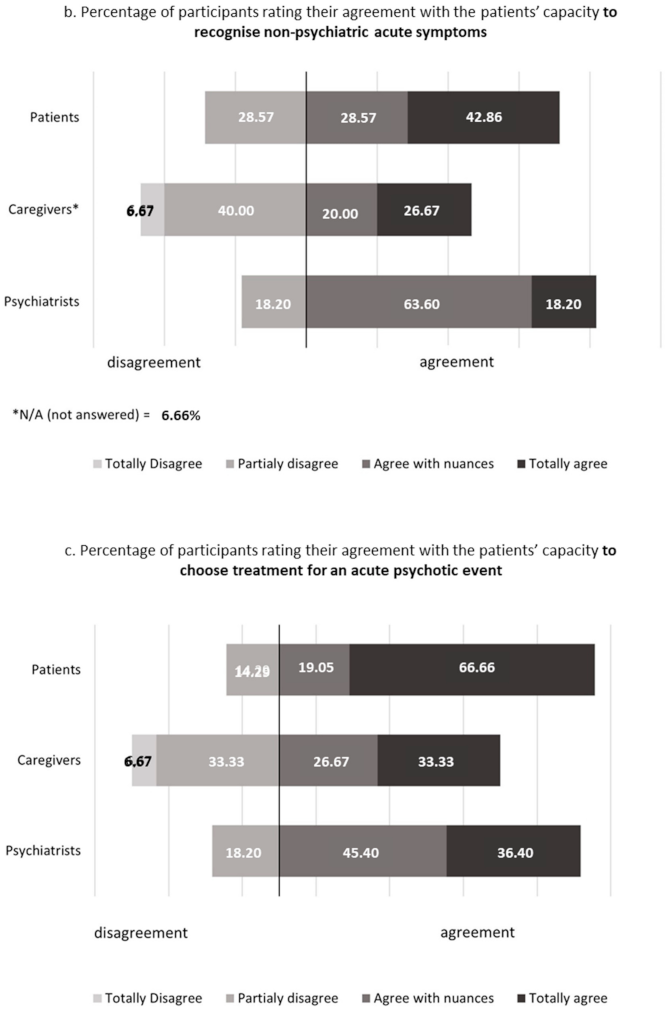
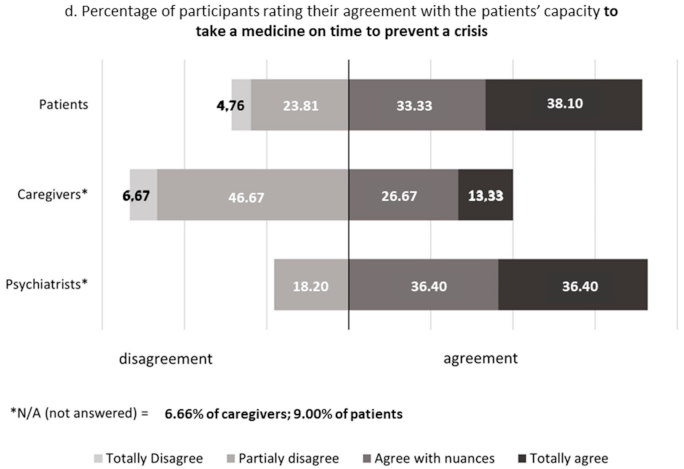
3.4. Participants’ Agreement with the Capacity of Schizophrenia or Bipolar Disorder Patients to Make and Execute Decisions Related to the Management of Acute Psychiatric Events
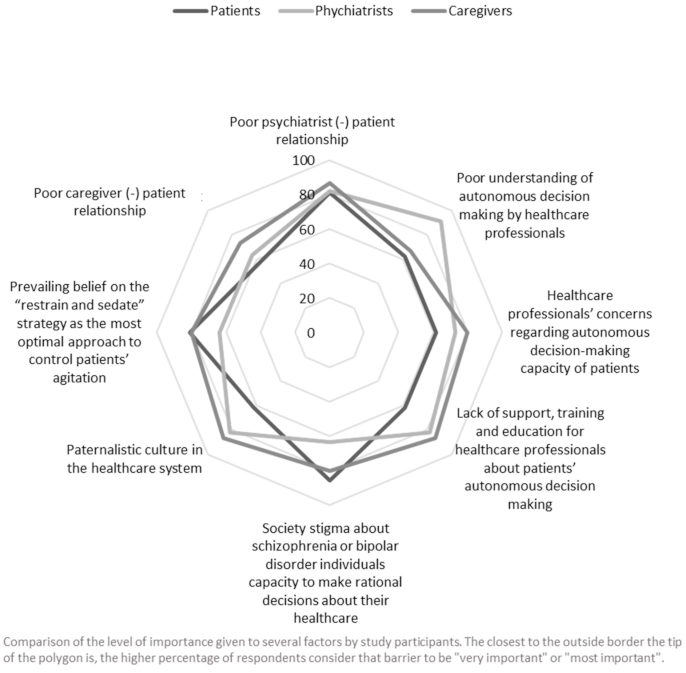
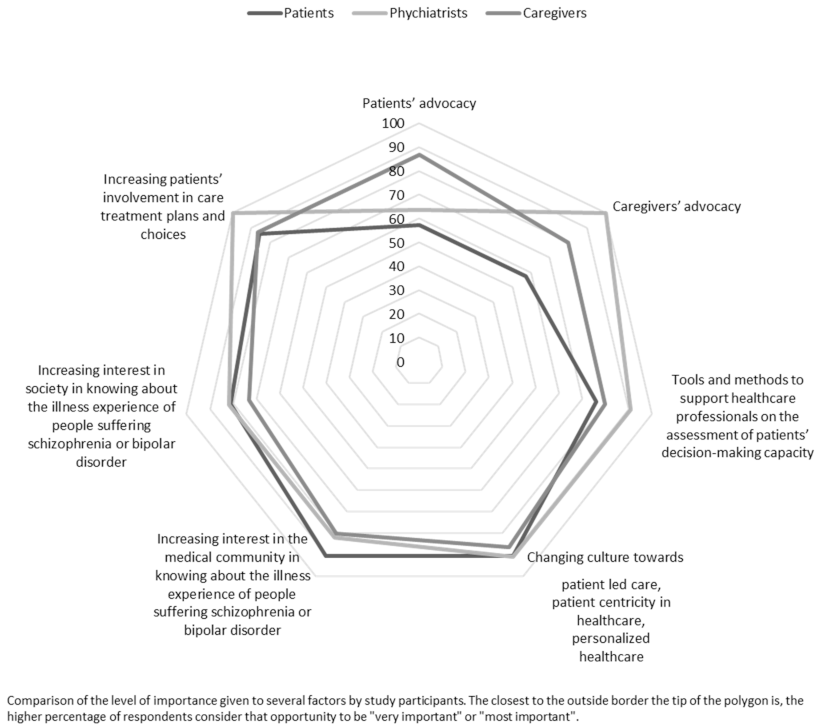
3.5. Participants’ Perception of Barriers and Opportunities for Empowering Schizophrenia and Bipolar Disorder Patients to Autonomous Decision Making
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Palmer, B.W.; Harmell, A.L. Assessment of Healthcare Decision-making Capacity. Arch. Clin. Neuropsychol. 2016, 31, 530–540. [Google Scholar] [CrossRef] [PubMed]
- Stroup, S.; Appelbaum, P.; Swartz, M.; Patel, M.; Davis, S.; Jeste, D.; Kim, S.; Keefe, R.; Manschreck, T.; McEvoy, J.; et al. Decision-making capacity for research participation among individuals in the CATIE schizophrenia trial. Schizophr. Res. 2005, 80, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Spencer, B.W.J.; Shields, G.; Gergel, T.; Hotopf, M.; Owen, G.S. Diversity or disarray? A systematic review of decision-making capacity for treatment and research in schizophrenia and other non-affective psychoses. Psychol. Med. 2017, 47, 1906–1922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeste, D.V.; Depp, C.A.; Palmer, B.W. Magnitude of impairment in decisional capacity in people with schizophrenia compared to normal subjects: An overview. Schizophr Bull. 2006, 32, 121–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pons, E.V.; Salvador-Carulla, L.; Calcedo-Barba, A.; Paz, S.; Messer, T.; Pacciardi, B.; Zeller, S.L. The capacity of schizophrenia and bipolar disorder individuals to make autonomous decisions about pharmacological treatments for their illness in real life: A scoping review. Health Sci. Rep. 2020, 3, e179. [Google Scholar] [CrossRef] [PubMed]
- Calcedo-Barba, A.; Fructuoso, A.; Martinez-Raga, J.; Paz, S.; De Carmona, M.S.; Vicens, E. A meta-review of literature reviews assessing the capacity of patients with severe mental disorders to make decisions about their healthcare. BMC Psychiatry 2020, 20, 1–14. [Google Scholar] [CrossRef]
- Fisher, A.; Manicavasagar, V.; Sharpe, L.; Laidsaar-Powell, R.; Juraskova, I. A Qualitative Exploration of Clinician Views and Experiences of Treatment Decision-Making in Bipolar II Disorder. Community Ment. Health J. 2017, 53, 958–971. [Google Scholar] [CrossRef]
- Jeste, D.V.; Eglit, G.M.L.; Palmer, B.W.; Martinis, J.G.; Blanck, P.; Saks, E.R. Supported Decision Making in Serious Mental Illness. Psychiatry 2018, 81, 28–40. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.-B.; Wang, Y.-Y.; Ungvari, G.S.; Ng, C.H.; Wu, R.-R.; Wang, J.; Xiang, Y.-T. The MacArthur Competence Assessment Tools for assessing decision-making capacity in schizophrenia: A meta-analysis. Schizophr. Res. 2017, 183, 56–63. [Google Scholar] [CrossRef]
- Matthias, M.S.; Salyers, M.P.; Rollins, A.L.; Frankel, R.M. Decision making in recovery-oriented mental health care. Psychiatr. Rehabilitation J. 2012, 35, 305–314. [Google Scholar] [CrossRef] [Green Version]
- Mikesell, L.; Bromley, E.; Young, A.S.; Vona, P.; Zima, B. Integrating Client and Clinician Perspectives on Psychotropic Medication Decisions: Developing a Communication-Centered Epistemic Model of Shared Decision Making for Mental Health Contexts. Health Commun. 2015, 31, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grim, K.; Rosenberg, D.; Svedberg, P.; Schön, U.-K. Shared decision-making in mental health care—A user perspective on decisional needs in community-based services. Int. J. Qual. Stud. Health Well-Being 2016, 11, 30563. [Google Scholar] [CrossRef] [PubMed]
- NICE. Decision-Making and Mental Capacity-NICE Guideline. 2018. Available online: https://www.nice.org.uk/guidance/ng108/resources/decisionmaking-and-mental-capacity-pdf-66141544670917 (accessed on 20 October 2018).
- Younas, M.; Bradley, E.; Holmes, N.; Sud, D.; Maidment, I.D. Mental health pharmacists views on shared decision-making for antipsychotics in serious mental illness. Int. J. Clin. Pharm. 2016, 38, 1191–1199. [Google Scholar] [CrossRef] [Green Version]
- Gamian-Europe. Global Alliance of Mental Illness Advocacy Networks-Europe [Internet]. 2020. Available online: https://www.gamian.eu/ (accessed on 20 April 2020).
- EUFAMI. European Federation of Families of People Affected by Mental Ill Health-UFAMI [Internet]. 2020. Available online: http://www.eufami.org/ (accessed on 20 April 2020).
- Garland, R. The mid-point on a rating scale: Is it desirable. Mark Bull. 1991, 2, 66–70. [Google Scholar]
- European Commission. Data Protection in the EU [Internet], The General Data Protection Regulation (GDPR), the Data Protection Law Enforcement Directive and Other Rules Concerning the Protection of Personal Data. Available online: https://ec.europa.eu/info/law/law-topic/data-protection/data-protection-eu_en (accessed on 6 March 2021).
- Brain, C.; Kymes, S.; DiBenedetti, D.B.; Brevig, T.; Velligan, D.I. Experiences, attitudes, and perceptions of caregivers of individuals with treatment-resistant schizophrenia: A qualitative study. BMC Psychiatry 2018, 18, 1–13. [Google Scholar] [CrossRef]
- Von Kardorff, E.; Soltaninejad, A.; Kamali, M.; Eslami Shahrbabaki, M. Family caregiver burden in mental illnesses: The case of affective disorders and schizophrenia-A qualitative exploratory study. Nord. J. Psychiatry. 2016, 70, 248–254. [Google Scholar] [CrossRef]
- Morán-Sánchez, I.; Gómez-Vallés, P.; Bernal-López, M.; Ángeles Pérez-Cárceles, M.D. Shared decision-making in outpatients with mental disorders: Patients´ preferences and associated factors. J. Evaluation Clin. Pr. 2019, 25, 1200–1209. [Google Scholar] [CrossRef]
- Beitinger, R.; Kissling, W.; Hamann, J. Trends and perspectives of shared decision-making in schizophrenia and related disorders. Curr. Opin. Psychiatry 2014, 27, 222–229. [Google Scholar] [CrossRef]
- Liebherz, S.; Tlach, L.; Härter, M.; Dirmaier, J. Information and decision-making needs of psychiatric patients: The perspective of relatives. PeerJ 2017, 5, e3378. [Google Scholar] [CrossRef] [Green Version]
- Hamann, J.; Heres, S. Adapting Shared Decision Making for Individuals With Severe Mental Illness. Psychiatr. Serv. 2014, 65, 1483–1486. [Google Scholar] [CrossRef]
- Ehrlich, C.; Dannapfel, P. Shared decision making: People with severe mental illness experiences of involvement in the care of their physical health. Ment. Health Prev. 2017, 5, 21–26. [Google Scholar] [CrossRef]
- Kemp, K.; Zelle, H.; Bonnie, R.J. Embedding Advance Directives in Routine Care for Persons with Serious Mental Illness: Implementation Challenges. Psychiatr. Serv. 2015, 66, 10–14. [Google Scholar] [CrossRef] [PubMed]
- De las Cuevas, C.; Peñate, W.; de Rivera, L. Psychiatric patients’ preferences and experiences in clinical decision-making: Examining concordance and correlates of patients’ preferences. Patient Educ. Couns. 2014, 96, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Gergel, T.; Owen, G.S. Fluctuating capacity and advance decision-making in Bipolar Affective Disorder—Self-binding directives and self-determination. Int. J. Law Psychiatry 2015, 40, 92–101. [Google Scholar] [CrossRef] [Green Version]
- Hindley, G.; Stephenson, L.A.; Keene, A.R.; Rifkin, L.; Gergel, T.; Owen, G. “Why have I not been told about this?”: A survey of experiences of and attitudes to advance decision-making amongst people with bipolar. Wellcome Open Res. 2019, 4, 16. [Google Scholar] [CrossRef]
- Scholten, M.; Gieselmann, A.; Gather, J.; Vollmann, J. Psychiatric Advance Directives Under the Convention on the Rights of Persons With Disabilities: Why Advance Instructions Should Be Able to Override Current Preferences. Front. Psychiatry 2019, 10, 1–13. [Google Scholar] [CrossRef]
- Fisher, A.; Manicavasagar, V.; Kiln, F.; Juraskova, I. Communication and decision-making in mental health: A systematic review focusing on Bipolar disorder. Patient Educ. Couns. 2016, 99, 1106–1120. [Google Scholar] [CrossRef]
- Okai, D.; Owen, G.; Mc, H. Mental capacity in psychiatric patients: Systematic review. Br. J. Psychiatry. 2007, 191, 291–297. [Google Scholar] [CrossRef]
- Hostiuc, S.; Rusu, M.C.; Negoi, I.; Drima, E. Testing decision-making competency of schizophrenia participants in clinical trials. A meta-analysis and meta-regression. BMC Psychiatry 2018, 18, 2. [Google Scholar] [CrossRef] [Green Version]
- Palmer, B.; Dunn, L.; Appelbaum, P.; Al, E. Assessment of capacity to consent to research among older persons with schizophrenia, Alzheimer disease, or diabetes mellitus: Comparison of a 3-item questionnaire with a comprehensive standardized capacity instrument. Arch. Gen. Psychiatry. 2005, 62, 726–733. [Google Scholar] [CrossRef] [Green Version]
- Sjöstrand, M.; Karlsson, P.; Sandman, L.; Helgesson, G.; Eriksson, S.; Juth, N. Conceptions of decision-making capacity in psychiatry: Interviews with Swedish psychiatrists Ethics in Public Health, medical law, and health policy. BMC Med Ethics 2015, 16, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Mandarelli, G.; Tarsitani, L.; Parmigiani, G.; Polselli, G.M.; Frati, P.; Biondi, M.; Ferracuti, S. Mental Capacity in Patients Involuntarily or Voluntarily Receiving Psychiatric Treatment for an Acute Mental Disorder. J. Forensic Sci. 2014, 59, 1002–1007. [Google Scholar] [CrossRef]
- Bridges, J.F.; Kinter, E.T.; Schmeding, A.; Rudolph, I.; Mühlbacher, A. Can Patients Diagnosed with Schizophrenia Complete Choice-Based Conjoint Analysis Tasks? Patient: Patient-Centered Outcomes Res. 2011, 4, 267–275. [Google Scholar] [CrossRef]
- Calvó-Perxas, L.; Vilalta-Franch, J.; Litwin, H.; Turro-Garriga, O.; Mira, P.; Garre-Olmo, J. What seems to matter in public policy and the health of informal caregivers? A cross-sectional study in 12 European countries. PLoS ONE 2018, 13, e0194232. [Google Scholar] [CrossRef] [Green Version]
- Mariani, E.; Vernooij-Dassen MKoopmans, R.; Engels, Y.; Chattat, R. Shared decision-making in dementia care planning: Barriers and facilitators in two European countries. Aging Ment. Health 2017, 21, 31–39. [Google Scholar] [CrossRef]
- Mental Health Commission of New South Wales. Medication and Mental Illness. Perspectives. [Internet]. 2015. Available online: https://nswmentalhealthcommission.com.au/sites/default/files/uploads/Medication%20and%20mental%20illness%20perspectives%20Nov%202015.pdf (accessed on 20 April 2020).
- Brophy, L.; Kokanovic, R.; Flore, J.; McSherry, B.; Herrman, H. Community Treatment Orders and Supported Decision-Making. Front. Psychiatry 2019, 10, 1–12. [Google Scholar] [CrossRef]
- Gondek, D.; Edbrooke-Childs JVelikonja, T.; Al, E. Facilitators and Barriers to Person-centred Care in Child and Young People Mental Health Services: A Systematic Review. Clin. Psychol. Psychother. 2017, 24, 870–886. [Google Scholar] [CrossRef]
- Guidry-Grimes, L. Overcoming Obstacles to Shared Mental Health Decision Making. AMA J. Ethic. 2020, 22, E446–E451. [Google Scholar] [CrossRef]
- Shepherd, A.; Shorthouse, O.; Gask, L. Consultant psychiatrists’ experiences of and attitudes towards shared decision making in antipsychotic prescribing, a qualitative study. BMC Psychiatry 2014, 14, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kikkert, M.J.; Schene, A.H.; Koeter, M.W.J.; Robson, D.; Born, A.; Helm, H.; Nosè, M.; Goss, C.; Thornicroft, G.; Gray, R.J. Medication Adherence in Schizophrenia: Exploring Patients’, Carers’ and Professionals’ Views. Schizophr. Bull. 2005, 32, 786–794. [Google Scholar] [CrossRef] [Green Version]
- Lloyd, J.; Lloyd, H.; Fitzpatrick, R.; Peters, M. Treatment outcomes in schizophrenia: Qualitative study of the views of family carers. BMC Psychiatry 2017, 17, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vasudeva, S.; Al, E. Caregivers burden of patients with schizophrenia and bipolar disorder: A sectional study. Indian J. Psychol. Med. 2013, 35, 352–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grover, S.; Chakrabarti, S.; Aggarwal, M.; Avasthi, A.; Kulhara, P.; Sharma, S.; Khehra, N. Comparative study of the experience of caregiving in bipolar affective disorder and schizophrenia. Int. J. Soc. Psychiatry 2011, 58, 614–622. [Google Scholar] [CrossRef] [PubMed]










Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vicens Pons, E.; Calcedo Barba, A.; Hastings, J.; Männikkö, M.; Paz Ruiz, S. What Is the Capacity of Individuals with Schizophrenia and Bipolar Disorder to Make Healthcare Decisions? An Exploratory Study of the Views of Patients, Psychiatrists, and Family Caregivers—A Survey on Decisional Capacity in Mental Health. Psychiatry Int. 2021, 2, 127-144. https://0-doi-org.brum.beds.ac.uk/10.3390/psychiatryint2020010
Vicens Pons E, Calcedo Barba A, Hastings J, Männikkö M, Paz Ruiz S. What Is the Capacity of Individuals with Schizophrenia and Bipolar Disorder to Make Healthcare Decisions? An Exploratory Study of the Views of Patients, Psychiatrists, and Family Caregivers—A Survey on Decisional Capacity in Mental Health. Psychiatry International. 2021; 2(2):127-144. https://0-doi-org.brum.beds.ac.uk/10.3390/psychiatryint2020010
Chicago/Turabian StyleVicens Pons, Enric, Alfredo Calcedo Barba, Jacinta Hastings, Miia Männikkö, and Silvia Paz Ruiz. 2021. "What Is the Capacity of Individuals with Schizophrenia and Bipolar Disorder to Make Healthcare Decisions? An Exploratory Study of the Views of Patients, Psychiatrists, and Family Caregivers—A Survey on Decisional Capacity in Mental Health" Psychiatry International 2, no. 2: 127-144. https://0-doi-org.brum.beds.ac.uk/10.3390/psychiatryint2020010