Biodistribution and Radiation Dosimetric Analysis of [68Ga]Ga-RM2: A Potent GRPR Antagonist in Prostate Carcinoma Patients


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Preparation of [68Ga]Ga-RM2
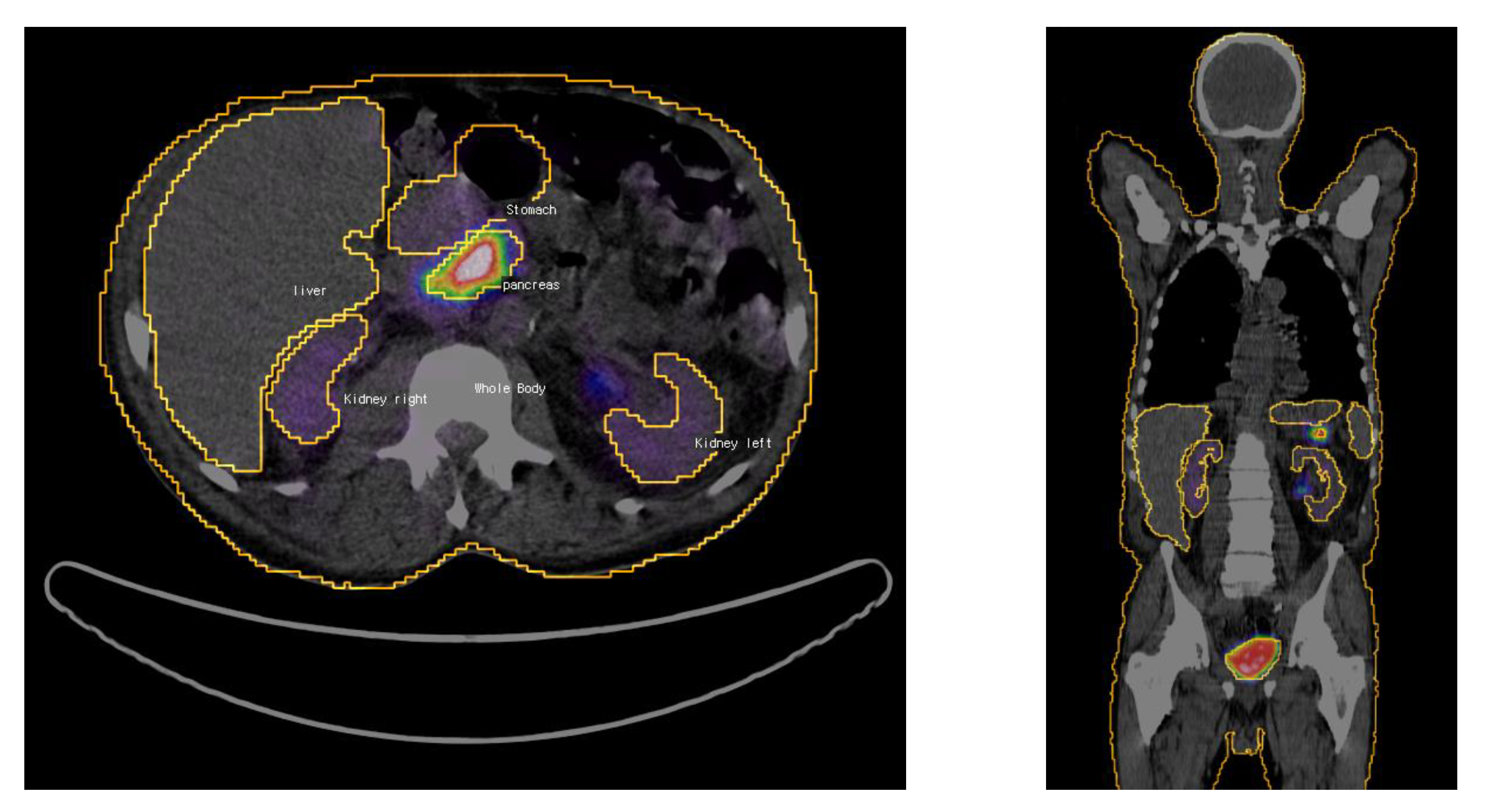
2.3. Imaging Protocol
2.4. Dosimetric Analysis
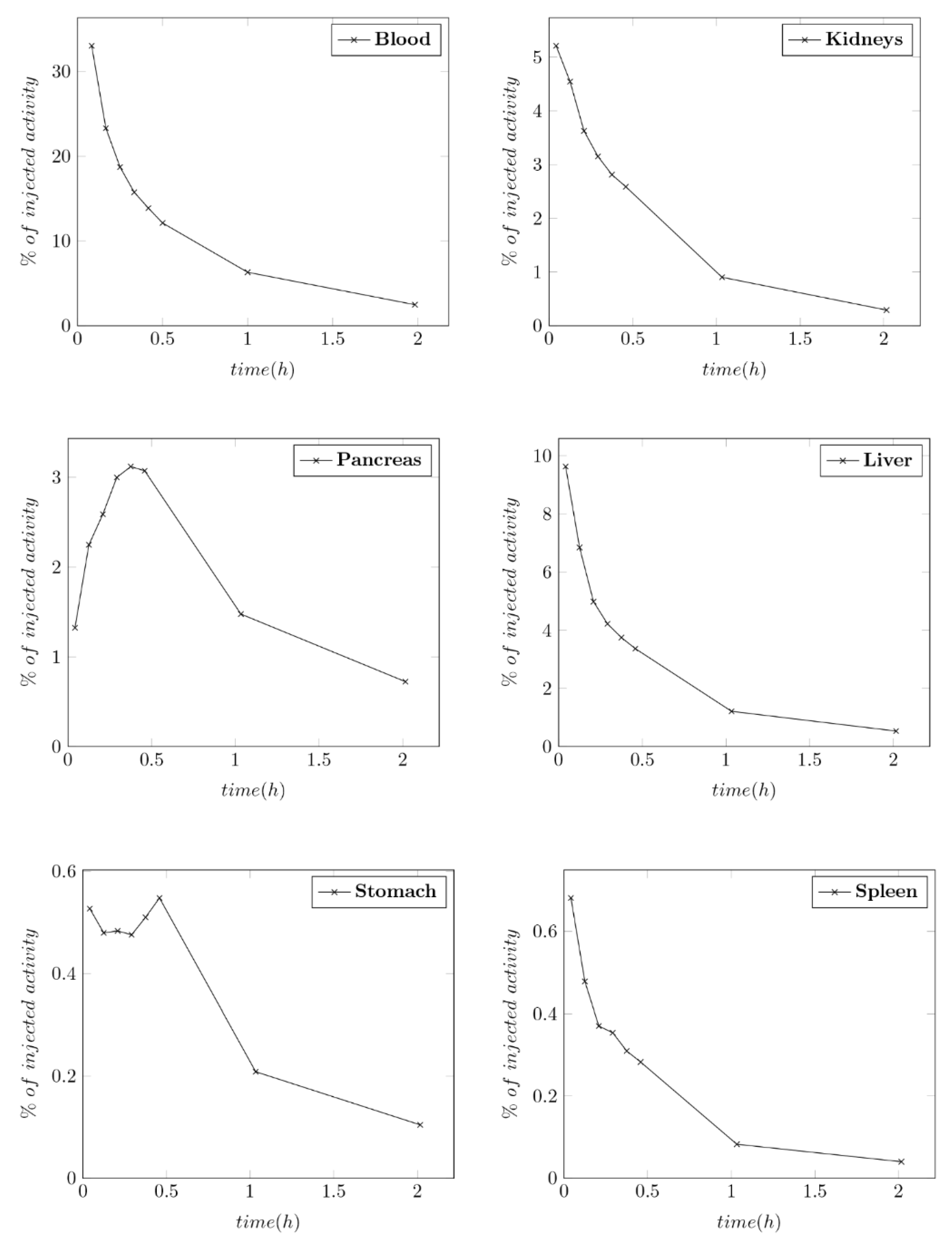
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Stewart, B.W.; Wild, C. World Cancer Report 2014; International Agency for Research on Cancer: Lyon, France; WHO Press World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Fox, J.; Schöder, H.; Larson, S.M. Molecular imaging of prostate cancer. Curr. Opin. Urol. 2012, 22, 320–327. [Google Scholar] [CrossRef] [Green Version]
- Pascale, M.; Azinwi, C.N.; Marongiu, B.; Pesce, G.; Stoffel, F.; Roggero, E. The outcome of prostate cancer patients treated with curative intent strongly depends on survival after metastatic progression. BMC Cancer 2017, 17, 651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freedland, S.J.; Humphreys, E.B.; Mangold, L.A.; Eisenberger, M.; Dorey, F.J.; Walsh, P.C.; Partin, A.W. Risk of Prostate Cancer–Specific Mortality Following Biochemical Recurrence After Radical Prostatectomy. JAMA 2005, 294, 433–439. [Google Scholar] [CrossRef] [Green Version]
- Minamimoto, R.; Sonni, I.; Hancock, S.; Vasanawala, S.S.; Loening, A.M.; Gambhir, S.S.; Iagaru, A. Prospective Evaluation of 68Ga-RM2 PET/MRI in Patients with Biochemical Recurrence of Prostate Cancer and Negative Findings on Conventional Imaging. J. Nucl. Med. 2017, 59, 803–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mason, B.R.; Eastham, J.A.; Davis, B.J.; Lance, A.M.; Thomas, J.P.; Richard, J.L.; Joseph, E.I. Current Status of MRI and PET in the NCCN Guidelines for Prostate Cancer. J. Natl. Compr. Canc. Netw. 2019, 17, 506–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelloff, G.J.; Choyke, P.; Coffey, D.S. Challenges in Clinical Prostate Cancer: Role of Imaging. Am. J. Roentgenol. 2009, 192, 1455–1470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lütje, S.; Heskamp, S.; Cornelissen, A.S.; Poeppel, T.D.; Van den Broek, S.A.M.W.; Rosenbaum-Krumme, S.; Bockisch, A.; Gotthardt, M.; Rijpkema, M.; Boerman, O.C. PSMA Ligands for Radionuclide Imaging and Therapy of Prostate Cancer: Clinical Status. Theranostics 2015, 5, 1388–1401. [Google Scholar] [CrossRef] [Green Version]
- Eiber, M.; Fendler, W.P.; Rowe, S.P.; Calais, J.; Hofman, M.S.; Maurer, T.; Schwarzenboeck, S.M.; Kratowchil, C.; Herrmann, K.; Giesel, F.L. Prostate-Specific Membrane Antigen Ligands for Imaging and Therapy. J. Nucl. Med. 2017, 58, 67S–76S. [Google Scholar] [CrossRef] [Green Version]
- Kasperzyk, J.L.; Finn, S.P.; Flavin, R.; Fiorentino, M.; Lis, R.; Hendrickson, W.K.; Clinton, S.K.; Sesso, H.D.; Giovannucci, E.L.; Stampfer, M.J.; et al. Prostate-Specific Membrane Antigen Protein Expression in Tumor Tissue and Risk of Lethal Prostate Cancer. Cancer Epidemiol. Biomark. Prev. 2013, 22, 2354–2363. [Google Scholar] [CrossRef] [Green Version]
- Mansi, R.; Wang, X.; Forrer, F.; Waser, B.; Cescato, R.; Graham, K.; Borkowski, S.; Reubi, J.C.; Maecke, H.R. Development of a potent DOTA-conjugated bombesin antagonist for targeting GRPr-positive tumours. Eur. J. Nucl. Med. Mol. Imaging 2010, 38, 97–107. [Google Scholar] [CrossRef] [Green Version]
- Cornelio, D.; Roesler, R.; Schwartsmann, G. Gastrin-releasing peptide receptor as a molecular target in experimental anticancer therapy. Ann. Oncol. 2007, 18, 1457–1466. [Google Scholar] [CrossRef] [PubMed]
- Liolios, C.; Schäfer, M.; Haberkorn, U.; Eder, M.; Kopka, K. Novel Bispecific PSMA/GRPr Targeting Radioligands with Optimized Pharmacokinetics for Improved PET Imaging of Prostate Cancer. Bioconjug. Chem. 2016, 27, 737–751. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Desai, P.; Koike, Y.; Houghton, J.; Carlin, S.D.; Tandon, N.; Touijer, K.; Weber, W.A. Dual-Modality Imaging of Prostate Cancer with a Fluorescent and Radiogallium-Labeled Gastrin-Releasing Peptide Receptor Antagonist. J. Nucl. Med. 2017, 58, 29–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kähkönen, E.; Jambor, I.; Kemppainen, J.; Lehtiö, K.; Grönroos, T.J.; Kuisma, A.; Luoto, P.; Sipilä, H.J.; Tolvanen, T.; Alanen, K.; et al. In Vivo Imaging of Prostate Cancer Using [68Ga]-Labeled Bombesin Analog BAY86-7548. Clin. Cancer Res. 2013, 19, 5434–5443. [Google Scholar] [CrossRef] [Green Version]
- Minamimoto, R.; Hancock, S.; Schneider, B. Pilot Comparison of ⁶⁸Ga-RM2 PET and ⁶⁸Ga-PSMA-11 PET in Patients with Biochemically Recurrent Prostate Cancer. J. Nucl. Med. 2016, 57, 557–562. [Google Scholar] [CrossRef] [Green Version]
- Wangerin, K.A.; Baratto, L.; Khalighi, M.M.; Hope, T.A.; Gulaka, P.K.; Deller, T.W.; Iagaru, A. Clinical Evaluation of 68Ga-PSMA-II and 68Ga-RM2 PET Images Reconstructed With an Improved Scatter Correction Algorithm. Am. J. Roentgenol. 2018, 211, 655–660. [Google Scholar] [CrossRef]
- Touijer, K.A.; Michaud, L.; Alvarez, H.A.V.; Gopalan, A.; Kossatz, S.; Gonen, M.; Beattie, B.; Sandler, I.; Lyaschenko, S.; Eastham, J.A.; et al. Prospective Study of the Radiolabeled GRPR Antagonist BAY86-7548 for Positron Emission Tomography/Computed Tomography Imaging of Newly Diagnosed Prostate Cancer. Eur. Urol. Oncol. 2019, 2, 166–173. [Google Scholar] [CrossRef]
- Wieser, G.; Popp, I.; Christian, R.H. Diagnosis of recurrent prostate cancer with PET/CT imaging using the gastrin-releasing peptide receptor antagonist 68Ga-RM2: Preliminary results in patients with negative or inconclusive 18FFluoroethylcholine-PET/CT. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1463–1472. [Google Scholar] [CrossRef]
- Kurth, J.; Krause, B.J.; Schwarzenböck, S.M.; Carina, B.; Oliver, W.H.; Martin, H. First-in-human dosimetry of gastrin-releasing peptide receptor antagonist 177LuLu-RM2: A radiopharmaceutical for the treatment of metastatic castration-resistant prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 123–135. [Google Scholar] [CrossRef]
- Roivainen, A.; Luoto, P.; Borkowski, S.; Jambor, I.; Rantala, T.; Sipilä, H.; Sparks, R.; Suilamo, S.; Tolvanen, T.; Valencia, R.; et al. Plasma Pharmacokinetics, Whole-Body Distribution, Metabolism, and Radiation Dosimetry of 68Ga Bombesin Antagonist BAY 86-7548 in Healthy Men. J. Nucl. Med. 2013, 54, 867–872. [Google Scholar] [CrossRef] [Green Version]
- Hindorf, C.; Glatting, G.; Chiesa, C.; Lindén, O.; Flux, G. EANM Dosimetry Committee guidelines for bone marrow and whole-body dosimetry. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 1238–1250. [Google Scholar] [CrossRef] [PubMed]
- ICRP. P089 Basic Anatomical and Physiological Data for Use in Radiological Protection Reference Values; ICRP: Stockholm, Sweden, 2011. [Google Scholar]
- ICRP. P103 the 2007 Recommendations of the International Commission on Radiological Protection; ICRP: Stockholm, Sweden, 2007. [Google Scholar]
- Gnesin, S.; Cicone, F.; Mitsakis, P.; Van Der Gucht, A.; Baechler, S.; Miralbell, R.; Garibotto, V.; Zilli, T.; Prior, J.O. First in-human radiation dosimetry of the gastrin-releasing peptide (GRP) receptor antagonist 68Ga-NODAGA-MJ9. EJNMMI Res. 2018, 8, 108. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Niu, G.; Fan, X.; Lang, L.; Hou, G.; Chen, L.; Wu, H.; Zhu, Z.; Li, F.; Chen, X. PET Using a GRPR Antagonist68Ga-RM26 in Healthy Volunteers and Prostate Cancer Patients. J. Nucl. Med. 2018, 59, 922–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, M.A.; Eitel, J.A.; Fletcher, J.W.; Mathias, C.J.; Tann, M.A.; Gardner, T.; Koch, M.O.; Territo, W.; Polson, H.; Hutchins, G.D. Estimation of radiation dosimetry for 68Ga-HBED-CC (PSMA-11) in patients with suspected recurrence of prostate cancer. Nucl. Med. Biol. 2017, 46, 32–35. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Li, D.; Lang, L.; Zhu, Z.; Wang, L.; Wu, P.; Niu, G.; Li, F.; Chen, X. 68Ga-NOTA-Aca-BBN(7-14) PET/CT in Healthy Volunteers and Glioma Patients. J. Nucl. Med. 2016, 57, 9–14. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characcteristics | Pt 1 | Pt 2 | Pt 3 | Pt 4 | Pt 5 | Mean | SD |
|---|---|---|---|---|---|---|---|
| Age | 74 | 66 | 72 | 76 | 69 | 71.4 | 3.97 |
| Weight | 72 | 89 | 72 | 96 | 80 | 81.8 | 10.59 |
| Height | 178 | 176 | 176 | 194 | 182 | 181.2 | 7.56 |
| Injected activity | 165 | 161 | 164 | 160 | 164 | 162.8 | 2.17 |
| PSA-Level (ng/mL) | 2045 * | 1.8 | 27.5 | 10.1 | 2.25 | 10.41 | 12.01 |
| Gleason score | 4 + 5 = 9 | 4 + 5 = 9 | 3 + 4 = 7 | 3 + 4 = 7 | 3 + 3 = 6 | - | - |
| Initial stage | IV B | II C | II C | III A | II C | - | - |
| Initial grade | 3 | 2 | 2 | 3 | 2 | - | - |
| Previous treatments | Hx, Bis, Ra, Lu, En, Arb, RTx | RPE, Rtx, Hx | RPE, RTx | RPE, Hx, RTx | RPE, RTx | - | - |
| Organ | Pt 1 | Pt 2 | Pt 3 | Pt 4 | Pt 5 | Mean | SD |
|---|---|---|---|---|---|---|---|
| Stomach | 0.239 | 0.012 | 0.005 | 0.006 | 0.007 | 0.054 | 0.104 |
| Kidneys | 0.026 | 0.038 | 0.025 | 0.035 | 0.033 | 0.032 | 0.006 |
| Liver | 0.066 | 0.053 | 0.049 | 0.033 | 0.047 | 0.049 | 0.012 |
| Pancreas | 0.062 | 0.040 | 0.011 | 0.034 | 0.040 | 0.037 | 0.018 |
| Red marrow | 0.013 | 0.012 | 0.014 | 0.023 | 0.015 | 0.015 | 0.004 |
| Spleen | 0.009 | 0.004 | 0.003 | 0.006 | 0.004 | 0.005 | 0.002 |
| Urinary bladder * | 0.400 | 0.400 | 0.400 | 0.400 | 0.400 | 0.400 | - |
| Remainder of body | 0.96 | 0.88 | 0.78 | 0.61 | 1.05 | 0.81 | 0.15 |
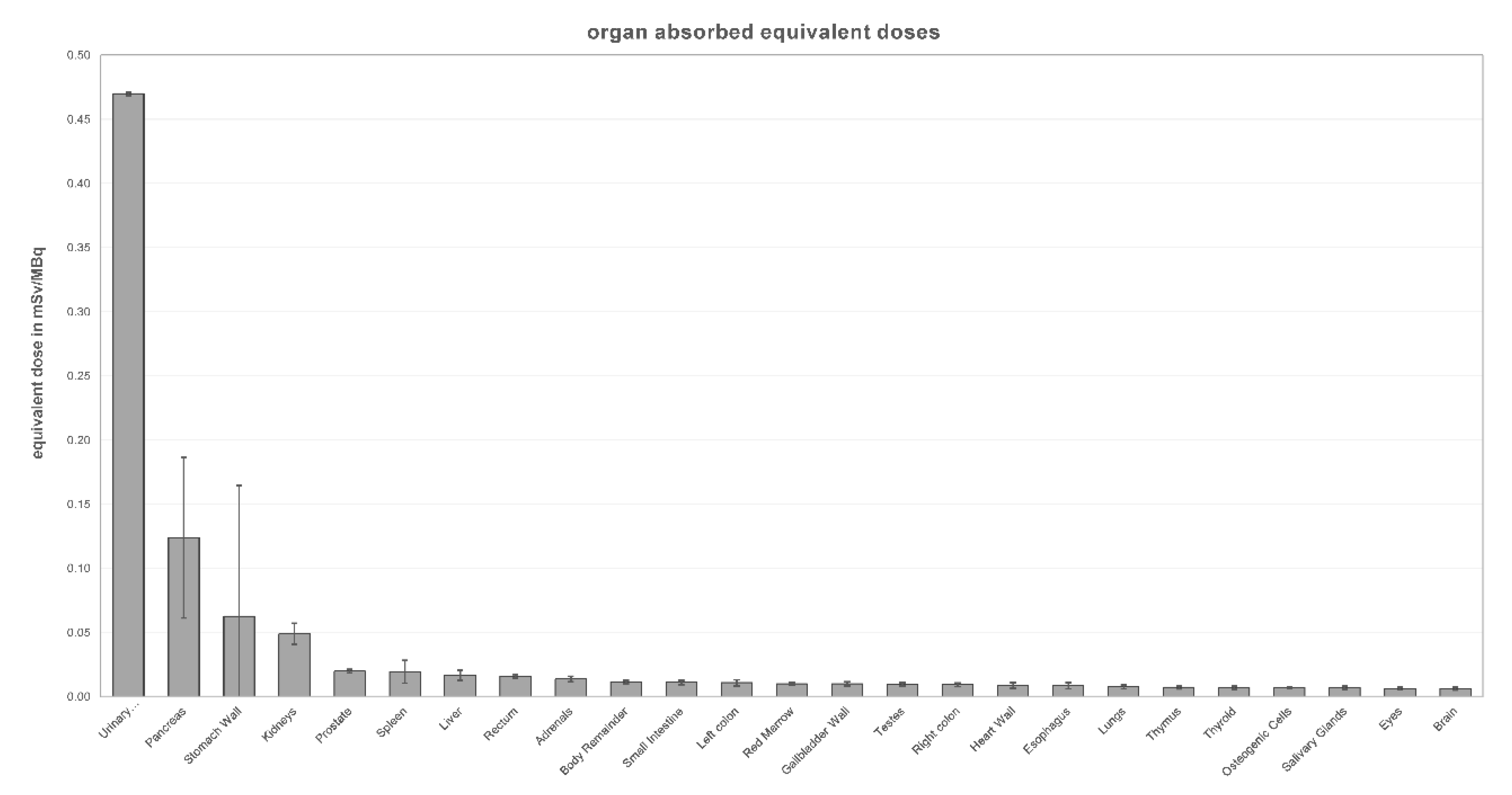
| Organ | Pt 1 | Pt 2 | Pt 3 | Pt 4 | Pt 5 | Mean | SD |
|---|---|---|---|---|---|---|---|
| Adrenals | 0.016 | 0.014 | 0.011 | 0.012 | 0.015 | 0.014 | 0.002 |
| Brain | 0.006 | 0.006 | 0.005 | 0.005 | 0.008 | 0.006 | 0.001 |
| Esophagus | 0.012 | 0.008 | 0.006 | 0.007 | 0.010 | 0.008 | 0.002 |
| Eyes | 0.006 | 0.006 | 0.005 | 0.005 | 0.008 | 0.006 | 0.001 |
| Gallbladder wall | 0.011 | 0.010 | 0.008 | 0.008 | 0.012 | 0.010 | 0.002 |
| Left colon | 0.014 | 0.011 | 0.008 | 0.009 | 0.012 | 0.011 | 0.002 |
| Small intestine | 0.012 | 0.011 | 0.009 | 0.010 | 0.013 | 0.011 | 0.002 |
| Stomach wall | 0.245 | 0.022 | 0.012 | 0.015 | 0.019 | 0.063 | 0.102 |
| Right colon | 0.009 | 0.009 | 0.008 | 0.008 | 0.011 | 0.009 | 0.001 |
| Rectum | 0.016 | 0.016 | 0.015 | 0.015 | 0.018 | 0.016 | 0.001 |
| Heart wall | 0.012 | 0.008 | 0.007 | 0.007 | 0.010 | 0.009 | 0.002 |
| Kidneys | 0.042 | 0.058 | 0.039 | 0.053 | 0.052 | 0.049 | 0.008 |
| Liver | 0.023 | 0.017 | 0.016 | 0.012 | 0.016 | 0.017 | 0.004 |
| Lungs | 0.009 | 0.007 | 0.006 | 0.006 | 0.009 | 0.008 | 0.002 |
| Pancreas | 0.212 | 0.131 | 0.037 | 0.109 | 0.130 | 0.124 | 0.063 |
| Prostate | 0.020 | 0.020 | 0.019 | 0.019 | 0.022 | 0.020 | 0.001 |
| Salivary glands | 0.006 | 0.007 | 0.006 | 0.006 | 0.009 | 0.007 | 0.001 |
| Red marrow | 0.010 | 0.009 | 0.009 | 0.010 | 0.011 | 0.010 | 0.001 |
| Osteogenic cells | 0.007 | 0.006 | 0.006 | 0.007 | 0.008 | 0.007 | 0.001 |
| Spleen | 0.034 | 0.017 | 0.010 | 0.021 | 0.015 | 0.019 | 0.009 |
| Testes | 0.009 | 0.010 | 0.009 | 0.009 | 0.012 | 0.009 | 0.001 |
| Thymus | 0.008 | 0.007 | 0.006 | 0.006 | 0.009 | 0.007 | 0.001 |
| Thyroid | 0.007 | 0.007 | 0.006 | 0.006 | 0.009 | 0.007 | 0.001 |
| Urinary bladder wall | 0.469 | 0.470 | 0.469 | 0.469 | 0.472 | 0.470 | 0.001 |
| Body remainder | 0.013 | 0.011 | 0.010 | 0.010 | 0.013 | 0.011 | 0.001 |
| Effective dose * | 0.063 | 0.033 | 0.030 | 0.031 | 0.034 | 0.038 | 0.014 |
| Organs | [68Ga]Ga-RM2 (Recent Study) | [68Ga]Ga-Bombesin [21] | [68Ga]Ga-MJ9 [25] | [68Ga]Ga-RM26 [26] | [68Ga]Ga-PSMA [27] | ||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | |
| Adrenals | 0.014 | 0.002 | 0.011 | 0.001 | 0.015 | 0.002 | 0.007 | 0.003 | 0.017 |
| Brain | 0.006 | 0.001 | 0.006 | 0.001 | 0.002 | 0.000 | 0.001 | 0.000 | 0.010 |
| Esophagus | 0.008 | 0.002 | — | — | 0.011 | 0.001 | — | — | — |
| Eyes | 0.006 | 0.001 | — | — | 0.008 | 0.000 | — | — | — |
| Gallbladder wall | 0.010 | 0.002 | 0.011 | 0.001 | 0.027 | 0.006 | 0.008 | 0.003 | 0.016 |
| Left colon | 0.011 | 0.002 | — | — | 0.034 | 0.009 | — | — | — |
| Small intestine | 0.011 | 0.002 | 0.010 | 0.000 | 0.039 | 0.010 | 0.010 | 0.003 | 0.014 |
| Stomach wall | 0.063 | 0.102 | 0.038 | 0.009 | 0.019 | 0.002 | 0.008 | 0.003 | 0.014 |
| Right colon | 0.009 | 0.001 | — | — | 0.032 | 0.010 | — | — | — |
| Rectum | 0.016 | 0.001 | — | — | 0.033 | 0.010 | — | — | — |
| Heart wall | 0.009 | 0.002 | 0.028 | 0.003 | 0.021 | 0.002 | 0.006 | 0.003 | 0.012 |
| Kidneys | 0.049 | 0.008 | 0.081 | 0.011 | 0.035 | 0.003 | 0.036 | 0.002 | 0.413 |
| Liver | 0.017 | 0.004 | 0.023 | 0.004 | 0.014 | 0.001 | 0.016 | 0.002 | 0.040 |
| Lungs | 0.008 | 0.002 | 0.007 | 0.000 | 0.013 | 0.002 | 0.006 | 0.001 | 0.012 |
| Pancreas | 0.124 | 0.063 | 0.510 | 0.160 | 0.260 | 0.061 | 0.225 | 0.038 | 0.020 |
| Prostate | 0.020 | 0.001 | — | — | 0.013 | 0.001 | — | — | — |
| Salivary glands | 0.007 | 0.001 | 0.022 | 0.002 | 0.009 | 0.000 | — | — | — |
| Red marrow | 0.010 | 0.001 | 0.013 | 0.009 | 0.009 | 0.000 | 0.009 | 0.002 | 0.010 |
| Osteogenic cells | 0.007 | 0.001 | 0.013 | 0.005 | 0.007 | 0.000 | 0.010 | 0.004 | 0.014 |
| Spleen | 0.019 | 0.009 | 0.023 | 0.004 | 0.014 | 0.002 | 0.019 | 0.001 | 0.058 |
| Testes | 0.009 | 0.001 | 0.010 | 0.000 | 0.010 | 0.001 | 0.011 | 0.001 | 0.011 |
| Thymus | 0.007 | 0.001 | 0.007 | 0.001 | 0.010 | 0.000 | 0.005 | 0.003 | 0.011 |
| Thyroid | 0.007 | 0.001 | 0.027 | 0.011 | 0.009 | 0.001 | 0.005 | 0.002 | 0.011 |
| Urinary bladder Wall | 0.470 | 0.001 | 0.610 | 0.057 | 0.112 | 0.020 | 1.090 | 0.225 | 0.067 |
| Body remainder | 0.011 | 0.001 | 0.010 | 0.000 | 0.012 | 0.001 | 0.010 | 0.003 | — |
| Effective dose * | 0.038 | 0.014 | 0.051 | 0.007 | 0.019 | 0.001 | 0.066 | 0.012 | 0.026 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haendeler, M.; Khawar, A.; Ahmadzadehfar, H.; Kürpig, S.; Meisenheimer, M.; Essler, M.; Gaertner, F.C.; Bundschuh, R.A. Biodistribution and Radiation Dosimetric Analysis of [68Ga]Ga-RM2: A Potent GRPR Antagonist in Prostate Carcinoma Patients. Radiation 2021, 1, 33-44. https://0-doi-org.brum.beds.ac.uk/10.3390/radiation1010004
Haendeler M, Khawar A, Ahmadzadehfar H, Kürpig S, Meisenheimer M, Essler M, Gaertner FC, Bundschuh RA. Biodistribution and Radiation Dosimetric Analysis of [68Ga]Ga-RM2: A Potent GRPR Antagonist in Prostate Carcinoma Patients. Radiation. 2021; 1(1):33-44. https://0-doi-org.brum.beds.ac.uk/10.3390/radiation1010004
Chicago/Turabian StyleHaendeler, Matthias, Ambreen Khawar, Hojjat Ahmadzadehfar, Stefan Kürpig, Michael Meisenheimer, Markus Essler, Florian C. Gaertner, and Ralph A. Bundschuh. 2021. "Biodistribution and Radiation Dosimetric Analysis of [68Ga]Ga-RM2: A Potent GRPR Antagonist in Prostate Carcinoma Patients" Radiation 1, no. 1: 33-44. https://0-doi-org.brum.beds.ac.uk/10.3390/radiation1010004