The Role of 2-[18F]-FDG PET/CT in Detecting Richter Transformation in Chronic Lymphocytic Leukemia: A Systematic Review

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
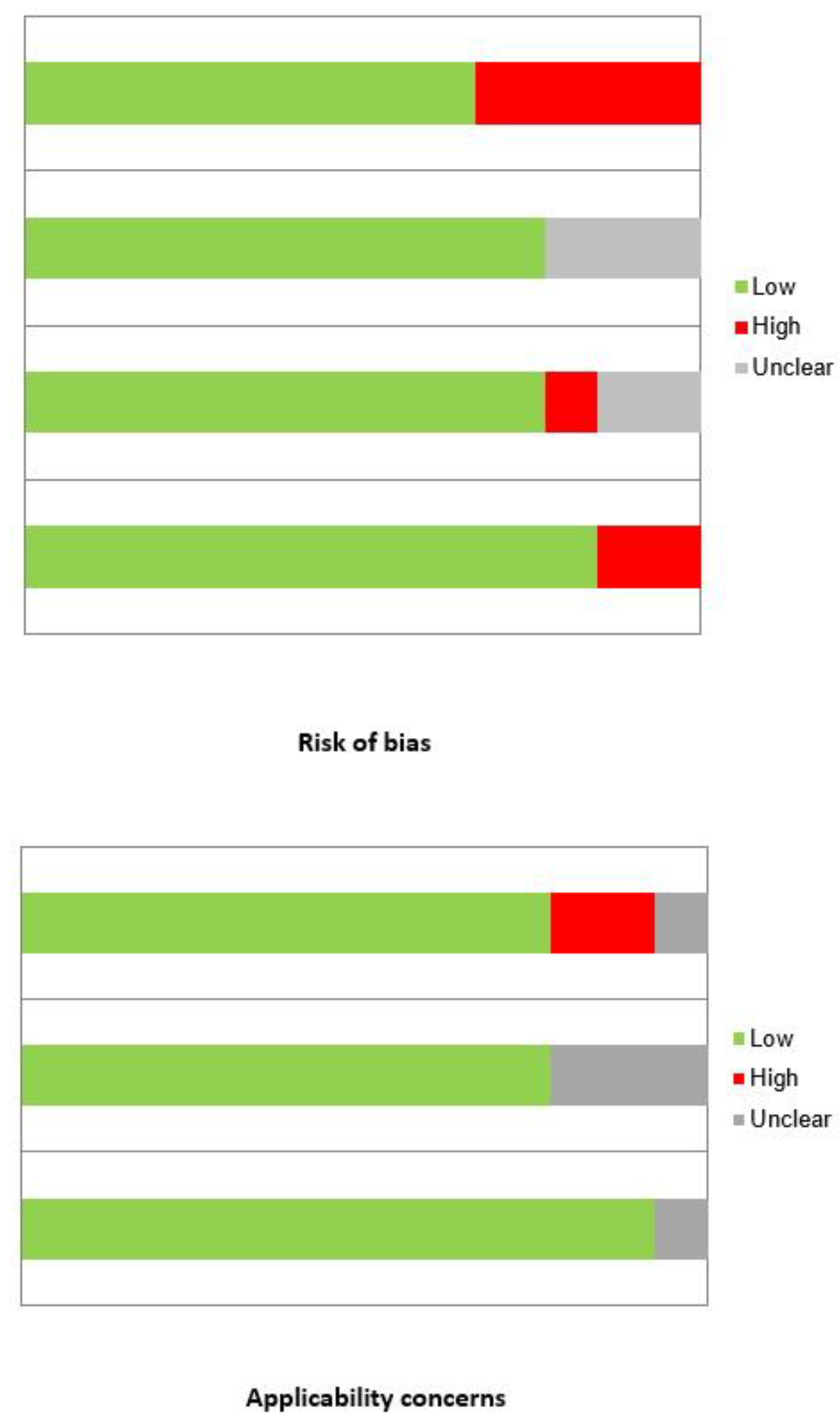
2.2. Study Selection and Quality Assessment
2.3. Data Extraction and Collection
3. Results
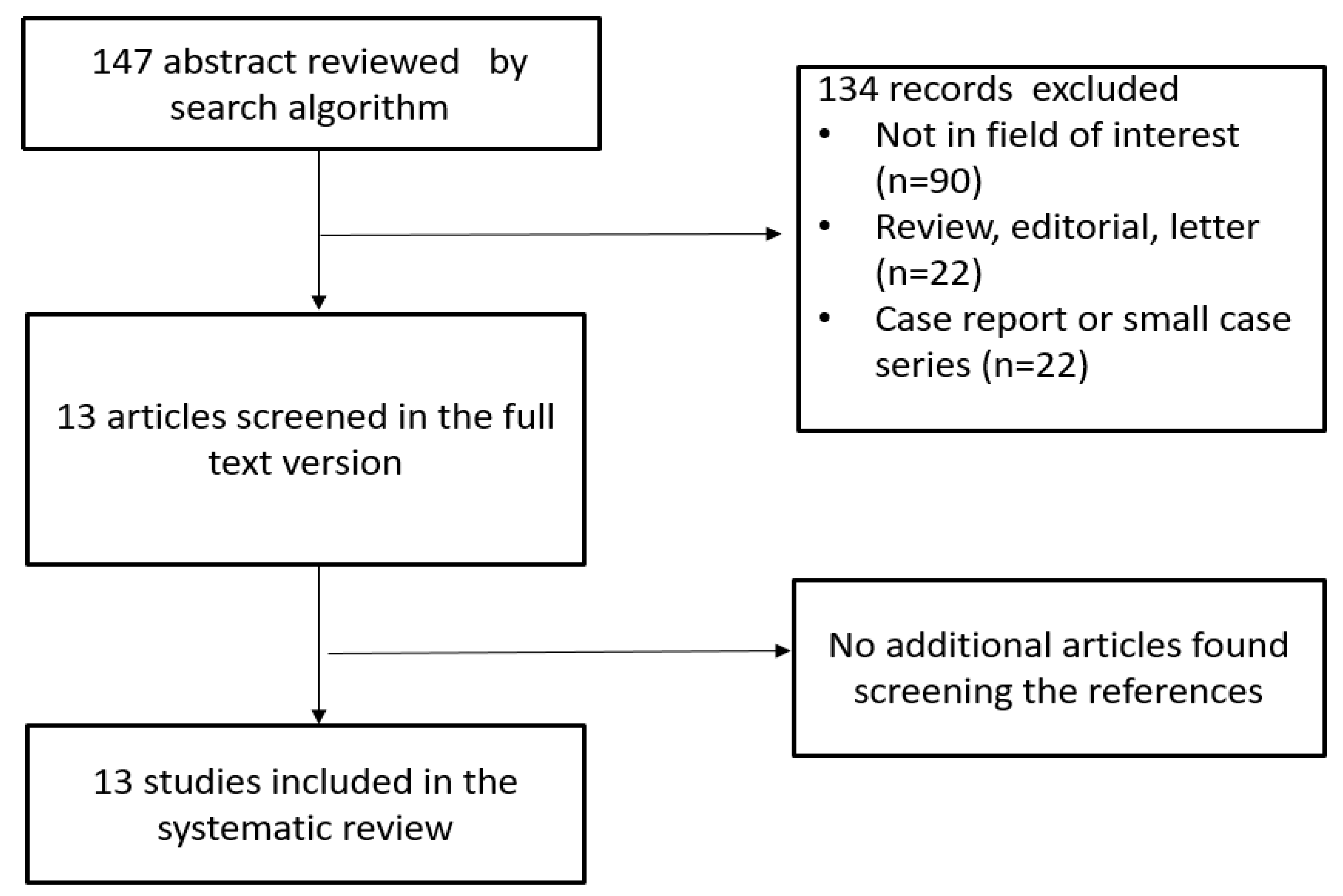
3.1. Literature Search
3.2. Qualitative Analysis
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hallek, M. Chronic lymphocytic leukemia: 2020 update on diagnosis, risk stratification and treatment. Am. J. Hematol. 2019, 94, 1266–1287. [Google Scholar] [CrossRef] [Green Version]
- Rozman, C.; Montserrat, E. Chronic Lymphocytic Leukemia. N. Engl. J. Med. 1995, 333, 1052–1057. [Google Scholar] [CrossRef] [Green Version]
- Parikh, S.A.; Kay, N.E.; Shanafelt, T.D. How we treat Richter syndrome. Blood 2014, 123, 1647–1657. [Google Scholar] [CrossRef] [PubMed]
- Parikh, S.A.; Rabe, K.G.; Call, T.G.; Zent, C.S.; Habermann, T.M.; Ding, W.; Leis, J.F.; Schwager, S.M.; Hanson, C.A.; Macon, W.R.; et al. Diffuse large B-cell lymphoma (Richter syndrome) in patients with chronic lymphocytic leukaemia: A cohort study of newly diagnosed patients. Br. J. Haematol. 2013, 162, 774–782. [Google Scholar] [CrossRef]
- Rossi, D. Richter’s syndrome: Novel and promising therapeutic alternatives. Best Pract. Res. Clin. Haematol. 2016, 29, 30–39. [Google Scholar] [CrossRef]
- Mato, A.R.; Nabhan, C.; Barr, P.M.; Ujjani, C.S.; Hill, B.T.; Lamanna, N.; Skarbnik, A.P.; Howlett, C.; Pu, J.J.; Sehgal, A.R.; et al. Outcomes of CLL patients treated with sequential kinase inhibitor therapy: A real world experience. Blood 2016, 128, 2199–2205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayers, E.C.; Mato, A.R. Richter’s Transformation in the Era of Kinase Inhibitor Therapy: A Review. Clin. Lymphoma Myeloma Leuk. 2017, 17, 1–6. [Google Scholar] [CrossRef]
- Khan, M.; Siddiqi, R.; Thompson, P.A. Approach to Richter transformation of chronic lymphocytic leukemia in the era of novel therapies. Ann. Hematol. 2018, 97, 1–15. [Google Scholar] [CrossRef]
- Condoluci, A.; Rossi, D. Treatment of Richter’s Syndrome. Curr. Treat. Options Oncol. 2017, 18, 75. [Google Scholar] [CrossRef]
- Eichhorst, B.; Robak, T.; Montserrat, E.; Ghia, P.; Niemann, C.; Kater, A.; Gregor, M.; Cymbalista, F.; Buske, C.; Hillmen, P.; et al. Chronic lymphocytic leukaemia: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2021, 32, 23–33. [Google Scholar] [CrossRef]
- Rhodes, J.M.; Mato, A.R. PET/Computed Tomography in Chronic Lymphocytic Leukemia and Richter Transformation. PET Clin. 2019, 14, 405–410. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, F.; Janjua, A.; Van Gestel, F.; Ahmad, A. Richter Transformation of Chronic Lymphocytic Leukemia: A Review of Fluorodeoxyglucose Positron Emission Tomography–Computed Tomography and Molecular Diagnostics. Cureus 2017, 9, e968. [Google Scholar] [CrossRef] [Green Version]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.M.; The QUADAS-2 Group. QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Bruzzi, J.F.; Macapinlac, H.; Tsimberidou, A.M.; Truong, M.T.; Keating, M.J.; Marom, E.M.; Munden, R.F. Detection of Richter’s transformation of chronic lymphocytic leukemia by PET/CT. J. Nucl. Med. 2006, 47, 1267–1273. [Google Scholar]
- Karam, M.; Novak, L.; Cyriac, J.; Ali, A.; Nazeer, T.; Nugent, F. Role of fluorine-18 fluoro-deoxyglucose positron emission tomography scan in the evaluation and follow-up of patients with low-grade lymphomas. Cancer 2006, 107, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Taralli, S.; Calcagni, M.L.; Rufini, V.; Laurenti, L.; Sica, S.; Chiusolo, P.; Leone, G.; Giordano, A. Role of 18F-FDG PET-CT for evaluating the response to reduced-intensity conditioning allogeneic transplant in heavily pre-treated patients with chronic lymphocytic leukemia: Preliminary results in nine patients. Ann. Nucl. Med. 2012, 26, 764–768. [Google Scholar] [CrossRef] [PubMed]
- Papajik, T.; Myslivecek, M.; Urbanova, R.; Buriankova, E.; Kapitanova, Z.; Procházka, V.; Turcsanyi, P.; Formánek, R.; Henzlová, L.; Flodr, P.; et al. 2-[18F]fluoro-2-deoxy-d-glucose positron emission tomography/computed tomography examination in patients with chronic lymphocytic leukemia may reveal Richter transformation. Leuk. Lymphoma 2014, 55, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Conte, M.J.; Bowen, D.A.; Wiseman, G.A.; Rabe, K.G.; Slager, S.L.; Schwager, S.M.; Call, T.G.; Viswanatha, D.S.; Zent, C.S. Use of positron emission tomography-computerized tomography (PET-CT) in the management of patients with chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL). Leuk. Lymphoma 2014, 55, 2079–2084. [Google Scholar] [CrossRef] [Green Version]
- Falchi, L.; Keating, M.J.; Marom, E.M.; Truong, M.T.; Schlette, E.J.; Sargent, R.L.; Trinh, L.; Wang, X.; Smith, S.C.; Jain, N.; et al. Correlation between FDG/PET findings, histological features, clinical characteristics and survival in 332 patients with chronic lymphocytic leukemia. Blood 2014, 123, 2783–2790. [Google Scholar] [CrossRef] [Green Version]
- Mauro, F.R.; Chauvie, S.; Paoloni, F.; Biggi, A.; Cimino, G.; Rago, A.; Gentile, M.A.; Morabito, F.C.; Coscia, M.; Bello, M.J.; et al. Diagnostic and prognostic role of PET/CT in patients with chronic lymphocytic leukemia and progressive disease. Leukemia 2015, 29, 1360–1365. [Google Scholar] [CrossRef]
- Michallet, A.S.; Sesques, P.; Rabe, K.G.; Itti, E.; Tordot, J.; Tychyj-Pinel, C.; Baseggio, L.; Subtil, F.; Salles, G.; Dupuis, J.M.; et al. An 18F-FDG-PET maximum standardized uptake value > 10 represents a novel valid marker for discerning Richter’s Syndrome. Leuk. Lymphoma 2016, 57, 1474–1477. [Google Scholar] [CrossRef]
- Mato, A.R.; Wierda, W.G.; Davids, M.S.; Cheson, B.D.; Coutre, S.E.; Choi, M.; Furman, R.R.; Heffner, L.; Barr, P.M.; Eradat, H.; et al. Utility of PET-CT in patients with chronic lymphocytic leukemia following B-cell receptor pathway inhibitor therapy. Haematologica 2019, 104, 2258–2264. [Google Scholar] [CrossRef] [Green Version]
- Pontoizeau, C.; Girard, A.; Mesbah, H.; Haumont, L.-A.; Devillers, A.; Tempescul, A.; Salaün, P.-Y.; Lamy, T.; Le Jeune, F.; Palard-Novello, X. Prognostic Value of Baseline Total Metabolic Tumor Volume Measured on FDG PET in Patients With Richter Syndrome. Clin. Nucl. Med. 2020, 45, 118–122. [Google Scholar] [CrossRef]
- Wang, Y.; Rabe, K.G.; Bold, M.S.; Shi, M.; Hanson, C.A.; Schwager, S.M.; Call, T.G.; Kenderian, S.S.; Muchtar, E.; Hayman, S.R.; et al. The role of 18F-FDG-PET in detecting Richter’s transformation of chronic lymphocytic leukemia in patients receiving therapy with a B-cell receptor inhibitor. Haematologica 2020, 105, 2675–2678. [Google Scholar] [CrossRef] [PubMed]
- Porrazzo, M.; Nicolai, E.; Riminucci, M.; Vitale, C.; Coscia, M.; De Paoli, L.; Rago, A.; Buscicchio, G.; Maestrini, G.; Ligia, S.; et al. Prognostic Significance of PET/CT in Patients with Chronic Lymphocytic Leukemia (CLL) Treated with Frontline Chemoimmunotherapy. Cancers 2020, 12, 1773. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Camoni, L.; Rodella, C.; Giubbini, R.; Bertagna, F. 2-[18F]-FDG PET/CT Role in Detecting Richter Transformation of Chronic Lymphocytic Leukemia and Predicting Overall Survival. Clin. Lymphoma Myeloma Leuk. 2021, 21, e277–e283. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A. Recommendations for Initial Evaluation, Staging, and Response Assessment of Hodgkin and Non-Hodgkin Lymphoma: The Lugano Classification. J. Clin. Oncol. 2014, 32, 3059–3067. [Google Scholar] [CrossRef]
- Barrington, S.F.; Mikhaeel, N.G.; Kostakoglu, L.; Meignan, M.; Hutchings, M.; Müeller, S.P.; Schwartz, L.H.; Zucca, E.; Fisher, R.I.; Trotman, J.; et al. Role of Imaging in the Staging and Response Assessment of Lymphoma: Consensus of the International Conference on Malignant Lymphomas Imaging Working Group. J. Clin. Oncol. 2014, 32, 3048–3058. [Google Scholar] [CrossRef]
- Albano, D.; Bosio, G.; Re, A.; Pagani, C.; Giubbini, R.; Bertagna, F. Metabolic behavior and prognostic value of early and end of treatment 18F-FDG PET/CT in adult Burkitt’s lymphoma: The role of Deauville and IHP criteria. Leuk. Lymphoma 2019, 60, 326–333. [Google Scholar] [CrossRef]
- Albano, D.; Bertagna, F.; Giubbini, R. 18F-FD PET/CT role in Burkitt lymphoma. Clin. Transl. Imaging 2020, 8, 39–45. [Google Scholar] [CrossRef]
- Albano, D.; Treglia, G.; Gazzilli, M.; Cerudelli, E.; Giubbini, R.; Bertagna, F. 18F-FDG PET or PET/CT in Mantle Cell Lymphoma. Clin. Lymphoma Myeloma Leuk. 2020, 20, 422–430. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Ferro, P.; Bosio, G.; Fallanca, F.; Re, A.; Tucci, A.; Ferreri, A.J.M.; Angelillo, P.; Gianolli, L.; Giubbini, R.; et al. Diagnostic and Clinical Impact of Staging 18F-FDG PET/CT in Mantle-Cell Lymphoma: A Two-Center Experience. Clin. Lymphoma Myeloma Leuk. 2019, 19, e457–e464. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Durmo, R.; Treglia, G.; Giubbini, R.; Bertagna, F. 18F-FDG PET/CT or PET Role in MALT Lymphoma: An Open Issue not Yet Solved—A Critical Review. Clin. Lymphoma Myeloma Leuk. 2020, 20, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Giubbini, R.; Bertagna, F. 18F-FDG PET/CT in splenic marginal lymphoma. Abdom. Radiol. 2018, 43, 2721–2727. [Google Scholar] [CrossRef] [PubMed]
- Alessandrino, F.; DiPiro, P.J.; Jagannathan, J.P.; Babina, G.; Krajewski, K.M.; Ramaiya, N.H.; Giardino, A.A. Multimodality imaging of indolent B cell lymphoma from diagnosis to transformation: What every radiologist should know. Insights Imaging 2019, 10, 25. [Google Scholar] [CrossRef] [Green Version]
- Constantino, C.S.; Oliveira, F.P.M.; Silva, M.; Oliveira, C.; Castanheira, J.C.; Silva, Â.; Vaz, S.C.; Vieira, P.; Costa, D.C. Are lesion features reproducible between 18F-FDG PET/CT images when acquired on analog or digital PET/CT scanners? Eur. Radiol. 2020, 1–9. [Google Scholar] [CrossRef]
- Kostakoglu, L.; Chauvie, S. Metabolic Tumor Volume Metrics in Lymphoma. Semin. Nucl. Med. 2018, 48, 50–66. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Bosio, G.; Bianchetti, N.; Pagani, C.; Re, A.; Tucci, A.; Giubbini, R.; Bertagna, F. Prognostic role of baseline 18F-FDG PET/CT metabolic parameters in mantle cell lymphoma. Ann. Nucl. Med. 2019, 33, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Bosio, G.; Pagani, C.; Re, A.; Tucci, A.; Giubbini, R.; Bertagna, F. Prognostic role of baseline 18F-FDG PET/CT metabolic parameters in Burkitt lymphoma. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 87–96. [Google Scholar] [CrossRef]
- Albano, D.; Bertoli, M.; Battistotti, M.; Rodella, C.; Statuto, M.; Giubbini, R.; Bertagna, F. Prognostic role of pretreatment 18F-FDG PET/CT in primary brain lymphoma. Ann. Nucl. Med. 2018, 32, 532–541. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Bosio, G.; Camoni, L.; Farina, M.; Re, A.; Tucci, A.; Giubbini, R.; Bertagna, F. Prognostic role of baseline 18F-FDG PET/CT parameters in MALT lymphoma. Hematol. Oncol. 2019, 37, 39–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayerhoefer, M.E.; Jaeger, U.; Staber, P.; Raderer, M.; Wadsak, W.; Pfaff, S.; Kornauth, C.; Senn, D.; Weber, M.; Wester, H.-J.; et al. [68Ga]Ga-Pentixafor PET/MRI for CXCR4 Imaging of Chronic Lymphocytic Leukemia: Preliminary Results. Investig. Radiol. 2018, 53, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, R.; Treglia, G. Systematic reviews and meta-analyses of diagnostic studies: A practical guideline. Clin. Transl. Imaging 2017, 5, 83–87. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| First Author | Year | Country | Study Design | CLL Patients | M:F Ratio | Mean Age (Range) | Patients with RT |
|---|---|---|---|---|---|---|---|
| Bruzzi J.F. [14] | 2006 | USA | Retrospective | 37 | 26:11 | 61 (40–82) | 11 (30%) |
| Karam M. [15] | 2006 | USA | Retrospective | 15 | nr | nr | 1 (7%) |
| Taralli S. [16] | 2012 | Italy | Retrospective | 9 | 8:1 | 57.7 (49–70) | 1 (11%) |
| Papajik T. [17] | 2014 | Czech Republic | Prospective | 44 | nr | nr | 8 (18%) |
| Conte M.J. [18] | 2014 | USA | Prospective | 272 | 197:75 | 61.5 * (21–91) | 25 (9%) |
| Falchi L. [19] | 2014 | USA | Retrospective | 332 | 218:114 | 68 * (31–85) | 95 (29%) |
| Mauro F.R. [20] | 2015 | Italy | Retrospective | 90 | 65:25 | 61.2 * (31–81) | 17 (19%) |
| Michallet A.S. [21] | 2016 | France | Retrospective | 240 | 94:146 | 62 (21–91) | 24 (10%) |
| Mato A.R. [22] | 2019 | USA | Prospective | 57 | nr | 67 * (28–85) | 8 (14%) |
| Pontoizeau C. [23] | 2020 | France | Retrospective | 28 | 22:6 | 71 * (36–89) | 28 (100%) |
| Wang Y. [24] | 2020 | USA | Retrospective | 92 | 69:23 | 68 * (43–89) | 25 (27%) |
| Porrazzo M. [25] | 2020 | Italy | Retrospective | 40 | 31:9 | 62 * (35–92) | 5 (13%) |
| Albano D. [26] | 2020 | Italy | Retrospective | 80 | 58:22 | 61 (27–83) | 18 (22.5%) |
| First Author | Device | Mean Radiopharmaceutical Injected Activity | Uptake Time (min) | Image Analysis | PET Semi-Quantitative Parameters |
|---|---|---|---|---|---|
| Bruzzi J.F. [14] | PET/CT | 555 MBq | 60 | Visual and semiquantitative | SUVmax |
| Karam M. [15] | PET | 592–700 MBq | 45 | Visual and semiquantitative | SUVmax |
| Taralli S. [16] | PET/CT | 166–318 MBq | 60 | Visual and semiquantitative | SUVmax |
| Papajik T. [17] | PET/CT | 400 MBq | 60 ± 3 | Visual and semiquantitative | SUVmax |
| Conte M.J. [18] | PET/CT | nr | nr | Visual and semiquantitative | SUVmax |
| Falchi L. [19] | PET & PET/CT | nr | nr | Visual and semiquantitative | SUVmax |
| Mauro F.R. [20] | PET/CT | nr | nr | Visual and semiquantitative | SUVmax |
| Michallet A.S. [21] | PET/CT | nr | nr | Visual and semiquantitative | SUVmax |
| Mato A.R. [22] | PET/CT | nr | nr | Visual and semiquantitative | SUVmax |
| Pontoizeau C. [23] | PET/CT | nr | nr | Visual and semiquantitative | SUVmax, MTV, TLG |
| Wang Y. [24] | PET | nr | nr | Visual and semiquantitative | SUVmax |
| Porrazzo M. [25] | PET/CT | 4 MBq/Kg | 60 ± 10 | Visual and semiquantitative | SUVmax |
| Albano D. [26] | PET/CT | 3.5–4.5 MBq/Kg | 60 | Visual and semiquantitative | SUVbw, SUVlbm, SUVbsa, L-L SUV R, L-BP SUV R, MTV, TLG |
| First Author | CLL Patients | RT Patients | SUVmax Cut-Off Used | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|---|
| Bruzzi J.F. [14] | 37 | 11 (30%) | 5 | 91% | 80% | 53% | 97% |
| Karam M. [15] | 15 | 1 (7%) | na | na | na | na | na |
| Taralli S. [16] | 9 | 1 (11%) | na | na | na | na | na |
| Papajik T. [17] | 44 | 8 (18%) | na | na | na | na | na |
| Conte M.J. [18] | 272 | 25 (9%) | 5 | na | na | na | na |
| Falchi L. [19] | 332 | 95 (29%) | 5 | 88% | 47% | 38% | 92% |
| Mauro F.R. [20] | 90 | 17 (19%) | 5 | 87% | 71% | 51% | 94% |
| Michallet A.S. [21] | 240 | 24 (10%) | 10 | 91% | 95% | 29% | 99% |
| Mato A.R. [22] | 57 | 8 (14%) | 5 | 71% | 4% | 16% | 33% |
| 10 | 71% | 50% | 26% | 88% | |||
| 11 | 71% | 61% | 31% | 89% | |||
| 12 | 57% | 68% | 31% | 86% | |||
| Pontoizeau C. [23] | 28 | 28 (100%) | na | na | na | na | na |
| Wang Y. [24] | 92 | 25 (27%) | 5 | 96% | 21% | 51% | 86% |
| 6 | 92% | 28% | 52% | 80% | |||
| 7 | 84% | 45% | 57% | 76% | |||
| 8 | 76% | 62% | 63% | 75% | |||
| 9 | 72% | 72% | 69% | 75% | |||
| 10 | 56% | 76% | 67% | 67% | |||
| 11 | 52% | 83% | 72% | 67% | |||
| 12 | 44% | 86% | 73% | 64% | |||
| 13 | 40% | 93% | 83% | 64% | |||
| 14 | 28% | 93% | 78% | 63% | |||
| 15 | 28% | 93% | 78% | 60% | |||
| Porrazzo M. [25] | 40 | 5 (13%) | 5 | 80% | 74% | 31% | 96% |
| Albano D. [26] | 80 | 18 (22.5%) | 9 | 67% | 90% | 67% | 90% |
Publisher‘s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albano, D.; Bertagna, F.; Dondi, F.; Annunziata, S.; Ceriani, L.; Giovanella, L.; Giubbini, R.; Treglia, G. The Role of 2-[18F]-FDG PET/CT in Detecting Richter Transformation in Chronic Lymphocytic Leukemia: A Systematic Review. Radiation 2021, 1, 65-76. https://0-doi-org.brum.beds.ac.uk/10.3390/radiation1010006
Albano D, Bertagna F, Dondi F, Annunziata S, Ceriani L, Giovanella L, Giubbini R, Treglia G. The Role of 2-[18F]-FDG PET/CT in Detecting Richter Transformation in Chronic Lymphocytic Leukemia: A Systematic Review. Radiation. 2021; 1(1):65-76. https://0-doi-org.brum.beds.ac.uk/10.3390/radiation1010006
Chicago/Turabian StyleAlbano, Domenico, Francesco Bertagna, Francesco Dondi, Salvatore Annunziata, Luca Ceriani, Luca Giovanella, Raffaele Giubbini, and Giorgio Treglia. 2021. "The Role of 2-[18F]-FDG PET/CT in Detecting Richter Transformation in Chronic Lymphocytic Leukemia: A Systematic Review" Radiation 1, no. 1: 65-76. https://0-doi-org.brum.beds.ac.uk/10.3390/radiation1010006