
Association between Self-Restraint Behavior, Stigma and Depressive Tendency in Office Workers during the COVID-19 Pandemic in Japan—Self-Restraint Behavior and Depression during the COVID-19


 ,
,
Abstract
:1. Introduction
Background
2. Methods
2.1. Data Collection
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Comparison between Epidemic Areas and Non-Epidemic Areas
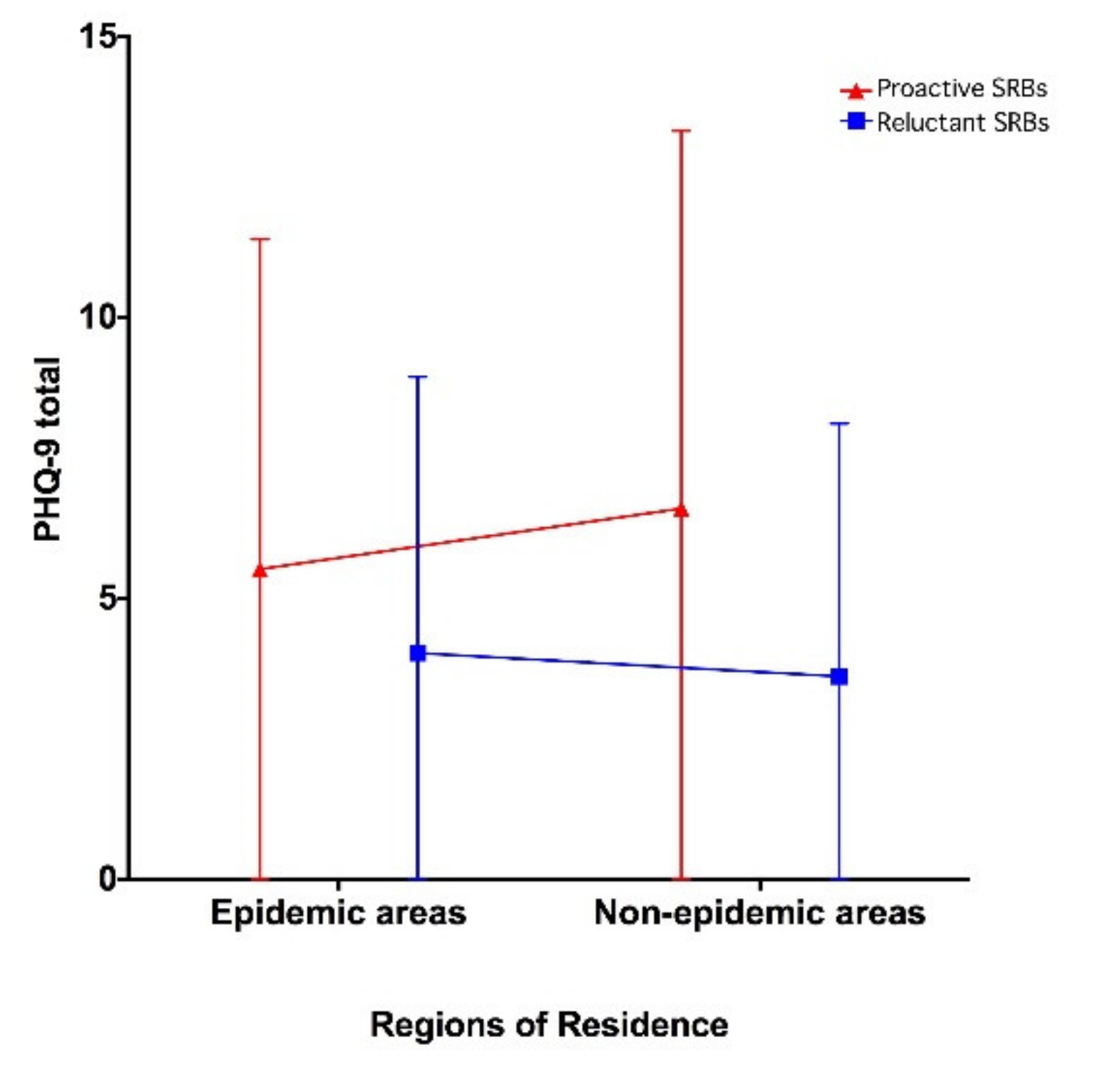
3.2. Two-Way ANOVA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Hellewell, J.; Abbott, S.; Gimma, A.; Bosse, N.I.; Jarvis, C.I.; Russell, T.W.; Munday, J.D.; Kucharski, A.J.; Edmunds, W.J. Centre for the Mathematical Modelling of Infectious Diseases C-WG et al.: Feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts. Lancet Glob. Health 2020, 8, e488–e496. [Google Scholar] [CrossRef] [Green Version]
- Xiang, M.; Yamamoto, S.; Mizoue, T. Depressive symptoms in students during school closure due to COVID-19 in Shanghai. Psychiatry Clin. Neurosci. 2020, 74, 664–666. [Google Scholar] [CrossRef] [PubMed]
- Pattojoshi, A.; Sidana, A.; Garg, S.; Mishra, S.N.; Singh, L.K.; Goyal, N.; Tikka, S.K. Staying home is NOT ‘staying safe’: A rapid 8-day online survey on spousal violence against women during the COVID-19 lockdown in India. Psychiatry Clin. Neurosci. 2020. [Google Scholar] [CrossRef]
- Torricelli, L.; Poletti, M.; Raballo, A. Managing COVID-19-related psychological distress in health workers: Field experience in northern Italy. Psychiatry Clin. Neurosci. 2021, 75, 23–24. [Google Scholar] [CrossRef] [PubMed]
- Mallik, C.I.; Radwan, R.B. Impact of lockdown due to COVID-19 pandemic in changes of prevalence of predictive psychiatric disorders among children and adolescents in Bangladesh. Asian J. Psychiatry 2021, 56, 102554. [Google Scholar] [CrossRef]
- Mackolil, J.; Mackolil, J. Addressing psychosocial problems associated with the COVID-19 lockdown. Asian J. Psychiatry 2020, 51, 102156. [Google Scholar] [CrossRef] [PubMed]
- Stavridou, A.; Stergiopoulou, A.A.; Panagouli, E.; Mesiris, G.; Thirios, A.; Mougiakos, T.; Troupis, T.; Psaltopoulou, T.; Tsolia, M.; Sergentanis, T.N.; et al. Psychosocial consequences of COVID-19 in children, adolescents and young adults: A systematic review. Psychiatry Clin. Neurosci. 2020, 74, 615–616. [Google Scholar] [CrossRef] [PubMed]
- Pignon, B.; Gourevitch, R.; Tebeka, S.; Dubertret, C.; Cardot, H.; Dauriac-Le Masson, V.; Trebalag, A.K.; Barruel, D.; Yon, L.; Hemery, F.; et al. Dramatic reduction of psychiatric emergency consultations during lockdown linked to COVID-19 in Paris and suburbs. Psychiatry Clin. Neurosci. 2020, 74, 557–559. [Google Scholar] [CrossRef]
- Muhidin, S.; Vizheh, M.; Moghadam, Z.B. Anticipating COVID-19-related stigma in survivors and health-care workers: Lessons from previous infectious diseases outbreaks-An integrative literature review. Psychiatry Clin. Neurosci. 2020, 74, 617–618. [Google Scholar] [CrossRef]
- Kuki, K.; Yamaguchi, Y.; Makinodan, M.; Honda, M.; Ueda, J.; Okazaki, K.; Okamura, K.; Kimoto, S.; Kishimoto, T. Effects of contacting with COVID-19 patients on the mental health of workers in a psychiatric hospital. Psychiatry Clin. Neurosci. 2020, 75, 67–69. [Google Scholar] [CrossRef] [PubMed]
- Do Duy, C.; Nong, V.M.; Van, A.N.; Thu, T.D.; Do Thu, N.; Quang, T.N. COVID-19 related stigma and its association with mental health of health-care workers after quarantined in Vietnam. Psychiatry Clin. Neurosci. 2020, 74, 566–568. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Bao, Y.; Lu, L. Addressing mental health care for the bereaved during the COVID-19 pandemic. Psychiatry Clin. Neurosci. 2020, 74, 406–407. [Google Scholar] [CrossRef]
- Shigemura, J.; Ursano, R.J.; Morganstein, J.C.; Kurosawa, M.; Benedek, D.M. Public responses to the novel 2019 coronavirus (2019-nCoV) in Japan: Mental health consequences and target populations. Psychiatry Clin. Neurosci. 2020, 74, 281–282. [Google Scholar] [CrossRef] [PubMed]
- Cheung, D.; Ip, E.C. COVID-19 Lockdowns: A Public Mental Health Ethics Perspective. Asian Bioeth. Rev. 2020, 12, 503–510. [Google Scholar] [CrossRef]
- Diamond, R.; Byrd, E. Standing up for health-improving mental wellbeing during COVID-19 isolation by reducing sedentary behaviour. J. Affect. Disord. 2020, 277, 232–234. [Google Scholar] [CrossRef]
- Katafuchi, Y.; Kurita, K.; Managi, S. COVID-19 with Stigma: Theory and Evidence from Mobility Data. Econ. Disasters Clim. Chang. 2020, 5, 71–95. [Google Scholar] [CrossRef]
- Cloninger, C.R.; Svrakic, D.M.; Przybeck, T.R. Can personality assessment predict future depression? A twelve-month follow-up of 631 subjects. J. Affect. Disord. 2006, 92, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Shirahama, M.; Terao, T.; Ishii, N.; Hatano, K.; Hirakawa, H.; Kohno, K. Relationship between anxious temperament and harm avoidance in medical students and staff. Psychiatry Clin. Neurosci. 2018, 72, 322–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qian, K.; Yahara, T. Mentality and behavior in COVID-19 emergency status in Japan: Influence of personality, morality and ideology. PLoS ONE 2020, 15, e0235883. [Google Scholar]
- Muto, K.; Yamamoto, I.; Nagasu, M.; Tanaka, M.; Wada, K. Japanese citizens’ behavioral changes and preparedness against COVID-19: An online survey during the early phase of the pandemic. PLoS ONE 2020, 15, e0234292. [Google Scholar]
- Kato, T.A.; Sartorius, N.; Shinfuku, N. Forced social isolation due to COVID-19 and consequent mental health problems: Lessons from hikikomori. Psychiatry Clin. Neurosci. 2020, 74, 506–507. [Google Scholar] [CrossRef] [PubMed]
- Fischer, L.S.; Mansergh, G.; Lynch, J. Santibanez S: Addressing Disease-Related Stigma During Infectious Disease Outbreaks. Disaster Med. Public Health Prep. 2019, 13, 989–994. [Google Scholar] [CrossRef]
- Person, B.; Sy, F.; Holton, K.; Govert, B.; Liang, A. Fear and stigma: The epidemic within the SARS outbreak. Emerg. Infect. Dis. 2004, 10, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Logie, C.H. Lessons learned from HIV can inform our approach to COVID-19 stigma. J. Int. 2020, 23, e25504. [Google Scholar] [CrossRef] [Green Version]
- Yamauchi, M. Naze Umareta “Jishuku Keisatsu” “Labeling” No Hitori Aruki, Massmedia Mo Katan? The Mainichi Newspapers. 2020. Available online: https://mainichi.jp/articles/20200818/k00/00m/040/229000c (accessed on 1 July 2021).
- Yoshida, M. Nihon-jin No Shinwateki-Shikou ga Kinou Seishin-Bunseki-i ga Yomitoku Korona. The Asahi Shimbun. 2020. Available online: https://www.asahi.com/articles/ASN5T3J9LN5RUCFI001.html (accessed on 1 July 2021).
- Muramatsu, K.; Miyaoka, H.; Kamijima, K.; Muramatsu, Y.; Tanaka, Y.; Hosaka, M.; Miwa, Y.; Fuse, K.; Yoshimine, F.; Mashima, I.; et al. Performance of the Japanese version of the Patient Health Questionnaire-9 (J-PHQ-9) for depression in primary care. Gen. Hosp. Psychiatry 2018, 52, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Connor, K.M.; Kobak, K.A.; Churchill, L.E.; Katzelnick, D.; Davidson, J.R. Mini-SPIN: A brief screening assessment for generalized social anxiety disorder. Depress. Anxiety 2001, 14, 137–140. [Google Scholar] [CrossRef]
- Kato, T.A.; Katsuki, R.; Kubo, H.; Shimokawa, N.; Sato-Kasai, M.; Hayakawa, K.; Kuwano, N.; Umene-Nakano, W.; Tateno, M.; Setoyama, D.; et al. Development and validation of the 22-item Tarumi’s Modern-Type Depression Trait Scale: Avoidance of Social Roles, Complaint, and Low Self-Esteem (TACS-22). Psychiatry Clin. Neurosci. 2019, 73, 448–457. [Google Scholar]
- Nishi, D.; Uehara, R.; Yoshikawa, E.; Sato, G.; Ito, M.; Matsuoka, Y. Culturally sensitive and universal measure of resilience for Japanese populations: Tachikawa Resilience Scale in comparison with Resilience Scale 14-item version. Psychiatry Clin. Neurosci. 2013, 67, 174–181. [Google Scholar]
- Kato, T.A.; Hashimoto, R.; Hayakawa, K.; Kubo, H.; Watabe, M.; Teo, A.R.; Kanba, S. Multidimensional anatomy of ‘modern type depression’ in Japan: A proposal for a different diagnostic approach to depression beyond the DSM-5. Psychiatry Clin. Neurosci. 2016, 70, 7–23. [Google Scholar] [CrossRef] [Green Version]
- Kato, T.A.; Shinfuku, N.; Fujisawa, D.; Tateno, M.; Ishida, T.; Akiyama, T.; Sartorius, N.; Teo, A.R.; Choi, T.Y.; Wand, A.P.; et al. Introducing the concept of modern depression in Japan; an international case vignette survey. J. Affect. Disord. 2011, 135, 66–76. [Google Scholar] [CrossRef] [PubMed]
- Kato, T.A.; Kanba, S.; Teo, A.R. Hikikomori: Multidimensional understanding, assessment, and future international perspectives. Psychiatry Clin. Neurosci. 2019, 73, 427–440. [Google Scholar] [CrossRef] [PubMed]
- Teo, A.R.; Nelson, S.; Strange, W.; Kubo, H.; Katsuki, R.; Kurahara, K.; Kanba, S.; Kato, T.A. Social withdrawal in major depressive disorder: A case-control study of hikikomori in japan. J. Affect. Disord. 2020, 274, 1142–1146. [Google Scholar] [CrossRef] [PubMed]
- Katsuki, R.; Tateno, M.; Kubo, H.; Kurahara, K.; Hayakawa, K.; Kuwano, N.; Kanba, S.; Kato, T.A. Autism spectrum conditions in hikikomori: A pilot case-control study. Psychiatry Clin. Neurosci 2020, 74, 652–658. [Google Scholar] [CrossRef] [PubMed]
- Kato, T.A.; Kanba, S. Modern-Type Depression as an “Adjustment” Disorder in Japan: The Intersection of Collectivistic Society Encountering an Individualistic Performance-Based System. Am. J. Psychiatry 2017, 174, 1051–1053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagiuda, K. Preventing Discrimination and Prejudice Related to Novel Coronavirus Infections; Japan Ministry of Education, Culture, Sports, Science and Technology: Tokyo, Japan, 2020.
- Taylor, S.; Landry, C.A.; Rachor, G.S.; Paluszek, M.M.; Asmundson, G.J.G. Fear and avoidance of healthcare workers: An important, under-recognized form of stigmatization during the COVID-19 pandemic. J. Anxiety Disord. 2020, 75, 102289. [Google Scholar] [CrossRef]
- Mamun, M.A.; Griffiths, M.D. First COVID-19 suicide case in Bangladesh due to fear of COVID-19 and xenophobia: Possible suicide prevention strategies. Asian J. Psychiatry 2020, 51, 102073. [Google Scholar] [CrossRef]
- Kahil, K.; Cheaito, M.A.; El Hayek, R.; Nofal, M.; El Halabi, S.; Kudva, K.G.; Pereira-Sanchez, V.; El Hayek, S. Suicide during COVID-19 and other major international respiratory outbreaks: A systematic review. Asian J. Psychiatry 2020, 56, 102509. [Google Scholar] [CrossRef]
- Panigrahi, M.; Pattnaik, J.I.; Padhy, S.K.; Menon, V.; Patra, S.; Rina, K.; Padhy, S.S.; Patro, B. COVID-19 and suicides in India: A pilot study of reports in the media and scientific literature. Asian J. Psychiatry 2021, 57, 102560. [Google Scholar] [CrossRef]
- Sudak, H.; Maxim, K.; Carpenter, M. Suicide and stigma: A review of the literature and personal reflections. Acad. Psychiatry 2008, 32, 136–142. [Google Scholar] [CrossRef]
- Van Rheenen, T.E.; Meyer, D.; Neill, E.; Phillipou, A.; Tan, E.J.; Toh, W.L.; Rossell, S.L. Mental health status of individuals with a mood-disorder during the COVID-19 pandemic in Australia: Initial results from the COLLATE project. J. Affect. Disord. 2020, 275, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Ueda, M.; Stickley, A.; Sueki, H.; Matsubayashi, T. Mental health status of the general population in Japan during the COVID-19 pandemic. Psychiatry Clin. Neurosci. 2020, 74, 505–506. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.; Hao, F.; McIntyre, R.S.; Jiang, L.; Jiang, X.; Zhang, L.; Zhao, X.; Zou, Y.; Hu, Y.; Luo, X.; et al. Is returning to work during the COVID-19 pandemic stressful? A study on immediate mental health status and psychoneuroimmunity prevention measures of Chinese workforce. Brain Behav. Immun. 2020, 87, 84–92. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| (The Following Instructions and Sentences Were Shown to the Respondents.) How Much Has the COVID-19 Pandemic Affected Your Daily Life? As of June 2020 and Presently, What Are Your Thoughts and Feelings about the Following Items? | ||||
|---|---|---|---|---|
| Strongly Disagree | Disagree | Agree | Strongly Agree | |
| 1. I proactively avoid direct social interaction. | 1 | 2 | 3 | 4 |
| 2. I proactively refrain from going out of the house. | 1 | 2 | 3 | 4 |
| 3 †. There is a limit to my patience, so I think it is better to act as freely as possible. | 1 | 2 | 3 | 4 |
| 4 †. I think I can go anywhere I want because there are no punitive laws with movement restriction. | 1 | 2 | 3 | 4 |
| 5. I think we need to refrain from moving because the populations in Japan are putting up with it. | 1 | 2 | 3 | 4 |
| 6 †. In order to relieve stress, I think it is unavoidable to behave in a manner that breaks the rule of avoiding “three Cs”. | 1 | 2 | 3 | 4 |
| 7 †. Even if there is a chance I am infected with the COVID-19, I still want to go out and take a break. | 1 | 2 | 3 | 4 |
| 8 †. Even if there is a chance that I am infected with the COVID-19, I still want to see people for a break. | 1 | 2 | 3 | 4 |
| 9. To prevent the spread of the COVID-19, I think it is necessary to refrain from moving. | 1 | 2 | 3 | 4 |
| 10. I do not want to be around people who have coughs, fevers and other cold symptoms. | 1 | 2 | 3 | 4 |
| 11. I do not want to be around people from foreign countries or domestic epidemic areas of the COVID-19. | 1 | 2 | 3 | 4 |
| 12. I do not want to be anywhere near health care workers. | 1 | 2 | 3 | 4 |
| 13. If I know from the license plate number that a car came from an epidemic area, I get nervous that I am going to be exposed to COVID-19. | 1 | 2 | 3 | 4 |
| 14. If I know from the license plate number that the car is from an epidemic area, I feel “Restrain yourself and don’t come here!” and become annoyed. | 1 | 2 | 3 | 4 |
| 15. I am scared of getting infected with the COVID-19 from people around me. | 1 | 2 | 3 | 4 |
| 16. I am scared of transmitting the COVID-19 to others. | 1 | 2 | 3 | 4 |
| 17. I am worried about my job status (employment, termination, leave of absence, job change, etc.). | 1 | 2 | 3 | 4 |
| 18. I am worried about my money (income, guaranteed absence from work, etc.). | 1 | 2 | 3 | 4 |
| 19. I am worried about my physical health. | 1 | 2 | 3 | 4 |
| 20. I am worried about my mental health. | 1 | 2 | 3 | 4 |
| 21. I feel tired. | 1 | 2 | 3 | 4 |
| 22. I feel irritated and angry. | 1 | 2 | 3 | 4 |
| 23. I feel depressed. | 1 | 2 | 3 | 4 |
| 24. I feel lonely. | 1 | 2 | 3 | 4 |
| Epidemic Areas | Non-Epidemic Areas | Statistics | ||||||
|---|---|---|---|---|---|---|---|---|
| n | Mean | SD | n | Mean | SD | t-Test, U-Test or x2 | p-Value | |
| Demographics | ||||||||
| Total (Male/Female) | 745 (357/388) | - | - | 308 (152/156) | - | - | x2 = 1.850 | 0.19 |
| Age | 44.88 | 8.27 | 44.84 | 8.284 | t = 0.072 | 0.943 | ||
| Work Status | ||||||||
| Employed/Self-employed | 703 (94.4%) | - | - | 293 (95.1%) | - | - | x2 = 1.043 | 0.594 |
| Without occupation | 33 (4.4%) | - | - | 10 (3.2%) | - | - | ||
| House Manager | 9 (1.2%) | - | - | 5 (1.6%) | - | - | ||
| COVID-19-related Factors | ||||||||
| Self-restraint behavior for COVID-19 prevention | 745 | 5.2 | 1.531 | 308 | 4.91 | 1.565 | t = 2.774 ** | 0.006 |
| The degree of motivation for self-restraint behavior | 745 | 22.61 | 3.73 | 308 | 22.56 | 3.192 | t = 0.206 | 0.837 |
| COVID-19-related stigma | 745 | 11.89 | 2.764 | 308 | 12 | 2.995 | t = −0.59 | 0.555 |
| COVID-19-related anxiety | 745 | 14.78 | 3.785 | 308 | 14.35 | 3.852 | t = 1.665 | 0.096 |
| COVID-19-related depressive feeling | 745 | 8.61 | 2.865 | 308 | 8.57 | 2.934 | t = 0.164 | 0.87 |
| Social Anxiety and Depressive Tendency | ||||||||
| MINI-SPIN total | 745 | 4.44 | 3.391 | 308 | 4.94 | 3.376 | t = −2.174 * | 0.03 |
| PHQ-9 total | 745 | 4.7 | 5.418 | 308 | 4.77 | 5.657 | t = −0.187 | 0.852 |
| Psychological Aspects | ||||||||
| TACS-22 total | 745 | 40.73 | 12.545 | 308 | 41.26 | 12.854 | t = −0.622 | 0.534 |
| Avoidance of social roles | 745 | 23.01 | 5.934 | 308 | 22.94 | 5.664 | t = 0.161 | 0.872 |
| Low self-esteem | 745 | 10.53 | 4.544 | 308 | 10.87 | 4.543 | t = −1.1 | 0.272 |
| Complaint | 745 | 7.19 | 5.054 | 308 | 7.45 | 5.2 | t = −0.746 | 0.456 |
| TRS total | 745 | 31.43 | 10.616 | 308 | 30.28 | 10.888 | t = 1.591 | 0.112 |
| Epidemic Areas (n = 745) | Non-Epidemic Areas (n = 308) | Statistics | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Proactive (n = 338) | Reluctant (n = 407) | Proactive (n = 120) | Reluctant (n = 188) | Effect of Region | Effect of Self-Restraint Behavior | Interaction | ||||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | F(1,1049) | p-Value | F(1,1049) | p-Value | F(1,1049) | p-Value | |
| COVID-19-related Factors | ||||||||||||||
| The degree of motivation for self-restraint behavior | 23.78 | 3.495 | 21.63 | 3.639 | 23.08 | 3.082 | 22.23 | 3.225 | 0.05 | 0.823 | 39.494 ** | <0.001 | 7.526 ** | 0.006 |
| COVID-19-related stigma | 12.93 | 2.409 | 11.03 | 2.746 | 13.22 | 2.689 | 11.23 | 2.928 | 1.761 | 0.185 | 111.28 ** | <0.001 | 0.054 | 0.816 |
| COVID-19-related anxiety | 15.98 | 3.608 | 13.78 | 3.639 | 15.98 | 3.653 | 13.31 | 3.614 | 0.887 | 0.346 | 94.801 ** | <0.001 | 0.896 | 0.344 |
| COVID-19-related depressive feelings | 9.14 | 2.861 | 8.16 | 2.794 | 9.59 | 3.129 | 7.93 | 2.611 | 0.298 | 0.585 | 46.026 ** | <0.001 | 3.096 | 0.079 |
| Social Anxiety and Depressive tendency | ||||||||||||||
| MINI-SPIN total | 4.9 | 3.536 | 4.05 | 3.221 | 5.79 | 3.474 | 4.39 | 3.203 | 7.059 ** | 0.008 | 23.552 ** | <0.001 | 1.47 | 0.226 |
| PHQ-9 total | 5.52 | 5.874 | 4.03 | 4.913 | 6.6 | 6.722 | 3.61 | 4.502 | 0.787 | 0.375 | 36.157 ** | <0.001 | 4.061 * | 0.044 |
| Psychological Aspects | ||||||||||||||
| TACS-22 total | 42.26 | 12.434 | 39.45 | 12.508 | 44.95 | 13.652 | 38.9 | 11.762 | 1.538 | 0.215 | 26.367 ** | <0.001 | 3.516 | 0.061 |
| Avoidance of social roles | 23.15 | 5.598 | 22.88 | 6.204 | 23.85 | 6.124 | 22.36 | 5.285 | 0.048 | 0.827 | 4.722 ** | 0.03 | 2.29 | 0.131 |
| Low self-esteem | 11.39 | 4.675 | 9.82 | 4.31 | 12.28 | 4.197 | 9.97 | 4.539 | 2.852 | 0.092 | 39.591 ** | <0.001 | 1.403 | 0.237 |
| Complaint | 7.72 | 5.149 | 6.75 | 4.938 | 8.83 | 5.848 | 6.57 | 4.542 | 1.751 | 0.186 | 21.426 ** | <0.001 | 3.386 | 0.066 |
| TRS total | 30.67 | 11.364 | 32.07 | 9.922 | 28.89 | 10.727 | 31.16 | 10.925 | 3.301 | 0.07 | 6.222 * | 0.013 | 0.349 | 0.555 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katsuki, R.; Kubo, H.; Yamakawa, I.; Shinfuku, N.; Sartorius, N.; Sakamoto, S.; Kato, T.A. Association between Self-Restraint Behavior, Stigma and Depressive Tendency in Office Workers during the COVID-19 Pandemic in Japan—Self-Restraint Behavior and Depression during the COVID-19. Psychiatry Int. 2021, 2, 300-309. https://0-doi-org.brum.beds.ac.uk/10.3390/psychiatryint2030023
Katsuki R, Kubo H, Yamakawa I, Shinfuku N, Sartorius N, Sakamoto S, Kato TA. Association between Self-Restraint Behavior, Stigma and Depressive Tendency in Office Workers during the COVID-19 Pandemic in Japan—Self-Restraint Behavior and Depression during the COVID-19. Psychiatry International. 2021; 2(3):300-309. https://0-doi-org.brum.beds.ac.uk/10.3390/psychiatryint2030023
Chicago/Turabian StyleKatsuki, Ryoko, Hiroaki Kubo, Itsuki Yamakawa, Naotaka Shinfuku, Norman Sartorius, Shinji Sakamoto, and Takahiro A. Kato. 2021. "Association between Self-Restraint Behavior, Stigma and Depressive Tendency in Office Workers during the COVID-19 Pandemic in Japan—Self-Restraint Behavior and Depression during the COVID-19" Psychiatry International 2, no. 3: 300-309. https://0-doi-org.brum.beds.ac.uk/10.3390/psychiatryint2030023